
Systematic Review on Saliva Biomarkers in Patients Diagnosed with Morbus Alzheimer and Morbus Parkinson

 ,
,  and
and
Abstract
1. Introduction
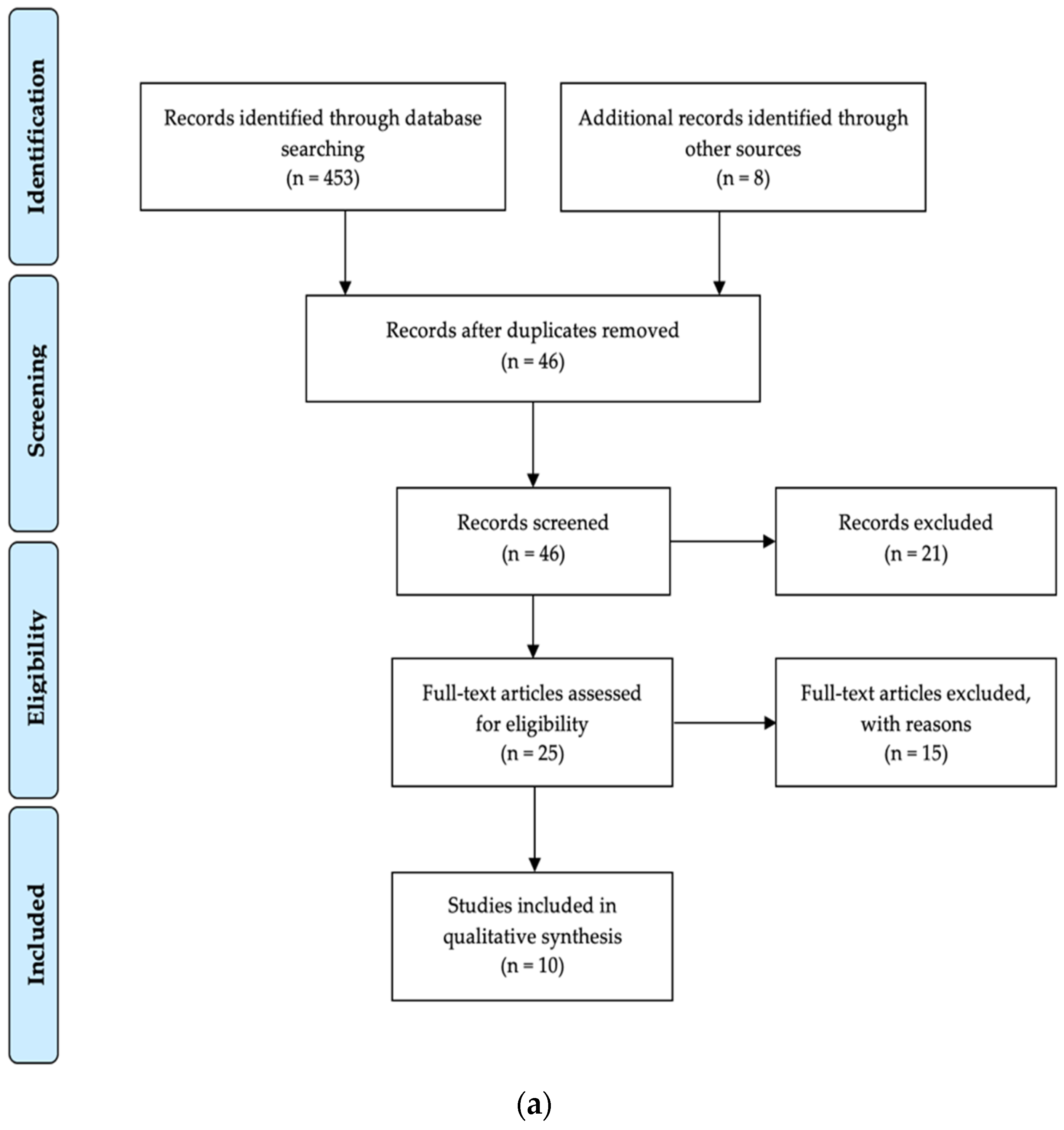
2. Materials and Methods
3. Results
3.1. Studies on Salivary Biomarkers Amyloid-β and Tau in AD Patients
3.1.1. Quality Assessment of Included Studies for Biomarkers Amyloid-β and Tau
3.1.2. Compilation, Characteristics, and Outcome of Included Studies for Biomarker Amyloid-β
3.1.3. Compilation, Characteristics, and Outcome of Included Studies for Biomarker Tau
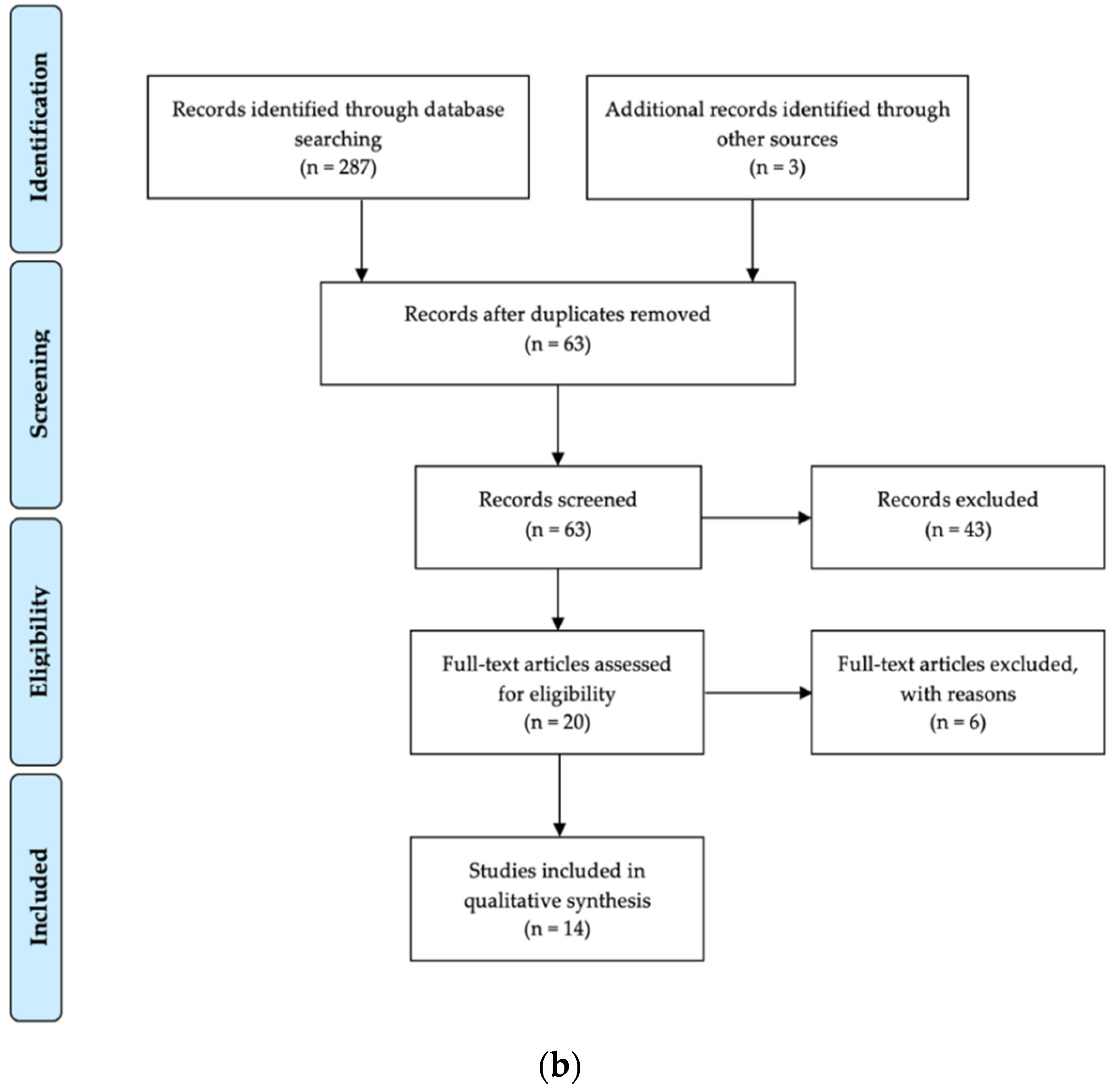
3.2. Studies on Salivary Biomarkers α-Synuclein and DJ-1 in PD Patients
3.2.1. Quality Assessment of Included Studies for Biomarkers α-Synuclein and DJ-1
3.2.2. Compilation, Characteristics, and Outcome of Included Studies for Biomarker DJ-1
3.2.3. Compilation, Characteristics, and Outcome of Included Studies for Biomarker α-Synuclein
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lane, C.A.; Hardy, J.; Schott, J.M. Alzheimer’s disease. Eur. J. Neurol. 2018, 25, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Scheltens, P.; Blennow, K.; Breteler, M.M.; de Strooper, B.; Frisoni, G.B.; Salloway, S.; Van der Flier, W.M. Alzheimer’s disease. Lancet 2016, 388, 505–517. [Google Scholar] [CrossRef]
- Garcia-Osta, A.; Alberini, C.M. Amyloid beta mediates memory formation. Learn. Mem. 2009, 16, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Green, A.J.; Harvey, R.J.; Thompson, E.J.; Rossor, M.N. Increased tau in the cerebrospinal fluid of patients with frontotemporal dementia and Alzheimer’s disease. Neurosci. Lett. 1999, 259, 133–135. [Google Scholar] [CrossRef]
- Blennow, K.; Hampel, H. CSF markers for incipient Alzheimer’s disease. Lancet Neurol. 2003, 2, 605–613. [Google Scholar] [CrossRef]
- de Lau, L.M.; Breteler, M.M. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef]
- Schneider, R.B.; Iourinets, J.; Richard, I.H. Parkinson’s disease psychosis: Presentation, diagnosis and management. Neurodegener. Dis. Manag. 2017, 7, 365–376. [Google Scholar] [CrossRef]
- Kalia, L.V.; Lang, A.E. Parkinson’s disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef]
- Bonifati, V.; Rizzu, P.; van Baren, M.J.; Schaap, O.; Breedveld, G.J.; Krieger, E.; Dekker, M.C.; Squitieri, F.; Ibanez, P.; Joosse, M.; et al. Mutations in the DJ-1 gene associated with autosomal recessive early-onset parkinsonism. Science 2003, 299, 256–259. [Google Scholar] [CrossRef]
- Junn, E.; Jang, W.H.; Zhao, X.; Jeong, B.S.; Mouradian, M.M. Mitochondrial localization of DJ-1 leads to enhanced neuroprotection. J. Neurosci. Res. 2009, 87, 123–129. [Google Scholar] [CrossRef]
- Shendelman, S.; Jonason, A.; Martinat, C.; Leete, T.; Abeliovich, A. DJ-1 is a redox-dependent molecular chaperone that inhibits alpha-synuclein aggregate formation. PLoS Biol. 2004, 2, e362. [Google Scholar] [CrossRef] [PubMed]
- Ashton, N.J.; Ide, M.; Zetterberg, H.; Blennow, K. Salivary Biomarkers for Alzheimer’s Disease and Related Disorders. Neurol. Ther. 2019, 8, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Farah, R.; Haraty, H.; Salame, Z.; Fares, Y.; Ojcius, D.M.; Said Sadier, N. Salivary biomarkers for the diagnosis and monitoring of neurological diseases. Biomed. J. 2018, 41, 63–87. [Google Scholar] [CrossRef]
- Reale, M.; Gonzales-Portillo, I.; Borlongan, C.V. Saliva, an easily accessible fluid as diagnostic tool and potent stem cell source for Alzheimer’s Disease: Present and future applications. Brain Res. 2020, 1727, 146535. [Google Scholar] [CrossRef]
- Schepici, G.; Silvestro, S.; Trubiani, O.; Bramanti, P.; Mazzon, E. Salivary Biomarkers: Future Approaches for Early Diagnosis of Neurodegenerative Diseases. Brain Sci. 2020, 10, 245. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA-Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Pareja, F.; Antequera, D.; Vargas, T.; Molina, J.A.; Carro, E. Saliva levels of Abeta1-42 as potential biomarker of Alzheimer’s disease: A pilot study. BMC Neurol. 2010, 10, 108. [Google Scholar] [CrossRef]
- Shi, M.; Sui, Y.T.; Peskind, E.R.; Li, G.; Hwang, H.; Devic, I.; Ginghina, C.; Edgar, J.S.; Pan, C.; Goodlett, D.R.; et al. Salivary tau species are potential biomarkers of Alzheimer’s disease. J. Alzheimers Dis. 2011, 27, 299–305. [Google Scholar] [CrossRef]
- Kim, C.B.; Choi, Y.Y.; Song, W.K.; Song, K.B. Antibody-based magnetic nanoparticle immunoassay for quantification of Alzheimer’s disease pathogenic factor. J. Biomed. Opt. 2014, 19, 051205. [Google Scholar] [CrossRef]
