
Influencing Factors of Depression among Adolescent Asians in North America: A Systematic Review

 ,
,  and
and {kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources
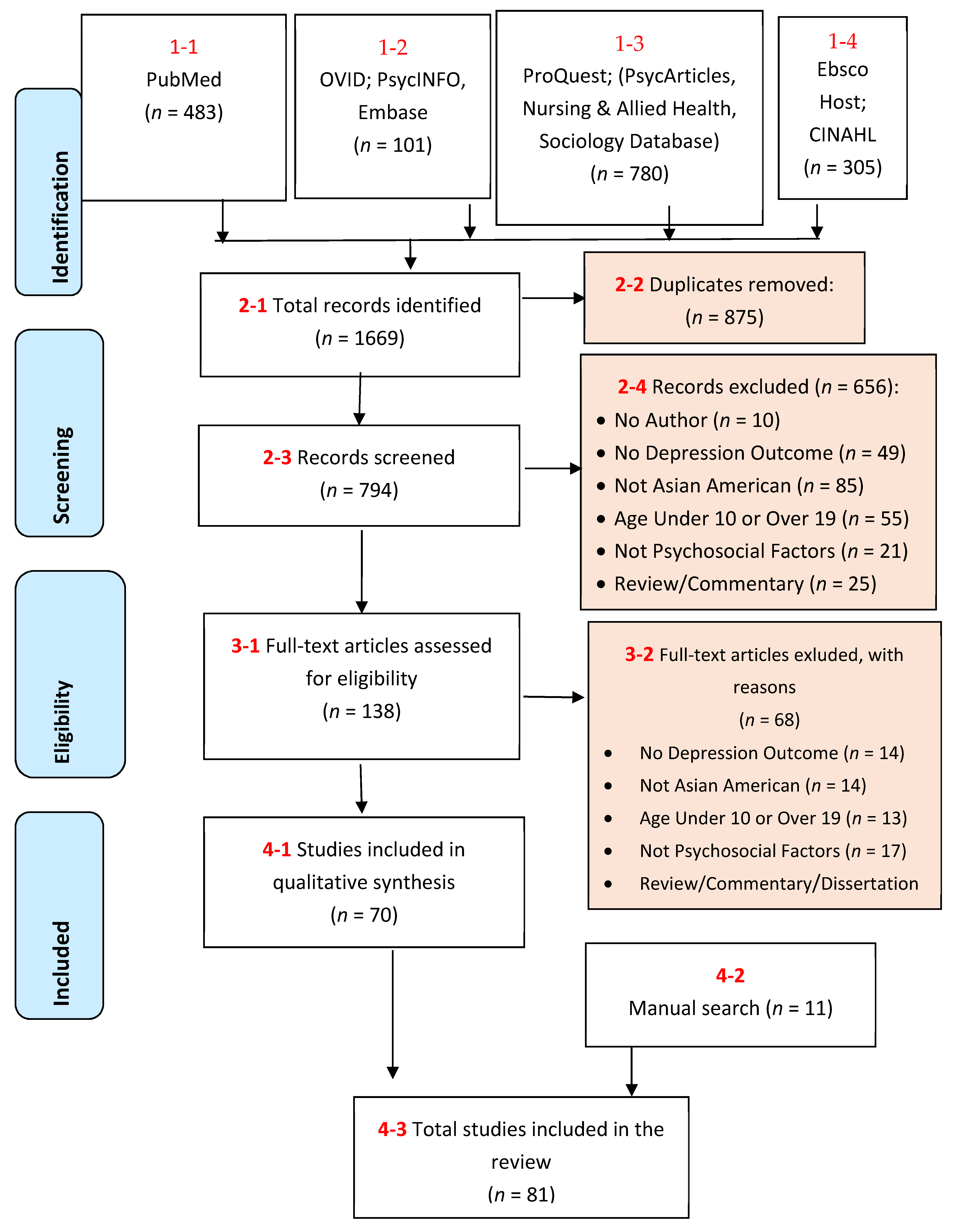
2.3. Search Strategy and Selection of Evidence
2.4. Quality Assessment
2.5. Data Extraction
2.6. Data Analysis and Synthesis of Results
3. Results
3.1. Characteristics of Included Studies
3.2. Individual Factors
3.2.1. Ascribed Indicators (Age, Gender, Immigration Status, Ethnicity)
3.2.2. Acculturation Factors (Acculturation, Generational Status, Coping Mechanism)
3.2.3. Psychological Indicators (Language Use, Academic Challenges, Religion, Diet/BMI)
3.3. Family Factors
3.3.1. Living Situation (Household Size, Socioeconomic Status)
3.3.2. Parent–Child Relations (Conflict; Affection/Cohesion; Parenting Style)
3.3.3. Parental Descriptors (Parental Language Use; Parental Psychological Factors)
3.4. Community and Social Factors
3.4.1. Racial/Ethnic Discrimination
3.4.2. Peer Relations
3.4.3. Broader Community Impact
4. Discussion
4.1. Summary of Findings
4.2. Individual Factors
4.3. Family Factors
4.4. Community and Social Factors
4.5. Integrative View
4.6. Limitations
4.7. Implications and Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wyatt, L.C.; Ung, T.; Park, R.; Kwon, S.C.; Trinh-Shevrin, C. Risk Factors of Suicide and Depression among Asian American, Native Hawaiian, and Pacific Islander Youth: A Systematic Literature Review. J. Health Care Poor Underserved. 2015, 26, 191–237. [Google Scholar] [CrossRef] [Green Version]
- The Johns Hopkins Hospital. Adolescent Depression. The Johns Hopkins Health System Corporation. 2021. Available online: https://www.hopkinsmedicine.org/psychiatry/specialty_areas/moods/adap/docs/adap-booklet_final.pdf (accessed on 26 April 2021).
