
Rota-Lithotripsy as a Novel Bail-Out Strategy for Highly Calcified Coronary Lesions in Acute Coronary Syndrome

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
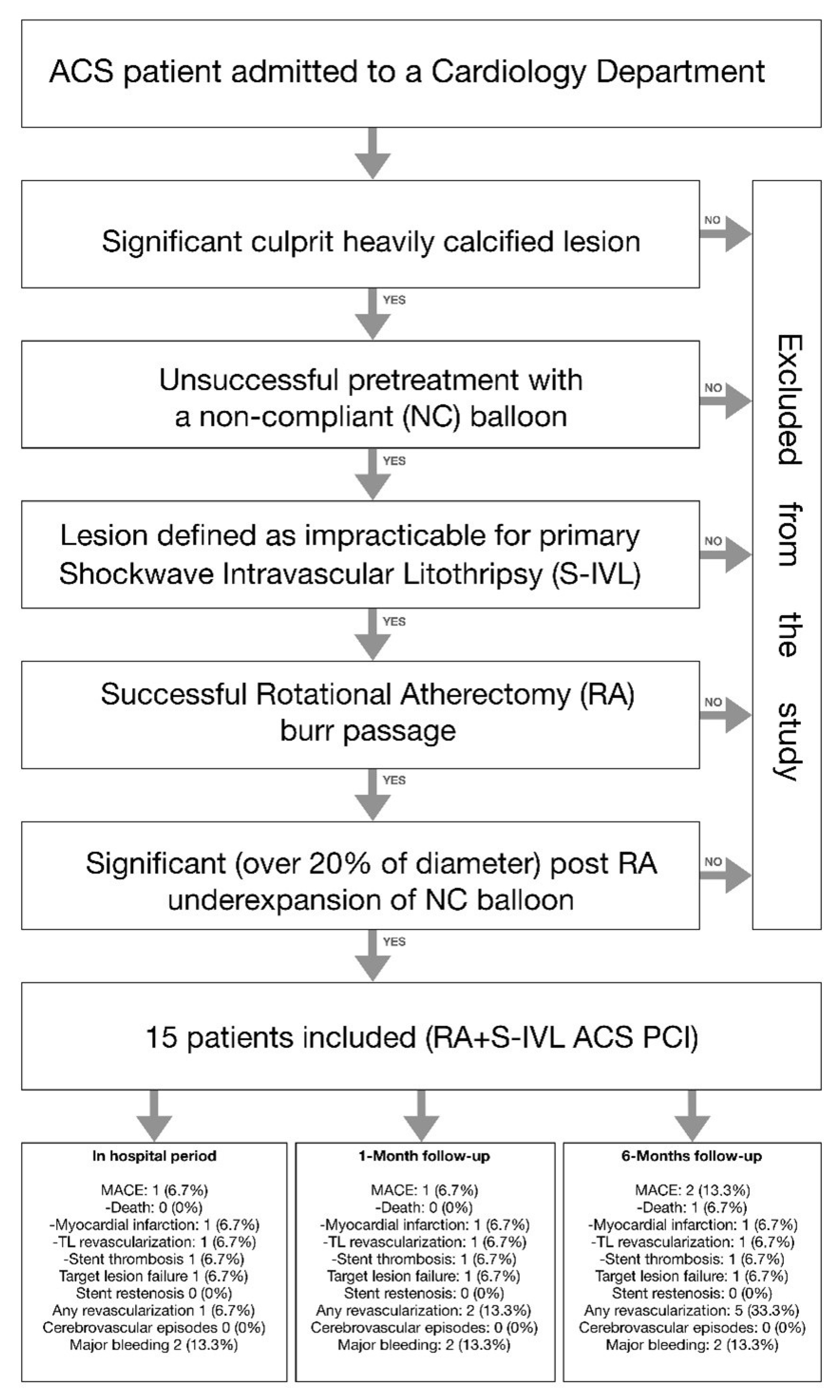
2.1. Study Population
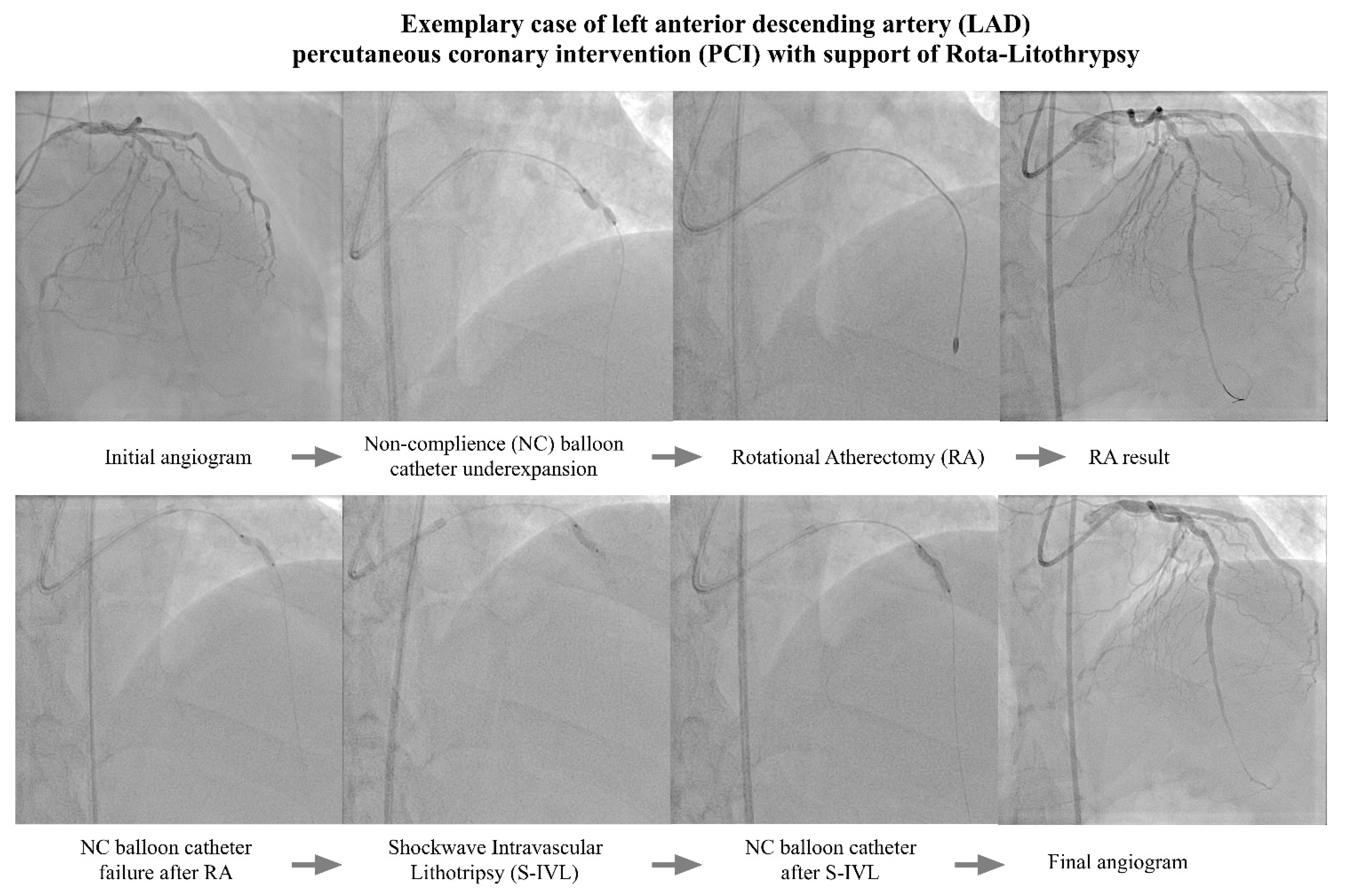
2.2. PCI Procedures
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Madhavan, M.V.; Tarigopula, M.; Mintz, G.S.; Maehara, A.; Stone, G.W.; Généreux, P. Coronary artery calcification: Pathogenesis and prognostic implications. J. Am. Coll. Cardiol. J. Am. Coll. Cardiol. 2014, 63, 1703–1714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassimis, G.; Raina, T.; Kontogiannis, N.; Patri, G.; Abramik, J.; Zaphiriou, A.; Banning, A. How Should We Treat Heavily Calcified Coronary Artery Disease in Contemporary Practice? From Atherectomy to Intravascular Lithotripsy. Revasc. Med. 2019, 20, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.M.; Tong, D.; Mintz, G.S.; Mamas, M.; Javed, A. Breaking the deadlock of calcified coronary artery lesions: A contemporary review. Catheter. Cardiovasc. Interv. 2021, 97, 108–120. [Google Scholar] [CrossRef] [PubMed]
- Rozenbaum, Z.; Takahashi, T.; Kobayashi, Y.; Bliagos, D.; Menegus, M.; Colombo, A.; Latib, A. Contemporary technologies to modify calcified plaque in coronary artery disease. Prog. Cardiovasc. Dis. 2021, 69, 18–26. [Google Scholar] [CrossRef]
- Brinton, T.J.; Ali, Z.A.; Hill, J.M.; Meredith, I.T.; Maehara, A.; Illindala, U.; Lansky, A.; Götberg, M.; Van Mieghem, N.M.; Whitbourn, R.; et al. Feasibility of Shockwave Coronary Intravascular Lithotripsy for the Treatment of Calcified Coronary Stenoses. Circulation 2019, 139, 834–836. [Google Scholar] [CrossRef]
- Rola, P.; Włodarczak, A.; Kulczycki, J.J.; Barycki, M.; Furtan, Ł.; Szudrowicz, M.; Jastrzębski, A.; Pęcherzewski, M.; Doroszko, A.; Lesiak, M. Feasibility of the intravascular lithotripsy in coronary artery disease. Short-term outcomes of the Lower-Silesia Shockwave Registry. Kardiol. Pol. 2021, 79, 1133–1135. [Google Scholar] [CrossRef] [PubMed]
- Włodarczak, A.; Rola, P.; Barycki, M.; Kulczycki, J.; Szudrowicz, M.; Lesiak, M.; Doroszko, A. Rota-Lithotripsy—A Novel Bail-Out Strategy for Calcified Coronary Lesions in Acute Coronary Syndrome. The First-in-Man Experience. J. Clin. Med. 2021, 10, 1872. [Google Scholar] [CrossRef]
- Gonzálvez-García, A.; Jiménez-Valero, S.; Galeote, G.; Moreno, R.; de Sá, E.L.; Jurado-Román, A. “RotaTripsy”: Combination of Rotational Atherectomy and Intravascular Lithotripsy in Heavily Calcified Coronary Lesions: A Case Series. Cardiovasc. Revasc. Med. 2022, 35, 179–184. [Google Scholar] [CrossRef]
