


Developmental Trajectories of Intrinsic Capacity Among Older Adults: Results from the China Longitudinal Study of Aging
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. IC
2.2.2. Independent Variables
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
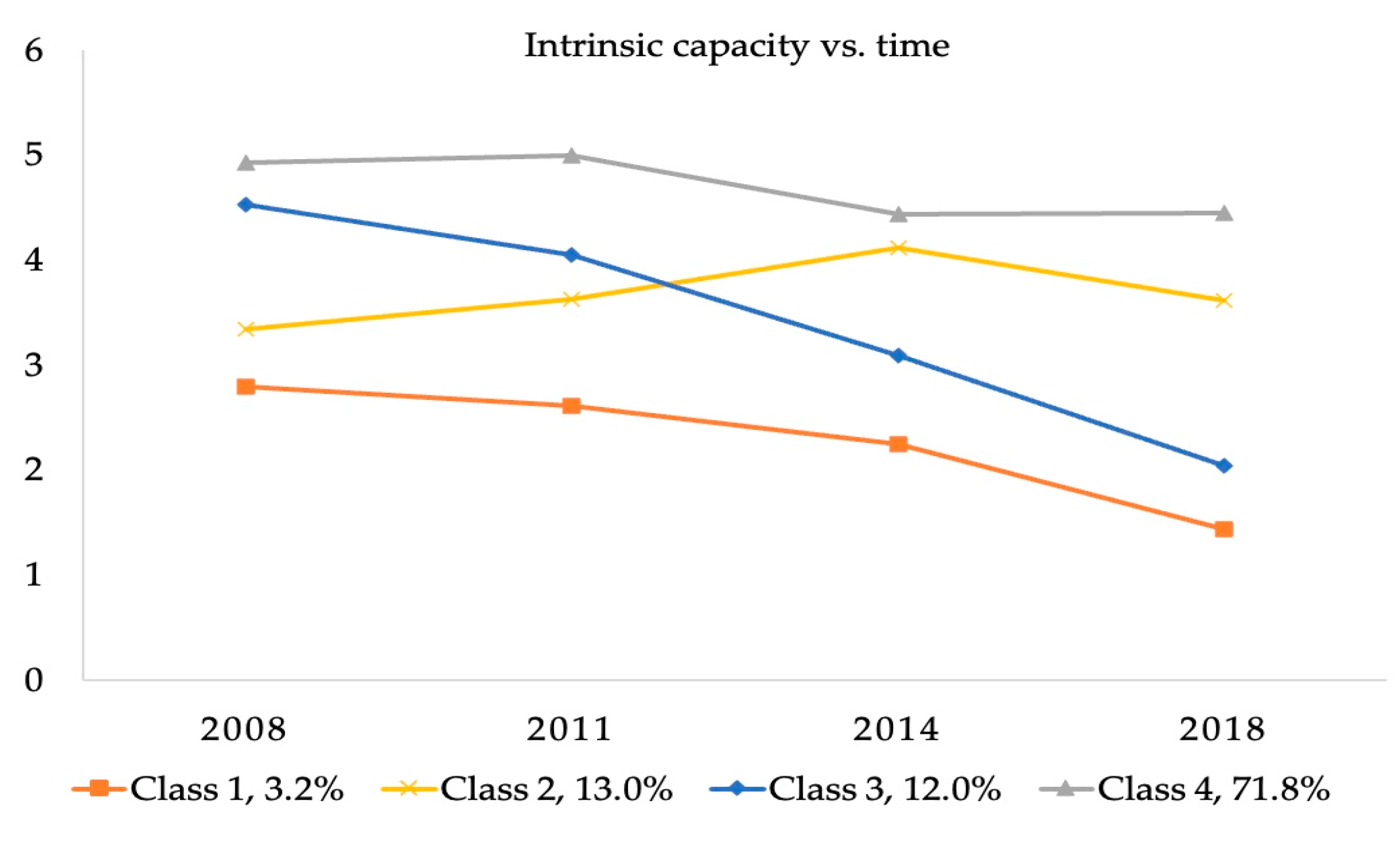
3.2. Classification of IC Trajectories
3.3. Influencing Factors of IC Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing; World Health Organization: Geneva, Switzerland; Available online: https://www.who.int/health-topics/ageing#tab=tab_1 (accessed on 10 February 2023).
