

The Impact of Antipsychotic Treatment on Neurological Soft Signs in Patients with Predominantly Negative Symptoms of Schizophrenia
 , , , ,
, , , , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Setting and Subjects
2.2. Measurements
2.2.1. Assessment of Clinical Symptoms
2.2.2. Assessment of Neurological Signs
2.3. Statistical Analysis and Data Evaluation
3. Results
4. Discussion
4.1. Correlations with Extrapyramidal Side Effects Documented with the SAS
4.2. Patients with Predominantly Negative Symptoms (PNS) (n = 39) vs. Patients with Non-Predominantly Negative Symptoms NPNS (n = 60)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A










References
- Tsapakis, E.M.; Dimopoulou, T.; Tarazi, F.I. Clinical management of negative symptoms of schizophrenia: An update. Pharmacol. Ther. 2015, 153, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Kandel, E.R.; Schwartz, J.H.; Jessel, T.M.; Siegelbaum, S. Principles of Neural Sciences, 4th ed.; McGraw—Hill Medical: New York, NY, USA, 2000. [Google Scholar]
- Nasrallah, H.A.; Weinberger, D.R. The Neurology of Schizophrenia; BV: Amsterdam, The Netherlands, 1986. [Google Scholar]
- Baldessarini, R.J. Schizophrenia. N. Engl. J. Med. 1977, 297, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, S.; Beck, M.; Tsai, D.-H.; Haupt, F. Neurological Soft Signs (NSS) in Census-Based, Decade-Adjusted Healthy Adults, 20 to >70 Years of Age. Front. Psychiatry 2021, 12, 670539. [Google Scholar] [CrossRef]
- Buchanan, R.W.; Heinrichs, D.W. The neurological evaluation scale (NES): A structured instrument for the assessment of neurological signs in schizophrenia. Psychiatry Res. 1989, 27, 335–350. [Google Scholar] [CrossRef]
- Chen, E.Y.-H.; Hui, C.L.-M.; Chan, R.C.-K.; Dunn, E.L.-W.; Miao, M.Y.-K.; Yeung, W.-S.; Wong, C.-K.; Chan, W.-F.; Tang, W.-N. A 3-year prospective study of neurological soft signs in first-episode schizophrenia. Schizophr. Res. 2005, 75, 45–54. [Google Scholar] [CrossRef]
- Dazzan, P.; Morgan, K.; Orr, K.G.; Hutchinson, G.; Chitnis, X.; Suckling, J.; Fearon, P.; Salvo, J.; McGuire, P.; Mallett, R.M.; et al. The structural brain correlates of neurological soft signs in AeSOP first-episode psychoses study. Brain 2004, 127, 143–153. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Panagiotidis, P.; Gonda, X.; Kimiskidis, V.; Nimatoudis, I. Neurological soft signs significantly differentiate schizophrenia patients from healthy controls. Acta Neuropsychiatr. 2017, 30, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Panagiotidis, P.; Tegos, T.; Kimiskidis, V.; Nimatoudis, I. Paternal age and specific neurological soft signs as reliable and valid neurobiological markers for the diagnosis of patients with schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Schröder, J.; Niethammer, R.; Geider, F.-J.; Reitz, C.; Binkert, M.; Jauss, M.; Sauer, H. Neurological soft signs in schizophrenia. Schizophr. Res. 1991, 6, 25–30. [Google Scholar] [CrossRef]
- Bombin, I.; Arango, C.; Buchanan, R.W. Significance and Meaning of Neurological Signs in Schizophrenia: Two Decades Later. Schizophr. Bull. 2005, 31, 962–977. [Google Scholar] [CrossRef]
- Rossi, A.; De Cataldo, S.; Di Michele, V.; Manna, V.; Ceccoli, S.; Stratta, P.; Casacchia, M. Neurological Soft Signs in Schizophrenia. Br. J. Psychiatry 1990, 157, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.Y.; Lam, L.C.; Chen, R.Y.; Nguyen, D.G. Neurological Signs, Age, and Illness Duration in Schizophrenia. J. Nerv. Ment. Dis. 1996, 184, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Merriam, A.E.; Kay, S.R.; Opler, L.A.; Kushner, S.F.; van Praag, H.M. Neurological signs and the positive-negative dimension in schizophrenia. Biol. Psychiatry 1990, 28, 181–192. [Google Scholar] [CrossRef]
- A Flashman, L.; Flaum, M.; Gupta, S.; Andreasen, N.C. Soft signs and neuropsychological performance in schizophrenia. Am. J. Psychiatry 1996, 153, 526–532. [Google Scholar] [CrossRef]
- Wong, A.H.; Voruganti, L.N.; Heslegrave, R.J.; Awad, A.G. Neurocognitive deficits and neurological signs in schizophrenia. Schizophr. Res. 1997, 23, 139–146. [Google Scholar] [CrossRef]
- Chan, R.C.; Xu, T.; Heinrichs, R.W.; Yu, Y.; Gong, Q.-Y. Neurological soft signs in non-psychotic first-degree relatives of patients with schizophrenia: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2010, 34, 889–896. [Google Scholar] [CrossRef]