- Buono, A.; Basavarajaiah, S.; Choudhury, A.; Lee, L.; Bhatia, G.; Hailan, A.; Sharma, V.; Upadhyaya, S.; Naneishvili, T.; Ielasi, A. “RotaTripsy” for Severe Calcified Coronary Artery Lesions: Insights From a Real-World Multicenter Cohort. Cardiovasc. Revasc. Med. 2022, 37, 78–81. [Google Scholar] [CrossRef]
- Aznaouridis, K.; Bonou, M.; Masoura, C.; Kapelios, C.; Tousoulis, D.; Barbetseas, J. Rotatripsy: A Hybrid “Drill and Disrupt” Approach for Treating Heavily Calcified Coronary Lesions. J. Invasive Cardiol. 2020, 32, E175. [Google Scholar]
- Włodarczak, A.; Kulczycki, J.; Furtan, Ł.; Rola, P.; Barycki, M.; Łanocha, M.; Szudrowicz, M.; Lesiak, M. Rotational atherectomy and intravascular lithotripsy: Two methods versus a single lesion. Kardiol. Pol. 2021, 79, 712–713. [Google Scholar] [CrossRef] [PubMed]
- Jurado-Román, A.; Gonzálvez, A.; Galeote, G.; Jiménez-Valero, S.; Moreno, R. RotaTripsy: Combination of Rotational Atherectomy and Intravascular Lithotripsy for the Treatment of Severely Calcified Lesions. JACC Cardiovasc. Interv. 2019, 12, e127–e129. [Google Scholar] [CrossRef] [PubMed]
- Rola, P.; Włodarczak, A.; Barycki, M.; Kulczycki, J.J.; Engel, B.; Doroszko, A. “All hands on deck”—Rota-lithotripsy—A combination of rotational atherectomy and intravascular lithotripsy (shockwave) with additional use of a Turnpike Gold microcatheter and guide extension as a novel approach for calcified lesions. Postep. Kardiol. Interwencyjnej 2021, 17, 214–217. [Google Scholar] [CrossRef]
- Ielasi, A.; Loffi, M.; De Blasio, G.; Tespili, M. “Rota-Tripsy”: A Successful Combined Approach for the Treatment of a Long and Heavily Calcified Coronary Lesion. Cardiovasc. Revasc. Med. 2020, 21, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Giacchi, G.; Contarini, M.; Ruscica, G.; Brugaletta, S. The “RotaTripsy Plus” Approach in a Heavily Calcified Coronary Stenosis. Cardiovasc. Revasc. Med. 2021, 28, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Włodarczak, A.; Rola, P.; Barycki, M.; Engel, B.; Szudrowicz, M.; Kulczycki, J.J.; Lesiak, M.; Doroszko, A. Rota-lithotripsy: A combination of rotational atherectomy and intravascular lithotripsy (Shockwaves) as a novel strategy for a rotablation-resistant lesion in a patient with ST-segment elevation myocardial infarction. Cardiol. J. 2021, 28, 993–994. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF). Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction. J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- Garcia-Garcia, H.M.; McFadden, E.P.; Farb, A.; Mehran, R.; Stone, G.W.; Spertus, J.; Onuma, Y.; Morel, M.-A.; Van Es, G.-A.; Zuckerman, B.; et al. Standardized end point definitions for coronary intervention trials: The academic research consortium-2 consensus document. Circulation 2018, 137, 2635–2650. [Google Scholar] [CrossRef]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [Green Version]
- Perfetti, M.; Fulgenzi, F.; Radico, F.; Toro, A.; Procopio, A.; Maddestra, N.; Zimarino, M. Calcific lesion preparation for coronary bifurcation stenting. Cardiol. J. 2019, 26, 429–437. [Google Scholar] [CrossRef] [Green Version]
- Doost, A.; Rankin, J.; Sapontis, J.; Ko, B.; Lo, S.; Jaltotage, B.; Dwivedi, G.; Wood, D.; Byrne, J.; Sathananthan, J.; et al. Contemporary Evidence-Based Diagnosis and Management of Severe Coronary Artery Calcification. Heart Lung Circ. 2022, 31, 766–778. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Pathogenesis and Clinical Significance of In-Stent Restenosis in Patients with Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef] [PubMed]
- Henein, M.Y.; Vancheri, S.; Bajraktari, G.; Vancheri, F. Coronary Atherosclerosis Imaging. Diagnostics 2020, 10, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorini Dini, C.; Nardi, G.; Ristalli, F.; Mattesini, A.; Hamiti, B.; Di Mario, C. Contemporary Approach to Heavily Calcified Coronary Lesions. Interv. Cardiol. 2019, 14, 154–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sielski, J.; Kaziród-Wolski, K.; Siudak, Z. Risk of perioperative death and sudden cardiac arrest: A study of 113 456 cases from the National Registry of Invasive Cardiology Procedures (ORPKI) for estimation of the perioperative prognosis. Kardiol. Pol. 2021, 79, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Qaqish, O.; Sharma, S.; Kumar, A.; Patel, K.; Mohammed, K.; Venigalla, P.; Ojha, A.; Sareen, N.; Goddla, V.; Dabaja, A.; et al. Rotational Atherectomy in Acute Coronary Syndrome: A Meta-Analysis. Cardiovasc. Revasc. Med. 2022, 42, 143–153. [Google Scholar] [CrossRef]
- Kübler, P.; Zimoch, W.; Kosowski, M.; Tomasiewicz, B.; Telichowski, A.; Reczuch, K. Acute coronary syndrome—Still a valid contraindication to perform rotational atherectomy? Early and one-year outcomes. J. Cardiol. 2018, 71, 382–388. [Google Scholar] [CrossRef] [Green Version]
- Cosgrove, C.S.; Wilson, S.J.; Bogle, R.; Hanratty, C.G.; Williams, R.; Walsh, S.J.; McEntegart, M.; Spratt, J.C. Intravascular lithotripsy for lesion preparation in patients with calcific distal left main disease. EuroIntervention 2020, 16, 76–79. [Google Scholar] [CrossRef]