- Logan, J.E.; Vagi, K.J.; Gorman-Smith, D. Characteristics of Youth with Combined Histories of Violent Behavior, Suicidal Ideation or Behavior, and Gun-Carrying. Crisis 2016, 37, 402–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, W. Adolescent Depression: National Trends, Risk Factors, and Healthcare Disparities. Am. J. Health Behav. 2019, 43, 181–194. [Google Scholar] [CrossRef]
- Garland, A.F.; Zigler, E.F. Psychological correlates of help-seeking attitudes among children and adolescents. Am. J. Orthopsychiatry 1994, 64, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Mojtabai, R.; Olfson, M.; Han, B. National Trends in the Prevalence and Treatment of Depression in Adolescents and Young Adults. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [Green Version]
- Avenevoli, S.; Swendsen, J.; He, J.P.; Burstein, M.; Merikangas, K.R. Major depression in the national comorbidity survey-adolescent supplement: Prevalence, correlates, and treatment. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 37–44.e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Census Bureau. ACS 5-Year Estimates Data Profiles. 2018. Available online: https://data.census.gov/cedsci/table?q=united%20states&g=0100000US&tid=ACSDP5Y2018.DP05&hidePreview=false (accessed on 20 December 2020).
- Statistics Canada. Census Profile, 2016 Census. 2016. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=PR&Code1=01&Geo2=PR&Code2=01&Data=Count&SearchText=canada&SearchType=Begins&SearchPR=01&B1=Ethnic%20origin&TABID=1 (accessed on 20 December 2020).
- U.S. Census Bureau. 2017 National Population Projections Tables: Main Series. United States Census Bureau. 2017. Available online: https://www.census.gov/data/tables/2017/demo/popproj/2017-summary-tables.html (accessed on 3 May 2021).
- Statistics Canada. A Portrait of Canadian Youth: March 2019 Updates. Statistics Canada. 2019. Available online: https://www150.statcan.gc.ca/n1/pub/11-631-x/11-631-x2019003-eng.htm#a1 (accessed on 3 May 2021).
- Statistics Canada. Visible Minority of Person; Statistics Canada: Ottawa, ON, Canada, 2021. Available online: https://www23.statcan.gc.ca/imdb/p3Var.pl?Function=DEC&Id=45152 (accessed on 3 May 2021).
- Esperat, M.C.; Inouye, J.; Gonzalez, E.W.; Owen, D.C.; Feng, D. Health disparities among Asian Americans and Pacific Islanders. Annu. Rev. Nurs. Res. 2004, 22, 135–159. [Google Scholar] [CrossRef]
- Kubik, M.Y.; Lytle, L.A.; Birnbaum, A.S.; Murray, D.M.; Perry, C.L. Prevalence and correlates of depressive symptoms in young adolescents. Am. J. Health Behav. 2003, 27, 546–553. [Google Scholar] [CrossRef]
- Gee, C.B. Assessment of anxiety and depression in Asian American youth. J. Clin. Child Adoles. Psychol. 2004, 33, 269–271. [Google Scholar] [CrossRef]
- Abright, A.R.; Chung, H. Depression in Asian American children. West. J. Med. 2002, 176, 244–248. [Google Scholar]
- Yuwen, W.; Chen, A.C. Chinese American adolescents: Perceived parenting styles and adolescents’ psychosocial health. Int. Nurs. Rev. 2013, 60, 236–243. [Google Scholar] [CrossRef]
- Stewart, S.M.; Simmons, A.; Habibpour, E. Treatment of culturally diverse children and adolescents with depression. J. Child Adolesc. Psychopharmacol. 2012, 22, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Finning, K.; Ukoumunne, O.C.; Ford, T.; Danielsson-Waters, E.; Shaw, L.; Romero De Jager, I.; Stentiford, L.; Moore, D.A. The association between child and adolescent depression and poor attendance at school: A systematic review and meta-analysis. J. Affect. Disord. 2019, 245, 928–938. [Google Scholar] [CrossRef]