- Prikryl, R.; Ceskova, E.; Tronerova, S.; Kasparek, T.; Kucerova, H.P.; Ustohal, L.; Venclikova, S.; Vrzalova, M. Dynamics of neurological soft signs and its relationship to clinical course in patients with first-episode schizophrenia. Psychiatry Res. 2012, 200, 67–72. [Google Scholar] [CrossRef]
- White, C.; Stirling, J.; Hopkins, R.; Morris, J.; Montague, L.; Tantam, D.; Lewis, S. Predictors of 10-year outcome of first-episode psychosis. Psychol. Med. 2009, 39, 1447–1456. [Google Scholar] [CrossRef]
- Hirjak, D.; Van Harten, P.; Wolf, R. Commentary on Motor system dysfunction in the schizophrenia diathesis: Neural systems to neurotransmitters. Eur. Psychiatry 2017, 48, 49–50. [Google Scholar] [CrossRef]
- Hirjak, D.; Wolf, R.C.; Stieltjes, B.; Hauser, T.; Seidl, U.; Schröder, J.; Thomann, P.A. Cortical Signature of Neurological Soft Signs in Recent Onset Schizophrenia. Brain Topogr. 2013, 27, 296–306. [Google Scholar] [CrossRef]
- Boks, M.P.M.; Liddle, P.F.; Burgerhof, J.G.M.; Knegtering, R.; Bosch, R.-J.V.D. Neurological soft signs discriminating mood disorders from first episode schizophrenia. Acta Psychiatr. Scand. 2004, 110, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, R.W.; Koeppl, P.; Breier, A. Stability of neurological signs with clozapine treatment. Biol. Psychiatry 1994, 36, 198–200. [Google Scholar] [CrossRef]
- Scheffer, R.E. Abnormal neurological signs at the onset of psychosis. Schizophr. Res. 2004, 70, 19–26. [Google Scholar] [CrossRef]
- Dazzan, P.; Lloyd, T.; Morgan, K.D.; Zanelli, J.; Morgan, C.; Orr, K.; Hutchinson, G.; Fearon, P.; Allin, M.; Rifkin, L.; et al. Neurological abnormalities and cognitive ability in first-episode psychosis. Br. J. Psychiatry 2008, 193, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, S.; Degen, C.; Geider, F.J.; Schröder, J. Neurological soft signs in the clinical course of schizophrenia: Results of a meta-analysis. Front. Psychiatry 2014, 5, 185. [Google Scholar] [CrossRef]
- Lieberman, J.A.; Murray, R.M. Comprehensive Care of Schizophrenia: A Textbook of Clinical Management; London Malden MA: London, UK, 2001. [Google Scholar]
- Wimberley, T.; Støvring, H.; Sørensen, H.J.; Horsdal, H.T.; MacCabe, J.H.; Gasse, C. Predictors of treatment resistance in patients with schizophrenia: A population-based cohort study. Lancet Psychiatry 2016, 3, 358–366. [Google Scholar] [CrossRef]
- Jahn, T.; Hubmann, W.; Karr, M.; Mohr, F.; Schlenker, R.; Heidenreich, T.; Cohen, R.; Schröder, J. Motoric neurological soft signs and psychopathological symptoms in schizophrenic psychoses. Psychiatry Res. 2006, 142, 191–199. [Google Scholar] [CrossRef]
- Galderisi, S.; Maj, M.; Mucci, A.; Cassano, G.B.; Invernizzi, G.; Rossi, A.; Vita, A.; Dell’Osso, L.; Daneluzzo, E.; Pini, S. Historical, Psychopathological, Neurological, and Neuropsychological Aspects of Deficit Schizophrenia: A Multicenter Study. Am. J. Psychiatry 2002, 159, 983–990. [Google Scholar] [CrossRef]
- Mittal, V.A.; Dean, D.J.; Bernard, J.A.; Orr, J.; Pelletier-Baldelli, A.; Carol, E.E.; Gupta, T.; Turner, J.; Leopold, D.R.; Robustelli, B.L.; et al. Neurological Soft Signs Predict Abnormal Cerebellar-Thalamic Tract Development and Negative Symptoms in Adolescents at High Risk for Psychosis: A Longitudinal Perspective. Schizophr. Bull. 2013, 40, 1204–1215. [Google Scholar] [CrossRef]
- Mouchet-Mages, S.; Rodrigo, S.; Cachia, A.; Mouaffak, F.; Olie, J.P.; Meder, J.F.; Oppenheim, C.; Krebs, M.O. Correlations of cerebello-thalamo-prefrontal structure and neurological soft signs in patients with first-episode psychosis. Acta Psychiatr. Scand. 2011, 123, 451–458. [Google Scholar] [CrossRef]
- Rubin, P.; Vorstrup, S.; Hemmingsen, R.; Andersen, H.S.; Bendsen, B.B.; Strømsø, N.; Larsen, J.K.; Bolwig, T.G. Neurological abnormalities in patients with schizophrenia or schizophreniform disorder at first admission to hospital: Correlations with computerized tomography and regional cerebral blood flow findings. Acta Psychiatr. Scand. 1994, 90, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Ismail, B.T.; Cantor-Graae, E.; Cardenal, S.; McNeil, T.F. Neurological abnormalities in schizophrenia: Clinical, etiological and demographic correlates. Schizophr. Res. 1998, 30, 229–238. [Google Scholar] [CrossRef]
