

Speaking Up and Taking Action: Psychological Safety and Joint Problem-Solving Orientation in Safety Improvement


Abstract
1. Introduction
1.1. Background: Psychological Safety and the Surfacing of Safety Concerns
1.2. Research Gap: From Surfacing Safety Concerns to Addressing Safety Concerns through Joint Problem-Solving
1.3. New Contribution and Significance of the Study
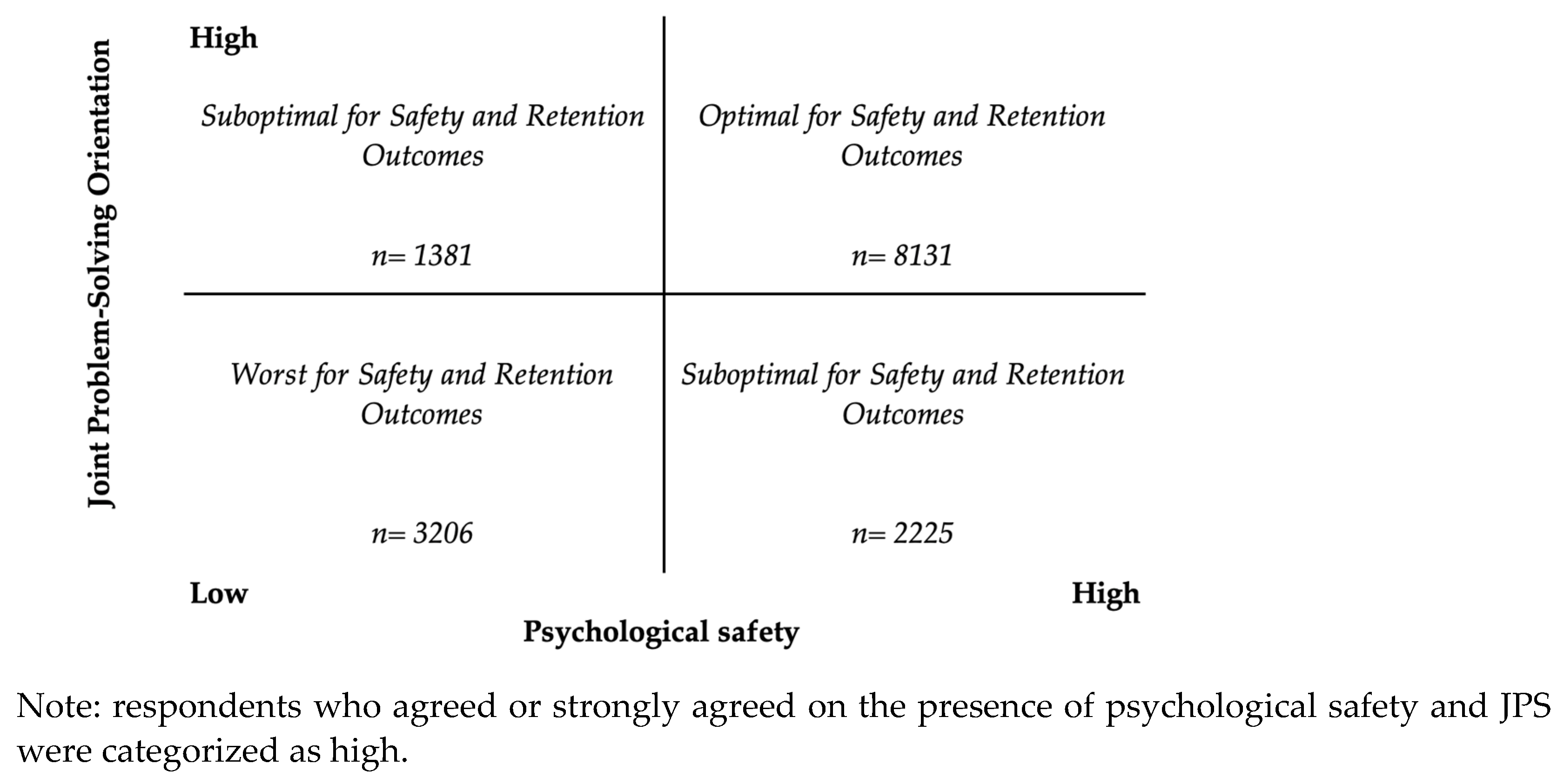
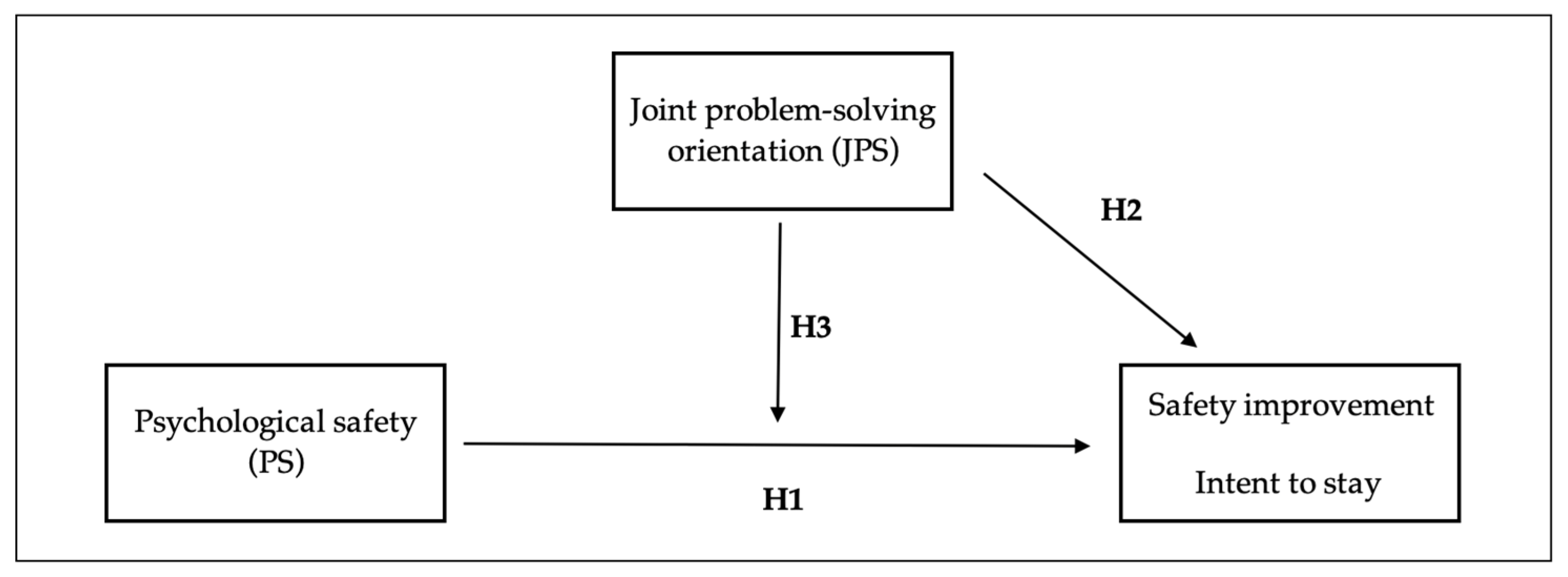
2. Conceptual Model and Hypotheses
3. Methods
3.1. Setting and Sample
3.2. Measurement Variables
3.2.1. Independent Variable
3.2.2. Independent and Moderating Variable
3.2.3. Dependent Variables
3.2.4. Control Variables
3.3. Statistical Analysis
4. Results
5. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Camargo, C.A.; Tsai, C.-L.; Sullivan, A.F.; Cleary, P.D.; Gordon, J.A.; Guadagnoli, E.; Kaushal, R.; Magid, D.J.; Rao, S.R.; Blumenthal, D. Safety Climate and Medical Errors in 62 US Emergency Departments. Ann. Emerg. Med. 2012, 60, 555–563.e20. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.W.; Levine, D.M.; Salmasian, H.; Syrowatka, A.; Shahian, D.M.; Lipsitz, S.; Zebrowski, J.P.; Myers, L.C.; Logan, M.S.; Roy, C.G.; et al. The Safety of Inpatient Health Care. N. Engl. J. Med. 2023, 388, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Committee on Quality of Healthcare in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Havens, D.H.; Boroughs, L. “To Err Is Human”: A Report from the Institute of Medicine. J. Pediatr. Health Care 2000, 14, 77–80. [Google Scholar]
- Singer, S.; Lin, S.; Falwell, A.; Gaba, D.; Baker, L. Relationship of Safety Climate and Safety Performance in Hospitals. Health Serv. Res. 2009, 44, 399–421. [Google Scholar] [CrossRef]
- Zohar, D. Safety Climate in Industrial Organizations: Theoretical and Applied Implications. J. Appl. Psychol. 1980, 65, 96–102. [Google Scholar] [CrossRef]
- Flin, R. Measuring Safety Climate in Health Care. Qual. Saf. Health Care 2006, 15, 109–115. [Google Scholar] [CrossRef]
- Naveh, E.; Katz-Navon, T.; Stern, Z. Treatment Errors in Healthcare: A Safety Climate Approach. Manag. Sci. 2005, 51, 948–960. [Google Scholar] [CrossRef]
- Brewer, B.B. Relationships Among Teams, Culture, Safety, and Cost Outcomes. West. J. Nurs. Res. 2006, 28, 641–653. [Google Scholar] [CrossRef]
- Clarke, S. The Relationship between Safety Climate and Safety Performance: A Meta-Analytic Review. J. Occup. Health Psychol. 2006, 11, 315–327. [Google Scholar] [CrossRef]