- Priest, N.; Paradies, Y.; Trenerry, B.; Truong, M.; Karlsen, S.; Kelly, Y. A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Soc. Sci. Med. 2013, 95, 115–127. [Google Scholar] [CrossRef]
- Tessler, H.; Choi, M.; Kao, G. The Anxiety of Being Asian American: Hate Crimes and Negative Biases During the COVID-19 Pandemic. Am. J. Crim. Justice 2020, 45, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Cheah, C.S.L.; Wang, C.; Ren, H.; Zong, X.; Cho, H.S.; Xue, X. COVID-19 Racism and Mental Health in Chinese American Families. Pediatrics 2020, 146. [Google Scholar] [CrossRef] [PubMed]
- Scharpf, F.; Kaltenbach, E.; Nickerson, A.; Hecker, T. A systematic review of socio-ecological factors contributing to risk and protection of the mental health of refugee children and adolescents. Clin. Psychol. Rev. 2021, 83, 101930. [Google Scholar] [CrossRef] [PubMed]
- Zou, P. Facilitators and Barriers to Healthy Eating in Aged Chinese Canadians with Hypertension: A Qualitative Exploration. Nutrients 2019, 11, 111. [Google Scholar] [CrossRef] [Green Version]
- Krieger, N. Methods for the scientific study of discrimination and health: An ecosocial approach. Am. J. Public Health 2012, 102, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Hammarstrom, A.; Virtanen, P. The importance of financial recession for mental health among students: Short- and long-term analyses from an ecosocial perspective. J. Public Health Res. 2019, 8, 1504. [Google Scholar] [CrossRef] [Green Version]
- Jang, C.Y.; Cho, E.H.; Kwak, Y.S.; Kim, T. The Relationship between Flourishing and Depression in Children in the U.S. Using a Socioecological Perspective. Int. J. Environ. Res. Public Health 2020, 17, 8246. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Bisaga, K.; Whitaker, A.; Davies, M.; Chuang, S.; Feldman, J.; Walsh, B.T. Eating disorder and depressive symptoms in urban high school girls from different ethnic backgrounds. J. Dev. Behav. Pediatr. JDBP 2005, 26, 257–266. [Google Scholar] [CrossRef]
- Cardeli, E.; Phan, J.; Mulder, L.; Benson, M.; Adhikari, R.; Ellis, B.H. Bhutanese Refugee Youth: The Importance of Assessing and Addressing Psychosocial Needs in a School Setting. J. School Health 2020. [Google Scholar] [CrossRef]
- Cho, Y.B.; Haslam, N. Suicidal ideation and distress among immigrant adolescents: The role of acculturation, life stress, and social support. J. Youth Adolesc. 2010, 39, 370–379. [Google Scholar] [CrossRef]
- Choi, Y.; Tan, K.P.H.; Yasui, M.; Hahm, H.C. Advancing understanding of acculturation for adolescents of Asian immigrants: Person-oriented analysis of acculturation strategy among Korean American youth. J. Youth Adolesc. 2016, 45, 1380–1395. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Kim, T.Y.; Pekelnicky, D.D.; Kim, K.; Kim, Y.S. Impact of youth cultural orientation on perception of family process and development among Korean Americans. Cult. Divers. Ethn. Minor. Psychol. 2017, 23, 244–257. [Google Scholar] [CrossRef]
- Choi, Y.; Park, M.; Noh, S.; Lee, J.P.; Takeuchi, D. Asian American mental health: Longitudinal trend and explanatory factors among young Filipino- and Korean Americans. SSM—Popul. Health 2020, 10, 100542. [Google Scholar] [CrossRef]
- Choi, Y.; Tan, K.P.H.; Yasui, M.; Pekelnicky, D.D. Race-Ethnicity and Culture in the Family and Youth Outcomes: Test of a Path Model with Korean American Youth and Parents. Race Soc.Probl. 2014, 6, 69–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Critical Appraisal Skills Programme. CASP Checklists. 2017. Available online: http://www.casp-uk.net/casp-tools-checklists (accessed on 26 April 2021).