- Lau, H.C.; Lee, I.K.; Ko, P.W.; Lee, H.W.; Huh, J.S.; Cho, W.J.; Lim, J.O. Non-invasive screening for Alzheimer’s disease by sensing salivary sugar using Drosophila cells expressing gustatory receptor (Gr5a) immobilized on an extended gate ion-sensitive field-effect transistor (EG-ISFET) biosensor. PLoS One 2015, 10, e0117810. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Guo, J.P.; Kennedy, K.; McGeer, E.G.; McGeer, P.L. A Method for Diagnosing Alzheimer’s Disease Based on Salivary Amyloid-β Protein 42 Levels. J. Alzheimers Dis. 2017, 55, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- McGeer, P.L.; Guo, J.P.; Lee, M.; Kennedy, K.; McGeer, E.G. Alzheimer’s Disease Can Be Spared by Nonsteroidal Anti-Inflammatory Drugs. J. Alzheimers Dis. 2018, 62, 1219–1222. [Google Scholar] [CrossRef]
- Sabbagh, M.N.; Shi, J.; Lee, M.; Arnold, L.; Al-Hasan, Y.; Heim, J.; McGeer, P. Salivary beta amyloid protein levels are detectable and differentiate patients with Alzheimer’s disease dementia from normal controls: Preliminary findings. BMC Neurol. 2018, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Pekeles, H.; Qureshi, H.Y.; Paudel, H.K.; Schipper, H.M.; Gornistky, M.; Chertkow, H. Development and validation of a salivary tau biomarker in Alzheimer’s disease. Alzheimers Dement. (Amst.) 2019, 11, 53–60. [Google Scholar] [CrossRef]
- Ashton, N.J.; Ide, M.; Schöll, M.; Blennow, K.; Lovestone, S.; Hye, A.; Zetterberg, H. No association of salivary total tau concentration with Alzheimer’s disease. Neurobiol. Aging 2018, 70, 125–127. [Google Scholar] [CrossRef]
- Tvarijonaviciute, A.; Zamora, C.; Ceron, J.J.; Bravo-Cantero, A.F.; Pardo-Marin, L.; Valverde, S.; Lopez-Jornet, P. Salivary biomarkers in Alzheimer’s disease. Clin. Oral Investig. 2020, 24, 3437–3444. [Google Scholar] [CrossRef]
- Devic, I.; Hwang, H.; Edgar, J.S.; Izutsu, K.; Presland, R.; Pan, C.; Goodlett, D.R.; Wang, Y.; Armaly, J.; Tumas, V.; et al. Salivary α-synuclein and DJ-1: Potential biomarkers for Parkinson’s disease. Brain 2011, 134, e178. [Google Scholar] [CrossRef]
- Kang, W.Y.; Yang, Q.; Jiang, X.F.; Chen, W.; Zhang, L.Y.; Wang, X.Y.; Zhang, L.N.; Quinn, T.J.; Liu, J.; Chen, S.D. Salivary DJ-1 could be an indicator of Parkinson’s disease progression. Front. Aging Neurosci. 2014, 6, 102. [Google Scholar] [CrossRef]
- Stewart, T.; Sui, Y.T.; Gonzalez-Cuyar, L.F.; Wong, D.T.; Akin, D.M.; Tumas, V.; Aasly, J.; Ashmore, E.; Aro, P.; Ginghina, C.; et al. Cheek cell-derived α-synuclein and DJ-1 do not differentiate Parkinson’s disease from control. Neurobiol. Aging 2014, 35, 418–420. [Google Scholar] [CrossRef][Green Version]
- Al-Nimer, M.S.; Mshatat, S.F.; Abdulla, H.I. Saliva α-Synuclein and A High Extinction Coefficient Protein: A Novel Approach in Assessment Biomarkers of Parkinson’s Disease. N. Am. J. Med. Sci. 2014, 6, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Masters, J.M.; Noyce, A.J.; Warner, T.T.; Giovannoni, G.; Proctor, G.B. Elevated salivary protein in Parkinson’s disease and salivary DJ-1 as a potential marker of disease severity. Parkinsonism Relat. Disord. 2015, 21, 1251–1255. [Google Scholar] [CrossRef]
- Kang, W.; Chen, W.; Yang, Q.; Zhang, L.; Zhang, L.; Wang, X.; Dong, F.; Zhao, Y.; Chen, S.; Quinn, T.J.; et al. Salivary total α-synuclein, oligomeric α-synuclein and SNCA variants in Parkinson’s disease patients. Sci. Rep. 2016, 6, 28143. [Google Scholar] [CrossRef] [PubMed]
- Vivacqua, G.; Latorre, A.; Suppa, A.; Nardi, M.; Pietracupa, S.; Mancinelli, R.; Fabbrini, G.; Colosimo, C.; Gaudio, E.; Berardelli, A. Abnormal Salivary Total and Oligomeric Alpha-Synuclein in Parkinson’s Disease. PLoS One 2016, 11, e0151156. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.G.; Andrews, H.; Amara, A.; Naito, A.; Alcalay, R.N.; Shaw, L.M.; Taylor, P.; Xie, T.; Tuite, P.; Henchcliffe, C.; et al. Cerebrospinal fluid, plasma, and saliva in the BioFIND study: Relationships among biomarkers and Parkinson’s disease Features. Mov. Disord. 2018, 33, 282–288. [Google Scholar] [CrossRef]
- Su, L.; Chen, Y.; Cai, Y.; Lou, A.; Ye, Q.; Chen, X. Salivary α-synuclein and DJ-1 for the value of the diagnosis of Parkinson disease. Chin. J. Nerv. Ment. Dis. 2018, 12, 1–5. [Google Scholar]
- Cao, Z.; Wu, Y.; Liu, G.; Jiang, Y.; Wang, X.; Wang, Z.; Feng, T. α-Synuclein in salivary extracellular vesicles as a potential biomarker of Parkinson’s disease. Neurosci. Lett. 2019, 696, 114–120. [Google Scholar] [CrossRef]