- Giordano, G.M.; Caporusso, E.; Pezzella, P.; Galderisi, S. Updated perspectives on the clinical significance of negative symptoms in patients with schizophrenia. Expert Rev. Neurother 2022, 22, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Schooler, N.R. Negative Symptoms in Schizophrenia: A Review and Clinical Guide for Recognition, Assessment, and Treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Laughren, T.; Levin, R. Food and Drug Administration Perspective on Negative Symptoms in Schizophrenia as a Target for a Drug Treatment Claim. Schizophr. Bull. 2005, 32, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Laughren, T.; Levin, R. Food and Drug Administration Commentary on Methodological Issues in Negative Symptom Trials. Schizophr. Bull. 2011, 37, 255–256. [Google Scholar] [CrossRef] [PubMed][Green Version]
- European Medicines Agency. Guideline on Clinical Investigation of Medicinal Products, Including Depot Preparations in the Treatment of Schizophrenia; European Medicines Agency: London, UK, 2012. [Google Scholar]
- Németh, G.; Laszlovszky, I.; Czobor, P.; Szalai, E.; Szatmári, B.; Harsányi, J.; Barabássy, Á.; Debelle, M.; Durgam, S.; Bitter, I.; et al. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: A randomised, double-blind, controlled trial. Lancet 2017, 389, 1103–1113. [Google Scholar] [CrossRef]
- Akinsulore, A.; Mapayi, B.M.; Aloba, O.O.; Oloniniyi, I.; Fatoye, F.O.; Makanjuola, R.O.A. Disability assessment as an outcome measure: A comparative study of Nigerian outpatients with schizophrenia and healthy control. Ann. Gen. Psychiatry 2015, 14, 40. [Google Scholar] [CrossRef]
- Schröder, J.; Tittel, A.; Stockert, A.; Karr, M. Memory deficits in subsyndromes of chronic schizophrenia. Schizophr. Res. 1996, 21, 19–26. [Google Scholar] [CrossRef]
- Whitty, P.; Clarke, M.; McTigue, O.; Browne, S.; Gervin, M.; Kamali, M.; Lane, A.; Kinsella, A.; Waddington, J.; Larkin, C.; et al. Diagnostic specificity and predictors of neurological soft signs in schizophrenia, bipolar disorder and other psychoses over the first 4 years of illness. Schizophr. Res. 2006, 86, 110–117. [Google Scholar] [CrossRef]
- Yazıcı, A.H.; Demir, B.; Yazıcı, K.M.; Gou, A.; Göğüş, A. Neurological soft signs in schizophrenic patients and their nonpsychotic siblings. Schizophr. Res. 2002, 58, 241–2466. [Google Scholar] [CrossRef]
- Chan, R.C.K.; Geng, F.-L.; Lui, S.S.Y.; Wang, Y.; Ho, K.K.Y.; Hung, K.S.Y.; Gur, R.E.; Gur, R.C.; Cheung, E.F.C. Course of neurological soft signs in first-episode schizophrenia: Relationship with negative symptoms and cognitive performances. Sci. Rep. 2015, 5, 11053. [Google Scholar] [CrossRef] [PubMed]
- Ciobanu, A.; Dionisie, V.; Neagu, C.; Bolog, O.; Riga, S.; Popa-Velea, O. Psychopharmacological Treatment, Intraocular Pressure and the Risk of Glaucoma: A Review of Literature. J. Clin. Med. 2021, 10, 2947. [Google Scholar] [CrossRef]
- Thomann, P.A.; Roebel, M.; Dos Santos, V.; Bachmann, S.; Essig, M.; Schröder, J. Cerebellar substructures and neurological soft signs in first-episode schizophrenia. Psychiatry Res. Neuroimaging 2009, 173, 83–87. [Google Scholar] [CrossRef]
- Mittal, V.A.; Hasenkamp, W.; Sanfilipo, M.; Wieland, S.; Angrist, B.; Rotrosen, J.; Duncan, E.J. Relation of neurological soft signs to psychiatric symptoms in schizophrenia. Schizophr. Res. 2007, 94, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Bersani, G.; Gherardelli, S.; Clemente, R.; Di Giannantonio, M.; Grilli, A.; Conti, C.M.V.; Exton, M.S.; Conti, P.; Doyle, R.; Pancheri, P. Neurologic Soft Signs in Schizophrenic Patients Treated With Conventional and Atypical Antipsychotics. J. Clin. Psychopharmacol. 2005, 25, 372–375. [Google Scholar] [CrossRef] [PubMed]
- de Bartolomeis, A.; Prinzivalli, E.; Callovini, G.; D’Ambrosio, L.; Altavilla, B.; Avagliano, C.; Iasevoli, F. Treatment resistant schizophrenia and neurological soft signs may converge on the same pathology: Evidence from explanatory analysis on clinical, psychopathological, and cognitive variables. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 81, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Rajaprabhakaran, R.; Arndt, S.; Flaum, M.; Andreasen, N.C. Premorbid adjustment as a predictor of phenomenological and neurobiological indices in schizophrenia. Schizophr. Res. 1995, 16, 189–197. [Google Scholar] [CrossRef]
- Smith, R.C.; Hussain, M.I.; Chowdhury, S.A.; Stearns, A. Stability of Neurological Soft Signs in Chronically Hospitalized Schizophrenic Patients. J. Neuropsychiatry Clin. Neurosci. 1999, 11, 91–96. [Google Scholar] [CrossRef]
- Browne, S.; Clarke, M.; Gervin, M.; Lane, A.; Waddington, J.L.; Larkin, C.; O’Callaghan, E. Determinants of neurological dysfunction in first episode schizophrenia. Psychol. Med. 2000, 30, 1433–1441. [Google Scholar] [CrossRef]