- Roley, M.E.; Kawakami, R.; Baker, J.; Hurtado, G.; Chin, A.; Hovey, J.D. Family Cohesion Moderates the Relationship between Acculturative Stress and Depression in Japanese Adolescent Temporary Residents. J. Immigr. Minor. Health 2014, 16, 1299–1302. [Google Scholar] [CrossRef]
- Weaver, S.R.; Kim, S.Y. A person-centered approach to studying the linkages among parent-child differences in cultural orientation, supportive parenting, and adolescent depressive symptoms in Chinese American families. J. Youth Adolesc. 2008, 37, 36–49. [Google Scholar] [CrossRef]
- Rivas-Drake, D.; Hughes, D.; Way, N. A Closer Look at Peer Discrimination, Ethnic Identity, and Psychological Well-being Among Urban Chinese American Sixth Graders. J. Youth Adolesc. 2008, 37, 12–21. [Google Scholar] [CrossRef]
- Wang, C.; Atwal, K. School climate, discrimination, and depressive symptoms among Asian American adolescents. Contemp. School Psychol. 2015, 19, 205–217. [Google Scholar] [CrossRef]
- Benner, A.D.; Kim, S.Y. Experiences of discrimination among Chinese American adolescents and the consequences for socioemotional and academic development. Dev. Psychol. 2009, 45, 1682–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, T.-F.; Han, E.-J.; Lee, J.-S.; Qin, D.B. Korean American adolescent ethnic-identity pride and psychological adjustment: Moderating effects of parental support and school environment. Asian Am. J. Psychol. 2015, 6, 190–199. [Google Scholar] [CrossRef]
- Chen, A.C.; Haas, S.; Gillmore, M.R.; Kopak, A. Trajectories of depressive symptoms from adolescence to young adulthood: Chinese Americans versus non-Hispanic whites. Res. Nurs. Health 2011, 34, 176–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.-Y. Violence Exposure and Its Relationship to Adolescents’ Internalizing Behaviors: A Comparison of African American and Asian American Youth. Soc. Coll. 2004, 65, 1538. [Google Scholar]
- Davis, R.F., III; Kiang, L. Religious Identity, Religious Participation, and Psychological Well-Being in Asian American Adolescents. J. Youth Adolesc. 2016, 45, 532–546. [Google Scholar] [CrossRef]
- Gartner, M.; Kiang, L.; Supple, A. Prospective links between ethnic socialization, ethnic and American identity, and well-being among Asian-American adolescents. J. Youth Adolesc. 2014, 43, 1715–1727. [Google Scholar] [CrossRef] [Green Version]
- Guerrero, A.P.S.; Hishinuma, E.S.; Andrade, N.N.; Nishimura, S.T.; Cunanan, V.L. Correlations among socioeconomic and family factors and academic, behavioral, and emotional difficulties in Filipino adolescents in Hawai’i. Int. J. Soc. Psychiatry 2006, 52, 343–359. [Google Scholar] [CrossRef]
- Juang, L.P.; Cookston, J.T. Acculturation, discrimination, and depressive symptoms among Chinese American adolescents: A longitudinal study. J. Prim. Prev. 2009, 30, 475–496. [Google Scholar] [CrossRef]
- Juang, L.P.; Syed, M.; Cookston, J.T. Acculturation-based and everyday parent-adolescent conflict among Chinese American adolescents: Longitudinal trajectories and implications for mental health. J. Fam. Psychol. 2012, 26, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Khuwaja, S.A.; Selwyn, B.J.; Kapadia, A.; McCurdy, S.; Alam, K. Pakistani Ismaili Muslim Adolescent Females Living in the United States of America: Stresses Associated with the Process of Adaptation to U.S. Culture. J. Immigr. Minor. Health 2007, 9, 35–42. [Google Scholar] [CrossRef]
- Kim, S.Y.; Ge, X. Parenting practices and adolescent depressive symptoms in Chinese American families. J. Fam. Psychol. 2000, 14, 420–435. [Google Scholar] [CrossRef]
- Kim, S.Y.; Wang, Y.; Deng, S.; Alvarez, R.; Li, J. Accent, perpetual foreigner stereotype, and perceived discrimination as indirect links between English proficiency and depressive symptoms in Chinese American adolescents. Dev. Psychol. 2011, 47, 289–301. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.L.; Benner, A.D.; Lau, A.S.; Kim, S.Y. Mother-adolescent language proficiency and adolescent academic and emotional adjustment among Chinese American families. J. Youth Adolesc. 2009, 38, 572–586. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.C.; Hopson, L.M.; Simpson, G.M.; Cheng, T.C. Racial/Ethnic Differences in Emotional Health: A Longitudinal Study of Immigrants’ Adolescent Children. Community Mental Health J. 2017, 53, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Niwa, E.Y.; Way, N.; Hughes, D.L. Trajectories of ethnic-racial discrimination among ethnically diverse early adolescents: Associations with psychological and social adjustment. Child Dev. 2014, 85, 2339–2354. [Google Scholar] [CrossRef] [PubMed]