- Cao, Z.; Wu, Y.; Liu, G.; Jiang, Y.; Wang, X.; Wang, Z.; Feng, T. Differential Diagnosis of Multiple System Atrophy-Parkinsonism and Parkinson’s Disease Using α-Synuclein and External Anal Sphincter Electromyography. Front. Neurol. 2020, 11, 1043. [Google Scholar] [CrossRef] [PubMed]
- Vivacqua, G.; Suppa, A.; Mancinelli, R.; Belvisi, D.; Fabbrini, A.; Costanzo, M.; Formica, A.; Onori, P.; Fabbrini, G.; Berardelli, A. Salivary alpha-synuclein in the diagnosis of Parkinson’s disease and Progressive Supranuclear Palsy. Parkinsonism Relat. Disord. 2019, 63, 143–148. [Google Scholar] [CrossRef]
- Shaheen, H.; Sobhy, S.; El Mously, S.; Aboumira, M.; Mansour, M. Salivary alpha-synuclein (total and oligomeric form): Potential biomarkers in Parkinson’s disease. Egypt. J. Neurol. Psychiatry Neurosurg. 2020, 56, 22. [Google Scholar] [CrossRef]
- Chahine, L.M.; Beach, T.G.; Brumm, M.C.; Adler, C.H.; Coffey, C.S.; Mosovsky, S.; Caspell-Garcia, C.; Serrano, G.E.; Munoz, D.G.; White, C.L., 3rd; et al. In vivo distribution of α-synuclein in multiple tissues and biofluids in Parkinson disease. Neurology 2020, 95, e1267–e1284. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Espejo, E.; Rodríguez de Fonseca, F.; Suárez, J.; Tolosa, E.; Vilas, D.; Aldecoa, I.; Berenguer, J.; Damas-Hermoso, F. Native α-Synuclein, 3-Nitrotyrosine Proteins, and Patterns of Nitro-α-Synuclein-Immunoreactive Inclusions in Saliva and Submandibulary Gland in Parkinson’s Disease. Antioxidants 2021, 10, 715. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Su, J.; Sun, Y.; Feng, Y.; Shen, N.; Li, B.; Liang, Y.; Yang, X.; Wu, H.; Zhang, H.; et al. Significant Upregulation of Alzheimer’s β-Amyloid Levels in a Living System Induced by Extracellular Elastin Polypeptides. Angew. Chem. Int. Ed. Engl. 2019, 58, 18703–18709. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Ma, C.; Li, J.; Sun, Y.; Ye, F.; Liu, K.; Zhang, H. Extracellular Matrix Proteins Involved in Alzheimer’s Disease. Chemistry 2020, 26, 12101–12110. [Google Scholar] [CrossRef]
- Pluta, R.; Kis, J.; Januszewski, S.; Jablonski, M.; Czuczwar, S.J. Cross-Talk between Amyloid, Tau Protein and Free Radicals in Post-Ischemic Brain Neurodegeneration in the Form of Alzheimer’s Disease Proteinopathy. Antioxidants 2022, 11, 146. [Google Scholar] [CrossRef]
- Szychowski, K.A.; Skóra, B.; Wójtowicz, A.K. Elastin-Derived Peptides in the Central Nervous System: Friend or Foe. Cell. Mol. Neurobiol. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study (Author/Year) | Clinical Diagnosis | Methods | Population Characteristics (Population Size, Sex, Age (Mean/Range)) |
|---|---|---|---|
| 1. Bermejo-Pareja et al., 2010 [18] | AD characterized using DSM-IV and NINCDS-ADRDA; vascular dementia excluded using DSM-III-R | MMSE MRT and/or CT Extensive biochemical measurements ApoE genotyping | AD (n = 70): Sex: m 21/f 49 Age: 77.20 years (60–91) Disease duration: 2.56 years (0–12) MMSE: 17 (4–28) Mild AD (n = 29) Moderate AD (n = 24) Severe AD (n = 17) Control (n = 56): Sex: m 17/f 39 Age: 74.35 years (64–85) Sex-, age-, and ethnicity-matched control |
| 2. Shi et al., 2011 [19] | AD characterized using NINDS-ADRDA | MMSE CDRS | AD (n = 21): Sex: m 10/f 11 Age: 68.80 years (52–85) Disease duration: 4.4 years (2–10) CDRS: 0.05 (0–0.5) MMSE: 19.2 (4–29) Control (n = 38): Sex: m 19/f 19 Age: 69.00 years (40–88) CDRS: 1.05 (0.5–2) MMSE: 29.4 (27–30) |
| 3. Kim et al., 2014 [20] | NS | MMSE | AD (n = 28): Sex, age, and ethnicity NS Mild AD (MCI) (n = NS) Severe AD (n = NS) Control (n = 17): Sex, age, and ethnicity NS |
| 4. Lau et al., 2015 [21] | NS | MMSE CDR-SOB | AD (n = 20): Sex: m 8/f 12 Age: 72.50 ± 7.68 years MMSE: 18.15 ± 5.4 CDR-SOB: 6.25 ± 2.67 Control (n = 20): Sex: m 9/f 11 Age: 66.10 ± 7.79 years MMSE: 28.7 ± 1.11 CDR-SOB: 0.23 ± 0.25 |
| 5. Lee et al., 2017 [22] | NS | NS | AD (n = 7): Sex: m 3/f 4 Age: 76.86 years (57–86) AD family history (n = 3) Pre-AD (n = 3): Sex: m 0/f 3 Age: 54.33 years (51–60) AD family history (n = 3) Control (n = 26): Sex: m 17/f 9 Age: 54.62 years (19–92) AD family history (n = 9) |
| 6. McGeer et al., 2018 [23] | NS | NS | AD (n = 23): Sex: m 8/f 15 Age: 74.14 ± 11.31 years Control (n = 31): Sex: m 20/f 11 Age: 57.06 ± 21.73 years High control (n = 6): (predicted risk for AD) Sex: m 3/f 3 Age: 69.00 ± 8.97 years Low control (n = 25): Sex: m 17/f 8 Age: 54.20 ± 23.0 years |