- Venkatasubramanian, G.; Latha, V.; Gangadhar, B.N.; Janakiramaiah, N.; Subbakrishna, D.K.; Jayakumar, P.N.; Keshavan, M.S. Neurological soft signs in never-treated schizophrenia. Acta Psychiatr. Scand. 2003, 108, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Andreasen, N.C.; Arndt, S.; Flaum, M.; Schultz, S.K.; Hubbard, W.C.; Smith, M. Neurological soft signs in neuroleptic-naive and neuroleptic-treated schizophrenic patients and in normal comparison subjects. Am. J. Psychiatry 1995, 152, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Caligiuri, M.P.; Lohr, J.B. A disturbance in the control of muscle force in neuroleptic-naive schizophrenic patients. Biol. Psychiatry 1994, 35, 104–111. [Google Scholar] [CrossRef]
- Schröder, J.; Silvestri, S.; Bubeck, B.; Karr, M.; Demisch, S.; Scherrer, S.; Geider, F.J.; Sauer, H. D2 Dopamine Receptor Up-Regulation, Treatment Response, Neurological Soft Signs, and Extrapyramidal Side Effects in Schizophrenia: A Follow-Up Study with 123I-Iodobenzamide Single Photon Emission Computed Tomography in the Drug-Naive State and after Neuroleptic Treatment. Biol. Psychiatry 1998, 43, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Sykes, D.; Moore, H.; Stott, L.; Holliday, N.; Javitch, J.; Lane, J.R.; Charlton, S.J. Extrapyramidal side effects of antipsychotics are linked to their association kinetics at dopamine D2 receptors. Nat. Commun. 2017, 8, 763. [Google Scholar] [CrossRef]
- Koning, J.P.; Tenback, D.E.; Van Os, J.; Aleman, A.; Kahn, R.S.; Van Harten, P.N. Dyskinesia and Parkinsonism in Antipsychotic-Naive Patients with Schizophrenia, First-Degree Relatives and Healthy Controls: A Meta-analysis. Schizophr. Bull. 2010, 36, 723–731. [Google Scholar] [CrossRef]
- López-Muñoz, F.; Alamo, C.; Cuenca, E.; Shen, W.; Clervoy, P.; Rubio, G. History of the Discovery and Clinical Introduction of Chlorpromazine. Ann. Clin. Psychiatry 2005, 17, 113–135. [Google Scholar] [CrossRef]
- Crilly, J. The history of clozapine and its emergence in the US market A Review and analysis. Hist. Psychiatry 2007, 18, 39–60. [Google Scholar] [CrossRef]
- Bachmann, S.; Schröder, J. Neurological Soft Signs in Schizophrenia: An Update on the State- versus Trait-Perspective. Front. Psychiatry 2017, 8, 272. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Davis, J.M. Dose equivalence of the anti-psychotic drugs. J. Psychiatr. Res. 1974, 11, 65–69. [Google Scholar] [CrossRef]
- Venkatasubramanian, G.; Danivas, V. Current perspectives on chlorpromazine equivalents: Comparing apples and oranges! Indian J. Psychiatry 2013, 55, 207–208. [Google Scholar] [CrossRef] [PubMed]
- Leucht, S.; Samara, M.; Heres, S.; Davis, J.M. Dose Equivalents for Antipsychotic Drugs: The DDD Method: Table 1. Schizophr. Bull. 2016, 42, S90–S94. [Google Scholar] [CrossRef] [PubMed]
- Woods, S.W. Chlorpromazine Equivalent Doses for the Newer Atypical Antipsychotics. J. Clin. Psychiatry 2003, 64, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Stauffer, V.L.; Song, G.; Kinon, B.J.; Ascher-Svanum, H.; Chen, L.; Feldman, P.D.; Conley, R.R. Responses to antipsychotic therapy among patients with schizophrenia or schizoaffective disorder and either predominant or prominent negative symptoms. Schizophr. Res. 2012, 134, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Olié, J.-P.; Spina, E.; Murray, S.; Yang, R. Ziprasidone and amisulpride effectively treat negative symptoms of schizophrenia: Results of a 12-week, double-blind study. Int. Clin. Psychopharmacol. 2006, 21, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Riedel, M.; Müller, N.; Strassnig, M.; Spellmann, I.; Engel, R.R.; Musil, R.; Dehning, S.; Douhet, A.; Schwarz, M.J.; Möller, H. Quetiapine has equivalent efficacy and superior tolerability to risperidone in the treatment of schizophrenia with predominantly negative symptoms. Eur. Arch. Psychiatry Clin. Neurosci. 2005, 255, 432–437. [Google Scholar] [CrossRef]
- Rabinowitz, J.; Werbeloff, N.; Caers, I.; Mandel, F.S.; Stauffer, V.; Menard, F.; Kinon, B.J.; Kapur, S. Negative symptoms in schizophrenia—The remarkable impact of inclusion definitions in clinical trials and their consequences. Schizophr. Res. 2013, 150, 334–338. [Google Scholar] [CrossRef]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; Revised; US Department of Health, Education, and Welfare Publication (ADM), National Institute of Mental Health: Rockville, MD, USA, 1976; pp. 76–338. [Google Scholar]
