
The Behavior of Muscle Oxygen Saturation, Oxy and Deoxy Hemoglobin during a Fatigue Test in Fibromyalgia

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Instruments
2.3.1. NIRS Sensor
2.3.2. Sociodemographic Data and Physical Activity Level
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Núñez-Fuentes, D.; Obrero-Gaitán, E.; Zagalaz-Anula, N.; Ibáñez-Vera, A.J.; Achalandabaso-Ochoa, A.; López-Ruiz, M.D.C.; Rodríguez-Almagro, D.; Lomas-Vega, R. Alteration of Postural Balance in Patients with Fibromyalgia Syndrome-A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 127. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, K.E.; Park, D.J.; Kim, S.H.; Nah, S.S.; Lee, J.H.; Kim, S.K.; Lee, Y.A.; Hong, S.J.; Kim, H.S.; et al. Determinants of quality of life in patients with fibromyalgia: A structural equation modeling approach. PLoS ONE 2017, 12, e0171186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Walitt, B.; Perrot, S.; Rasker, J.J.; Häuser, W. Fibromyalgia diagnosis and biased assessment: Sex, prevalence and bias. PLoS ONE 2018, 13, e0203755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bachasson, D.; Guinot, M.; Wuyam, B.; Favre-Juvin, A.; Millet, G.Y.; Levy, P.; Verges, S. Neuromuscular fatigue and exercise capacity in fibromyalgia syndrome. Arthritis Care Res. 2013, 65, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Villafaina, S.; Collado-Mateo, D.; Fuentes-García, J.P.; Cano-Plasencia, R.; Gusi, N. Impact of fibromyalgia on alpha-2 EEG power spectrum in the resting condition: A descriptive correlational study. BioMed Res. Int. 2019, 2019, 7851047. [Google Scholar] [CrossRef] [Green Version]
- Leon-Llamas, J.L.; Villafaina, S.; Murillo-Garcia, A.; Gusi, N. Impact of Fibromyalgia in the Hippocampal Subfields Volumes of Women—An MRI Study. Int. J. Environ. Res. Public Health 2021, 18, 1549. [Google Scholar] [CrossRef]
- Jacomini, L.C.L.; Silva, N.A.D. Dysautonomia: An emerging concept in fibromyalgia syndrome. Rev. Bras. De Reumatol. 2007, 47, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Raj, S.R.; Brouillard, D.; Simpson, C.S.; Hopman, W.M.; Abdollah, H. Dysautonomia among patients with fibromyalgia: A noninvasive assessment. J. Rheumatol. 2000, 27, 2660–2665. [Google Scholar]
- Solano, C.; Martinez, A.; Becerril, L.; Vargas, A.; Figueroa, J.; Navarro, C.; Ramos-Remus, C.; Martinez-Lavin, M. Autonomic dysfunction in fibromyalgia assessed by the Composite Autonomic Symptoms Scale (COMPASS). JCR J. Clin. Rheumatol. 2009, 15, 172–176. [Google Scholar] [CrossRef]
