
Intranasal Oxytocin Modulates Decision-Making Depending on Outcome Predictability—A Randomized Within-Subject Controlled Trial in Healthy Males
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Substance Administration
2.4. Decision-Making/Risk-Taking Tasks
2.5. Neuropsychological Tasks
2.6. Analysis
3. Results
3.1. Decision-Making
3.2. Emotional Valence (AGN) and Rule Acquisition (IED)
3.3. Side Effects
4. Discussion
4.1. Limitations
4.2. Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horta, M.; Pehlivanoglu, D.; Ebner, N.C. The Role of Intranasal Oxytocin on Social Cognition: An Integrative Human Lifespan Approach. Curr. Behav. Neurosci. Rep. 2020, 7, 175–192. [Google Scholar] [CrossRef] [PubMed]
- Churchland, P.S.; Winkielman, P. Modulating Social Behavior with Oxytocin: How Does It Work? What Does It Mean? Horm. Behav. 2012, 61, 392–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winterton, A.; Westlye, L.T.; Steen, N.E.; Andreassen, O.A.; Quintana, D.S. Improving the Precision of Intranasal Oxytocin Research. Nat. Hum. Behav. 2021, 5, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Quintana, D.S.; Lischke, A.; Grace, S.; Scheele, D.; Ma, Y.; Becker, B. Advances in the Field of Intranasal Oxytocin Research: Lessons Learned and Future Directions for Clinical Research. Mol. Psychiatry 2021, 26, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Peled-Avron, L.; Abu-Akel, A.; Shamay-Tsoory, S. Exogenous Effects of Oxytocin in Five Psychiatric Disorders: A Systematic Review, Meta-Analyses and a Personalized Approach through the Lens of the Social Salience Hypothesis. Neurosci. Biobehav. Rev. 2020, 114, 70–95. [Google Scholar] [CrossRef]
- Guastella, A.J.; Mitchell, P.B.; Mathews, F. Oxytocin Enhances the Encoding of Positive Social Memories in Humans. Biol. Psychiatry 2008, 64, 256–258. [Google Scholar] [CrossRef]
- Klackl, J.; Pfundmair, M.; Agroskin, D.; Jonas, E. Who Is to Blame? Oxytocin Promotes Nonpersonalistic Attributions in Response to a Trust Betrayal. Biol. Psychol. 2013, 92, 387–394. [Google Scholar] [CrossRef]
- Zhang, H.; Gross, J.; De Dreu, C.; Ma, Y. Oxytocin Promotes Coordinated Out-Group Attack during Intergroup Conflict in Humans. eLife 2019, 8, e40698. [Google Scholar] [CrossRef]
- Yatawara, C.J.; Einfeld, S.L.; Hickie, I.B.; Davenport, T.A.; Guastella, A.J. The Effect of Oxytocin Nasal Spray on Social Interaction Deficits Observed in Young Children with Autism: A Randomized Clinical Crossover Trial. Mol. Psychiatry 2016, 21, 1225–1231. [Google Scholar] [CrossRef] [Green Version]
- Parker, K.J.; Oztan, O.; Libove, R.A.; Sumiyoshi, R.D.; Jackson, L.P.; Karhson, D.S.; Summers, J.E.; Hinman, K.E.; Motonaga, K.S.; Phillips, J.M.; et al. Intranasal Oxytocin Treatment for Social Deficits and Biomarkers of Response in Children with Autism. Proc. Natl. Acad. Sci. USA 2017, 114, 8119–8124. [Google Scholar] [CrossRef]
- Quintana, D.S.; Guastella, A.J. An Allostatic Theory of Oxytocin. Trends Cogn. Sci. 2020, 24, 515–528. [Google Scholar] [CrossRef]