- Leucht, S.; Barabássy, Á.; Laszlovszky, I.; Szatmári, B.; Acsai, K.; Szalai, E.; Harsányi, J.; Earley, W.; Németh, G. Linking PANSS negative symptom scores with the Clinical Global Impressions Scale: Understanding negative symptom scores in schizophrenia. Neuropsychopharmacology 2019, 44, 1589–1596. [Google Scholar] [CrossRef]
- Simpson, G.M.; Angus, J.W.S. Rating Scale for Extrapyramidal Side Effects. Acta Psychiatr. Scand. 1970, 45, 11–19. [Google Scholar] [CrossRef]
- Hawley, C.; Fineberg, N.; Roberts, A.; Baldwin, D.; Sahadevan, A.; Sharman, V. The use of the Simpson Angus Scale for the assessment of movement disorder: A training guide. Int. J. Psychiatry Clin. Pr. 2003, 7, 349–2257. [Google Scholar] [CrossRef] [PubMed]
- Merhej, G.; Hallit, S.; Haddad, C.; Hachem, D.; Haddad, G. Neurological soft signs in schizophrenia: Gender differences and promising suggestions. J. Psychopathol. 2017, 23, 74–78. [Google Scholar]
- Herold, C.J.; Duval, C.Z.; Lässer, M.M.; Schröder, J. Neurological soft signs (NSS) and cognitive impairment in chronic schizophrenia. Schizophr. Res. Cogn. 2019, 16, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.D.; McEvoy, J.P.; Davis, S.M.; Caroff, S.N.; Saltz, B.L.; Chakos, M.H.; Swartz, M.S.; Keefe, R.S.; Rosenheck, R.A.; Stroup, T.S.; et al. Clinical correlates of tardive dyskinesia in schizophrenia: Baseline data from the CATIE schizophrenia trial. Schizophr. Res. 2005, 80, 33–43. [Google Scholar] [CrossRef]
- Misdrahi, D.; Tessier, A.; Daubigney, A.; Meissner, W.G.; Schurhoff, F.; Boyer, L.; Godin, O.; Bulzacka, E.; Aouizerate, B.; Andrianarisoa, M.; et al. Prevalence of and Risk Factors for Extrapyramidal Side Effects of Antipsychotics. J. Clin. Psychiatry 2019, 80, 7055. [Google Scholar] [CrossRef]
- Leucht, S.; Corves, C.; Arbter, D.; Engel, R.R.; Li, C.; Davis, J.M. Second-generation versus first-generation antipsychotic drugs for schizophrenia: A meta-analysis. Lancet 2009, 373, 31–41. [Google Scholar] [CrossRef]
- Minzenberg, M.J.; Poole, J.H.; Benton, C.; Vinogradov, S. Association of Anticholinergic Load With Impairment of Complex Attention and Memory in Schizophrenia. Am. J. Psychiatry 2004, 161, 116–124. [Google Scholar] [CrossRef]
- Ogino, S.; Miyamoto, S.; Miyake, N.; Yamaguchi, N. Benefits and limits of anticholinergic use in schizophrenia: Focusing on its effect on cognitive function. Psychiatry Clin. Neurosci. 2014, 68, 37–49. [Google Scholar] [CrossRef]
- Prikryl, R.; Ceskova, E.; Kasparek, T.; Kucerova, H. Neurological soft signs, clinical symptoms and treatment reactivity in patients suffering from first episode schizophrenia. J. Psychiatr. Res. 2006, 40, 141–146. [Google Scholar] [CrossRef]
- Cvetić, T.; Vuković, O.; Britvić, D.; Ivković, M.; Dukić-Dejanović, S.; Lecić-Tosevski, D. Comparative analysis of soft neurological signs in positive and negative subtype of schizophrenia. Psychiatr. Danub. 2009, 21, 174–178. [Google Scholar]
- Bègue, I.; Kaiser, S.; Kirschner, M. Pathophysiology of negative symptom dimensions of schizophrenia—Current developments and implications for treatment. Neurosci. Biobehav. Rev. 2020, 116, 74–88. [Google Scholar] [CrossRef] [PubMed]
- Roth, R.M.; Garlinghouse, M.A.; Flashman, L.A.; Koven, N.S.; Pendergrass, J.C.; Ford, J.C.; McAllister, T.W.; Saykin, A.J. Apathy Is Associated with Ventral Striatum Volume in Schizophrenia Spectrum Disorder. J. Neuropsychiatry Clin. Neurosci. 2016, 28, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Caravaggio, F.; Fervaha, G.; Iwata, Y.; Plitman, E.; Chung, J.K.; Nakajima, S.; Mar, W.; Gerretsen, P.; Kim, J.; Chakravarty, M.M.; et al. Amotivation is associated with smaller ventral striatum volumes in older patients with schizophrenia. Int. J. Geriatr. Psychiatry 2017, 33, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Giordano, G.M.; Stanziano, M.; Papa, M.; Mucci, A.; Prinster, A.; Soricelli, A.; Galderisi, S. Functional connectivity of the ventral tegmental area and avolition in subjects with schizophrenia: A resting state functional MRI study. Eur. Neuropsychopharmacol. 2018, 28, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Walton, E.; Hibar, D.P.; Van Erp, T.G.M.; Potkin, S.G.; Roiz-Santiañez, R.; Crespo-Facorro, B.; Suarez-Pinilla, P.; Van Haren, N.E.M.; De Zwarte, S.M.C.; Kahn, R.S.; et al. Prefrontal cortical thinning links to negative symptoms in schizophrenia via the ENIGMA consortium. Psychol. Med. 2017, 48, 82–94. [Google Scholar] [CrossRef]