- Ulas, U.H.; Unlu, E.; Hamamcioglu, K.; Odabasi, Z.; Cakci, A.; Vural, O. Dysautonomia in fibromyalgia syndrome: Sympathetic skin responses and RR interval analysis. Rheumatol. Int. 2006, 26, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lavin, M. Fibromyalgia as a sympathetically maintained pain syndrome. Curr. Pain Headache Rep. 2004, 8, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Furlan, R.; Colombo, S.; Perego, F.; Atzeni, F.; Diana, A.; Barbic, F.; Porta, A.; Pace, F.; Malliani, A.; Sarzi-Puttini, P. Abnormalities of cardiovascular neural control and reduced orthostatic tolerance in patients with primary fibromyalgia. J. Rheumatol. 2005, 32, 1787–1793. [Google Scholar] [PubMed]
- Montoro, C.I.; Duschek, S.; Schuepbach, D.; Gandarillas, M.A.; Reyes Del Paso, G.A. Cerebral blood flow variability in fibromyalgia syndrome: Relationships with emotional, clinical and functional variables. PLoS ONE 2018, 13, e0204267. [Google Scholar] [CrossRef] [Green Version]
- Duschek, S.; Mannhart, T.; Winkelmann, A.; Merzoug, K.; Werner, N.S.; Schuepbach, D.; Montoya, P. Cerebral blood flow dynamics during pain processing in patients with fibromyalgia syndrome. Psychosom. Med. 2012, 74, 802–809. [Google Scholar] [CrossRef]
- Cook, D.B.; Stegner, A.J.; Nagelkirk, P.R.; Meyer, J.D.; Togo, F.; Natelson, B.H. Responses to exercise differ for chronic fatigue syndrome patients with fibromyalgia. Med. Sci. Sport. Exerc. 2012, 44, 1186–1193. [Google Scholar] [CrossRef] [Green Version]
- Shang, Y.; Gurley, K.; Symons, B.; Long, D.; Srikuea, R.; Crofford, L.J.; Peterson, C.A.; Yu, G. Noninvasive optical characterization of muscle blood flow, oxygenation, and metabolism in women with fibromyalgia. Arthritis Res. Ther. 2012, 14, R236. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Hauser, W.; Fluss, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Busch, A.J.; Webber, S.C.; Brachaniec, M.; Bidonde, J.; Bello-Haas, V.D.; Danyliw, A.D.; Overend, T.J.; Richards, R.S.; Sawant, A.; Schachter, C.L. Exercise therapy for fibromyalgia. Curr. Pain Headache Rep. 2011, 15, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Overend, T.J.; Kim, S.Y.; Góes, S.M.; Boden, C.; Foulds, H.J.A. Aerobic exercise training for adults with fibromyalgia. Cochrane Database Syst. Rev. 2017, 2017, CD012700. [Google Scholar] [CrossRef]
- Júnior, J.C.A.; de Almeida Silva, H.J.; da Silva, J.F.C.; da Silva Cruz, R.; de Almeida Lins, C.A.; de Souza, M.C. Zumba dancing can improve the pain and functional capacity in women with fibromyalgia. J. Bodyw. Mov. Ther. 2018, 22, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Gavi, M.B.R.O.; Vassalo, D.V.; Amaral, F.T.; Macedo, D.C.F.; Gava, P.L.; Dantas, E.M.; Valim, V. Strengthening exercises improve symptoms and quality of life but do not change autonomic modulation in fibromyalgia: A randomized clinical trial. PLoS ONE 2014, 9, e90767. [Google Scholar] [CrossRef] [PubMed]