| 7. Sabbagh et al., 2018 [24] | NIA-AA Exclusion of subjects with medical history of major systemic diseases that affect cognitive function | MMSE | AD (n = 15): Sex: m 7/f 8 Age: 77.8 ± 1.8 years MMSE: 19.0 ± 1.3 Control (n = 7): Sex: m 2/f 5 Age: 60.4 ± 4.7 years MMSE: 29.0 ± 0.4 |
| 8. Pekeles et al., 2019 [25] | NIA-AA | Clock-drawing test MoCA WMS | AD (n = 46): Sex: m 24/f 22 Age: 80 years (median), 9 (IQR) MCI (n = 55): Sex: m 23/32 Age: 78 years (median), 14 (IQR) Control (n = 47): Sex: m 15/f 32 Age: 73 years (median), 6 (IQR) MoCA ≥ 25 |
| 9. Ashton et al., 2018 [26] | NS | CDR MMSE MRI APOE genotyping | AD (n = 53): Sex: m 23/f 30 Age: 81.4 ± 6.6 years CDR: 0.89 ± 0.82 MMSE: 22.3 ± 5.7 MCI (n = 68): Sex: m 33/f 35 Age: 79.8 ± 7.4 years CDR: 0.48 ± 0.14 MMSE: 26.8 ± 2.3 Control (n = 160): Sex: m 66/f 94 Age: 78.0 ± 6.7 years CDR: 0.15 ± 0.24 MMSE: 28.9 ± 1.1 |
| 10. Tvarijonaviciute et al., 2020 [27] | AD characterized using GDS | Controls characterized using MMSE | AD (n = 69): Sex: NS Age: 75.6 ± 7.2 years MMSE: NS Control (n = 83): Sex: NS Age: 75.6 ± 7.2 years MMSE: ≥ 28 |
| Study (Author/Year) | Biomarker Tested | Biomarker/ Concentration (Saliva) | Detection Method (Saliva) | Body Fluids Tested |
|---|---|---|---|---|
| 1. Bermejo- Pareja et al., 2010 [18] | Aβ42 | Aβ42 markedly elevated in AD patients compared to controls: AD: 6.81 ± 20.04 pg/mL Mild AD: 7.67 ± 16.25 pg/mL Moderate AD: 11.70 ± 34.76 pg/mL Severe AD: 3.03 ± 3.49 pg/mL Control: 2.89 ± 4.96 pg/mL No significant changes with Aβ42 in plasma | ELISA | Saliva Plasma |
| Aβ40 | Aβ40 unaltered in AD patients compared to controls: AD: 22.3 ± 4.88 pg/mL Mild AD: 21.87 ± 5.7 pg/mL Moderate AD: 21.5 ± 4.17 pg/mL Severe AD: 23.92 ± 4.55 pg/mL Control: 20.82 ± 5.55 pg/mL No significant changes with Aβ40 in plasma | ELISA | Saliva Plasma | |
| Aβ42/ Aβ40 ratio | Aβ42/Aβ40 ratio is moderately (but non-significantly) elevated in patients with mild and moderate AD compared to controls | ELISA | Saliva Plasma | |
| 2. Shi et al., 2011 [19] | Aβ42 | Data cannot be extracted Aβ42 not detected in the cohort, neither with Luminex nor with IP/MS | Luminex IP/MS | Saliva |
| t-tau | Data cannot be extracted tau detected with IP/MS in saliva t-tau unaltered in patients with AD compared to controls | Luminex IP/MS | Saliva | |
| p-tau | Data cannot be extracted p-tau markedly elevated in patients with AD compared to controls | Luminex | Saliva | |
| p-tau/ t-tau ratio | Data cannot be extracted p-tau/t-tau ratio significantly elevated in patients with AD compared to controls | Luminex | Saliva | |
| 3. Kim et al., 2014 [20] | Aβ42 | Data cannot be extracted Aβ42 significantly elevated in patients with severe AD compared to patients with mild AD or controls | MIA ELISA | Saliva |
| Aβ40 | Data cannot be extracted Aβ40 non-significantly elevated in patients with severe AD compared to patients with mild AD or controls | MIA ELISA | Saliva | |
| Aβ42/Aβ40 ratio | Data cannot be extracted Aβ42/Aβ40 ratio is not elevated in patients with severe or mild AD compared to controls Aβ42/Aβ40 ratio is elevated in patients with severe AD compared to patients with mild AD (significance unclear) | MIA | Saliva | |
| 4. Lau et al., 2015 [21] | Aβ42 | Data cannot be extracted Aβ42 not detected in salivary samples of patients with AD or controls | ELISA | Saliva |
| t-tau | Data cannot be extracted t-tau unaltered in patients with AD compared to controls | ELISA | Saliva | |
| p-tau | Data cannot be extracted p-tau moderately (but non-significantly) elevated in patients with AD compared to controls | ELISA | Saliva | |
| p-tau/ t-tau ratio | Data cannot be extracted p-tau/t-tau ratio moderately (but non-significantly) elevated in patients with AD compared to controls | ELISA | Saliva | |
| 5. Lee et al., 2017 [22] | Aβ42 | Aβ42 significantly elevated in AD patients compared to controls Aβ42 markedly elevated in pre-AD patients compared to controls Aβ42 unaltered in AD patients compared to pre-AD patients AD: 59.07 ± 6.33 pg/mL Pre-AD: 56.14 ± 7.12 pg/mL Control: 22.06 ± 0.41 pg/ml | ELISA | Saliva |
| 6. McGeer et al., 2018 [23] | Aβ42 | Aβ42 significantly elevated in AD patients compared to controls and low controls Aβ42 unaltered in AD patients compared to high controls AD: 53.95 ± 2.24 pg/mL Control: 26.55 ± 1.85 pg/mL High control: 45.96 ± 3.01 pg/mL Low control: 21.54 ± 0.19 pg/mL | ELISA | Saliva |
| 7. Sabbagh et al., 2018 [24] | Aβ42 | Aβ42 significantly elevated in AD patients compared to controls AD: 51.7 ± 1.6 pg/mL Control: 21.1 ± 0.3 pg/mL | ELISA | Saliva |