- Park, W. Acculturative Stress and Mental Health Among Korean Adolescents in the United States. J. Hum. Behav. Soc. Environ. 2009, 19, 626–634. [Google Scholar] [CrossRef]
- Sangalang, C.C.; Jager, J.; Harachi, T.W. Effects of maternal traumatic distress on family functioning and child mental health: An examination of Southeast Asian refugee families in the U.S. Soc. Sci. Med. 2017, 184, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Song, S.J.; Ziegler, R.; Arsenault, L.; Fried, L.E.; Hacker, K. Asian Student Depression in American High Schools: Differences in Risk Factors. J. School Nurs. 2011, 27, 455–462. [Google Scholar] [CrossRef]
- Vaghela, P.; Ueno, K. Racial-ethnic identity pairings and mental health of second-generation Asian adolescents. Sociol. Perspect. 2017, 60, 834–852. [Google Scholar] [CrossRef]
- Willgerodt, M.A.; Thompson, E.A. Ethnic and generational influences on emotional distress and risk behaviors among Chinese and Filipino American adolescents. Res. Nurs. Health 2006, 29, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.L. Depression Level in Inner-City Asian American Adolescents: The Contributions of Cultural Orientation and Interpersonal Relationships. J. Hum. Behav. Soc. Environ. 2001, 3, 49–64. [Google Scholar] [CrossRef]
- Ying, Y.-W.; Han, M. The Effect of Intergenerational Conflict and School-Based Racial Discrimination on Depression and Academic Achievement in Filipino American Adolescents. J. Immigr. Refugee Stud. 2006, 4, 19–35. [Google Scholar] [CrossRef]
- Ying, Y.-W.; Han, M. Familism and mental health: Variation between Asian American children of refugees and immigrants. Int. J. Appl. Psychoanal. Stud. 2007, 4, 333–348. [Google Scholar] [CrossRef]
- Qin, D.B.; Rak, E.; Rana, M.; Donnellan, M.B. Parent-child relations and psychological adjustment among high-achieving Chinese and European American adolescents. J. Adolesc. 2012, 35, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Kiang, L.; Yip, T.; Gonzales-Backen, M.; Witkow, M.; Fuligni, A.J. Ethnic identity and the daily psychological well-being of adolescents from Mexican and Chinese backgrounds. Child Dev. 2006, 77, 1338–1350. [Google Scholar] [CrossRef]
- Kim, E.; Cain, K.C. Korean American adolescent depression and parenting. J. Child Adolesc. Psychiatr. Nurs. 2008, 21, 105–115. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.V. Perceptions of Vietnamese fathers’ acculturation levels, parenting styles, and mental health outcomes in Vietnamese American adolescent immigrants. Soc. Work 2008, 53, 337–346. [Google Scholar] [CrossRef]
- Tsai, W.; Nguyen, D.; Weiss, B.; Ngo, V.; Lau, A.; Nguyen, D.J.; Lau, A.S. Cultural Differences in the Reciprocal Relations between Emotion Suppression Coping, Depressive Symptoms and Interpersonal Functioning among Adolescents. J. Abnorm. Child Psychol. 2017, 45, 657–669. [Google Scholar] [CrossRef] [PubMed]
- DuongTran, P. Coping Resources among Southeast Asian-American Adolescents. J. Hum. Behav. Soc. Environ. 2011, 21, 196. [Google Scholar] [CrossRef]
- Huntsinger, C.S.; Jose, P.E. A longitudinal investigation of personality and social adjustment among Chinese American and European American adolescents. Child Dev. 2006, 77, 1309–1324. [Google Scholar] [CrossRef] [PubMed]
- Park, I.J.; Kim, P.Y.; Cheung, R.Y.; Kim, M. The role of culture, family processes, and anger regulation in Korean American adolescents’ adjustment problems. Am. J. Orthopsychiatry 2010, 80, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, W.; Weiss, B.; Kim, J.H.J.; Lau, A.S. Longitudinal Relations between Emotion Restraint Values, Life Stress, and Internalizing Symptoms among Vietnamese American and European American Adolescents. J. Clin. Child Adolesc. Psychol. 2019, 1–13. [Google Scholar] [CrossRef]
- Willgerodt, M.A.; Thompson, E.A. The influence of ethnicity and generational status on parent and family relations among Chinese and Filipino adolescents. Public Health Nurs. 2005, 22, 460–471. [Google Scholar] [CrossRef]
- Fang, L.; Schinke, S.P. Alcohol use among Asian American adolescent girls: The impact of immigrant generation status and family relationships. J. Ethn. Subst. Abuse 2011, 10, 275–294. [Google Scholar] [CrossRef] [PubMed]