- Sinclair, H.; Fan, L.; Fahy, E.; Shahid, F.; Ratib, K.; Nolan, J.; Mamas, M.; Zaman, A.; Ahmed, J. Intravascular imaging-guided intracoronary lithotripsy: First real-world experience. Health Sci. Rep. 2021, 4, e307. [Google Scholar] [CrossRef]
- Rola, P.; Włodarczak, A.; Kulczycki, J.J.; Barycki, M.; Furtan, Ł.; Pęcherzewski, M.; Szudrowicz, M.; Włodarczak, S.; Doroszko, A.; Lesiak, M. Efficacy and safety of shockwave intravascular lithotripsy (S-IVL) in calcified unprotected left main percutaneous coronary intervention—Short-term outcomes. Postep. Kardiol. Interwencyjnej. 2021, 17, 344–348. [Google Scholar] [CrossRef]
- Wong, J.J.; Umapathy, S.; Keh, Y.S.; Lau, Y.H.; Yap, J.; Idu, M.; Chin, C.Y.; Fam, J.M.; Liew, B.W.; Chin, C.T.; et al. Coronary Intravascular Lithotripsy Versus Rotational Atherectomy in an Asian Population: Clinical Outcomes in Real-World Patients. Korean Circ. J. 2022, 52, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Rola, P.; Włodarczak, A.; Jastrzębski, A.; Barycki, M.; Turkiewicz, K.; Kulczycki, J.J.; Szudrowicz, M.; Pęcherzewski, M.; Doroszko, A.; Lesiak, M. Impella protected percutaneous coronary intervention on the last remaining highly calcified coronary artery facilitated by shockwave intravascular lithotripsy and levosimendan infusion. Kardiol. Pol. 2021, 79, 1145–1146. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Gordin, J.S.; Stone, G.W.; Sharma, S.K.; Saito, S.; Mahmud, E.; Chambers, J.; Généreux, P.; Shlofmitz, R. Orbital and rotational atherectomy during percutaneous coronary intervention for coronary artery calcification. Catheter. Cardiovasc. Interv. 2018, 92, 61–67. [Google Scholar] [CrossRef]
- Sharma, S.K.; Tomey, M.I.; Teirstein, P.S.; Kini, A.S.; Reitman, A.B.; Lee, A.C.; Généreux, P.; Chambers, J.W.; Grines, C.L.; Himmelstein, S.I.; et al. North American Expert Review of Rotational Atherectomy. Circ. Cardiovasc. Interv. 2019, 12, e007448. [Google Scholar] [CrossRef] [PubMed]
- Rola, P.; Włodarczak, A.; Barycki, M.; Doroszko, A. Use of the Shock Wave Therapy in Basic Research and Clinical Applications-From Bench to Bedsite. Biomedicines 2022, 10, 568. [Google Scholar] [CrossRef]
- Gardiner, R.; Muradagha, H.; Kiernan, T.J. Intravascular lithotripsy during percutaneous coronary intervention: Current concepts. Expert Rev. Cardiovasc. Ther. 2022, 20, 323–338. [Google Scholar] [CrossRef]