- Collado-Mateo, D.; Dominguez-Muñoz, F.J.; Adsuar, J.C.; Merellano-Navarro, E.; Gusi, N. Exergames for women with fibromyalgia: A randomised controlled trial to evaluate the effects on mobility skills, balance and fear of falling. PeerJ 2017, 5, e3211. [Google Scholar] [CrossRef]
- Villafaina, S.; Collado-Mateo, D.; Fuentes, J.P.; Rohlfs-Domínguez, P.; Gusi, N. Effects of exergames on brain dynamics in women with fibromyalgia: A Randomized controlled trial. J. Clin. Med. 2019, 8, 1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijs, J.; Roussel, N.; Van Oosterwijck, J.; De Kooning, M.; Ickmans, K.; Struyf, F.; Meeus, M.; Lundberg, M. Fear of movement and avoidance behaviour toward physical activity in chronic-fatigue syndrome and fibromyalgia: State of the art and implications for clinical practice. Clin. Rheumatol. 2013, 32, 1121–1129. [Google Scholar] [CrossRef]
- Lorente, G.D.; Stefani, L.F.B.D.; Martins, M.R.I. Kinesiophobia, adherence to treatment, pain and quality of life in fibromyalgia syndrome patients. Rev. Dor 2014, 15, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Gerdle, B.; Ghafouri, B.; Lund, E.; Bengtsson, A.; Lundberg, P.; Ettinger-Veenstra, H.V.; Leinhard, O.D.; Forsgren, M.F. Evidence of Mitochondrial Dysfunction in Fibromyalgia: Deviating Muscle Energy Metabolism Detected Using Microdialysis and Magnetic Resonance. J. Clin. Med. 2020, 9, 3527. [Google Scholar] [CrossRef]
- Freeman, J.V.; Dewey, F.E.; Hadley, D.M.; Myers, J.; Froelicher, V.F. Autonomic nervous system interaction with the cardiovascular system during exercise. Prog. Cardiovasc. Dis. 2006, 48, 342–362. [Google Scholar] [CrossRef]
- Schamne, J.C.; Ressetti, J.C.; Lima-Silva, A.E.; Okuno, N.M. Impaired Cardiac Autonomic Control in Women with Fibromyalgia is Independent of Their Physical Fitness. J. Clin. Rheumatol. Pract. Rep. Rheum. Musculoskelet. Dis. 2021, 27, S278–S283. [Google Scholar] [CrossRef]
- Kingsley, J.D.; Panton, L.B.; McMillan, V.; Figueroa, A. Cardiovascular autonomic modulation after acute resistance exercise in women with fibromyalgia. Arch. Phys. Med. Rehabil. 2009, 90, 1628–1634. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Tomas-Carus, P.; Ortega-Alonso, A.; Pietilainen, K.H.; Santos, V.; Goncalves, H.; Ramos, J.; Raimundo, A. A randomized controlled trial on the effects of combined aerobic-resistance exercise on muscle strength and fatigue, glycemic control and health-related quality of life of type 2 diabetes patients. J. Sport. Med. Phys. Fit. 2016, 56, 572–578. [Google Scholar]