- Kong, L.; Bachmann, S.; Thomann, P.A.; Essig, M.; Schröder, J. Neurological soft signs and gray matter changes: A longitudinal analysis in first-episode schizophrenia. Schizophr. Res. 2012, 134, 27–32. [Google Scholar] [CrossRef]
- Kong, L.; Herold, C.J.; Lässer, M.M.; Schmid, L.A.; Hirjak, D.; Thomann, P.A.; Essig, M.; Schröder, J. Association of Cortical Thickness and Neurological Soft Signs in Patients with Chronic Schizophrenia and Healthy Controls. Neuropsychobiology 2015, 71, 225–233. [Google Scholar] [CrossRef]
- Hirjak, D.; Kubera, K.M.; Wolf, R.C.; Thomann, A.K.; Hell, S.K.; Seidl, U.; Thomann, P.A. Local brain gyrification as a marker of neurological soft signs in schizophrenia. Behav. Brain Res. 2015, 292, 19–25. [Google Scholar] [CrossRef]
- Kring, A.M.; Gur, R.E.; Blanchard, J.J.; Horan, W.P.; Reise, S.P. The Clinical Assessment Interview for Negative Symptoms (CAINS): Final Development and Validation. Am. J. Psychiatry 2013, 170, 165–172. [Google Scholar] [CrossRef]
- Kirkpatrick, B.; Strauss, G.P.; Nguyen, L.; Fischer, B.A.; Daniel, D.G.; Cienfuegos, A.; Marder, S.R. The Brief Negative Symptom Scale: Psychometric Properties. Schizophr. Bull. 2010, 37, 300–305. [Google Scholar] [CrossRef]
- Galderisi, S.; Mucci, A.; Dollfus, S.; Nordentoft, M.; Falkai, P.; Kaiser, S.; Giordano, G.M.; Vandevelde, A.; Nielsen, M.; Glenthøj, L.B.; et al. EPA guidance on assessment of negative symptoms in schizophrenia. Eur. Psychiatry 2021, 64, e23. [Google Scholar] [CrossRef] [PubMed]
- Addington, D.; Addington, J.; Schissel, B. A depression rating scale for schizophrenics. Schizophr. Res. 1990, 3, 247–251. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CGI Score | n |
|---|---|
| 1 = Normal, not at all ill | 0 |
| 2 = Borderline mentally ill | 2 |
| 3 = Mildly ill | 13 |
| 4 = Moderately ill | 24 |
| 5 = Markedly ill | 45 |
| 6 = Severely ill | 15 |
| 7 = Among the most extremely ill patients | 0 |
| Total | 99 |
| Variable | Global (n = 99) |
|---|---|
| Sex | |
| F | 56 (56.6%) |
| M | 43 (43.4%) |
| Age | |
| Mean (SD) | 30.6 (10.4) |
| Median (Min, Max) | 26.0 (18.0, 65.0) |
| Environment | |
| R | 12 (12.1%) |
| U | 87 (87.9%) |
| Years of education | |
| Mean (SD) | 12.4 (1.94) |
| Median (Min, Max) | 12.0 (8.00, 18.0) |
| Economic status | |
| Employed | 11 (11.1%) |
| Retired | 44 (44.4%) |
| Unemployed | 37 (37.4%) |
| Student | 7 (7.1%) |
| Age of onset | |
| Mean (SD) | 22.5 (4.67) |
| Median (Min, Max) | 21.0 (17.0, 40.0) |
| Duration of illness | |
| Mean (SD) | 8.15 (7.78) |
| Median (Min, Max) | 5.00 (1.00, 35.0) |
| Age at first treatment | |
| Mean (SD) | 22.8 (4.72) |
| Median (Min, Max) | 21.0 (18.0, 40.0) |
| Missing | 3 (3.0%) |
| Age at first hospitalisation | |
| Mean (SD) | 23.3 (5.24) |
| Median (Min, Max) | 22.0 (18.0, 40.0) |
| N/A | 2 (2.0%) |
| Number of hospitalisations | |
| Mean (SD) | 5.27 (4.21) |
| Median [Min, Max] | 4.00 (1.00, 25.0) |
| Cumulative hospitalised period | |
| Mean (SD) | 3.98 (3.05) |
| Median (Min, Max) | 3.50 (0.500, 15.0) |
| PANSS, CGI correlation | |
| Mean (SD) | 4.59 (0.969) |
| Median (Min, Max) | 5.00 (2.00, 6.00) |
| PANSS P | |
| Mean (SD) | 21.6 (6.06) |
| Median (Min, Max) | 22.0 (8.00, 35.0) |
| PANSS N | |
| Mean (SD) | 21.4 (6.32) |
| Median (Min, Max) | 21.0 (8.00, 39.0) |
| PANSS, general | |
| Mean (SD) | 41.8 (8.66) |
| Median (Min, Max) | 41.0 (20.0, 65.0) |
| PANSS, total | |
| Mean (SD) | 84.8 (16.8) |
| Median (Min, Max) | 86.0 (42.0, 123) |
| PANSS, predominantly negative | |
| Yes | 39 (39.4%) |
| No | 60 (60.6%) |
| Type of treatment | |
| TA | 4 (4.0%) |
| AA | 86 (86.9%) |
| 2 AA | 9 (9.1%) |
| Daily dose of CPZE | |
| Mean (SD) | 424 (219) |
| Median (Min, Max) | 400 (75.0, 1500) |
| Anticholinergic treatment | |
| Yes | 24 (24.2%) |
| No | 75 (75.8%) |
| NES, sensory integration | |
| Mean (SD) | 1.67 (1.52) |
| Median (Min, Max) | 2.00 (0, 7.00) |
| NES, motor coordination | |
| Mean (SD) | 2.08 (1.60) |
| Median (Min, Max) | 2.00 (0, 8.00) |
| NES, sequencing of complex motor acts | |
| Mean (SD) | 3.12 (1.98) |
| Median (Min, Max) | 3.00 (0, 8.00) |
| NES, other | |
| Mean (SD) | 3.57 (2.62) |
| Median (Min, Max) | 3.00 (0, 10.0) |
| NES, total | |
| Mean (SD) | 10.5 (5.50) |
| Median (Min, Max) | 10.0 (0, 22.0) |
| SAS | |
| Mean (SD) | 3.04 (2.01) |
| Median (Min, Max) | 3.00 (0, 9.00) |
| Predictors | n | Beta (95% CI) | p-Value |
|---|---|---|---|
| Sex | 99 | ||
| F | — | ||
| M | 3.3 (1.3 to 5.4) | 0.002 | |
| Age | 99 | 0.19 (0.09 to 0.29) | <0.001 |
| Environment | 99 | ||
| R | — | ||
| U | −2.5 (−5.8 to 0.78) | 0.138 | |