- Stone, P.W.; Gershon, R.R.M. Nurse Work Environments and Occupational Safety in Intensive Care Units. JONA J. Nurs. Adm. 2009, 39, S27. [Google Scholar] [CrossRef]
- Edmondson, A. Psychological Safety and Learning Behavior in Work Teams. Adm. Sci. Q. 1999, 44, 350–383. [Google Scholar] [CrossRef]
- Collins, C.J.; Smith, K.G. Knowledge Exchange and Combination: The Role of Human Resource Practices in the Performance of High-Technology Firms. Acad. Manag. J. 2006, 49, 544–560. [Google Scholar] [CrossRef]
- Siemsen, E.; Roth, A.V.; Balasubramanian, S.; Anand, G. The Influence of Psychological Safety and Confidence in Knowledge on Employee Knowledge Sharing. Manuf. Serv. Oper. Manag. 2009, 11, 429–447. [Google Scholar] [CrossRef]
- Ashford, S.J.; Rothbard, N.P.; Piderit, S.K.; Dutton, J.E. Out on a Limb: The Role of Context and Impression Management in Selling Gender-Equity Issues. Adm. Sci. Q. 1998, 43, 23. [Google Scholar] [CrossRef]
- Bunderson, J.S.; Boumgarden, P. Structure and Learning in Self-Managed Teams: Why “Bureaucratic” Teams Can Be Better Learners. Organ. Sci. 2010, 21, 609–624. [Google Scholar] [CrossRef]
- Carmeli, A. Social Capital, Psychological Safety and Learning Behaviours from Failure in Organisations. Long Range Plan. 2007, 40, 30–44. [Google Scholar] [CrossRef]
- Carmeli, A.; Gittell, J.H. High-quality Relationships, Psychological Safety, and Learning from Failures in Work Organizations. J. Organ. Behav. 2009, 30, 709–729. [Google Scholar] [CrossRef]
- Edmondson, A.C.; Bransby, D.P. Psychological Safety Comes of Age: Observed Themes in an Established Literature. Annu. Rev. Organ. Psychol. Organ. Behav. 2023, 10, 55–78. [Google Scholar] [CrossRef]
- Rosenbaum, L. Cursed by Knowledge—Building a Culture of Psychological Safety. N. Engl. J. Med. 2019, 380, 786–790. [Google Scholar] [CrossRef]
- Kark, R.; Carmeli, A. Alive and Creating: The Mediating Role of Vitality and Aliveness in the Relationship between Psychological Safety and Creative Work Involvement. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2009, 30, 785–804. [Google Scholar] [CrossRef]
- Rathert, C.; Ishqaidef, G.; Porter, T.H. Caring Work Environments and Clinician Emotional Exhaustion: Empirical Test of an Exploratory Model. Health Care Manag. Rev. 2022, 47, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Nembhard, I.M.; Edmondson, A.C. Making It Safe: The Effects of Leader Inclusiveness and Professional Status on Psychological Safety and Improvement Efforts in Health Care Teams. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2006, 27, 941–966. [Google Scholar] [CrossRef]