- Kang, P.P.; Romo, L.F. The role of religious involvement on depression, risky behavior, and academic performance among Korean American adolescents. J. Adolesc. 2011, 34, 767–778. [Google Scholar] [CrossRef]
- Mistry, R.S.; Benner, A.D.; Tan, C.S.; Kim, S.Y. Family economic stress and academic well-being among Chinese-American youth: The influence of adolescents’ perceptions of economic strain. J. Fam. Psychol. 2009, 23, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Kiang, L.; Witkow, M.R. Normative changes in meaning in life and links to adjustment in adolescents from Asian American backgrounds. Asian Am. J. Psychol. 2015, 6, 164–173. [Google Scholar] [CrossRef]
- Arat, G. Emerging protective and risk factors of mental health in Asian American students: Findings from the 2013 Youth Risk Behavior Survey. Vulnerable Child. Youth Stud. 2015, 10, 192. [Google Scholar] [CrossRef]
- Lanza, H.I.; Echols, L.; Graham, S. Deviating from the norm: Body mass index (BMI) differences and psychosocial adjustment among early adolescent girls. J. Pediatr. Psychol. 2013, 38, 376–386. [Google Scholar] [CrossRef] [Green Version]
- Crane, D.R.; So Wa, N.; Larson, J.H.; Hafen, M., Jr. The Influence of Family Functioning and Parent-Adolescent Acculturation on North American Chinese Adolescent Outcomes. Fam. Relat. 2005, 54, 400–410. [Google Scholar] [CrossRef]
- DiBlasi, T.; Shin, J.Y.; Dill, C.A. Bullying and Discrimination Experiences among Korean-American Junior High School Students. Rom. J. Appl. Psychol. 2018, 20, 28–36. [Google Scholar] [CrossRef]
- Hou, Y.; Kim, S.; Wang, Y. Parental Acculturative Stressors and Adolescent Adjustment Through Interparental and Parent-Child Relationships in Chinese American Families. J. Youth Adolesc. 2016, 45, 1466–1481. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Kim, S.Y.; Hazen, N.; Benner, A.D. Parents’ Perceived Discrimination and Adolescent Adjustment in Chinese American Families: Mediating Family Processes. Child Dev. 2017, 88, 317–331. [Google Scholar] [CrossRef]
- Hwang, W.C.; Wood, J.J.; Fujimoto, K. Acculturative family distancing (AFD) and depression in Chinese American families. J. Consult. Clin. Psychol. 2010, 78, 655–667. [Google Scholar] [CrossRef] [PubMed]
- Juang, L.P.; Syed, M.; Takagi, M. Intergenerational discrepancies of parental control among Chinese American families: Links to family conflict and adolescent depressive symptoms. J. Adolesc. 2007, 30, 965–975. [Google Scholar] [CrossRef]
- Kim, S.Y.; Chen, Q.; Li, J.; Huang, X.; Moon, U.J. Parent-child acculturation, parenting, and adolescent depressive symptoms in Chinese immigrant families. J. Fam. Psychol. 2009, 23, 426–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, B.T. Self-Construal and Depression among Vietnamese-American Adolescents. Int. J. Intercult. Relat. 2005, 29, 239–250. [Google Scholar] [CrossRef]
- Park, W. Parental Attachment Among Korean-American Adolescents. Child Adolesc. Soc. Work J. 2009, 26, 307–319. [Google Scholar] [CrossRef]
- Shen, Y.; Kim, S.Y.; Benner, A.D. Burdened or Efficacious? Subgroups of Chinese American Language Brokers, Predictors, and Long-Term Outcomes. J. Youth Adolesc. 2019, 48, 154–169. [Google Scholar] [CrossRef] [PubMed]
- Supple, A.J.; Cavanaugh, A.M. Tiger mothering and Hmong American parent–adolescent relationships. Asian Am. J. Psychol. 2013, 4, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Yasui, M.; Kim, T.Y.; Choi, Y. Culturally Specific Parent Mental Distress, Parent-Child Relations and Youth Depression among Korean American Families. J. Child Fam. Stud. 2018, 27, 3371–3384. [Google Scholar] [CrossRef]
- Ying, Y.W.; Han, M. The longitudinal effect of intergenerational gap in acculturation on conflict and mental health in Southeast Asian American adolescents. Am. J. Orthopsychiatry 2007, 77, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.-W.; Han, M. Parental Acculturation, Parental Involvement, Intergenerational Relationship and Adolescent Outcomes in Immigrant Filipino American Families. J. Immigr. Refugee Stud. 2008, 6, 112–131. [Google Scholar] [CrossRef]
- Ying, Y.-W.; Han, M. Parental contributions to Southeast Asian American adolescents’ well-being. Youth Soc. 2008, 40, 289–306. [Google Scholar] [CrossRef]
- Guan, S.-S.A.; Fuligni, A.J. Changes in Parent, Sibling, and Peer Support During the Transition to Young Adulthood. J. Res. Adolesc. 2016, 26, 286–299. [Google Scholar] [CrossRef]