| 8. Pekeles et al., 2019 [25] | p-tau/ t-tau ratio | Data cannot be extracted p-tau/t-tau ratio significantly elevated in patients with AD compared to controls (for three of the four phosphorylation sites tested) | Western blot (for saliva) ELISA (for CSF) | Saliva CSF |
| 9. Ashton et al., 2018 [26] | t-tau | t-tau non-significantly altered among AD, MCI, and controls AD: 12.3 ng/L MCI: 9.8 ng/L Control: 9.6 ng/L | SIMOA immunoassay | Saliva |
| 10. Tvarijonaviciute et al., 2020 [27] | Aβ40 | Aβ40 non-significantly elevated in AD patients compared to controls AD: 21.98 ± 16.94 pg/mL Control: 19.97 ± 6.35 pg/mL | MILLIPLEX® MAP | Saliva |
| Aβ42 | Aβ42 non-significantly decreased in AD patients compared to controls AD: 3.15 ± 0.72 pg/mL Control: 3.57 ± 0.93 pg/mL | MILLIPLEX® MAP | Saliva | |
| t-tau | t-tau unaltered in patients with AD compared to controls AD: 21.57 ± 22.11 pg/mL Control: 21.15 ± 16.58 pg/mL | MILLIPLEX® MAP | Saliva | |
| p-tau | p-tau moderately (but non-significantly) decreased in patients with AD compared to controls AD: 40.33 ± 42.95 pg/mL Control: 42.5 ± 38.35 pg/ml | MILLIPLEX® MAP | Saliva |
| Study (Author/Year) | Clinical Diagnosis | Methods | Population Characteristics (Population Size, Sex, Age (Mean/Range)) |
|---|---|---|---|
| 1. Devic et al., 2011 [28] | UK PD Society Brain Bank clinical diagnostic criteria for PD as determined by a movement disorder specialist | UPDRS | PD (n = 24): Sex: m 17/f 7 Age: 63.5 ± 11.3 years Duration of disease: 8.5 ± 6.4 years Patients with UPDRS III scores: 18/24 Control (n = 25): Sex: m 11/f 14 Age: 58.0 ± 10.4 years |
| 2a. Kang et al., 2014 (pilot study) [29] | UK PD Society Brain Bank clinical diagnostic criteria for PD as determined by at least two senior movement disorder specialists | HAMD-17 MMSE REM Sleep Behavior Disorder Scale SCOPA-AUT UPDRS III HY Scale | PD (n = 74): Sex: m 50/f 24 Age: 61.8 ± 7.8 years Duration of disease: 4.36 ± 3.59 years UPDRS III: 17.63 ± 11.69 Control (n = 12): Sex: m 6/f 6 Age: 55.5 ± 6.11 years |
| 2b. Kang et al., 2014 (large cohort study) [29] | UK PD Society Brain Bank clinical diagnostic criteria for PD as determined by at least two senior movement disorder specialists | HAMD-17 MMSE REM Sleep Behavior Disorder Scale SCOPA-AUT UPDRS III HY Scale | PD (n = 285): Sex: m 171/f 114 Age: 63.34 ± 9.11 years UPDRS III: 23.8 ± 15.7 Control (n = 91): Sex: m 59/f 32 Age: 61.59 ± 10.61 years |
| 3. Stewart et al., 2014 [30] | UK PD Society Brain Bank clinical diagnostic criteria for PD as determined by a movement disorder specialist | UPDRS | PD (n = 24): Sex: m 17/f 7 Age: 63.5 ± 11.3 years Duration of disease: 8.5 ± 6.4 years Patients with UPDRS III scores: 18/24 (see Devic et al., 2011) Control (n = 25): Sex: m 11/f 14 Age: 58.0 ± 10.4 years (see Devic et al., 2011) |
| 4. Al-Nimer et al., 2014 [31] | UK PD Society Brain Bank clinical diagnostic criteria for PD | MDS-UPDRS | PD (n = 20): Sex: m 16/f 4 Age: 64.4 ± 10.6 years Duration of disease: 6.55 ± 6.83 years Family history: 6 Control (n = 20): Sex: m 18/f 2 Age: 65.4 ± 8.2 years |
| 5. Masters et al., 2015 [32] | Queen Square Brain Bank clinical diagnostic criteria for PD as determined by two trained clinicians | MDS-UPDRS ACB | PD (n = 16) Control (n = 22) (further details not available) |
| 6. Kang et al., 2016 [33] | UK PD Society Brain Bank clinical diagnostic criteria for PD | UPDRS III Genotyping for SNCA variants | PD (n = 201): Sex: m 122/f 79 Age: 63.18 ± 9.67 years Control (n = 67): Sex: m 41/f 26 Age: 61.04 ± 10.01 years |
| 7. Vivacqua et al., 2016 [34] | Queen Square Brain Bank clinical diagnostic criteria for PD | BDI-II HY Scale MDS-UPDRS MoCA FAB LEDD | PD (n = 60): Sex: m 31/f 29 Age: 66.3 ± 8.78 years MoCA score > 18 FAB score > 12 Control (n = 40): Sex: m 22/f 18 Age: 68.3 ± 7.9 years |
| 8. Goldman et al., 2018 [35] | UK PD Society Brain Bank clinical diagnostic criteria for PD; atypical or secondary parkinsonian syndromes excluded | HY Scale MDS-UPDRS MoCA | PD (n = 115): Sex: m 72/f 43 Age: 68.24 ± 6.40 years Duration of disease: 8.34 ± 3.09 years HY stage: 2.18 ± 0.67 MoCA score: 26.76 ± 2.56 UPDRS III score: 39.13 ± 13.19 Control (n = 88): Sex: m 59/f 29 Age: 65.64 ± 7.36 years MoCA score ≥ 26 No first-degree PD family members |