- Detert, J.R.; Treviño, L.K. Speaking Up to Higher-Ups: How Supervisors and Skip-Level Leaders Influence Employee Voice. Organ. Sci. 2010, 21, 249–270. [Google Scholar] [CrossRef]
- Fast, N.J.; Burris, E.R.; Bartel, C.A. Managing to Stay in the Dark: Managerial Self-Efficacy, Ego Defensiveness, and the Aversion to Employee Voice. Acad. Manag. J. 2014, 57, 1013–1034. [Google Scholar] [CrossRef]
- Satterstrom, P.; Vogus, T.J.; Jung, O.S.; Kerrissey, M. Voice Is Not Enough: A Multilevel Model of How Frontline Voice Can Reach Implementation. Health Care Manag. Rev. 2024, 49, 35. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, M.K.; Ahire, S.; Shang, G. Mitigating the Impact of Functional Dominance in Cross-Functional Process Improvement Teams. Decis. Sci. 2017, 48, 39–70. [Google Scholar] [CrossRef]
- Martins, L.L.; Schilpzand, M.C.; Kirkman, B.L.; Ivanaj, S.; Ivanaj, V. A Contingency View of the Effects of Cognitive Diversity on Team Performance: The Moderating Roles of Team Psychological Safety and Relationship Conflict. Small Group Res. 2013, 44, 96–126. [Google Scholar] [CrossRef]
- Detert, J.R.; Burris, E.R.; Harrison, D.A.; Martin, S.R. Voice Flows to and around Leaders: Understanding When Units Are Helped or Hurt by Employee Voice. Adm. Sci. Q. 2013, 58, 624–668. [Google Scholar] [CrossRef]
- Edmondson, A.C. Learning from Mistakes Is Easier Said Than Done: Group and Organizational Influences on the Detection and Correction of Human Error. J. Appl. Behav. Sci. 1996, 32, 5–28. [Google Scholar] [CrossRef]
- Valentine, M.A.; Edmondson, A.C. Team Scaffolds: How Mesolevel Structures Enable Role-Based Coordination in Temporary Groups. Organ. Sci. 2015, 26, 405–422. [Google Scholar] [CrossRef]
- Kerrissey, M.J.; Mayo, A.T.; Edmondson, A.C. Joint Problem-Solving Orientation in Fluid Cross-Boundary Teams. Acad. Manag. Discov. 2021, 7, 381–405. [Google Scholar] [CrossRef]
- Kerrissey, M.J.; Novikov, Z. Joint Problem-Solving Orientation, Mutual Value Recognition, and Performance in Fluid Teamwork Environments. Front. Psychol. 2024, 15, 1288904. [Google Scholar] [CrossRef] [PubMed]
- Belyansky, I.; Martin, T.R.; Prabhu, A.S.; Tsirline, V.B.; Howley, L.D.; Phillips, R.; Sindram, D.; Heniford, B.T.; Stefanidis, D. Poor Resident-Attending Intraoperative Communication May Compromise Patient Safety. J. Surg. Res. 2011, 171, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Leroy, H.; Dierynck, B.; Anseel, F.; Simons, T.; Halbesleben, J.R.B.; McCaughey, D.; Savage, G.T.; Sels, L. Behavioral Integrity for Safety, Priority of Safety, Psychological Safety, and Patient Safety: A Team-Level Study. J. Appl. Psychol. 2012, 97, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