| Marital status | 99 | ||
| With a partner | — | ||
| No partner | 0.01 (−2.4 to 2.5) | 0.991 | |
| Years of education | 99 | −0.41 (−1.0 to 0.15) | 0.157 |
| Economic status | 99 | ||
| Employed | — | ||
| Retired | 6.8 (3.4 to 10) | <0.001 | |
| Unemployed | 3.3 (−0.11 to 6.7) | 0.061 | |
| Student | 1.9 (−2.9 to 6.7) | 0.436 | |
| Age of onset | 99 | 0.23 (0.01 to 0.46) | 0.048 |
| Duration of illness (years) | 99 | 0.25 (0.12 to 0.38) | <0.001 |
| Age at first treatment | 96 | 0.20 (−0.03 to 0.43) | 0.098 |
| Age at first hospitalisation | 97 | 0.20 (−0.01 to 0.40) | 0.069 |
| Number of hospitalizations | 99 | 0.54 (0.30 to 0.77) | <0.001 |
| Cumulative hospitalised period (months) | 99 | 0.80 (0.47 to 1.1) | <0.001 |
| Daily dose of CPZE | 99 | 0.001 (−0.003 to 0.007) | 0.438 |
| Anticholinergic | 99 | ||
| Yes | — | ||
| No | −0.45 (−3.0 to 2.1) | 0.732 | |
| Dominance | 99 | ||
| L | — | ||
| R | −5.2 (−8.5 to −1.9) | 0.003 |
| Paired Two-Sample t-Test for Means | Paired Two-Sample t-Test for Means | ||||
|---|---|---|---|---|---|
| PANSS negative | Total NES | Total PANSS | Total NES | ||
| Mean | 21.42 | 10.45 | Mean | 84.84 | 10.45 |
| Variance | 39.96 | 30.27 | Variance | 281.418 | 30.27 |
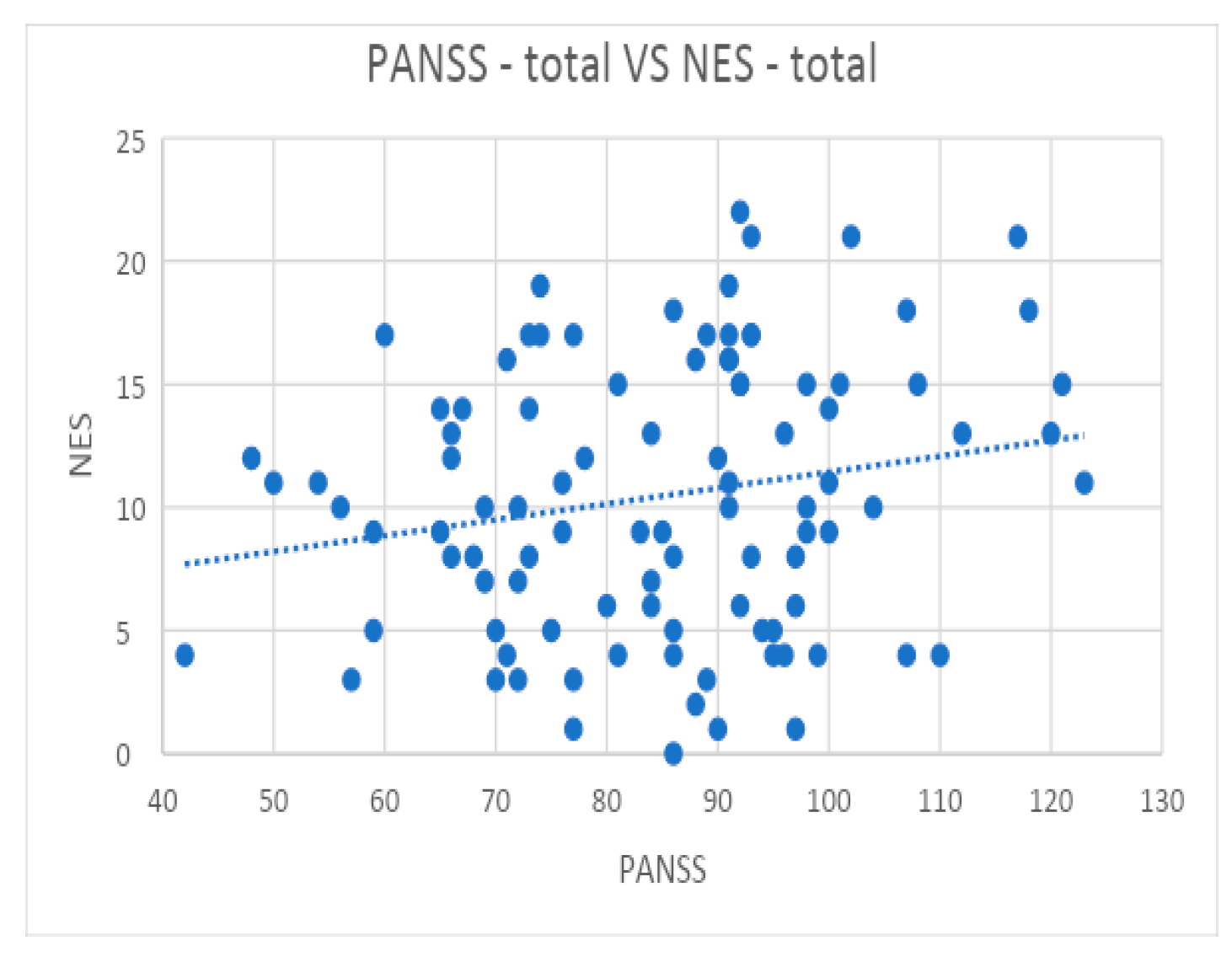
| r | 0.33 | r | 0.19 | ||
| Predictors | n | Beta (95% CI) 1 | p-Value |
|---|---|---|---|
| Sex | 99 | ||
| F | — | ||
| M | 0.75 (−0.04 to 1.5) | 0.066 | |
| Age | 99 | 0.02 (−0.02 to 0.06) | 0.385 |
| Environment | 99 | ||
| R | — | ||
| U | −0.71 (−1.9 to 0.50) | 0.253 | |
| Marital status | 99 | ||
| With a partner | — | ||
| No partner | 0.21 (−0.69 to 1.1) | 0.649 | |
| Years of education | 99 | −0.19 (−0.39 to 0.01) | 0.072 |
| Economic status | 99 | ||
| Employed | — | ||
| Retired | 1.0 (−0.37 to 2.3) | 0.16 | |
| Unemployed | 0.24 (−1.1 to 1.6) | 0.729 | |
| Student | −0.26 (−2.2 to 1.6) | 0.789 | |
| Age at onset | 99 | −0.03 (−0.11 to 0.06) | 0.544 |
| Duration of illness (years) | 99 | 0.04 (−0.01 to 0.09) | 0.127 |
| Age at first treatment | 96 | −0.02 (−0.10 to 0.06) | 0.645 |
| Age at first hospitalisation | 97 | 0.00 (−0.08 to 0.08) | 0.983 |
| Number of hospitalizations | 99 | 0.15 (0.06 to 0.24) | 0.001 |
| Cumulative hospitalised period (months) | 99 | 0.21 (0.09 to 0.34) | 0.001 |
| Type of treatment | 99 | ||
| TA | — | ||
| AA | −3.9 (−5.8 to −2.0) | <0.001 | |
| 2 AA | −3.6 (−5.9 to −1.4) | 0.002 | |
| Daily dose of CPZE | 99 | 0.01 (0.00 to 0.01) | <0.001 |
| Anticholinergic | 99 | ||
| Yes | — | ||
| No | −1.2 (−2.1 to −0.31) | 0.010 | |
| Dominance | 99 | ||
| L | — | ||
| R | 0.05 (−1.2 to 1.3) | 0.944 |
| Predictors | Beta (95% CI) 1 | p-Value |
|---|---|---|
| Daily dose of CPZE | 0.004 (0.003 to 0.006) | <0.001 |
| Number of hospitalizations | 0.16 (0.09 to 0.23) | <0.001 |
| Type of treatment | ||
| TA | — | |
| AA | −2.1 (−3.8 to −0.51) | 0.011 |
| 2 AA | −2.7 (−4.6 to −0.89) | 0.004 |
| NES-SI | NES-MC | NES-SCMA | NES-Others | NES-Total | SAS | CLPZE MG | |
|---|---|---|---|---|---|---|---|
| NES-SI | 1 | ||||||
| NES-MC | 0.34 | 1 | |||||
| NES-SCMA | 0.39 | 0.34 | 1 | ||||
| NES-Other | 0.40 | 0.25 | 0.28 | 1 | |||
| NES-Total | 0.71 | 0.63 | 0.7 | 0.76 | 1 | ||
| SAS | 0.33 | 0.17 | 0.27 | 0.26 | 0.37 | 1 | |
| CPZE | 0.03 | 0.15 | 0.15 | −0.07 | 0.07 | 0.57 | 1 |
| Variables | PNS n = 39 | NPNS n = 60 | p-Value 1 |
|---|---|---|---|
| Ex, n (%) | <0.001 | ||
| F | 13 (33) | 43 (72) | |
| M | 26 (67) | 17 (28) | |
| Age, mean (SD) | 29.31 (8.72) | 31.47 (11.30) | 0.29 |
| Environment, n (%) | >0.99 | ||
| R | 5 (13) | 7 (12) | |
| U | 34 (87) | 53 (88) | |
| Marital status, n (%) | 0.093 | ||
| With a partner (actual or historical) | 7 (18) | 20 (33) | |
| No partner | 32 (82) | 40 (67) | |
| Years of schooling (number of years of education), mean (SD) | 12.38 (1.90) | 12.42 (1.99) | 0.94 |
| Economic status, n (%) | 0.27 | ||
| Employed | 2 (5.1) | 9 (15) | |
| Retired | 16 (41) | 28 (47) | |
| Unemployed | 17 (44) | 20 (33) | |
| Student | 4 (10) | 3 (5.0) | |
| Age at onset, mean (SD) | 21.85 (3.62) | 22.87 (5.23) | 0.25 |
| Duration of illness (years), mean (SD) | 7.46 (7.22) | 8.60 (8.15) | 0.47 |
| Age at first treatment, mean (SD) | 22.08 (3.73) | 23.29 (5.25) | 0.19 |
| N/A | 1 | 2 | |
| Age at first hospitalisation, mean (SD) | 22.67 (4.37) | 23.72 (5.75) | 0.31 |
| N/A | 0 | 2 | |
| Number of pre-evaluation (pre-diagnosis) hospitalizations, mean (SD) | 5.87 (4.73) | 4.88 (3.83) | 0.28 |
| Cumulative hospitalised period, mean (SD) | 4.63 (3.73) | 3.56 (2.45) | 0.12 |
