
Maternal Body Mass Index Is Associated with Profile Variation in Circulating MicroRNAs at First Trimester of Pregnancy

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Discovery Cohort: Genetics of Glucose Regulation in Gestation and Growth (Gen3G) Cohort
2.2. Anthropometric Measurements in Gen3G
2.3. Replication Cohort: Design, Develop, Discover (3D) Cohort Study
2.4. RNA Extraction
2.5. Library Preparation
2.6. Library Quality Control and Sequencing
2.7. Bioinformatics Analysis
2.8. Statistical Analysis
2.9. Biological Pathway Analysis
3. Results
3.1. Participant’s Characteristics
3.2. Association between miRNA Levels and Maternal BMI at the First Trimester of Pregnancy
3.3. Replication of miRNAs Associated with Maternal BMI at the First Trimester of Pregnancy in the 3D Cohort
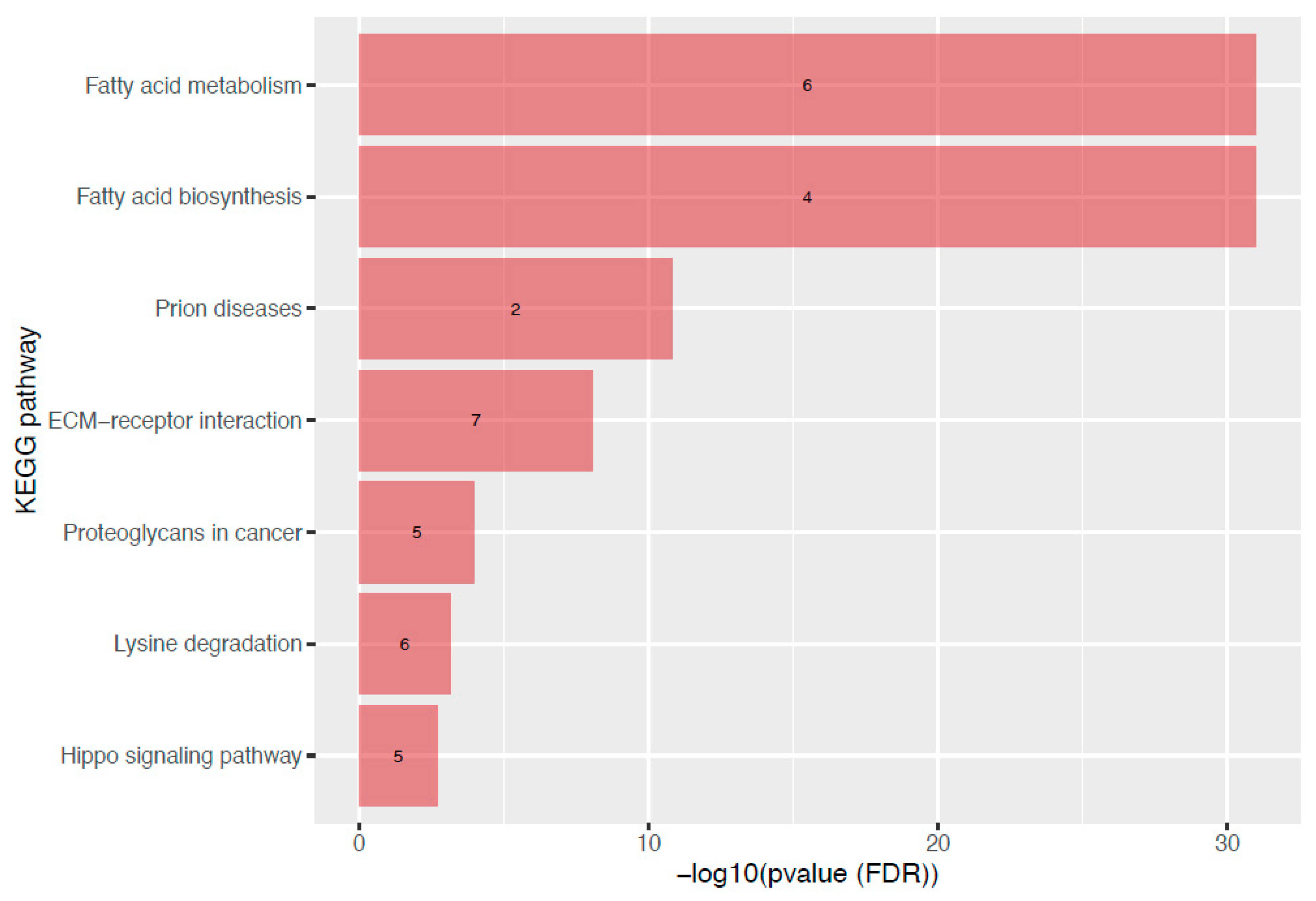
3.4. Metabolic Pathway Analysis of miRNAs Associated with Maternal BMI at the First Trimester of Pregnancy
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caballero, B. The Global Epidemic of Obesity: An Overview. Epidemiol. Rev. 2007, 29, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valsamakis, G.; Kyriazi, E.; Mouslech, Z.; Siristatidis, C.; Mastorakos, G. Effect of Maternal Obesity on Pregnancy Outcomes and Long-Term Metabolic Consequences. Hormones 2015, 14, 345–357.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tauqeer, Z.; Gomez, G.; Stanford, F.C. Obesity in Women: Insights for the Clinician. J. Womens Health 2018, 27, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Shankar, K. Obesity and Pregnancy: Mechanisms of Short Term and Long Term Adverse Consequences for Mother and Child. BMJ Br. Med. J. Online 2017, 356, j1. [Google Scholar] [CrossRef]
- Berger, H.; Melamed, N.; Murray-Davis, B.; Hasan, H.; Mawjee, K.; Barrett, J.; McDonald, S.D.; Geary, M.; Ray, J.G. Prevalence of Pre-Pregnancy Diabetes, Obesity, and Hypertension in Canada. J. Obstet. Gynaecol. Can. 2019, 41, 1579–1588.e2. [Google Scholar] [CrossRef]
- Overweight & Obesity Statistics | NIDDK. Available online: https://www.niddk.nih.gov/health-information/health-statistics/overweight-obesity (accessed on 21 March 2022).
- Catalano, P.M.; McIntyre, H.D.; Cruickshank, J.K.; McCance, D.R.; Dyer, A.R.; Metzger, B.E.; Lowe, L.P.; Trimble, E.R.; Coustan, D.R.; Hadden, D.R.; et al. The Hyperglycemia and Adverse Pregnancy Outcome Study: Associations of GDM and Obesity with Pregnancy Outcomes. Diabetes Care 2012, 35, 780–786. [Google Scholar] [CrossRef] [Green Version]
- Kelly, A.C.; Powell, T.L.; Jansson, T. Placental Function in Maternal Obesity. Clin. Sci. 2020, 134, 961–984. [Google Scholar] [CrossRef] [Green Version]