- Mao, G.; Lu, F.; Fan, X.; Wu, D. China’s Ageing Population: The Present Situation and Prospects; Poot, J.M.R., Ed.; Springer: Singapore, 2020; pp. 269–287. [Google Scholar]
- Qiao, X. China’s Population Development, Changes and Current Situation, Reference to Data of the Seventh Population Census. Popul. Dev. 2021, 27, 74–88. [Google Scholar]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Beard, J.R.; Jotheeswaran, A.T.; Cesari, M.; De Carvalho, I.A. The structure and predictive value of intrinsic capacity in a longitudinal study of ageing. BMJ Open 2019, 9, e026119. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; Available online: https://www.who.int/publications/i/item/world-report-on-ageing-and-health (accessed on 10 February 2023).
- World Health Organization. Integrated Care for Older People (ICOPE): Guidance for Person-Centred Assessment and Pathways in Primary Care; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/handle/10665/326843 (accessed on 10 February 2023).
- World Health Organization. Integrated Care for Older People: Guidelines on Community-Level Interventions to Manage Declines in Intrinsic Capacity; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/258981 (accessed on 10 February 2023).
- World Health Organization. Ageing and Health. 2018. Available online: http://www.who.int/en/news-room/fact-sheets/detail/ageing-and-health (accessed on 10 February 2023).
- Liu, S.; Kang, L.; Liu, X.; Zhao, S.; Wang, X.; Li, J.; Jiang, S. Trajectory and Correlation of Intrinsic Capacity and Frailty in a Beijing Elderly Community. Front. Med. 2021, 8, 751586. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Liu, L.F.; Chang, S.M. Approaching person-centered long-term care: The trajectories of intrinsic capacity and functional decline in Taiwan. Geriatr. Gerontol. Int. 2022, 22, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Robledo, L.M.; García-Chanes, R.E.; Pérez-Zepeda, M.U. Allostatic Load as a Biological Substrate to Intrinsic Capacity: A Secondary Analysis of CRELES. J. Nutr. Health Aging 2019, 23, 788–795. [Google Scholar] [CrossRef]
- Zhao, J.; Chhetri, J.K.; Chang, Y.; Zheng, Z.; Ma, L.; Chan, P. Intrinsic Capacity vs. Multimorbidity: A Function-Centered Construct Predicts Disability Better Than a Disease-Based Approach in a Community-Dwelling Older Population Cohort. Front. Med. 2021, 8, 753295. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, J.; Li, J.; Li, H.; Wu, J.; Shen, J.; Wu, W.; Yuan, Y. Analysis of intrinsic capacity and influencing factors in community-dwelling elderly people. Chin. J. Geriat. 2022, 41, 591–595. [Google Scholar] [CrossRef]
- Ma, L.; Chhetri, J.K.; Zhang, L.; Sun, F.; Li, Y.; Tang, Z. Cross-sectional study examining the status of intrinsic capacity decline in community-dwelling older adults in China: Prevalence, associated factors and implications for clinical care. BMJ Open 2021, 11, e043062. [Google Scholar] [CrossRef]