- Abramova, O.; Zorkina, Y.; Ushakova, V.; Zubkov, E.; Morozova, A.; Chekhonin, V. The Role of Oxytocin and Vasopressin Dysfunction in Cognitive Impairment and Mental Disorders. Neuropeptides 2020, 83, 102079. [Google Scholar] [CrossRef]
- Wirth, M.M. Hormones, Stress, and Cognition: The Effects of Glucocorticoids and Oxytocin on Memory. Adapt. Hum. Behav. Physiol. 2015, 1, 177–201. [Google Scholar] [CrossRef]
- Kapetaniou, G.E.; Reinhard, M.A.; Christian, P.; Jobst, A.; Tobler, P.N.; Padberg, F.; Soutschek, A. The Role of Oxytocin in Delay of Gratification and Flexibility in Non-Social Decision Making. eLife 2021, 10, e61844. [Google Scholar] [CrossRef]
- Friedman, N.P.; Robbins, T.W. The Role of Prefrontal Cortex in Cognitive Control and Executive Function. Neuropsychopharmacology 2022, 47, 72–89. [Google Scholar] [CrossRef]
- Knobloch, H.S.; Charlet, A.; Hoffmann, L.C.; Eliava, M.; Khrulev, S.; Cetin, A.H.; Osten, P.; Schwarz, M.K.; Seeburg, P.H.; Stoop, R.; et al. Evoked Axonal Oxytocin Release in the Central Amygdala Attenuates Fear Response. Neuron 2012, 73, 553–566. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Nakajima, M.; Ibañez-Tallon, I.; Heintz, N. A Cortical Circuit for Sexually Dimorphic Oxytocin-Dependent Anxiety Behaviors. Cell 2016, 167, 60–72.e11. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, M.; Görlich, A.; Heintz, N. Oxytocin Modulates Female Sociosexual Behavior through a Specific Class of Prefrontal Cortical Interneurons. Cell 2014, 159, 295–305. [Google Scholar] [CrossRef] [Green Version]
- Sha, Z.; Wager, T.D.; Mechelli, A.; He, Y. Common Dysfunction of Large-Scale Neurocognitive Networks Across Psychiatric Disorders. Biol. Psychiatry 2019, 85, 379–388. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.H. Executive Function and Developmental Disorders: The Flip Side of the Coin. Trends Cogn. Sci. 2012, 16, 454–457. [Google Scholar] [CrossRef]
- Hiser, J.; Koenigs, M. The Multifaceted Role of the Ventromedial Prefrontal Cortex in Emotion, Decision Making, Social Cognition, and Psychopathology. Biol. Psychiatry 2018, 83, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Lee, D. Decision Making: From Neuroscience to Psychiatry. Neuron 2013, 78, 233–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.; Sun, S.; Camilleri, J.A.; Eickhoff, S.B.; Yu, R. Better the Devil You Know than the Devil You Don’t: Neural Processing of Risk and Ambiguity. NeuroImage 2021, 236, 118109. [Google Scholar] [CrossRef]
- Patel, N.; Grillon, C.; Pavletic, N.; Rosen, D.; Pine, D.S.; Ernst, M. Oxytocin and Vasopressin Modulate Risk-Taking. Physiol. Behav. 2015, 139, 254–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leslie, M.; Leppanen, J.; Paloyelis, Y.; Nazar, B.P.; Treasure, J. The Influence of Oxytocin on Risk-Taking in the Balloon Analogue Risk Task among Women with Bulimia Nervosa and Binge Eating Disorder. J. Neuroendocrinol. 2019, 31, e12771. [Google Scholar] [CrossRef]
- Figner, B.; Weber, E.U. Who Takes Risks When and Why?: Determinants of Risk Taking. Curr. Dir. Psychol. Sci. 2011, 20, 211–216. [Google Scholar] [CrossRef]