- Godfrey, K.M.; Reynolds, R.M.; Prescott, S.L.; Nyirenda, M.; Jaddoe, V.W.V.; Eriksson, J.G.; Broekman, B.F.P. Influence of Maternal Obesity on the Long-Term Health of Offspring. Lancet Diabetes Endocrinol. 2017, 5, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Poirier, C.; Desgagné, V.; Guérin, R.; Bouchard, L. MicroRNAs in Pregnancy and Gestational Diabetes Mellitus: Emerging Role in Maternal Metabolic Regulation. Curr. Diab. Rep. 2017, 17, 35. [Google Scholar] [CrossRef]
- Morales-Prieto, D.M.; Ospina-Prieto, S.; Chaiwangyen, W.; Schoenleben, M.; Markert, U.R. Pregnancy-Associated MiRNA-Clusters. J. Reprod. Immunol. 2013, 97, 51–61. [Google Scholar] [CrossRef]
- Légaré, C.; Clément, A.-A.; Desgagné, V.; Thibeault, K.; White, F.; Guay, S.-P.; Arsenault, B.J.; Scott, M.S.; Jacques, P.-É.; Perron, P.; et al. Human Plasma Pregnancy-Associated MiRNAs and Their Temporal Variation within the First Trimester of Pregnancy. Reprod. Biol. Endocrinol. 2022, 20, 14. [Google Scholar] [CrossRef]
- Morales-Prieto, D.M.; Favaro, R.R.; Markert, U.R. Placental MiRNAs in Feto-Maternal Communication Mediated by Extracellular Vesicles. Placenta 2020, 102, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Awamleh, Z.; Gloor, G.B.; Han, V.K.M. Placental MicroRNAs in Pregnancies with Early Onset Intrauterine Growth Restriction and Preeclampsia: Potential Impact on Gene Expression and Pathophysiology. BMC Med. Genom. 2019, 12, 91. [Google Scholar] [CrossRef] [Green Version]
- Hromadnikova, I.; Kotlabova, K.; Ondrackova, M.; Pirkova, P.; Kestlerova, A.; Novotna, V.; Hympanova, L.; Krofta, L. Expression Profile of C19MC MicroRNAs in Placental Tissue in Pregnancy-Related Complications. DNA Cell Biol. 2015, 34, 437–457. [Google Scholar] [CrossRef]
- Hromadnikova, I.; Dvorakova, L.; Kotlabova, K.; Krofta, L. The Prediction of Gestational Hypertension, Preeclampsia and Fetal Growth Restriction via the First Trimester Screening of Plasma Exosomal C19MC MicroRNAs. Int. J. Mol. Sci. 2019, 20, 2972. [Google Scholar] [CrossRef] [PubMed]
- Légaré, C.; Desgagné, V.; Poirier, C.; Thibeault, K.; White, F.; Clément, A.-A.; Scott, M.S.; Jacques, P.-É.; Perron, P.; Guérin, R.; et al. First Trimester Plasma MicroRNAs Levels Predict Matsuda Index-Estimated Insulin Sensitivity between 24th and 29th Week of Pregnancy. BMJ Open Diabetes Res. Care 2022, 10, e002703. [Google Scholar] [CrossRef]
- Jing, J.; Wang, Y.; Quan, Y.; Wang, Z.; Liu, Y.; Ding, Z. Maternal Obesity Alters C19MC MicroRNAs Expression Profile in Fetal Umbilical Cord Blood. Nutr. Metab. 2020, 17, 52. [Google Scholar] [CrossRef] [PubMed]