- Stephens, C.; Allen, J.; Keating, N.; Szabó, Á.; Alpass, F. Neighborhood environments and intrinsic capacity interact to affect the health-related quality of life of older people in New Zealand. Maturitas 2020, 139, 1–5. [Google Scholar] [CrossRef]
- Wei, X.; Chen, Y.; Qin, J.; Yang, Y.; Yang, T.; Yan, F.; Zhang, Z.; Han, L.; Ma, Y. Factors associated with the intrinsic capacity in older adults: A scoping review. J. Clin. Nurs. 2024, 33, 1739–1750. [Google Scholar] [CrossRef] [PubMed]
- Salinas-Rodríguez, A.; González-Bautista, E.; Rivera-Almaraz, A.; Manrique-Espinoza, B. Longitudinal trajectories of intrinsic capacity and their association with quality of life and disability. Maturitas 2022, 161, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Yi, Z.; Vlosky, D.A.; Gu, D. Healthy Longevity in China: Demographic, Socioeconomic, and Psychological Dimensions; Springer: Dordrecht, The Netherlands, 2008; p. 120. [Google Scholar]
- Feng, Q.; Son, J.; Zeng, Y. Prevalence and correlates of successful ageing: A comparative study between China and South Korea. Eur. J. Ageing 2015, 12, 83–94. [Google Scholar] [CrossRef] [PubMed]
- George, P.P.; Lun, P.; Ong, S.P.; Lim, W.S. A Rapid Review of the Measurement of Intrinsic Capacity in Older Adults. J. Nutr. Health Aging 2021, 25, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Feng, Q.; Hesketh, T.; Christensen, K.; Vaupel, J.W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 2017, 389, 1619–1629. [Google Scholar] [CrossRef]
- Cooperartive Meta-analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults-study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Environ. Sci. 2002, 15, 83–96. [Google Scholar]
- Charles, A.; Buckinx, F.; Locquet, M.; Reginster, J.Y.; Petermans, J.; Gruslin, B.; Bruyère, O. Prediction of Adverse Outcomes in Nursing Home Residents According to Intrinsic Capacity Proposed by the World Health Organization. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1594–1599. [Google Scholar] [CrossRef]
- Lv, Y.B.; Gao, X.; Yin, Z.X.; Chen, H.S.; Luo, J.S.; Brasher, M.S.; Kraus, V.B.; Li, T.T.; Zeng, Y.; Shi, X.M. Revisiting the association of blood pressure with mortality in oldest old people in China: Community based, longitudinal prospective study. BMJ 2018, 361, k2158. [Google Scholar] [CrossRef]
- Zhang, Y.; Harper, S. The impact of son or daughter care on Chinese older adults’ mental health. Soc. Sci. Med. 2022, 306, 115104. [Google Scholar] [CrossRef]
- Wickrama, K.A.S.; Lee, T.K.; O’Neal, C.W.; Lorenz, F. Higher-Order Growth Curves and Mixture Modeling with Mplus: A Practical Guide; Routledge, Taylor & Francis Group: New York, NY, USA, 2016. [Google Scholar]
- Kim, S.Y. Determining the Number of Latent Classes in Single- and Multi-Phase Growth Mixture Models. Struct. Equ. Model. 2014, 21, 263–279. [Google Scholar] [CrossRef]
- Wang, M.C.; Deng, Q.W.; Bi, X.Y.; Ye, H.; Yang, W. Performance of the entropy as an index of classification accuracy in latent profile analysis: A monte Carlo simulation study. Acta Psychol. Sin. 2017, 49, 1473–1482. [Google Scholar] [CrossRef]