- Rathert, C.; Ishqaidef, G.; May, D.R. Improving Work Environments in Health Care: Test of a Theoretical Framework. Health Care Manag. Rev. 2009, 34, 334. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, J.E.; Gaimon, C. Improving Manufacturing Performance Through Process Change and Knowledge Creation. Manag. Sci. 2000, 46, 265–288. [Google Scholar] [CrossRef]
- Tucker, A.L.; Nembhard, I.M.; Edmondson, A.C. Implementing New Practices: An Empirical Study of Organizational Learning in Hospital Intensive Care Units. Manag. Sci. 2007. [Google Scholar] [CrossRef]
- Jung, O.S.; Kundu, P.; Edmondson, A.C.; Hegde, J.; Agazaryan, N.; Steinberg, M.; Raldow, A. Resilience vs. Vulnerability: Psychological Safety and Reporting of near Misses with Varying Proximity to Harm in Radiation Oncology. Jt. Comm. J. Qual. Patient Saf. 2021, 47, 15–22. [Google Scholar] [CrossRef]
- Tucker, A.L.; Singer, S.J.; Hayes, J.E.; Falwell, A. Front-Line Staff Perspectives on Opportunities for Improving the Safety and Efficiency of Hospital Work Systems. Health Serv. Res. 2008, 43, 1807–1829. [Google Scholar] [CrossRef]
- Morrison, E.W. Employee Voice and Silence. Annu. Rev. Organ. Psychol. Organ. Behav. 2014, 1, 173–197. [Google Scholar] [CrossRef]
- Morrison, E.W. Employee Voice Behavior: Integration and Directions for Future Research. Acad. Manag. Ann. 2011, 5, 373–412. [Google Scholar] [CrossRef]
- Morrison, E.W.; Milliken, F.J. Organizational Silence: A Barrier to Change and Development in a Pluralistic World. Acad. Manag. Rev. 2000, 25, 706–725. [Google Scholar] [CrossRef]
- Robbins, J.; McAlearney, A.S. Toward a High-Performance Management System in Health Care, Part 5: How High-Performance Work Practices Facilitate Speaking up in Health Care Organizations. Health Care Manag. Rev. 2020, 45, 278. [Google Scholar] [CrossRef] [PubMed]
- Salas, E.; Reyes, D.L.; McDaniel, S.H. The Science of Teamwork: Progress, Reflections, and the Road Ahead. Am. Psychol. 2018, 73, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Swinth, R.L. Organizational Joint Problem-Solving. Manag. Sci. 1971, 18, B68–B79. [Google Scholar] [CrossRef]
- Hollnagel, E. Safer Complex Industrial Environments: A Human Factors Approach; CRC Press: Boca Raton, FL, USA, 2009. [Google Scholar]