- Tsamou, M.; Martens, D.S.; Winckelmans, E.; Madhloum, N.; Cox, B.; Gyselaers, W.; Nawrot, T.S.; Vrijens, K. Mother’s Pre-Pregnancy BMI and Placental Candidate MiRNAs: Findings from the ENVIRONAGE Birth Cohort. Sci. Rep. 2017, 7, 5548. [Google Scholar] [CrossRef]
- Enquobahrie, D.A.; Wander, P.L.; Tadesse, M.G.; Qiu, C.; Holzman, C.; Williams, M.A. Maternal Pre-Pregnancy Body Mass Index and Circulating MicroRNAs in Pregnancy. Obes. Res. Clin. Pract. 2017, 11, 464–474. [Google Scholar] [CrossRef]
- Carreras-Badosa, G.; Bonmatí, A.; Ortega, F.-J.; Mercader, J.-M.; Guindo-Martínez, M.; Torrents, D.; Prats-Puig, A.; Martinez-Calcerrada, J.-M.; de Zegher, F.; Ibáñez, L.; et al. Dysregulation of Placental MiRNA in Maternal Obesity Is Associated with Pre- and Postnatal Growth. J. Clin. Endocrinol. Metab. 2017, 102, 2584–2594. [Google Scholar] [CrossRef] [Green Version]
- Guillemette, L.; Allard, C.; Lacroix, M.; Patenaude, J.; Battista, M.-C.; Doyon, M.; Moreau, J.; Ménard, J.; Bouchard, L.; Ardilouze, J.-L.; et al. Genetics of Glucose Regulation in Gestation and Growth (Gen3G): A Prospective Prebirth Cohort of Mother–Child Pairs in Sherbrooke, Canada. BMJ Open 2016, 6, e010031. [Google Scholar] [CrossRef]
- Krukowski, R.A.; West, D.S.; DiCarlo, M.; Shankar, K.; Cleves, M.A.; Saylors, M.E.; Andres, A. Are Early First Trimester Weights Valid Proxies for Preconception Weight? BMC Pregnancy Childbirth 2016, 16, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, W.D.; Shapiro, G.D.; Audibert, F.; Dubois, L.; Pasquier, J.; Julien, P.; Bérard, A.; Muckle, G.; Trasler, J.; Tremblay, R.E.; et al. 3D Cohort Study: The Integrated Research Network in Perinatology of Quebec and Eastern Ontario. Paediatr. Perinat. Epidemiol. 2016, 30, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgos, K.L.; Javaherian, A.; Bomprezzi, R.; Ghaffari, L.; Rhodes, S.; Courtright, A.; Tembe, W.; Kim, S.; Metpally, R.; Van Keuren-Jensen, K. Identification of Extracellular MiRNA in Human Cerebrospinal Fluid by Next-Generation Sequencing. RNA 2013, 19, 712–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rozowsky, J.; Kitchen, R.; Park, J.J.; Galeev, T.R.; Diao, J.; Warrell, J.; Thistlethwaite, W.; Subramanian, S.L.; Milosavljevic, A.; Gerstein, M. ExceRpt: A Comprehensive Analytic Platform for Extracellular RNA Profiling. Cell Syst. 2019, 8, 352–357.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozomara, A.; Griffiths-Jones, S. MiRBase: Annotating High Confidence MicroRNAs Using Deep Sequencing Data. Nucleic Acids Res. 2014, 42, D68–D73. [Google Scholar] [CrossRef] [Green Version]