- Clemente-Suárez, V.; Parraca, J.; Silva, V.; Batalha, N.; Costa, A.; Tomas-Carus, P. Differences in Peripheral Vascular Response of a Fibromyalgia Patient in a Physical Fatigue Situation; A Case Control Report; Universidade de Évora: Évora, Portugal, 2021. [Google Scholar]
- Crum, E.M.; O’connor, W.J.; Van Loo, L.; Valckx, M.; Stannard, S.R. Validity and reliability of the Moxy oxygen monitor during incremental cycling exercise. Eur. J. Sport Sci. 2017, 17, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E. SF-36 Health Survey: Manual and Interpretation Guide; Quality Metric Inc.: Johnston, RI, USA, 1993. [Google Scholar]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. Bmj 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 2050312116671725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Kaleth, A.S.; Ang, D.C.; Chakr, R.; Tong, Y. Validity and reliability of community health activities model program for seniors and short-form international physical activity questionnaire as physical activity assessment tools in patients with fibromyalgia. Disabil. Rehabil. 2010, 32, 353–359. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Coolican, H. Research Methods and Statistics in Psychology; Psychology Press: London, UK, 2017. [Google Scholar]
- Cordero, M.D.; De Miguel, M.; Moreno Fernández, A.M.; Carmona López, I.M.; Garrido Maraver, J.; Cotán, D.; Gómez Izquierdo, L.; Bonal, P.; Campa, F.; Bullon, P. Mitochondrial dysfunction and mitophagy activation in blood mononuclear cells of fibromyalgia patients: Implications in the pathogenesis of the disease. Arthritis Res. Ther. 2010, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, Ş.; Kiralp, M.Z.; Akin, A.; Keskin, I.; Ay, H.; Dursun, H.; Cimsit, M. A new treatment modality for fibromyalgia syndrome: Hyperbaric oxygen therapy. J. Int. Med. Res. 2004, 32, 263–267. [Google Scholar] [CrossRef] [Green Version]
- McIver, K.L.; Evans, C.; Kraus, R.M.; Ispas, L.; Sciotti, V.M.; Hickner, R.C. NO-mediated alterations in skeletal muscle nutritive blood flow and lactate metabolism in fibromyalgia. Pain 2006, 120, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Valkeinen, H.; Häkkinen, A.; Hannonen, P.; Häkkinen, K.; Alén, M. Acute heavy-resistance exercise-induced pain and neuromuscular fatigue in elderly women with fibromyalgia and in healthy controls: Effects of strength training. Arthritis Rheum. 2006, 54, 1334–1339. [Google Scholar] [CrossRef] [PubMed]