- Lo, Y.; Mendell, N.R.; Rubin, D.B. Testing the number of components in a normal mixture. Biometrika 2001, 88, 767–778. [Google Scholar] [CrossRef]
- Yu, J.; Si, H.; Jin, Y.; Qiao, X.; Ji, L.; Bian, Y.; Liu, Q.; Wang, W.; Wang, C. Patterns of intrinsic capacity among community-dwelling older adults: Identification by latent class analysis and association with one-year adverse outcomes. Geriatr. Nurs. 2022, 45, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.Y.M.; Su, J.J.; Lee, E.S.H.; Fung, J.T.; Molassiotis, A. Intrinsic capacity of older people in the community using WHO Integrated Care for Older People (ICOPE) framework: A cross-sectional study. BMC Geriatr. 2022, 22, 304. [Google Scholar] [CrossRef]
- Liu, Y.; Ouyang, X.; Hu, J. Influence of aging on intrinsic ability of elderly patients and analysis of related factors. Chin. J. Clin. Healthc. 2022, 25, 460–467. [Google Scholar] [CrossRef]
- Lee, Y.; Back, J.H.; Kim, J.; Kim, S.H.; Na, D.L.; Cheong, H.K.; Hong, C.H.; Kim, Y.G. Systematic review of health behavioral risks and cognitive health in older adults. Int. Psychogeriatr. 2010, 22, 174–187. [Google Scholar] [CrossRef]
- Rehm, J.; Hasan, O.S.M.; Black, S.E.; Shield, K.D.; Schwarzinger, M. Alcohol use and dementia: A systematic scoping review. Alzheimers Res. Ther. 2019, 11, 1. [Google Scholar] [CrossRef]
- Lemon, B.W.; Bengtson, V.L.; Peterson, J.A. An exploration of the activity theory of aging: Activity types and life satisfaction among in-movers to a retirement community. J. Gerontol. 1972, 27, 511–523. [Google Scholar] [CrossRef]
- Pinheiro, M.B.; Oliveira, J.S.; Baldwin, J.N.; Hassett, L.; Costa, N.; Gilchrist, H.; Wang, B.; Kwok, W.; Albuquerque, B.S.; Pivotto, L.R.; et al. Impact of physical activity programs and services for older adults: A rapid review. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 87. [Google Scholar] [CrossRef]
- Gutiérrez-Robledo, L.M.; García-Chanes, R.E.; Pérez-Zepeda, M.U. Screening intrinsic capacity and its epidemiological characterization: A secondary analysis of the Mexican Health and Aging Study. Rev. Panam. Salud Publica 2021, 45, e121. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Model | AIC | BIC | SABIC | Entropy | VLMR-LRT p-Value | BLRT p-Value | Classification Probability |
|---|---|---|---|---|---|---|---|
| 1-class | 31,036.680 | 31,071.513 | 31,052.449 | / | / | / | 1 |
| 2-class | 30,003.871 | 30,056.120 | 30,027.525 | 0.757 | <0.001 | <0.001 | 0.195/0.805 |
| 3-class | 29,904.699 | 29,974.365 | 29,936.238 | 0.749 | 0.0273 | <0.001 | 0.742/0.027/0.231 |
| 4-class | 29,791.254 | 29,878.336 | 29,830.677 | 0.729 | <0.001 | <0.001 | 0.032/0.130/0.120/0.718 |
| 5-class | 29,781.631 | 29,886.129 | 29,828.939 | 0.662 | 0.055 | <0.001 | 0.037/0.174/0.639/0.123/0.027 |
| Group | All (n) | Group 1 (n, %) | Group 2 (n, %) | Group 3 (n, %) | Group 4 (n, %) | χ2 | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Sociodemographic characteristics | ||||||||