- Dobin, A.; Davis, C.A.; Schlesinger, F.; Drenkow, J.; Zaleski, C.; Jha, S.; Batut, P.; Chaisson, M.; Gingeras, T.R. STAR: Ultrafast Universal RNA-Seq Aligner. Bioinformatics 2013, 29, 15–21. [Google Scholar] [CrossRef]
- Love, M.I.; Huber, W.; Anders, S. Moderated Estimation of Fold Change and Dispersion for RNA-Seq Data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [Green Version]
- Blighe, K.; Rana, S.; Lewis, M. EnhancedVolcano: Publication-Ready Volcano Plots with Enhanced Colouring and Labeling. Available online: https://github.com/kevinblighe/EnhancedVolcano (accessed on 16 February 2022).
- Vlachos, I.S.; Zagganas, K.; Paraskevopoulou, M.D.; Georgakilas, G.; Karagkouni, D.; Vergoulis, T.; Dalamagas, T.; Hatzigeorgiou, A.G. DIANA-MiRPath v3.0: Deciphering MicroRNA Function with Experimental Support. Nucleic Acids Res. 2015, 43, W460–W466. [Google Scholar] [CrossRef]
- Luo, S.-S.; Ishibashi, O.; Ishikawa, G.; Ishikawa, T.; Katayama, A.; Mishima, T.; Takizawa, T.; Shigihara, T.; Goto, T.; Izumi, A.; et al. Human Villous Trophoblasts Express and Secrete Placenta-Specific MicroRNAs into Maternal Circulation via Exosomes. Biol. Reprod. 2009, 81, 717–729. [Google Scholar] [CrossRef] [Green Version]
- Légaré, C.; Desgagné, V.; Thibeault, K.; White, F.; Clément, A.-A.; Poirier, C.; Luo, Z.-C.; Scott, M.; Jacques, P.-É.; Perron, P.; et al. First Trimester Plasma MicroRNA Levels Predict Risk of Developing Gestational Diabetes Mellitus. Front. Endocrinol. 2022, 13. [Google Scholar]
- Liu, L.; Zhang, J.; Liu, Y. MicroRNA-1323 Serves as a Biomarker in Gestational Diabetes Mellitus and Aggravates High Glucose-Induced Inhibition of Trophoblast Cell Viability by Suppressing TP53INP1. Exp. Ther. Med. 2021, 21, 230. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.-Y.; Xiao, Y.-P.; Ren, C.-L.; Guo, Y.-W.; Qu, D.-H.; Zhang, J.-H.; Zhu, Y.-J. Up-Regulation of MiR-517-5p Inhibits ERK/MMP-2 Pathway: Potential Role in Preeclampsia. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 6599–6608. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Lei, Y.; Luo, S.; Huang, Z.; Chen, C.; Wang, K.; Yang, P.; Huang, X. MicroRNA Expression Profile and Identification of Novel MicroRNA Biomarkers for Metabolic Syndrome. Bioengineered 2021, 12, 3864–3872. [Google Scholar] [CrossRef] [PubMed]
- Klop, B.; Elte, J.W.F.; Castro Cabezas, M. Dyslipidemia in Obesity: Mechanisms and Potential Targets. Nutrients 2013, 5, 1218–1240. [Google Scholar] [CrossRef] [Green Version]
- Herrera, E. Lipid Metabolism in Pregnancy and Its Consequences in the Fetus and Newborn. Endocrine 2002, 19, 43–55. [Google Scholar] [CrossRef]