- Zald, D.H.; Andreotti, C. Neuropsychological Assessment of the Orbital and Ventromedial Prefrontal Cortex. Neuropsychologia 2010, 48, 3377–3391. [Google Scholar] [CrossRef]
- Li, X.; Lu, Z.; D’Argembeau, A.; Ng, M.; Bechara, A. The Iowa Gambling Task in FMRI Images. Hum. Brain Mapp. 2009, 31, 410–423. [Google Scholar] [CrossRef] [Green Version]
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to Future Consequences Following Damage to Human Prefrontal Cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef]
- Rogers, R.D.; Owen, A.M.; Middleton, H.C.; Williams, E.J.; Pickard, J.D.; Sahakian, B.J.; Robbins, T.W. Choosing between Small, Likely Rewards and Large, Unlikely Rewards Activates Inferior and Orbital Prefrontal Cortex. J. Neurosci. 1999, 19, 9029–9038. [Google Scholar] [CrossRef] [Green Version]
- Brand, M.; Recknor, E.C.; Grabenhorst, F.; Bechara, A. Decisions under Ambiguity and Decisions under Risk: Correlations with Executive Functions and Comparisons of Two Different Gambling Tasks with Implicit and Explicit Rules. J. Clin. Exp. Neuropsychol. 2007, 29, 86–99. [Google Scholar] [CrossRef]
- Liebherr, M.; Schiebener, J.; Averbeck, H.; Brand, M. Decision Making under Ambiguity and Objective Risk in Higher Age—A Review on Cognitive and Emotional Contributions. Front. Psychol. 2017, 8, 2128. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.J.; Vassileva, J. Decision-Making Under Risk, but Not Under Ambiguity, Predicts Pathological Gambling in Discrete Types of Abstinent Substance Users. Front. Psychiatry 2018, 9, 239. [Google Scholar] [CrossRef]
- Macchia, A.; Zebhauser, P.T.; Salcedo, S.; Burum, B.; Gold, E.; Alonso-Alonso, M.; Pascual-Leone, A.; Gilbert, D.; Brem, A.-K. Divergent Effects of Oxytocin on “Mind-Reading” in Healthy Males. Cogn. Affect. Behav. Neurosci. 2022, 22, 112–122. [Google Scholar] [CrossRef]
- Buelow, M.T.; Barnhart, W.R. Test–Retest Reliability of Common Behavioral Decision Making Tasks. Arch. Clin. Neuropsychol. 2018, 33, 125–129. [Google Scholar] [CrossRef] [Green Version]
- De Wilde, B.; Bechara, A.; Sabbe, B.; Hulstijn, W.; Dom, G. Risky Decision-Making but Not Delay Discounting Improves during Inpatient Treatment of Polysubstance Dependent Alcoholics. Front. Psychiatry 2013, 4, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters-Wood, S.M.; Xiao, L.; Denburg, N.L.; Hernandez, M.; Bechara, A. Failure to Learn from Repeated Mistakes: Persistent Decision-Making Impairment as Measured by the Iowa Gambling Task in Patients with Ventromedial Prefrontal Cortex Lesions. J. Int. Neuropsychol. Soc. 2012, 18, 927–930. [Google Scholar] [CrossRef]
- Spengler, F.B.; Schultz, J.; Scheele, D.; Essel, M.; Maier, W.; Heinrichs, M.; Hurlemann, R. Kinetics and Dose Dependency of Intranasal Oxytocin Effects on Amygdala Reactivity. Biol. Psychiatry 2017, 82, 885–894. [Google Scholar] [CrossRef]
- JASP Team JASP (Version 0.15) Computer Software. 2022. Available online: https://jasp-stats.org/ (accessed on 1 July 2022).