- Juang, L.P.; Cookston, J.T. A longitudinal study of family obligation and depressive symptoms among Chinese American adolescents. J. Fam. Psychol. 2009, 23, 396–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiang, L.; Bhattacharjee, K. Developmental Change and Correlates of Autonomy in Asian American Adolescents. J. Youth Adolesc. 2019, 48, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Chen, Q.; Wang, Y.; Shen, Y.; Orozco-Lapray, D. Longitudinal linkages among parent-child acculturation discrepancy, parenting, parent-child sense of alienation, and adolescent adjustment in Chinese immigrant families. Dev. Psychol. 2013, 49, 900–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Wang, Y.; Orozco-Lapray, D.; Shen, Y.; Murtuza, M. Does “Tiger Parenting” Exist? Parenting Profiles of Chinese Americans and Adolescent Developmental Outcomes. Asian Am. J. Psychol. 2013, 4, 7–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, P.V. East Meets West: Acculturation Levels, Parenting Styles, and Mental Health Outcomes of Vietnamese American Adolescents Immigrants. Soc. Coll. 2005, 66, 1166. [Google Scholar]
- Schires, S.M.; Buchanan, N.T.; Lee, R.M.; McGue, M.; Iacono, W.G.; Burt, S.A. Discrimination and Ethnic-Racial Socialization Among Youth Adopted From South Korea Into White American Families. Child Dev. 2020, 91, e42–e58. [Google Scholar] [CrossRef] [PubMed]
- Arora, P.G.; Fisher, S.; Wheeler, L.A.; Barnes, J.; Arora, P.G. A prospective examination of anxiety as a predictor of depressive symptoms among Asian American early adolescent youth: The role of parent, peer, and teacher support and school engagement. Cult. Divers. Ethn. Minor. Psychol. 2017, 23, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Yasui, M.; Dishion, T.J. The Ethnic Context of Child and Adolescent Problem Behavior: Implications for Child and Family Interventions. Clin. Child Fam. Psychol. Rev. 2007, 10, 137–179. [Google Scholar] [CrossRef]
- Grossman, J.M.; Liang, B. Discrimination Distress among Chinese American Adolescents. J. Youth Adolesc. 2008, 37, 1–11. [Google Scholar] [CrossRef]
- Hou, Y.; Kim, S.; Wang, Y.; Shen, Y.; Orozco-Lapray, D. Longitudinal Reciprocal Relationships Between Discrimination and Ethnic Affect or Depressive Symptoms Among Chinese American Adolescents. J. Youth Adolesc. 2015, 44, 2110–2121. [Google Scholar] [CrossRef] [Green Version]
- Huynh, V.W. Ethnic microaggressions and the depressive and somatic symptoms of Latino and Asian American adolescents. J. Youth Adolesc. 2012, 41, 831–846. [Google Scholar] [CrossRef]
- Huynh, V.W.; Fuligni, A.J. Discrimination Hurts: The Academic, Psychological, and Physical Well-Being of Adolescents. J. Res. Adolesc. 2010, 20, 916–941. [Google Scholar] [CrossRef]
- Mali, L.V.; Schwartz, D.; Badaly, D.; Luo, T.J.; Malamut, S.; Ross, A.C.; Duong, M.T. Unpopularity with same- and cross-ethnicity peers as predictors of depressive symptoms during adolescence. J. Appl. Dev. Psychol. 2019, 62, 93. [Google Scholar] [CrossRef]
- Shin, J.Y.; D’Antonio, E.; Son, H.; Kim, S.A.; Park, Y. Bullying and discrimination experiences among Korean-American adolescents. J. Adolesc. 2011, 34, 873–883. [Google Scholar] [CrossRef] [PubMed]
- Teja, Z.; Schonert-Reichl, K.A. Peer Relations of Chinese Adolescent Newcomers: Relations of Peer Group Integration and Friendship Quality to Psychological and School Adjustment. J. Int. Migr. Integr. 2013, 14, 535–556. [Google Scholar] [CrossRef]
- Haddad, E.; Chen, C.; Greenberger, E. The role of important non-parental adults (VIPs) in the lives of older adolescents: A comparison of three ethnic groups. J. Youth Adolesc. 2011, 40, 310–319. [Google Scholar] [CrossRef] [Green Version]
- Lam, B.T.; Chen, C.; Greenberger, E. The Important Roles of Non-Parental Adults in Vietnamese-American Adolescents’ Cultural and Socioemotional Development. Soc. Work Mental Health 2012, 10, 343–366. [Google Scholar] [CrossRef]
- Ozer, E.J.; McDonald, K.L. Exposure to violence and mental health among Chinese American urban adolescents. J. Adolesc. Health 2006, 39, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G. Research on religion, spirituality, and mental health: A review. Can. J. Psychiatry 2009, 54, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Leu, J.; Walton, E.; Takeuchi, D. Contextualizing acculturation: Gender, family, and community reception influences on Asian immigrant mental health. Am. J. Community Psychol. 2011, 48, 168–180. [Google Scholar] [CrossRef]