- Tam, S.; de Borja, R.; Tsao, M.-S.; McPherson, J.D. Robust Global MicroRNA Expression Profiling Using Next-Generation Sequencing Technologies. Lab. Investig. J. Tech. Methods Pathol. 2014, 94, 350–358. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Characteristics | Gen3G Cohort | 3D Cohort | Comparison between Cohorts (p-Value) * | ||
|---|---|---|---|---|---|
| Mean ± SD | Range | Mean ± SD | Range | ||
| BMI (kg/m2) | 25.95 ± 5.98 | 16.10–54.10 | 25.39 ± 5.91 | 16.80–48.50 | 0.22 |
| Age (years) | 28.48 ± 4.26 | 18–47 | 30.60 ± 3.90 | 20–42 | <0.001 |
| Gestational age (weeks) | 9.63 ± 2.26 | 4.09–16.30 | 11.89 ± 1.52 | 7.71–16.43 | <0.001 |
| Parity(% nulliparous) | 0.69 ± 0.91 (53.56) | 0–6 | 0.47 ± 0.66 (60.99) | 0–3 | 0.01 |
| miRNA | DESeq2 Normalized Read Count (Mean ± SD) | Fold Change * | Unadjusted p-Value | FDR-Adjusted q-Value |
|---|---|---|---|---|
| hsa-miR-1323 a | 146.39 ± 230.60 | 0.957 | 2.79 × 10−10 | 9.60 × 10−8 |
| hsa-miR-516b-5p a | 101.50 ± 150.35 | 0.958 | 1.79 × 10−10 | 9.60 × 10−8 |
| hsa-miR-371a-5p b | 11.02 ± 17.09 | 0.941 | 2.13 × 10−10 | 9.60 × 10−8 |
| hsa-miR-525-5p a | 9.07 ± 15.31 | 0.952 | 1.63 × 10−9 | 4.21 × 10−7 |
| hsa-miR-516a-5p a | 31.25 ± 53.81 | 0.959 | 4.55 × 10−9 | 7.83 × 10−7 |
| hsa-miR-524-5p a | 8.64 ± 14.48 | 0.952 | 3.90 × 10−9 | 7.83 × 10−7 |
| hsa-miR-518e-5p a | 43.96 ± 62.52 | 0.962 | 8.92 × 10−9 | 1.22 × 10−6 |
| hsa-miR-520a-3p a | 86.75 ± 132.37 | 0.960 | 9.41 × 10−9 | 1.22 × 10−6 |
| hsa-miR-518e-3p a | 7.99 ± 14.22 | 0.956 | 2.02 × 10−8 | 2.09 × 10−6 |
| hsa-miR-520d-5p a | 5.92 ± 10.35 | 0.955 | 1.98 × 10−8 | 2.09 × 10−6 |
| Gen3G | 3D | ||||||
|---|---|---|---|---|---|---|---|
| miRNA | DESeq2 Normalized Read Count (Mean ± SD) | Fold Change * | Unadjusted p-Value | FDR-Adjusted q-Value | DESeq2 Normalized Read Count (Mean ± SD) | Fold Change * | Unadjusted p-Value |
| hsa-miR-1323 a | 146.39 ± 230.60 | 0.957 | 2.79 × 10−10 | 9.60 × 10−8 | 676.45 ± 581.88 | 0.966 | 2.56 × 10−5 |
| hsa-miR-516b-5p a | 101.50 ± 150.35 | 0.958 | 1.79 × 10−10 | 9.60 × 10−8 | 327.56 ± 247.26 | 0.966 | 2.92 × 10−5 |
| hsa-miR-525-5p a | 9.07 ± 15.31 | 0.952 | 1.63 × 10−9 | 4.21 × 10−7 | 79.89 ± 71.16 | 0.982 | 0.04471 |
| hsa-miR-516a-5p a | 31.25 ± 53.81 | 0.959 | 4.55 × 10−9 | 7.83 × 10−7 | 150.92 ± 135.76 | 0.974 | 0.00141 |
| hsa-miR-518e-5p a | 43.96 ± 62.52 | 0.962 | 8.92 × 10−9 | 1.22 × 10−6 | 99.07 ± 88.52 | 0.981 | 0.02118 |
| hsa-miR-520a-3p a | 86.75 ± 132.37 | 0.960 | 9.41 × 10−9 | 1.22 × 10−6 | 220.91 ± 243.90 | 0.982 | 0.04009 |
| hsa-miR-518e-3p a | 7.99 ± 14.22 | 0.956 | 2.02 × 10−8 | 2.09 × 10−6 | 29.60 ± 25.75 | 0.971 | 0.00189 |