- Wańha, W.; Tomaniak, M.; Wańczura, P.; Bil, J.; Januszek, R.; Wolny, R.; Opolski, M.P.; Kuźma, Ł.; Janas, A.; Figatowski, T.; et al. Intravascular Lithotripsy for the Treatment of Stent Underexpansion: The Multicenter IVL-DRAGON Registry. J. Clin. Med. 2022, 11, 1779. [Google Scholar] [CrossRef]
- McLaughlin, T.J.; Sachdeva, R.; Kumar, G. First United States Experience With Rota-Shock: A Case Series. Cardiovasc. Revasc. Med. 2022, 40, 209–213. [Google Scholar] [CrossRef]
- Sakakura, K.; Ito, Y.; Shibata, Y.; Okamura, A.; Kashima, Y.; Nakamura, S.; Hamazaki, Y.; Ako, J.; Yokoi, H.; Kobayashi, Y.; et al. Clinical expert consensus document on rotational atherectomy from the Japanese association of cardiovascular intervention and therapeutics. Cardiovasc. Interv. Ther. 2021, 36, 1–18. [Google Scholar] [CrossRef]
- Barbato, E.; Carrié, D.; Dardas, P.; Fajadet, J.; Gaul, G.; Haude, M.; Khashaba, A.; Koch, K.; Meyer-Gessner, M.; Palazuelos, J.; et al. European expert consensus on rotational atherectomy. EuroIntervention 2015, 11, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Bajraktari, G.; Rexhaj, Z.; Elezi, S.; Zhubi-Bakija, F.; Bajraktari, A.; Bytyçi, I.; Batalli, A.; Henein, M.Y. Radial Access for Coronary Angiography Carries Fewer Complications Compared with Femoral Access: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 2163. [Google Scholar] [CrossRef] [PubMed]
- Wańha, W.; Januszek, R.; Kołodziejczak, M.; Kuźma, Ł.; Tajstra, M.; Figatowski, T.; Smolarek-Nicpoń, M.; Gruz-Kwapisz, M.; Tomasiewicz, B.; Bartuś, J.; et al. Procedural and 1-year outcomes following large vessel coronary artery perforation treated by covered stents implantation: Multicentre CRACK registry. PLoS ONE 2021, 16, e0249698. [Google Scholar] [CrossRef]
- Nowak, A.; Ratajczak, J.; Kasprzak, M.; Sukiennik, A.; Fabiszak, T.; Wojakowski, W.; Ochała, A.; Wańha, W.; Kuczmik, W.; Navarese, E.P.; et al. Long-term outcome of rotational atherectomy according to burr-to-artery ratio and changes in coronary artery blood flow: Observational analysis. Cardiol. J. 2021. [Google Scholar] [CrossRef]
- Roczniak, J.; Koziołek, W.; Piechocki, M.; Tokarek, T.; Surdacki, A.; Bartuś, S.; Chyrchel, M. Comparison of Access Site-Related Complications and Quality of Life in Patients after Invasive Cardiology Procedures According to the Use of Radial, Femoral, or Brachial Approach. Int. J. Environ. Res. Public Health 2021, 18, 6151. [Google Scholar] [CrossRef]
- Sakakura, K.; Taniguchi, Y.; Yamamoto, K.; Tsukui, T.; Jinnouchi, H.; Seguchi, M.; Wada, H.; Fujita, H. Modifiable and unmodifiable factors associated with slow flow following rotational atherectomy. PLoS ONE 2021, 16, e0250757. [Google Scholar] [CrossRef] [PubMed]