- Valkeinen, H.; Alén, M.; Häkkinen, A.; Hannonen, P.; Kukkonen-Harjula, K.; Häkkinen, K. Effects of concurrent strength and endurance training on physical fitness and symptoms in postmenopausal women with fibromyalgia: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2008, 89, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Greene, L.; Ali, A.; Faridi, Z. The pain of fibromyalgia syndrome is due to muscle hypoperfusion induced by regional vasomotor dysregulation. Med. Hypotheses 2007, 69, 517–525. [Google Scholar] [CrossRef]
- Maquet, D.; Croisier, J.-L.; Renard, C.; Crielaard, J.-M. Muscle performance in patients with fibromyalgia. Jt. Bone Spine 2002, 69, 293–299. [Google Scholar] [CrossRef]
- Okumus, M.; Gokoglu, F.; Kocaoglu, S.; Ceceli, E.; Yorgancioglu, Z.R. Muscle performance in patients with fibromyalgia. Singap. Med. J. 2006, 47, 752. [Google Scholar]
- Park, J.H.; Phothimat, P.; Oates, C.T.; Hernanz-Schulman, M.; Olsen, N.J. Use of P-31 magnetic resonance spectroscopy to detect metabolic abnormalities in muscles of patients with fibromyalgia. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1998, 41, 406–413. [Google Scholar] [CrossRef]
- Lund, E.; Kendall, S.A.; Janerot-Sjöberg, B.; Bengtsson, A. Muscle metabolism in fibromyalgia studied by P-31 magnetic resonance spectroscopy during aerobic and anaerobic exercise. Scand. J. Rheumatol. 2003, 32, 138–145. [Google Scholar] [CrossRef]
- Morf, S.; Amann-Vesti, B.; Forster, A.; Franzeck, U.K.; Koppensteiner, R.; Uebelhart, D.; Sprott, H. Microcirculation abnormalities in patients with fibromyalgia–measured by capillary microscopy and laser fluxmetry. Arthritis Res. Ther. 2004, 7, 1–8. [Google Scholar]
- Costa, A.R.; Freire, A.; Parraca, J.A.; Silva, V.; Tomas-Carus, P.; Villafaina, S. Heart Rate Variability and Salivary Biomarkers Differences between Fibromyalgia and Healthy Participants after an Exercise Fatigue Protocol: An Experimental Study. Diagnostics 2022, 12, 2220. [Google Scholar] [CrossRef]
- Adler, G.K.; Geenen, R. Hypothalamic–pituitary–adrenal and autonomic nervous system functioning in fibromyalgia. Rheum. Dis. Clin. 2005, 31, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Staud, R. Heart rate variability as a biomarker of fibromyalgia syndrome. Future Rheumatol. 2008, 3, 475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Lavín, M.; Hermosillo, A.G. Autonomic nervous system dysfunction may explain the multisystem features of fibromyalgia. Semin. Arthritis Rheum. 2000, 29, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Bote, M.E.; Garcia, J.J.; Hinchado, M.D.; Ortega, E. Fibromyalgia: Anti-inflammatory and stress responses after acute moderate exercise. PLoS ONE 2013, 8, e74524. [Google Scholar] [CrossRef]
- Lange, E.; Mannerkorpi, K.; Cider, A.; Archer, T.; Wentz, K. Physiological adaptation in women presenting fibromyalgia: Comparison with healthy controls. Clin. Exp. Psychol. 2017, 3, 1–8. [Google Scholar] [CrossRef]