- Schaefer, H.G.; Helmreich, R.L.; Scheidegger, D. Human Factors and Safety in Emergency Medicine. Resuscitation 1994, 28, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Lainidi, O.; Jendeby, M.K.; Montgomery, A.; Mouratidis, C.; Paitaridou, K.; Cook, C.; Johnson, J.; Karakasidou, E. An Integrative Systematic Review of Employee Silence and Voice in Healthcare: What Are We Really Measuring? Front. Psychiatry 2023, 14, 1111579. [Google Scholar] [CrossRef] [PubMed]
- Morrow, K.J.; Gustavson, A.M.; Jones, J. Speaking up Behaviours (Safety Voices) of Healthcare Workers: A Metasynthesis of Qualitative Research Studies. Int. J. Nurs. Stud. 2016, 64, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.C.; Shanafelt, T.D.; West, C.P.; Sinsky, C.A.; Trockel, M.T.; Nedelec, L.; Maldonado, Y.A.; Tutty, M.; Dyrbye, L.N.; Fassiotto, M. Burnout, Depression, Career Satisfaction, and Work-Life Integration by Physician Race/Ethnicity. JAMA Netw. Open 2020, 3, e2012762. [Google Scholar] [CrossRef]
- McPeek-Hinz, E.; Boazak, M.; Sexton, J.B.; Adair, K.C.; West, V.; Goldstein, B.A.; Alphin, R.S.; Idris, S.; Hammond, W.E.; Hwang, S.E.; et al. Clinician Burnout Associated with Sex, Clinician Type, Work Culture, and Use of Electronic Health Records. JAMA Netw. Open 2021, 4, e215686. [Google Scholar] [CrossRef]
- Driskell, J.E.; Salas, E. Group Decision Making under Stress. J. Appl. Psychol. 1991, 76, 473. [Google Scholar] [CrossRef]
- Foushee, H.C.; Helmreich, R.L. 7—Group Interaction and Flight Crew Performance. In Human Factors in Aviation; Wiener, E.L., Nagel, D.C., Eds.; Cognition and Perception; Academic Press: San Diego, CA, USA, 1988; pp. 189–227. ISBN 978-0-08-057090-7. [Google Scholar]
- Hermann, C.F. Some Consequences of Crisis Which Limit the Viability of Organizations. Adm. Sci. Q. 1963, 8, 61–82. [Google Scholar] [CrossRef]
- Detert, J.R.; Burris, E.R. Leadership Behavior and Employee Voice: Is the Door Really Open? Acad. Manag. J. 2007, 50, 869–884. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Female | 11,589 (77.55%) |
| Role | |
| Physician | 2214 (14.82%) |
| Nurse | 8024 (53.70%) |
| Advanced practice clinician | 1019 (6.82%) |
| Allied health professional | 3686 (24.67%) |
| Race | |
| White (not of Hispanic origin) | 12,217 (81.76%) |
| Black or African American | 1142 (7.64%) |
| Asian | 810 (5.42%) |
| Hispanic or Latino | 519 (3.47%) |
| Other | 255 (1.71%) |
| Tenure | |
| Less than 1 year | 1461 (9.78%) |
| Tenure 1–10 years | 7929 (53.06%) |
| Tenure 11–20 years | 3490 (23.36%) |
| Tenure >20 years | 2063 (13.81%) |