| PANSS–CGI correlation, mean (SD) | 4.92 (0.70) | 4.37 (1.07) | 0.002 |
| General PANSS, mean (SD) | 43.79 (8.08) | 40.48 (8.84) | 0.058 |
| PANSS Negative, Mean (SD) | 26.15 (4.25) | 18.35 (5.51) | <0.001 |
| PANSS Positive, Mean (SD) | 20.44 (4.91) | 22.42 (6.63) | 0.091 |
| Total PANSS, mean (SD) | 90.38 (13.90) | 81.25 (17.60) | 0.005 |
| Daily dose of CPZE, mean (SD) | 446.79 (179.84) | 409.58 (241.99) | 0.38 |
| SAS mean (SD) | 2.98 (1.97) | 3.13 (2.10) | 0.73 |
| Anticholinergic, n (%) | 0.83 | ||
| Yes | 9 (23) | 15 (25) | |
| No | 30 (77) | 45 (75) | |
| Dominance, n (%) | 0.11 | ||
| L | 7 (18) | 4 (6.7) | |
| R | 32 (82) | 56 (93) | |
| NES—motor coordination, mean (SD) | 2.59 (1.71) | 1.75 (1.43) | 0.013 |
| NES—sensory integration, mean (SD) | 2.13 (1.82) | 1.37 (1.21) | 0.024 |
| NES—sequencing of complex motor acts, mean (SD) | 3.67 (2.07) | 2.77 (1.84) | 0.03 |
| Other NES, mean (SD) | 4.05 (2.66) | 3.25 (2.57) | 0.14 |
| Total NES, mean (SD) | 12.49 (5.35) | 9.13 (5.23) | 0.003 |
| Age | YOE | AAO | DOI | AFT | AFH | NOH | CHP | PANSS P | PANSS N | PANSS, general | PANSS, total | CPZE | NES-SI | NES-MC | NES-SCMA | NES, other | NES, total | SAS | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 1 | ||||||||||||||||||
| YOE | −0.02 | 1 | |||||||||||||||||
| AAO | 0.59 | 0.16 | 1 | ||||||||||||||||
| DOI (years) | 0.91 | −0.1 | 0.2 | 1 | |||||||||||||||
| AFT (years) | 0.57 | 0.14 | 0.97 | 0.18 | 1 | ||||||||||||||
| AFH (years) | 0.65 | 0.13 | 0.89 | 0.33 | 0.98 | 1 | |||||||||||||
| NOH | 0.54 | 0 | 0.11 | 0.6 | 0.05 | 0.27 | 1 | ||||||||||||
| CHP | 0.44 | −0.1 | 0.03 | 0.51 | −0.01 | 0.17 | 0.92 | 1 | |||||||||||
| PANSS P | −0.32 | −0.22 | −0.21 | −0.28 | −0.25 | −0.24 | −0.09 | 0.01 | 1 | ||||||||||
| PANSS N | −0.37 | −0.35 | −0.19 | −0.36 | −0.19 | −0.14 | −0.09 | 0.09 | 0.69 | 1 | |||||||||
| PANSS, general | 0.2 | −0.27 | 0.09 | 0.2 | 0.03 | 0.04 | 0.1 | 0.12 | 0.46 | 0.29 | 1 | ||||||||
| PANSS, total | −0.1 | −0.35 | −0.07 | −0.09 | −0.12 | −0.1 | 0.02 | 0.11 | 0.83 | 0.71 | 0.83 | 1 | |||||||
| DD CPZE | 0.1 | −0.03 | −0.08 | 0.17 | −0.06 | 0.04 | 0.28 | 0.3 | −0.13 | 0.13 | −0.11 | −0.07 | 1 | ||||||
| NES-SI | 0.17 | −0.22 | 0.18 | 0.11 | 0.17 | 0.24 | 0.34 | 0.33 | 0.13 | 0.3 | −0.04 | 0.11 | 0.09 | 1 | |||||
| NES-MC | 0.02 | 0.04 | 0.11 | −0.02 | 0.03 | 0.12 | 0.12 | 0.12 | 0.09 | 0.2 | 0.1 | 0.15 | 0.08 | 0.31 | 1 | ||||
| NES-SCMA | 0.2 | −0.1 | 0.11 | 0.19 | 0.14 | 0.07 | 0.27 | 0.38 | 0.01 | 0.09 | 0.31 | 0.21 | 0.24 | 0.22 | 0.16 | 1 | |||
| NES, other | 0.54 | −0.21 | 0.24 | 0.53 | 0.27 | 0.26 | 0.25 | 0.23 | 0.06 | 0.01 | 0.27 | 0.18 | 0.02 | 0.28 | 0.07 | 0.22 | 1 | ||
| NES, total | 0.43 | −0.18 | 0.27 | 0.38 | 0.27 | 0.29 | 0.41 | 0.42 | 0.1 | 0.2 | 0.28 | 0.26 | 0.17 | 0.67 | 0.52 | 0.62 | 0.7 | 1 | |
| SAS | 0.38 | −0.06 | 0.06 | 0.43 | 0.01 | 0.2 | 0.41 | 0.4 | −0.12 | −0.01 | 0 | −0.05 | 0.69 | 0.4 | 0.13 | 0.31 | 0.28 | 0.44 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrescu, C.; Papacocea, I.R.; Vilciu, C.; Mihalache, O.A.; Vlad, D.M.; Marian, G.; Focseneanu, B.E.; Sima, C.T.; Ciobanu, C.A.; Riga, S.; et al. The Impact of Antipsychotic Treatment on Neurological Soft Signs in Patients with Predominantly Negative Symptoms of Schizophrenia. Biomedicines 2022, 10, 2939. https://doi.org/10.3390/biomedicines10112939
Petrescu C, Papacocea IR, Vilciu C, Mihalache OA, Vlad DM, Marian G, Focseneanu BE, Sima CT, Ciobanu CA, Riga S, et al. The Impact of Antipsychotic Treatment on Neurological Soft Signs in Patients with Predominantly Negative Symptoms of Schizophrenia. Biomedicines. 2022; 10(11):2939. https://doi.org/10.3390/biomedicines10112939
Chicago/Turabian StylePetrescu, Cristian, Ioana R. Papacocea, Crisanda Vilciu, Oana A. Mihalache, Diana M. Vlad, Gabriela Marian, Brindusa E. Focseneanu, Cristian T. Sima, Constantin A. Ciobanu, Sorin Riga, and et al. 2022. "The Impact of Antipsychotic Treatment on Neurological Soft Signs in Patients with Predominantly Negative Symptoms of Schizophrenia" Biomedicines 10, no. 11: 2939. https://doi.org/10.3390/biomedicines10112939
APA StylePetrescu, C., Papacocea, I. R., Vilciu, C., Mihalache, O. A., Vlad, D. M., Marian, G., Focseneanu, B. E., Sima, C. T., Ciobanu, C. A., Riga, S., & Ciobanu, A. M. (2022). The Impact of Antipsychotic Treatment on Neurological Soft Signs in Patients with Predominantly Negative Symptoms of Schizophrenia. Biomedicines, 10(11), 2939. https://doi.org/10.3390/biomedicines10112939