| 9. Su et al., 2018 [36] | International Parkinson and Movement Disorder Society (The Movement Disorder Society) | HY Scale MDP-UPDRS-II/III SS-12 MMSE MoCA | PD (n = 27): Sex: m 15/f 12 Age: 61.52 ± 9.57 years HY stage: 1–3 UPDRS II score: 10.93 ± 5.35 UPDRS III score: 25.52 ± 11.34 SS-12: 4.70 ± 2.89 Control (n = 27): Sex: m 15/f 12 Age: 58.37 ± 9.85 years |
| 10a. Cao et al., 2019 [37] | UK PD Society Brain Bank clinical diagnostic criteria for PD as diagnosed by two expert professional neurologists | HY Scale UPDRS-III | PD (n = 74): Sex: m 40 /f 34 Age: 59.62 ± 8.57 years HY stage: 2.5 (2–3) UDPRS-III: 38.40 ± 19.39 Control (n = 60): Sex: m 26/f 34 Age: 58.75 ± 9.85 years |
| 10b. Cao et al., 2020 [38] | UK PD Society Brain Bank clinical diagnostic criteria for PD as diagnosed by two expert professional neurologists | HY Scale HAMA HAMD MMSE MoCA RBDSQ | PD (n = 26): Sex: m 12/f 14 Age: 57.31 ± 7.78 years Duration of disease: 2.64 ± 1.19 years HY stage: 2.50 ± 0.62 UPDRS III score: 40.77 ± 16.00 MSA-P (n = 16): Sex: m 9/f 7 Age: 56.82 ± 6.45 years Duration of disease: 3.06 ± 1.73 years HY stage: 2.81 ± 0.75 UPDRS III score: 42.75 ± 18.87 |
| 11. Vivacqua et al., 2019 [39] | Queen Square Brain Bank clinical diagnostic criteria for PD as determined by two trained clinicians | FAB HY Scale LEDD MDS-UPDRS MoCA PSPRS | PD (n = 112): Sex: m 59/f 53 Age: 69.01 ± 11.16 years Duration of disease: 6.29 ± 5.03 years FAB: 16.376 ± 1.918 HY stage: 2.11 ± 0.74 MDS-UPDRS score: 38.06 ± 21.06 MoCA: 26.60 ± 3.284 PSP (n = 22): Sex: m 12/10 Age: 68.84 ± 6.16 years Duration of disease: 3.07 ± 1.31 years FAB: 14.153 ± 1.918 HY stage: 3.19 ± 0.15 MDS-UPDRS score: 32.384 ± 11.2 MoCA: 22.538 ± 3.9 PSPRS: 32.61 ± 11.5 Control (n = 90): Sex: m 53/f 37 Age: 62.09 ± 15.08 years |
| 12. Shaheen et al., 2020 [40] | UK PD Society Brain Bank clinical diagnostic criteria for PD | BRS HY Scale LEDD UPDRS | PD (n = 25): Sex: m 15/f 10 Age: 60.1 ± 5.6 years Duration of disease: 0.5 to 10.0 years UPDRS III score: 29.9 ± 11.1 HY stage: 2.08 ± 0.6 Control (n = 15): Sex: m 10/f 5; Age: 60.0 ± 6.7 years Age- and sex-matched control |
| 13. Chahine et al., 2020 [41] | NS | HY Scale MDS-UPDRS MoCA RBDSQR SCOPA-AUT | PD (n = 59): Sex: m 41/f 18 Age: 63.1 ± 8.6 years Duration of disease: 4.81 ± 4.58 UPDRS III score: 26.4 ± 11.9 Early PD (n = 18) Moderate PD (n = 20) Advanced PD (n = 21) Control (n = 21): Sex: m 9/f 12 Age: 61.0 ± 6.3 years UPDRS III score: 1.1 ± 2.3 |
| 14. Fernández-Espejo et al., 2021 [42] | UK PD Society Brain Bank clinical diagnostic criteria for PD SPECT scans | HY Scale MDS-UPDRS Modified Schwab and England ADL | PD (n = 45): Sex: m 27/f 18 Age: 61.4 ± 18.5 years Duration of disease: 9.9 ± 6.8 HY stage: 2.1 ± 0.8 Modified Schwab and England ADL: 86 ± 25 MDS-UPDRS III score: 24 ± 12 MDS-UPDRS IV score: 1.2 ± 2.4 MDS-UPDRS (I-III)) score: 37.2 ± 20 Control (n = 30): Sex: m 18/f 12 Age: 59.6 ± 11 years |
| Study (Author/Year) | Biomarker Tested | Biomarker/ Concentration (Saliva) | Detection Method (Saliva) | Body Fluids Tested |
|---|---|---|---|---|
| 1. Devic et al., 2011 [28] | Total α-Syn | Total α-Syn markedly (but non-significantly) reduced in PD compared to controls: PD: 70 ± 80 pg/mL Control: 110 ± 130 pg/mL α-Syn depletion markedly correlated (but non-significantly) with UPDRS scores (i.e., disease severity) | Luminex IP/Western blot | Saliva |
| DJ-1 | DJ-1 moderately (but non-significantly) increased in PD compared to controls: PD: 190 ± 70 ng/mL Control: 120 ± 30 ng/mL DJ-1 enrichment did not correlate with UPDRS scores (i.e., disease severity) | Luminex IP/Western blot | Saliva | |
| 2a. Kang et al., 2014 (pilot study) [29] | DJ-1 | Moderate correlation between salivary DJ-1 levels and striatal dopaminergic function | Luminex | Saliva |
| 2b. Kang et al., 2014 (large cohort study) [29] | DJ-1 | DJ-1 levels were unaltered in PD patients compared to controls: PD: 4.11 ± 5.88 ng/mL Control: 3.86 ± 5.44 ng/mL DJ-1 enrichment did not correlate with UPDRS III scores (i.e., disease severity) | Luminex | Saliva |
| 3. Stewart et al., 2014 [30] | Total α-Syn | Total α-Syn slightly (but non-significantly) increased in cellular components of saliva in PD patients compared to controls (data extracted from paper graph): PD: 0.42 ± 0.09 pg/μg Control: 0.36 ± 0.03 pg/μg | Luminex | Cellular components of saliva |
| DJ-1 | DJ-1 levels were unaltered in cellular components of saliva in PD patients vs. controls (data extracted from paper graph): PD: 88 ± 8 pg/μg Control: 70 ± 8 pg/μg | Luminex | Cellular components of saliva | |