- Iannaccone, M.; Piazza, F.; Boccuzzi, G.G.; D’Ascenzo, F.; Latib, A.; Pennacchi, M.; Rossi, M.L.; Ugo, F.; Meliga, E.; Kawamoto, H.; et al. ROTational AThErectomy in acute coronary syndrome: Early and midterm outcomes from a multicentre registry. EuroIntervention 2016, 12, 1457–1464. [Google Scholar] [CrossRef] [Green Version]
- Allali, A.; Abdelghani, M.; Mankerious, N.; Abdel-Wahab, M.; Richardt, G.; Toelg, R. Feasibility and clinical outcome of rotational atherectomy in patients presenting with an acute coronary syndrome. Catheter. Cardiovasc. Interv. 2019, 93, 382–389. [Google Scholar] [CrossRef]
- Baruś, P.; Modrzewski, J.; Gumiężna, K.; Dunaj, P.; Głód, M.; Bednarek, A.; Wańha, W.; Roleder, T.; Kochman, J.; Tomaniak, M. Comparative Appraisal of Intravascular Ultrasound and Optical Coherence Tomography in Invasive Coronary Imaging: 2022 Update. J. Clin. Med. 2022, 11, 4055. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Rota-Lithotripsy Atherectomy (RA) N-15 | |
|---|---|
| Age | 70.9 ± 9.1 |
| Gender male (ratio) | 13 (86.7%) |
| Unstable angina | 2 (13.3%) |
| NSTEMI | 11 (73.4%) |
| STEMI | 2 (13.3%) |
| Diabetes mellitus | 10 (66.6%) |
| Chronic heart failure | 7 (46.7%) |
| Hypertension | 13 (86.6%) |
| Hyperlipidemia | 15 (100%) |
| Atrial fibrillation | 5 (33.3%) |
| History of PCI | 7 (46.7%) |
| History of MI | 8 (53.3%) |
| History of CABG | 2 (13.3%) |
| COPD | 3 (20%) |
| Chronic kidney diseases | 5 (33.3%) |
| History of stroke | 3 (20%) |
| Rota-Lithotripsy Atherectomy (RA) N-15 | |
|---|---|
| Syntax I score | 21.1 ± 10.9 |
| Syntax II—PCI score | 39.0 ± 14.9 |
| Syntax II PCI four-year mortality | 22.1 [5.2–23.5] |
| Syntax II—CABG score | 36.3 ± 8.7 |
| Syntax II CABG year mortality | 14.1 [7.6–18.3] |
| Radial access | 12 (80.0%) |
| 6F guide catheter | 4 (26.7%) |
| 7F or larger guide catheter | 11 (73.3%) |
| Initial unsuccessful predilatation | 9 (60.0%) |
| Rota burr diameter (mm) | 1.55 ± 0.15 |
| Rotablation duration time (s) | 111.7 ± 61.2 |
| RPM | 162,300 ± 4242 |
| IVL diameter (mm) | 3.2 ± 0.15 |
| Number of pulses | 45.3 ± 19.9 |
| Intravascular guidance | 4 (26.7%) |
| DES diameter (mm) | 3.16 ± 0.48 |
| Total DES length (mm) | 64 ± 29.7 |
| Postdilatation | 11 (73.3%) |
| Postdilatation balloon diameter (mm) | 3.41 ± 3.95 |
| Postdilatation pressure (atm) | 19.72 ± 0.55 |
| Acetylsalicylic acid | 15 (100%) |
| Clopidogrel | 6 (40%) |
| Ticagrelor | 6 (40%) |
| Prasugrel | 3 (20%) |