| Psychological Safety (2019) | Joint Problem-Solving (2019) | Safety Improvement (2019) | Safety Improvement (2021) | Intent to Stay (2019) | Intent to Stay (2021) | |
|---|---|---|---|---|---|---|
| Psychological safety (2019) | 1 | 0.67 * | 0.66 * | 0.37 * | 0.50 * | 0.31 * |
| Joint problem-solving (2019) | 1 | 0.52 * | 0.33 * | 0.49 * | 0.30 * | |
| Safety improvement (2019) | 1 | 0.43 * | 0.46 * | 0.31 * | ||
| Safety improvement (2021) | 1 | 0.29 * | 0.49 * | |||
| Intent to stay (2019) | 1 | 0.44 * | ||||
| Intent to stay (2021) | 1 |
| Measures | n | Mean | SD | Response Distribution (%) | ||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||
| Psychological safety (2019) | 14,936 | 4.12 | 0.71 | |||||
| Report patient safety mistakes without fear of punishment | 14,671 | 4.37 | 0.85 | 1.45 | 2.91 | 6.94 | 34.94 | 53.77 |
| Feel free to raise workplace safety concerns | 14,886 | 4.32 | 0.82 | 1.07 | 2.81 | 7.78 | 40.20 | 48.15 |
| Caregivers speak up if something negatively affects patient care | 14,759 | 4.29 | 0.85 | 1.16 | 3.69 | 8.02 | 39.64 | 47.49 |
| Caregivers feel free to question those with more authority | 14,752 | 3.53 | 1.09 | 4.77 | 13.72 | 23.67 | 39.19 | 18.65 |
| Joint problem-solving orientation (2019) | 14,606 | 3.92 | 0.82 | |||||
| View addressing problems as a team effort | 14,547 | 3.94 | 0.96 | 1.97 | 7.34 | 15.40 | 45.25 | 30.05 |
| Involve whomever needed to address the problem | 14,416 | 3.99 | 0.91 | 1.65 | 5.69 | 14.73 | 47.96 | 29.97 |
| Rely on people in other department to address problems with us | 14,157 | 3.83 | 0.90 | 1.53 | 6.56 | 21.83 | 47.51 | 22.58 |
| Safety improvement (2019) | 14,855 | 4.31 | 0.72 | |||||
| We are actively doing things to improve patient safety | 14,818 | 4.38 | 0.77 | 0.88 | 1.88 | 7.22 | 38.39 | 51.63 |
| Mistakes have led to positive changes | 14,586 | 4.24 | 0.79 | 0.73 | 1.89 | 12.42 | 42.80 | 42.17 |
| Safety improvement (2021) | 14,865 | 4.21 | 0.79 | |||||
| We are actively doing things to improve patient safety | 14,834 | 4.27 | 0.86 | 1.51 | 2.96 | 9.30 | 39.31 | 46.93 |
| Mistakes have led to positive changes | 14,620 | 4.15 | 0.85 | 1.07 | 2.81 | 14.63 | 42.59 | 38.90 |
| Intent to stay (2019) | 14,790 | 4.05 | 0.90 | 1.16 | 3.56 | 20.22 | 39.67 | 35.38 |
| Intent to stay (2021) | 14,763 | 3.94 | 0.97 | 2.08 | 5.03 | 22.62 | 36.97 | 33.30 |
| Safety Improvement | Intent to Stay | |||||||
|---|---|---|---|---|---|---|---|---|
| Cross-Sectional | Longitudinal | Cross-Sectional | Longitudinal | |||||