- Van Doorn, J.; van den Bergh, D.; Böhm, U.; Dablander, F.; Derks, K.; Draws, T.; Etz, A.; Evans, N.J.; Gronau, Q.F.; Haaf, J.M.; et al. The JASP Guidelines for Conducting and Reporting a Bayesian Analysis. Psychon. Bull. Rev. 2021, 28, 813–826. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H.; Murai, T.; Fukuyama, H.; Hayashi, T.; Hanakawa, T. Functional Activity Related to Risk Anticipation during Performance of the Iowa Gambling Task. Neuroimage 2005, 24, 253–259. [Google Scholar] [CrossRef]
- Schutter, D.J.L.G.; Van Honk, J. Electrophysiological Ratio Markers for the Balance between Reward and Punishment. Brain Res. Cogn. Brain Res. 2005, 24, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Horstmann, A.; Villringer, A.; Neumann, J. Iowa Gambling Task: There Is More to Consider than Long-Term Outcome. Using a Linear Equation Model to Disentangle the Impact of Outcome and Frequency of Gains and Losses. Front. Neurosci. 2012, 6, 61. [Google Scholar] [CrossRef] [Green Version]
- Bayard, S.; Jacus, J.-P.; Raffard, S.; Gely-Nargeot, M.-C. Apathy and Emotion-Based Decision-Making in Amnesic Mild Cognitive Impairment and Alzheimer’s Disease. Behav. Neurol. 2014, 2014, e231469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurage, P.; Lannoy, S.; Dormal, V.; Blanco, M.; Trabut, J.-B. Clinical Usefulness of the Iowa Gambling Task in Severe Alcohol Use Disorders: Link with Relapse and Cognitive-Physiological Deficits. Alcohol. Clin. Exp. Res. 2018, 42, 2266–2273. [Google Scholar] [CrossRef] [PubMed]
- Lejuez, C.W.; Read, J.P.; Kahler, C.W.; Richards, J.B.; Ramsey, S.E.; Stuart, G.L.; Strong, D.R.; Brown, R.A. Evaluation of a Behavioral Measure of Risk Taking: The Balloon Analogue Risk Task (BART). J. Exp. Psychol. Appl. 2002, 8, 75–84. [Google Scholar] [CrossRef]
- Xu, X.; Li, J.; Chen, Z.; Kendrick, K.M.; Becker, B. Oxytocin Reduces Top-down Control of Attention by Increasing Bottom-up Attention Allocation to Social but Not Non-Social Stimuli—A Randomized Controlled Trial. Psychoneuroendocrinology 2019, 108, 62–69. [Google Scholar] [CrossRef]
- Zhuang, Q.; Zheng, X.; Yao, S.; Zhao, W.; Becker, B.; Xu, X.; Kendrick, K.M. Oral Administration of Oxytocin, Like Intranasal Administration, Decreases Top-Down Social Attention. Int. J. Neuropsychopharmacol. 2022, 25, 912–923. [Google Scholar] [CrossRef]
- Northoff, G.; Grimm, S.; Boeker, H.; Schmidt, C.; Bermpohl, F.; Heinzel, A.; Hell, D.; Boesiger, P. Affective Judgment and Beneficial Decision Making: Ventromedial Prefrontal Activity Correlates with Performance in the Iowa Gambling Task. Hum. Brain Mapp. 2006, 27, 572–587. [Google Scholar] [CrossRef]