| 4. Al-Nimer et al., 2014 [31] | Total α-Syn | Total α-Syn significantly reduced in PD compared to controls: PD 65 ± 52.2 pg/mL Control: 314.01 ± 435.9 pg/mL | ELISA | Saliva |
| 5. Masters et al., 2015 [32] | DJ-1 | DJ-1 levels significantly elevated in PD patients compared to controls: PD: 0.84 µg/mL Control: 0.42 µg/mL After normalization for total protein concentration, no alteration of DJ-1 in PD patients compared to controls Normalized DJ-1 levels correlated with UPDRS scores (i.e., disease severity) | Western blot | Saliva |
| 6. Kang et al., 2016 [33] | Total α-Syn | Total α-Syn levels unaltered in PD patients compared to controls: PD: 128.66 ± 98.21 pg/mg Control: 131.31 ± 104.2 pg/mg | Luminex | Saliva |
| Oligomeric α-Syn/ total α-Syn ratio | Oligomeric α-Syn/total α-Syn significantly decreased in early disease state (HY I), but significantly increased in later disease states (HY II to IV) | Western blot after size exclusion chromatography | Saliva | |
| 7. Vivacqua et al., 2016 [34] | Total α-Syn | Total α-Syn significantly reduced in PD patients compared to controls: PD: 5.08 ± 3.01 pg/mL Control: 31.3 ± 22.4 pg/mL | ELISA | Saliva |
| Oligomeric α-Syn | Oligomeric α-Syn significantly increased in PD patients compared to controls: PD: 1.062 ± 0.266 ng/mL Control: 0.498 ± 0.203 ng/mL | ELISA | Saliva | |
| Oligomeric α-Syn/ total α-Syn ratio | Oligomeric α-Syn/total α-Syn ratio significantly increased in PD patients compared to controls: PD: 0.174 ± 0.044 Control: 0.065 ± 0.027 | ELISA | Saliva | |
| 8. Goldman et al., 2018 [35] | Total α-Syn | Total α-Syn moderately (but non-significantly) increased in PD patients compared to controls: PD: 285.42 ± 400.13 pg/mL Control: 165.97 ± 272.3 pg/mL | ELISA | Saliva CSF Plasma |
| 9. Su et al., 2018 [36] | Total α-Syn | Total α-Syn significantly reduced in PD patients compared to controls: PD: 1269.02 ± 16.09 pg/mL Control: 1350.51 ± 25.79 pg/mL | ELISA | Saliva |
| DJ-1 | DJ-1 levels significantly decreased in PD patients compared to controls: PD: 6.07 ± 3.23 ng/mL Control: 8.43 ± 4.33 ng/mL | ELISA | Saliva | |
| 10.a Cao et al., 2019 [37] | Total α-Syn | Total α-Syn in PD patients unaltered compared to controls: PD: 11.93 (6.23~28.11) pg/ng Control: 12.23 (5.47~58.83) pg/ng (mean and interquartile range) | Extracellular Vesicle Enrichment Kit followed by ECL immunoassays | Extracellular vesicles in saliva |
| Oligomeric α-Syn | Oligomeric α-Syn in PD patients significantly increased compared to controls: PD: 7.03 (3.58~12.11) pg/ng Control: 0.92 (0.49~1.61) pg/ng (mean and interquartile range) | Extracellular Vesicle Enrichment Kit followed by ECL immunoassays | Extracellular vesicles in saliva | |
| Oligomeric α-Syn/ total α-Syn ratio | Oligomeric α-Syn/total α-Syn ratio significantly increased in PD patients compared to controls: PD: 0.79 (0.23~1.82) Control: 0.10 (0.04~0.28) (mean and interquartile range) | Extracellular Vesicle Enrichment Kit followed by ECL immunoassays | Extracellular vesicles in saliva | |
| 10b. Cao et al., 2020 [38] | Total α-Syn | Total α-Syn increased in PD patients compared to MSA-P patients: PD: 8.07 ± 4.71 pg/ng MSA-P: 5.44 ± 1.50 pg/ng | Extracellular Vesicle Enrichment Kit followed by ECL immunoassays | Extracellular vesicles in saliva |
| Oligomeric α-Syn | Oligomeric α-Syn unaltered in PD patients compared to MSA-P patients: PD: 8.25 ± 3.98 pg/ng MSA-P: 7.29 ± 4.44 pg/ng | Extracellular Vesicle Enrichment Kit followed by ECL immunoassays | Extracellular vesicles in saliva | |
| 11. Vivacqua et al., 2019 [39] | Total α-Syn | Total α-Syn significantly reduced in PD patients compared to control and to PSP: PD: 7.104 ± 5.122 pg/mL PSP: 29.091 ± 18.677 pg/mL Control: 28.444 ± 25.877 pg/mL | ELISA | Saliva |
| Oligomeric α-Syn | Oligomeric α-Syn significantly increased in PD patients compared to controls: PD: 0.893 ± 1.949 ng/mL Control: 0.217 ± 0.191 ng/mL | ELISA | Saliva | |
| Oligomeric α-Syn/ total α-Syn ratio | Oligomeric α-Syn/total α-Syn ratio significantly increased in PD patients compared to controls: PD: 0.235 ± 0.793 Control: 0.0126 ± 0.0079 | ELISA | Saliva | |
| 12. Shaheen et al., 2020 [40] | Total α-Syn | Total α-Syn levels significantly reduced in PD patients compared to controls: PD: 159.4 ± 61.6 ng/mL Control: 229.9 ± 64 ng/mL | ELISA | Saliva |
| Oligomeric α-Syn | Oligomeric α-Syn levels significantly increased in PD patients compared to controls: PD: 47.8 ± 11.8 ng/mL Control: 39.2 ± 9.2 ng/mL | ELISA | Saliva | |