- Tang, X.; Tang, S.; Ren, Z.; Wong, D.F.K. Psychosocial risk factors associated with depressive symptoms among adolescents in secondary schools in mainland china: A systematic review and meta-analysis. J. Affect. Disord. 2020, 263, 155–165. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, Z. Chinese high school students’ academic stress and depressive symptoms: Gender and school climate as moderators. Stress Health 2012, 28, 340–346. [Google Scholar] [CrossRef]
- Gorostiaga, A.; Aliri, J.; Balluerka, N.; Lameirinhas, J. Parenting Styles and Internalizing Symptoms in Adolescence: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 3192. [Google Scholar] [CrossRef] [Green Version]
- Herman, K.C.; Ostrander, R.; Tucker, C.M. Do family environments and negative cognitions of adolescents with depressive symptoms vary by ethnic group? J. Fam. Psychol. 2007, 21, 325–330. [Google Scholar] [CrossRef]
- Li, W.; Meng, X.; Xu, Z.; Yu, Q.; Shi, J.; Yu, Y.; D’Arcy, C.; Huang, Y.; Kou, C. Prevalence, correlates of major depression: A mental health survey among undergraduates at a mainland Chinese university. Asia Pac. Psychiatry 2016, 8, 206–214. [Google Scholar] [CrossRef]
- Ho, G.W. Acculturation and its implications on parenting for Chinese immigrants: A systematic review. J. Transcult. Nurs. 2014, 25, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Gariepy, G.; Honkaniemi, H.; Quesnel-Vallee, A. Social support and protection from depression: Systematic review of current findings in Western countries. Br. J. Psychiatry 2016, 209, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Stirling, K.; Toumbourou, J.W.; Rowland, B. Community factors influencing child and adolescent depression: A systematic review and meta-analysis. Aust. N. Z. J. Psychiatry 2015, 49, 869–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, P.A.; Porche, M.V.; Shippen, N.A.; Dallenbach, N.T.; Fortuna, L.R. Which girls, which boys? The intersectional risk for depression by race and ethnicity, and gender in the U.S. Clin. Psychol. Rev. 2018, 66, 51–68. [Google Scholar] [CrossRef]
- Karanikola, M.N.K.; Lyberg, A.; Holm, A.L.; Severinsson, E. The Association between Deliberate Self-Harm and School Bullying Victimization and the Mediating Effect of Depressive Symptoms and Self-Stigma: A Systematic Review. Biomed. Res. Int. 2018, 2018, 4745791. [Google Scholar] [CrossRef] [Green Version]
- Joung, K.H.; Saewyc, E.M. Factors related to heavy drinking between British Columbia Asian adolescents and South Korean adolescents. J. Spec. Pediatr. Nurs. 2020, 25, e12296. [Google Scholar] [CrossRef]
- Sieger, K.; Rojas-Vilches, A.; McKinney, C.; Renk, K. The effects and treatment of community violence in children and adolescents: What should be done? Trauma Violence Abuse 2004, 5, 243–259. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Le, P.D.; Goldmann, E.; Yang, L.H. Psychological impact of anti-Asian stigma due to the COVID-19 pandemic: A call for research, practice, and policy responses. Psychol. Trauma 2020, 12, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Adia, A.C.; Nazareno, J.; Operario, D.; Ponce, N.A. Health Conditions, Outcomes, and Service Access Among Filipino, Vietnamese, Chinese, Japanese, and Korean Adults in California, 2011-2017. Am. J. Public Health 2020, 110, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Shreffler, J.; Petrey, J.; Huecker, M. The Impact of COVID-19 on Healthcare Worker Wellness: A Scoping Review. West. J. Emerg. Med. 2020, 21, 1059–1066. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, P.; Siu, A.; Wang, X.; Shao, J.; Hallowell, S.G.; Yang, L.L.; Zhang, H. Influencing Factors of Depression among Adolescent Asians in North America: A Systematic Review. Healthcare 2021, 9, 537. https://doi.org/10.3390/healthcare9050537
Zou P, Siu A, Wang X, Shao J, Hallowell SG, Yang LL, Zhang H. Influencing Factors of Depression among Adolescent Asians in North America: A Systematic Review. Healthcare. 2021; 9(5):537. https://doi.org/10.3390/healthcare9050537
Chicago/Turabian StyleZou, Ping, Annisa Siu, Xiyi Wang, Jing Shao, Sunny G. Hallowell, Lihua Lydia Yang, and Hui Zhang. 2021. "Influencing Factors of Depression among Adolescent Asians in North America: A Systematic Review" Healthcare 9, no. 5: 537. https://doi.org/10.3390/healthcare9050537
APA StyleZou, P., Siu, A., Wang, X., Shao, J., Hallowell, S. G., Yang, L. L., & Zhang, H. (2021). Influencing Factors of Depression among Adolescent Asians in North America: A Systematic Review. Healthcare, 9(5), 537. https://doi.org/10.3390/healthcare9050537