- Clark, L.; Bechara, A.; Damasio, H.; Aitken, M.R.F.; Sahakian, B.J.; Robbins, T.W. Differential Effects of Insular and Ventromedial Prefrontal Cortex Lesions on Risky Decision-Making. Brain 2008, 131, 1311–1322. [Google Scholar] [CrossRef] [Green Version]
- Bishop, S.J.; Gagne, C. Anxiety, Depression, and Decision Making: A Computational Perspective. Annu. Rev. Neurosci. 2018, 41, 371–388. [Google Scholar] [CrossRef]
- Saperia, S.; Da Silva, S.; Siddiqui, I.; Agid, O.; Daskalakis, Z.J.; Ravindran, A.; Voineskos, A.N.; Zakzanis, K.K.; Remington, G.; Foussias, G. Reward-Driven Decision-Making Impairments in Schizophrenia. Schizophr. Res. 2019, 206, 277–283. [Google Scholar] [CrossRef]
- Luke, L.; Clare, I.C.H.; Ring, H.; Redley, M.; Watson, P. Decision-Making Difficulties Experienced by Adults with Autism Spectrum Conditions. Autism 2012, 16, 612–621. [Google Scholar] [CrossRef]
- Mowinckel, A.M.; Pedersen, M.L.; Eilertsen, E.; Biele, G. A Meta-Analysis of Decision-Making and Attention in Adults With ADHD. J. Atten. Disord. 2015, 19, 355–367. [Google Scholar] [CrossRef] [Green Version]
- Buelow, M.T.; Suhr, J.A. Construct Validity of the Iowa Gambling Task. Neuropsychol. Rev. 2009, 19, 102–114. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, H.; Tranel, D.; Damasio, A.R. The Iowa Gambling Task and the Somatic Marker Hypothesis: Some Questions and Answers. Trends Cogn. Sci. 2005, 9, 159–162. [Google Scholar] [CrossRef]
- Quintana, D.S.; Westlye, L.T.; Alnæs, D.; Kaufmann, T.; Mahmoud, R.A.; Smerud, K.T.; Djupesland, P.G.; Andreassen, O.A. Low-Dose Intranasal Oxytocin Delivered with Breath Powered Device Modulates Pupil Diameter and Amygdala Activity: A Randomized Controlled Pupillometry and FMRI Study. Neuropsychopharmacology 2019, 44, 306–313. [Google Scholar] [CrossRef] [Green Version]
- Martins, D.; Dipasquale, O.; Paloyelis, Y. Oxytocin Modulates Local Topography of Human Functional Connectome in Healthy Men at Rest. Commun. Biol. 2021, 4, 68. [Google Scholar] [CrossRef]
- Liu, P.; Lin, T.; Feifel, D.; Ebner, N.C. Intranasal Oxytocin Modulates the Salience Network in Aging. NeuroImage 2022, 253, 119045. [Google Scholar] [CrossRef]
- Kumar, J.; Iwabuchi, S.J.; Völlm, B.A.; Palaniyappan, L. Oxytocin Modulates the Effective Connectivity between the Precuneus and the Dorsolateral Prefrontal Cortex. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 567–576. [Google Scholar] [CrossRef]