| Age | 60~69 | 751 (30.6) | 2 (0.3) | 39 (5.2) | 57 (7.6) | 653 (86.9) | 323.277 | <0.001 |
| 70~79 | 1011 (41.2) | 20 (1.9) | 106 (10.5) | 106 (10.5) | 779 (77.1) | |||
| ≥80 | 692 (28.2) | 57 (8.2) | 173 (25) | 132 (19.1) | 330 (47.7) | |||
| Gender | Male | 1147 (46.7) | 20 (1.7) | 79 (6.9) | 84 (7.3) | 964 (84.0) | 160.320 | <0.001 |
| Female | 1307 (53.3) | 59 (4.5) | 239 (18.3) | 211 (16.1) | 798 (61.1) | |||
| Marital status | Married | 1433 (58.4) | 26 (1.8) | 127 (8.9) | 124 (8.7) | 1156 (80.7) | 165.032 | <0.001 |
| Divorced | 77 (3.1) | 1 (1.3) | 3 (3.9) | 9 (11.7) | 64 (83.1) | |||
| Widowed | 919 (37.4) | 51 (5.5) | 185 (20.1) | 159 (17.3) | 524 (57.0) | |||
| Never married | 25 (1.1) | 1 (4) | 3 (12) | 3 (12) | 18 (72) | |||
| Co-residence with household member(s) | Yes | 2061 (84.0) | 66 (3.2) | 245 (11.9) | 225 (10.9) | 1525 (74.0) | 33.068 | <0.001 |
| No | 393 (16.0) | 13 (3.3) | 73 (18.6) | 70 (17.8) | 237 (60.3) | |||
| Financial support | Yes | 1915 (78.0) | 53 (2.8) | 243 (12.7) | 213 (11.1) | 1406 (73.4) | 15.050 | 0.002 |
| No | 539 (22.0) | 26 (4.8) | 75 (13.9) | 82 (15.2) | 356 (66.0) | |||
| Self-rated economic status | Rich | 319 (13.0) | 14 (4.4) | 38 (11.9) | 28 (8.8) | 239 (74.9) | 40.980 | <0.001 |
| Not bad | 1742 (71.0) | 44 (2.5) | 222 (12.7) | 191 (11.0) | 1285 (73.8) | |||
| Poor | 393 (16.0) | 21 (5.3) | 58 (14.8) | 76 (19.3) | 238 (60.6) | |||
| Lifestyles | ||||||||
| Smoking | Yes | 554 (22.6) | 11 (2.0) | 35 (6.3) | 54 (9.7) | 454 (82.0) | 41.075 | <0.001 |
| No | 1900 (77.4) | 68 (3.6) | 283 (14.9) | 241 (12.7) | 1308 (68.8) | |||
| Drinking | Yes | 542 (22.1) | 6 (1.1) | 44 (8.1) | 41 (7.6) | 451 (83.2) | 46.323 | <0.001 |
| No | 1912 (77.9) | 73 (3.8) | 274 (14.3) | 254 (13.3) | 1311 (68.6) | |||
| Exercise | Yes | 852 (34.7) | 14 (1.6) | 107 (12.6) | 96 (11.3) | 635 (74.5) | 12.202 | 0.007 |
| No | 1602 (65.3) | 65 (4.1) | 211 (13.2) | 199 (12.4) | 1127 (70.3) | |||
| Social activity | Yes | 461 (18.8) | 2 (0.4) | 39 (8.5) | 39 (8.5) | 381 (82.6) | 37.832 | <0.001 |
| No | 1993 (81.2) | 77 (3.9) | 279 (14.0) | 256 (12.8) | 1381 (69.3) | |||
| Social services | ||||||||
| Medical service | Yes | 2291 (93.4) | 66 (2.9) | 290 (12.7) | 260 (11.3) | 1675 (73.1) | 35.898 | <0.001 |
| No | 163 (6.6) | 13 (8.0) | 28 (17.1) | 35 (21.5) | 87 (53.4) | |||
| Retirement pension | Yes | 417 (17.0) | 4 (1.0) | 48 (11.5) | 27 (6.5) | 338 (81.1) | 27.630 | <0.001 |
| No | 2037 (83.0) | 75 (3.7) | 270 (13.3) | 268 (13.2) | 1424 (69.9) | |||
| Life satisfaction | Good | 1417 (57.7) | 47 (3.3) | 176 (12.4) | 146 (10.3) | 1048 (74.0) | 11.253 | 0.010 |
| Bad | 1037 (42.3) | 32 (3.1) | 142 (13.7) | 149 (14.4) | 714 (68.8) | |||
| Self-rated health | Good | 1393 (56.8) | 37 (2.7) | 161 (11.6) | 131 (9.4) | 1064 (76.3) | 35.823 | <0.001 |
| Bad | 1061 (43.2) | 42 (4.0) | 157 (14.8) | 164 (15.5) | 698 (65.8) |
| Measures |
Class 1 OR (95% CI) |
Class 2 OR (95% CI) |
Class 3 OR (95% CI) |
Class 4 OR (95% CI) |
|---|---|---|---|---|