| Rota-Lithotripsy Atherectomy (RA) N-15 | |
|---|---|
| In-hospital period | |
| MACE | 1 (6.7%) |
| Death | 0 (0%) |
| Myocardial infarction | 1 (6.7%) |
| Target vessel revascularization | 1 (6.7%) |
| Stent thrombosis | 1 (6.7%) |
| Target lesion failure | 1 (6.7%) |
| Stent restenosis | 0 (0%) |
| Any revascularization | 1 (6.7%) |
| Cerebrovascular episodes | 0 (0%) |
| Major bleeding | 2 (13.3%) |
| 1-month follow-up | |
| MACE | 1 (6.7%) |
| Death | 0 (0%) |
| Myocardial infarction | 1 (6.7%) |
| Target vessel revascularization | 1 (6.7%) |
| Stent thrombosis | 1 (6.7%) |
| Target lesion failure | 1 (6.7%) |
| Stent restenosis | 0 (0%) |
| Any revascularization | 2 (13.3%) |
| Cerebrovascular episodes | 0 (0%) |
| Major bleeding | 2 (13.3%) |
| 6-month follow-up | |
| MACE | 2 (13.3%) |
| Death | 1 (6.7%) |
| Myocardial infarction | 1 (6.7%) |
| Target vessel revascularization | 1 (6.7%) |
| Stent thrombosis | 1 (6.7%) |
| Target lesion failure | 1 (6.7%) |
| Stent restenosis | 0 (0%) |
| Any revascularization | 5 (33.3%) |
| Cerebrovascular episodes | 0 (0%) |
| Major bleeding | 2 (13.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rola, P.; Furtan, Ł.; Włodarczak, S.; Kulczycki, J.J.; Barycki, M.; Szudrowicz, M.; Kędzierska, M.; Pszonka, A.; Korus, J.; Doroszko, A.; et al. Rota-Lithotripsy as a Novel Bail-Out Strategy for Highly Calcified Coronary Lesions in Acute Coronary Syndrome. Biomedicines 2022, 10, 2795. https://doi.org/10.3390/biomedicines10112795
Rola P, Furtan Ł, Włodarczak S, Kulczycki JJ, Barycki M, Szudrowicz M, Kędzierska M, Pszonka A, Korus J, Doroszko A, et al. Rota-Lithotripsy as a Novel Bail-Out Strategy for Highly Calcified Coronary Lesions in Acute Coronary Syndrome. Biomedicines. 2022; 10(11):2795. https://doi.org/10.3390/biomedicines10112795
Chicago/Turabian StyleRola, Piotr, Łukasz Furtan, Szymon Włodarczak, Jan Jakub Kulczycki, Mateusz Barycki, Marek Szudrowicz, Michalina Kędzierska, Anna Pszonka, Justyna Korus, Adrian Doroszko, and et al. 2022. "Rota-Lithotripsy as a Novel Bail-Out Strategy for Highly Calcified Coronary Lesions in Acute Coronary Syndrome" Biomedicines 10, no. 11: 2795. https://doi.org/10.3390/biomedicines10112795
APA StyleRola, P., Furtan, Ł., Włodarczak, S., Kulczycki, J. J., Barycki, M., Szudrowicz, M., Kędzierska, M., Pszonka, A., Korus, J., Doroszko, A., Lesiak, M., & Włodarczak, A. (2022). Rota-Lithotripsy as a Novel Bail-Out Strategy for Highly Calcified Coronary Lesions in Acute Coronary Syndrome. Biomedicines, 10(11), 2795. https://doi.org/10.3390/biomedicines10112795