- Lambert, B.; Declerck, C.H.; Boone, C.; Parizel, P.M. A Functional MRI Study on How Oxytocin Affects Decision Making in Social Dilemmas: Cooperate as Long as It Pays off, Aggress Only When You Think You Can Win. Horm. Behav. 2017, 94, 145–152. [Google Scholar] [CrossRef]
- Fellows, L.K.; Farah, M.J. The Role of Ventromedial Prefrontal Cortex in Decision Making: Judgment under Uncertainty or Judgment per Se? Cereb. Cortex 2007, 17, 2669–2674. [Google Scholar] [CrossRef] [PubMed]
- Kohlhoff, J.; Cibralic, S.; Hawes, D.J.; Eapen, V. Oxytocin Receptor Gene (OXTR) Polymorphisms and Social, Emotional and Behavioral Functioning in Children and Adolescents: A Systematic Narrative Review. Neurosci. Biobehav. Rev. 2022, 135, 104573. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
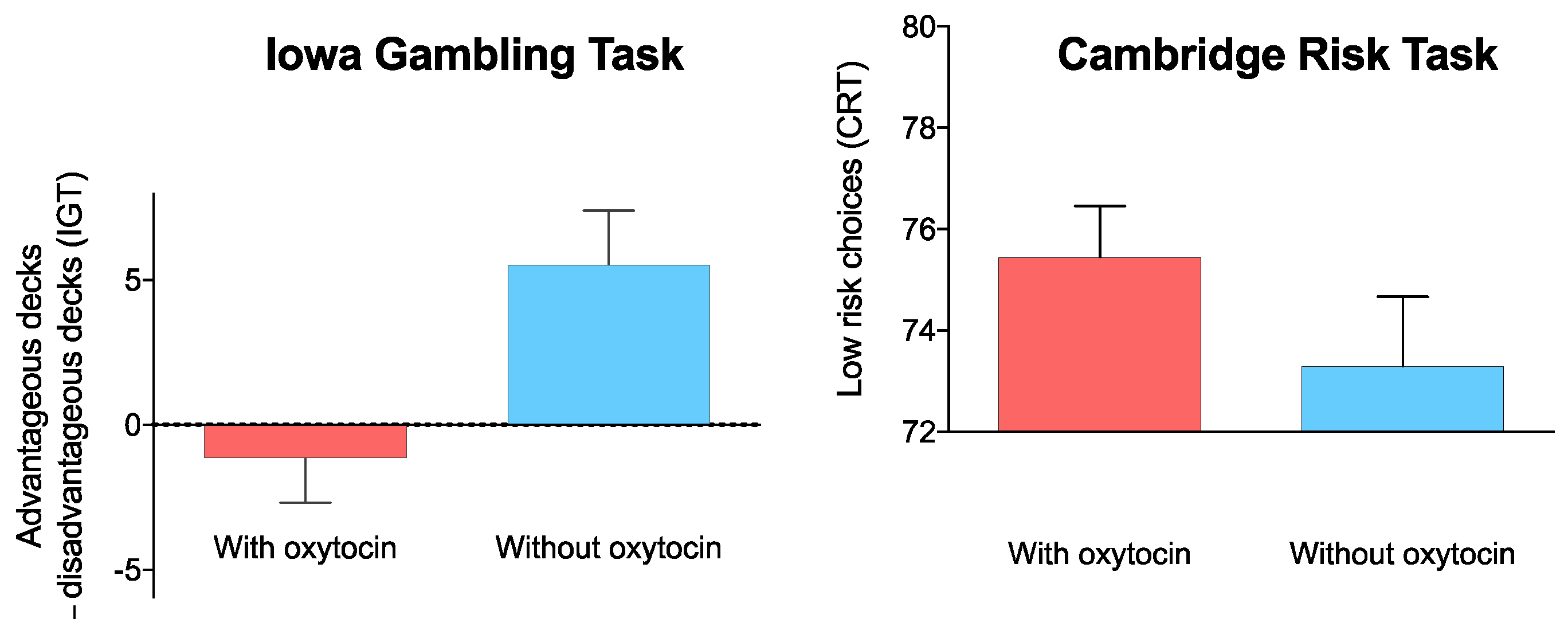
| OT Condition | Control Condition | p-Value | BF10 | |
|---|---|---|---|---|
| IGT (net score) | −1.16 ± 6.98 | 5.52 ± 8.51 | 0.004 | 10.76 |
| CRT (low-risk choices) * | 75.45 ± 4.50 | 73.30 ± 6.08 | 0.063 | 1.56 |
| CRT (deliberation time (millisec.)) | 1588.12 ± 520.86 | 1537.14 ± 536.85 | 0.705 | 0.248 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zebhauser, P.T.; Macchia, A.; Gold, E.; Salcedo, S.; Burum, B.; Alonso-Alonso, M.; Gilbert, D.T.; Pascual-Leone, A.; Brem, A.-K. Intranasal Oxytocin Modulates Decision-Making Depending on Outcome Predictability—A Randomized Within-Subject Controlled Trial in Healthy Males. Biomedicines 2022, 10, 3230. https://doi.org/10.3390/biomedicines10123230
Zebhauser PT, Macchia A, Gold E, Salcedo S, Burum B, Alonso-Alonso M, Gilbert DT, Pascual-Leone A, Brem A-K. Intranasal Oxytocin Modulates Decision-Making Depending on Outcome Predictability—A Randomized Within-Subject Controlled Trial in Healthy Males. Biomedicines. 2022; 10(12):3230. https://doi.org/10.3390/biomedicines10123230
Chicago/Turabian StyleZebhauser, Paul Theo, Ana Macchia, Edward Gold, Stephanie Salcedo, Bethany Burum, Miguel Alonso-Alonso, Daniel T. Gilbert, Alvaro Pascual-Leone, and Anna-Katharine Brem. 2022. "Intranasal Oxytocin Modulates Decision-Making Depending on Outcome Predictability—A Randomized Within-Subject Controlled Trial in Healthy Males" Biomedicines 10, no. 12: 3230. https://doi.org/10.3390/biomedicines10123230
APA StyleZebhauser, P. T., Macchia, A., Gold, E., Salcedo, S., Burum, B., Alonso-Alonso, M., Gilbert, D. T., Pascual-Leone, A., & Brem, A. -K. (2022). Intranasal Oxytocin Modulates Decision-Making Depending on Outcome Predictability—A Randomized Within-Subject Controlled Trial in Healthy Males. Biomedicines, 10(12), 3230. https://doi.org/10.3390/biomedicines10123230