| Main Effect | Interaction | Main Effect | Interaction | Main Effect | Interaction | Main Effect | Interaction | |
| Psychological safety (PS) | 0.565 *** | 0.485 *** | 0.286 *** | 0.186 *** | 0.392 *** | 0.049 | 0.276 *** | 0.046 |
| Joint problem-solving (JPS) | 0.131 *** | 0.040 | 0.162 *** | 0.048 | 0.305 *** | −0.086 * | 0.199 *** | −0.062 |
| PS # JPS | 0.023 ** | 0.028 *** | 0.097 *** | 0.065 *** | ||||
| Female | 0.018 | 0.020 * | 0.023 | 0.025 | 0.028 * | 0.035 ** | 0.026 | 0.030 |
| Role | ||||||||
| Advanced practice provider | −0.040 | −0.039 * | −0.148 *** | −0.146 *** | 0.086 *** | 0.092 *** | −0.054 | −0.050 |
| Nurse | −0.082 *** | −0.080 *** | −0.242 *** | −0.240 *** | 0.143 *** | 0.150 *** | −0.049 * | −0.044 |
| Allied health professional | −0.083 *** | −0.082*** | −0.185 *** | −0.184 *** | 0.171 *** | 0.177 *** | −0.029 | −0.025 |
| Tenure | ||||||||
| 1–10 years | −0.007 | −0.008 | 0.127 *** | 0.126 *** | −0.075 *** | −0.079 *** | 0.149 *** | 0.147 *** |
| 11–20 years | 0.025 | 0.023 | 0.223 *** | 0.221 *** | −0.030 | −0.038 | 0.306 *** | 0.301 *** |
| >20 years | 0.073 *** | 0.071 *** | 0.278 *** | 0.275 *** | 0.060 ** | 0.052 ** | 0.439 *** | 0.434 *** |
| White | 0.011 | 0.012 | −0.029 | −0.028 | −0.039 ** | −0.035 ** | 0.035 * | 0.038 * |
| Intercept | 1.498 *** | 1.807 *** | 2.432 *** | 2.820 *** | 1.156 *** | 2.485 *** | 1.800 *** | 2.690 *** |
| Number of observations | 14,549 | 14,549 | 14,545 | 14,545 | 14,474 | 14,474 | 14,438 | 14,438 |
| R-squared | 0.45 | 0.45 | 0.17 | 0.17 | 0.30 | 0.31 | 0.13 | 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahadurzada, H.; Kerrissey, M.; Edmondson, A.C. Speaking Up and Taking Action: Psychological Safety and Joint Problem-Solving Orientation in Safety Improvement. Healthcare 2024, 12, 812. https://doi.org/10.3390/healthcare12080812
Bahadurzada H, Kerrissey M, Edmondson AC. Speaking Up and Taking Action: Psychological Safety and Joint Problem-Solving Orientation in Safety Improvement. Healthcare. 2024; 12(8):812. https://doi.org/10.3390/healthcare12080812
Chicago/Turabian StyleBahadurzada, Hassina, Michaela Kerrissey, and Amy C. Edmondson. 2024. "Speaking Up and Taking Action: Psychological Safety and Joint Problem-Solving Orientation in Safety Improvement" Healthcare 12, no. 8: 812. https://doi.org/10.3390/healthcare12080812
APA StyleBahadurzada, H., Kerrissey, M., & Edmondson, A. C. (2024). Speaking Up and Taking Action: Psychological Safety and Joint Problem-Solving Orientation in Safety Improvement. Healthcare, 12(8), 812. https://doi.org/10.3390/healthcare12080812