- Fernandez-Feijoo, F.; Samartin-Veiga, N.; Carrillo-de-la-Peña, M.T. Quality of life in patients with fibromyalgia: Contributions of disease symptoms, lifestyle and multi-medication. Front. Psychol. 2022, 13, 924405. [Google Scholar] [CrossRef]
- Ursini, F.; Naty, S.; Grembiale, R.D. Fibromyalgia and obesity: The hidden link. Rheumatol. Int. 2011, 31, 1403–1408. [Google Scholar] [CrossRef]
- Menazza, S.; Murphy, E. The expanding complexity of estrogen receptor signaling in the cardiovascular system. Circ. Res. 2016, 118, 994–1007. [Google Scholar] [CrossRef]
- Enns, D.L.; Tiidus, P.M. The influence of estrogen on skeletal muscle. Sport. Med. 2010, 40, 41–58. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Fibromyalgia Mean (SD) | Healthy Controls Mean (SD) | p-Value |
|---|---|---|---|
| Age (years) | 51.3 (10.4) | 40.3 (1.8) | 0.014 |
| BMI (kg/m2) | 31.5 (7.9) | 22.6 (3.7) | 0.001 |
| Duration of fibromyalgia symptoms (years) | 12.5 (9) | - | - |
| Years since diagnosis (years) | 7.7 (6.4) | - | - |
| Work | 0.025 | ||
| With physical load | 10 (55.6) | 3 (21.4) | |
| Without physical load | 2 (11.1) | 11 (78.6) | |
| Without work | 6 (33.3) | 0 | |
| Education level, N (%) | 0.009 | ||
| Primary school | 9 (50%) | 0 (0%) | |
| Secondary school | 7 (38.9%) | 3 (21.4%) | |
| University | 2 (11.1%) | 11 (78.6%) | |
| Physical activity level | |||
| Vigorous intensity (min) | 43.3 (145.2) | 158.5 (163.5) | 0.003 |
| Moderate intensity (min) | 1443.8 (1054.7) | 764.2 (1566) | 0.007 |
| Walking (min) | 228.7 (268.1) | 388.4 (627.6) | 0.761 |
| Sitting time (min) | 152.1 (199.2) | 293.1 (186.4) | 0.573 |
| HRQoL | 0.58 (0.11) | 0.82 (0.12) | 0.001 |
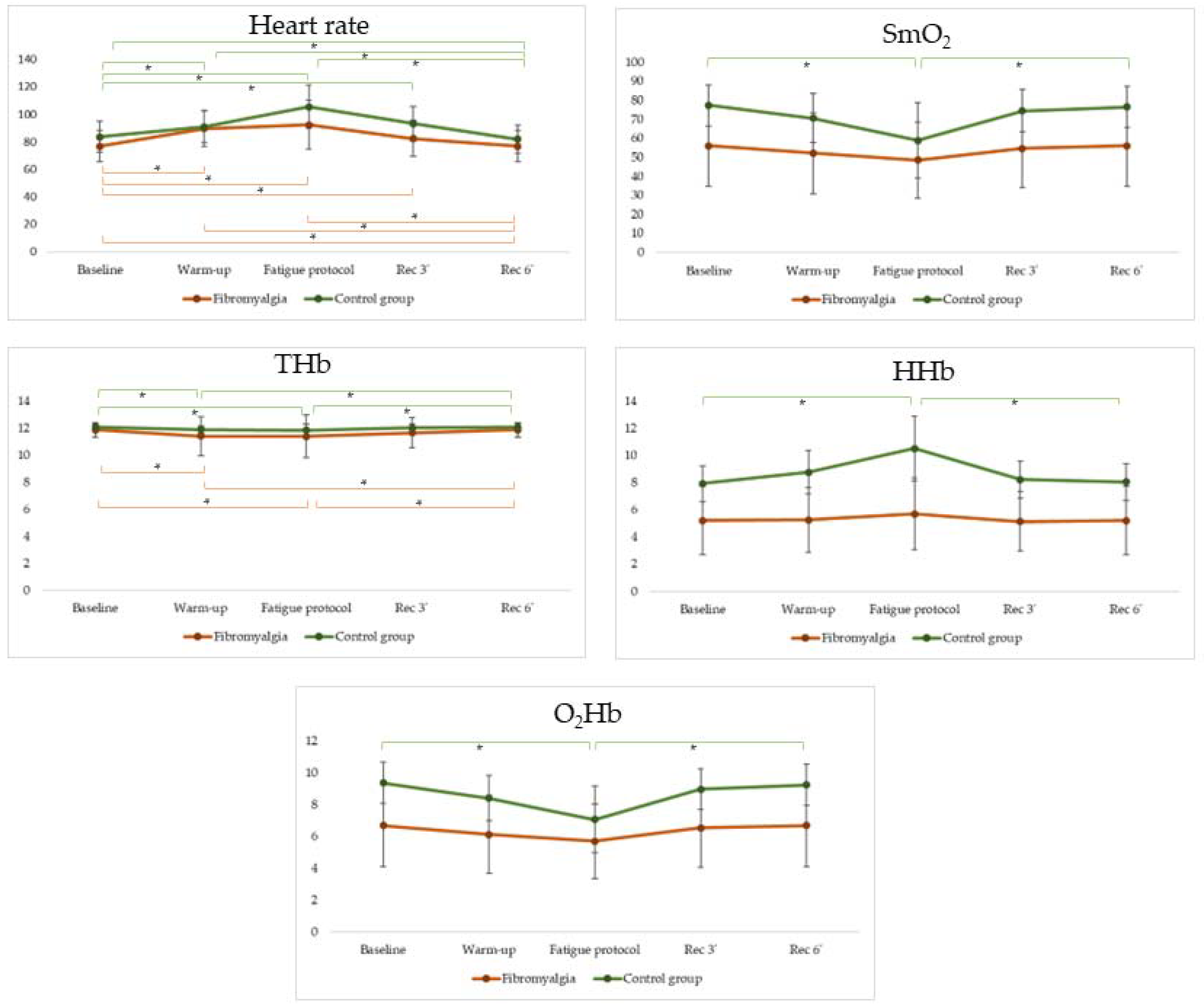
| Variable | Fibromyalgia Mean (SD) | Healthy Controls Mean (SD) | p-Value | F | Effect Size |
|---|---|---|---|---|---|
| Baseline | |||||
| HR (bpm) | 76.79 (11.45) | 83.58 (11.48) | 0.354 | 0.890 | 0.131 |
| SmO2 (%) | 56.03 (21.36) | 77.41 (10.82) | 0.036 | 4.879 | 0.153 |
| THb (g/dL) | 11.89 (0.54) | 12.10 (0.26) | 0.387 | 0.772 | 0.029 |
| O2Hb (g/dL) | 6.69 (2.59) | 9.37 (1.31) | 0.030 | 5.274 | 0.163 |
| HHb (g/dL) | 5.20 (2.51) | 2.73 (1.32) | 0.039 | 4.705 | 0.148 |
| Warm-up | |||||
| HR (bpm) | 89.68 (13.13) | 90.96 (11.59) | 0.739 | 0.423 | 0.045 |
| SmO2 (%) | 52.31 (21.31) | 70.65 (13.02) | 0.079 | 3.325 | 0.110 |
| THb (g/dL) | 11.41 (1.43) | 11.91 (0.27) | 0.677 | 0.178 | 0.007 |
| O2Hb (g/dL) | 6.13 (2.46) | 8.40 (1.43) | 0.062 | 3.804 | 0.123 |
| HHb (g/dL) | 5.25 (2.37) | 3.51 (1.59) | 0.093 | 3.042 | 0.101 |
| Fatigue protocol | |||||
| HR (bpm) | 92.46 (17.91) | 105.49 (15.69) | 0.499 | 0.471 | 0.018 |