| hsa-miR-512-3p a | 287.04 ± 575.48 | 0.963 | 3.63 × 10−8 | 3.41 × 10−6 | 771.74 ± 982.11 | 0.982 | 0.02747 |
| hsa-miR-1283 a | 57.10 ± 87.82 | 0.962 | 4.17 × 10−8 | 3.59 × 10−6 | 203.52 ± 173.84 | 0.977 | 0.00635 |
| hsa-miR-517a-3p a | 20.19 ± 37.78 | 0.960 | 5.17 × 10−8 | 4.11 × 10−6 | 76.56 ± 73.88 | 0.980 | 0.01599 |
| hsa-miR-526b-5p a | 17.12 ± 25.90 | 0.962 | 2.19 × 10−7 | 1.62 × 10−5 | 39.62 ± 34.83 | 0.977 | 0.01056 |
| hsa-miR-517-5p a | 16.90 ± 29.75 | 0.962 | 9.56 × 10−7 | 6.17 × 10−5 | 70.67 ± 67.45 | 0.981 | 0.02191 |
| hsa-miR-519c-3p a | 11.08 ± 20.08 | 0.965 | 5.11 × 10−6 | 0.00026 | 36.44 ± 32.83 | 0.966 | 0.00034 |
| hsa-miR-519d-5p a | 6.12 ± 9.51 | 0.961 | 1.53 × 10−5 | 0.00063 | 10.75 ± 11.77 | 0.969 | 0.01205 |
| hsa-miR-515-5p a | 10.50 ± 19.12 | 0.967 | 1.50 × 10−5 | 0.00063 | 26.70 ± 26.08 | 0.968 | 0.00076 |
| hsa-miR-27b-3p | 29,699.76 ± 20,347.78 | 1.008 | 4.98 × 10−5 | 0.00172 | 55,214.27 ± 41,098.16 | 1.011 | 0.00110 |
| hsa-miR-885-5p | 13.50 ± 17.92 | 1.036 | 4.98 × 10−5 | 0.00172 | 40.63 ± 78.98 | 1.034 | 0.00588 |
| hsa-miR-520a-5p a | 3.06 ± 5.66 | 0.963 | 0.00032 | 0.00830 | 27.63 ± 27.09 | 0.965 | 0.00136 |
| hsa-miR-375 | 1938.28 ± 3939.32 | 0.975 | 0.00040 | 0.00986 | 2900.08 ± 2878.58 | 0.982 | 0.03889 |
| hsa-miR-520d-3p a | 9.80 ± 15.84 | 0.972 | 0.00091 | 0.01877 | 10.77 ± 13.37 | 0.966 | 0.00638 |
| hsa-miR-592 | 1.64 ± 3.00 | 1.042 | 0.00162 | 0.03103 | 2.43 ± 4.89 | 1.058 | 0.00400 |
| hsa-miR-21-5p | 85,256.17 ± 61,108.55 | 1.005 | 0.00224 | 0.03811 | 82,095.57 ± 63,195.51 | 1.008 | 0.02738 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thibeault, K.; Légaré, C.; Desgagné, V.; White, F.; Clément, A.-A.; Scott, M.S.; Jacques, P.-É.; Guérin, R.; Perron, P.; Hivert, M.-F.; et al. Maternal Body Mass Index Is Associated with Profile Variation in Circulating MicroRNAs at First Trimester of Pregnancy. Biomedicines 2022, 10, 1726. https://doi.org/10.3390/biomedicines10071726
Thibeault K, Légaré C, Desgagné V, White F, Clément A-A, Scott MS, Jacques P-É, Guérin R, Perron P, Hivert M-F, et al. Maternal Body Mass Index Is Associated with Profile Variation in Circulating MicroRNAs at First Trimester of Pregnancy. Biomedicines. 2022; 10(7):1726. https://doi.org/10.3390/biomedicines10071726
Chicago/Turabian StyleThibeault, Kathrine, Cécilia Légaré, Véronique Desgagné, Frédérique White, Andrée-Anne Clément, Michelle S. Scott, Pierre-Étienne Jacques, Renée Guérin, Patrice Perron, Marie-France Hivert, and et al. 2022. "Maternal Body Mass Index Is Associated with Profile Variation in Circulating MicroRNAs at First Trimester of Pregnancy" Biomedicines 10, no. 7: 1726. https://doi.org/10.3390/biomedicines10071726