| Sociodemographic characteristics | ||||
| Age (≥80) | ||||
| 60~69 | ref | 5.890 (1.344–25.812) * | 11.295 (2.599–49.081) ** | 45.947 (10.876–194.110) *** |
| 70~79 | ref | 1.580 (0.874–2.854) | 2.087 (1.149–3.791) * | 5.720 (3.275–9.991) *** |
| Gender (female) | ||||
| Male | ref | 0.834 (0.422–1.648) | 0.920 (0.464–1.826) | 2.576 (1.364–4.865) ** |
| Marital status (never married) | ||||
| Married | ref | 2.230 (0.194–25.685) | 3.131 (0.269–36.498) | 5.203 (0.548–49.379) |
| Divorced | ref | 1.236 (0.046–33.514) | 5.208 (0.216–125.534) | 7.110 (0.358–141.191) |
| Widowed | ref | 1.797 (0.158–20.422) | 2.555 (0.222–29.398) | 3.128 (0.333–29.353) |
| Co-residence with household member(s) (no) | ||||
| Yes | ref | 0.536 (0.262–1.096) | 0.514 (0.250–1.057) | 0.577 (0.289–1.149) |
| financial support (no) | ||||
| Yes | ref | 1.474 (0.741–2.933) | 1.681 (0.843–3.352) | 1.382 (0.723–2.639) |
| Self-rated economic status (poor) | ||||
| Not bad | ref | 0.566 (0.207–1.493) | 0.376 (0.138–1.024) | 0.633 (0.251–1.593) |
| Rich | ref | 1.251 (0.597–2.619) | 0.869 (0.418–1.808) | 1.484 (0.739–2.977) |
| Lifestyles | ||||
| Smoking (no) | ||||
| Yes | ref | 0.570 (0.248–1.307) | 1.010 (0.449–2.273) | 0.710 (0.331–1.522) |
| Drinking (no) | ||||
| Yes | ref | 2.306 (0.902–5.898) | 1.866 (0.725–4.804) | 2.630 (1.072–6.450) * |
| Exercise (no) | ||||
| Yes | ref | 1.872 (0.973–3.602) | 1.944 (1.006–3.756) * | 1.679 (0.896–3.145) |
| Social activity (no) | ||||
| Yes | ref | 3.807 (0.878–16.498) | 4.648 (1.072–20.147) * | 5.905 (1.401–24.888) * |
| Social services | ||||
| Medical service (no) | ||||
| Yes | ref | 1.590 (0.679–3.722) | 1.370 (−0.594–3.163) | 2.061 (0.924–4.598) |
| Retirement pension (no) | ||||
| Yes | ref | 0.427 (0.139–1.313) | 0.809 (0.255–2.567) | 0.505 (0.169–1.504) |
| Life satisfaction (bad) | ||||
| Good | ref | 0.663 (0.361–1.217) | 0.652 (0.354–1.201) | 0.753 (0.423–1.342) |
| Self-rated health (bad) | ||||
| Good | ref | 1.277 (0.726–2.248) | 1.072 (0.606–1.898) | 1.860 (1.088–3.180) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, J.; Chang, H.; Wang, Z. Developmental Trajectories of Intrinsic Capacity Among Older Adults: Results from the China Longitudinal Study of Aging. Healthcare 2025, 13, 520. https://doi.org/10.3390/healthcare13050520
Zhou J, Chang H, Wang Z. Developmental Trajectories of Intrinsic Capacity Among Older Adults: Results from the China Longitudinal Study of Aging. Healthcare. 2025; 13(5):520. https://doi.org/10.3390/healthcare13050520
Chicago/Turabian StyleZhou, Jia, Hui Chang, and Zhiwen Wang. 2025. "Developmental Trajectories of Intrinsic Capacity Among Older Adults: Results from the China Longitudinal Study of Aging" Healthcare 13, no. 5: 520. https://doi.org/10.3390/healthcare13050520
APA StyleZhou, J., Chang, H., & Wang, Z. (2025). Developmental Trajectories of Intrinsic Capacity Among Older Adults: Results from the China Longitudinal Study of Aging. Healthcare, 13(5), 520. https://doi.org/10.3390/healthcare13050520