| SmO2 (%) | 48.54 (19.96) | 58.87 (19.72) | 0.038 | 4.753 | 0.155 |
| THb (g/dL) | 11.40 (1.60) | 11.86 (0.44) | 0.901 | 0.016 | 0.001 |
| O2Hb (g/dL) | 5.70 (2.34) | 7.06 (2.09) | 0.027 | 5.517 | 0.175 |
| HHb (g/dL) | 5.69 (2.65) | 4.81 (2.39) | 0.048 | 4.287 | 0.142 |
| Recovery—three min | |||||
| HR (bpm) | 82.35 (13.15) | 93.34 (12.61) | 0.231 | 1.504 | 0.055 |
| SmO2 (%) | 54.65 (20.52) | 74.47 (11.17) | 0.049 | 4.281 | 0.141 |
| THb (g/dL) | 11.67 (1.11) | 12.04 (0.25) | 0.659 | 0.200 | 0.008 |
| O2Hb (g/dL) | 6.53 (2.46) | 8.97 (1.28) | 0.041 | 4.623 | 0.151 |
| HHb (g/dL) | 5.14 (2.19) | 3.08 (1.36) | 0.041 | 4.614 | 0.151 |
| Recovery—six min | |||||
| HR (bpm) | 76.79 (11.45) | 81.92 (10.23) | 0.436 | 0.627 | 0.024 |
| SmO2 (%) | 56.03 (21.36) | 76.54 (10.82) | 0.044 | 4.472 | 0.147 |
| THb (g/dL) | 11.89 (0.54) | 12.08 (0.26) | 0.425 | 0.656 | 0.025 |
| O2Hb (g/dL) | 6.69 (2.59) | 9.25 (1.29) | 0.037 | 4.818 | 0.156 |
| HHb (g/dL) | 5.20 (2.51) | 2.84 (1.32) | 0.048 | 4.307 | 0.142 |
| Variable | Fibromyalgia Mean (SD) | Healthy Controls Mean (SD) | p-Value | F | Effect Size |
|---|---|---|---|---|---|
| Peak torque at extension (N∙m) | 62.48 (24.45) | 88.31 (23.51) | 0.033 | 5.086 | 0.929 |
| Peak torque at flexion (N∙m) | 24.16 (11.58) | 42.05 (9.85) | 0.010 | 7.733 | 1.412 |
| Total work at extension (J) | 1039.78 (434.51) | 1535.61 (474.22) | 0.007 | 8.564 | 1.564 |
| Total work at flexion (J) | 423.79 (239.89) | 797.16 (194.37) | 0.005 | 9.574 | 1.748 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villafaina, S.; Tomas-Carus, P.; Silva, V.; Costa, A.R.; Fernandes, O.; Parraca, J.A. The Behavior of Muscle Oxygen Saturation, Oxy and Deoxy Hemoglobin during a Fatigue Test in Fibromyalgia. Biomedicines 2023, 11, 132. https://doi.org/10.3390/biomedicines11010132
Villafaina S, Tomas-Carus P, Silva V, Costa AR, Fernandes O, Parraca JA. The Behavior of Muscle Oxygen Saturation, Oxy and Deoxy Hemoglobin during a Fatigue Test in Fibromyalgia. Biomedicines. 2023; 11(1):132. https://doi.org/10.3390/biomedicines11010132
Chicago/Turabian StyleVillafaina, Santos, Pablo Tomas-Carus, Vanda Silva, Ana Rodrigues Costa, Orlando Fernandes, and Jose A. Parraca. 2023. "The Behavior of Muscle Oxygen Saturation, Oxy and Deoxy Hemoglobin during a Fatigue Test in Fibromyalgia" Biomedicines 11, no. 1: 132. https://doi.org/10.3390/biomedicines11010132
APA StyleVillafaina, S., Tomas-Carus, P., Silva, V., Costa, A. R., Fernandes, O., & Parraca, J. A. (2023). The Behavior of Muscle Oxygen Saturation, Oxy and Deoxy Hemoglobin during a Fatigue Test in Fibromyalgia. Biomedicines, 11(1), 132. https://doi.org/10.3390/biomedicines11010132