| Oligomeric α-Syn/ total α-Syn ratio | Oligomeric α-Syn/total α-Syn ratio significantly increased in PD patients compared to controls: PD: 0.35 ± 0.18 Control: 0.19 ± 0.08 | ELISA | Saliva | |
| 13. Chahine et al., 2020 [41] | Total α-Syn | Total α-Syn non-significantly altered in saliva of PD patients compared to controls: PD: 65.6 ± 42.1 pg/mL Early PD: 49.2 ± 25.4 pg/mL Moderate PD: 63.1 ± 30.3 pg/mL Advanced PD: 83.7 ± 57.9 pg/mL Control: 64.4 ± 60.7 pg/mL | ELISA | Blood CSF Saliva |
| 14. Fernández-Espejo et al., 2021 [42] | Total α-Syn | Total α-Syn levels non-significantly decreased in PD patients compared to controls: PD: 361.89 ± 89 pg/mL Control: 372.1 ± 92 pg/mL | ELISA | Serum Saliva human submandibular gland tissue |
| Criteria | 1 [18] | 2 [19] | 3 [20] | 4 [21] | 5 [22] | 6 [23] | 7 [24] | 8 [25] | 9 [26] | 10 [27] | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Representativeness of the sample | * | * | - | - | - | * | - | * | * | - |
| Sample size | - | - | - | - | - | - | - | - | - | - | |
| Non-respondents | - | - | - | - | - | - | - | * | - | - | |
| Ascertainment of the exposure (risk factor) | * | * | * | * | - | - | * | * | * | * | |
| Comparability | Subjects in different outcome (concentration in saliva) groups are comparable (confounding factors controlled) | (*) (-) | (*) (-) | (*) (-) | (-) (-) | (*) (-) | (*) (-) | (*) (-) | (*) (*) | (*) (-) | (-) (-) |
| Outcome | Assessment of the outcome | * | * | * | * | * | * | * | * | * | * |
| Statistical test | * | * | - | * | * | * | * | * | * | * | |
| Total Score | 5 | 5 | 3 | 3 | 3 | 4 | 4 | 7 | 5 | 3 | |
| Quality | fair | fair | poor | poor | poor | fair | fair | good | fair | poor | |
| Risk of Bias | mod | mod | high | high | high | mod | mod | low | mod | high | |
| Criteria | 1 [28] | 2 [29] | 3 [30] | 4 [31] | 5 [32] | 6 [33] | 7 [34] | 8 [35] | 9 [36] | 10 [37,38] | 11 [39] | 12 [40] | 13 [41] | 14 [42] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Representativeness of the sample | * | * | - | * | * | * | * | * | * | * | * | * | * | * |
| Sample size | - | - | - | - | - | - | - | - | - | - | - | - | * | - | |
| Non-respondents | - | - | - | - | - | - | - | - | - | - | - | - | - | - | |
| Ascertainment of the exposure (risk factor) | * | * | - | * | * | * | * | * | * | * | * | * | * | * | |
| Comparability | Subjects in different outcome groups are comparable (confounding factors controlled) | (*) (*) | (*) (-) | (*) (*) | (*) (-) | (*) (-) | (*) (*) | (*) (-) | (*) (*) | (*) (*) | (*) (*) | (*) (-) | (*) (-) | (*) (*) | (*) (*) |
| Outcome | Assessment of the outcome | * | * | - | * | * | * | * | * | * | * | * | * | * | * |
| Statistical test | * | * | * | * | * | * | * | * | * | * | * | * | * | * | |
| Total Score | 6 | 5 | 3 | 5 | 5 | 6 | 5 | 6 | 6 | 6 | 5 | 5 | 7 | 6 | |
| Quality | fair | fair | poor | fair | fair | fair | fair | fair | fair | fair | fair | fair | good | fair | |
| Risk of Bias | mod | mod | high | mod | mod | mod | mod | mod | mod | mod | mod | mod | low | mod | |
| Biomarker | Morbus Alzheimer | Morbus Parkinson |
|---|---|---|
| Aβ42 | elevated | |
| t-tau | unaltered | |
| p-tau | moderately elevated | |
| t-tau/p-tau ratio | moderately elevated | |
| Total α-synuclein | reduced | |
| Oligomeric α-synuclein | elevated | |
| Oligomeric α-Syn/total α-Syn ratio | elevated | |
| DJ-1 | unaltered |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolgin, M.; Zobernig, M.; Dvornyk, V.; Braun, R.J.; Kielbassa, A.M. Systematic Review on Saliva Biomarkers in Patients Diagnosed with Morbus Alzheimer and Morbus Parkinson. Biomedicines 2022, 10, 1702. https://doi.org/10.3390/biomedicines10071702
Wolgin M, Zobernig M, Dvornyk V, Braun RJ, Kielbassa AM. Systematic Review on Saliva Biomarkers in Patients Diagnosed with Morbus Alzheimer and Morbus Parkinson. Biomedicines. 2022; 10(7):1702. https://doi.org/10.3390/biomedicines10071702
Chicago/Turabian StyleWolgin, Michael, Magdalena Zobernig, Valentyn Dvornyk, Ralf J. Braun, and Andrej M. Kielbassa. 2022. "Systematic Review on Saliva Biomarkers in Patients Diagnosed with Morbus Alzheimer and Morbus Parkinson" Biomedicines 10, no. 7: 1702. https://doi.org/10.3390/biomedicines10071702
APA StyleWolgin, M., Zobernig, M., Dvornyk, V., Braun, R. J., & Kielbassa, A. M. (2022). Systematic Review on Saliva Biomarkers in Patients Diagnosed with Morbus Alzheimer and Morbus Parkinson. Biomedicines, 10(7), 1702. https://doi.org/10.3390/biomedicines10071702