
Pathological Cycle between Pain, Insomnia, and Anxiety in Women with Fibromyalgia and its Association with Disease Impact

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Means, Standard Deviations, Minimum, Maximum and Pearson Correlations between the Study Variables
3.3. Testing of Mediation Models
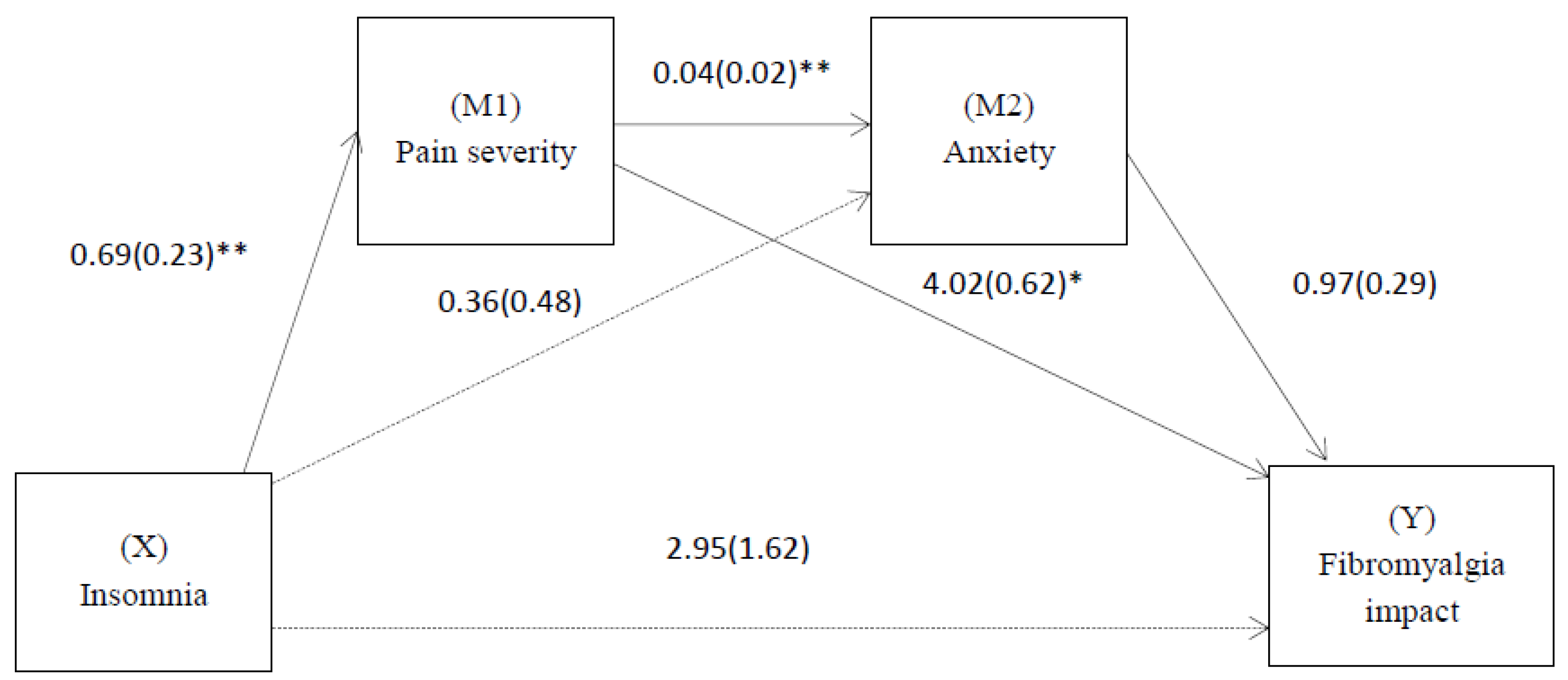
3.4. Effect of Insomnia on the Impact of Fibromyalgia through Pain Severity and Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marques, A.P.; Santo, A.S.D.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. (Engl. Ed.) 2017, 57, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Montero, P.J.; Segura-Jimenez, V.; Alvarez-Gallardo, I.C.; Nijs, J.; Mannerkorpi, K.; Delgado-Fernandez, M.; van Wilgen, C.P. Fibromyalgia impact score in women with fibromyalgia across southern, central, and Northern Areas of Europe. Pain Physician 2019, 22, E511. [Google Scholar] [PubMed]
- Pérez-Aranda, A.; Andrés-Rodríguez, L.; Feliu-Soler, A.; Núñez, C.; Stephan-Otto, C.; Pastor-Mira, M.A.; López-Roig, S.; Peñacoba, C.; Calandre, E.P.; Slim, M.; et al. Clustering a large Spanish sample of patients with fibromyalgia using the Fibromyalgia Impact Questionnaire–Revised: Differences in clinical outcomes, economic costs, inflammatory markers, and gray matter volumes. Pain 2019, 160, 908–921. [Google Scholar] [CrossRef]
- Choy, E.H.S. The role of sleep in pain and fibromyalgia. Nat. Rev. Rheumatol. 2015, 11, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.; Vilarino, G.T.; Sieczkowska, S.M.; Coimbra, D.R.; Bevilacqua, G.G.; de Azevedo Klumb Steffens, R. The relationship between sleep quality and fibromyalgia symptoms. J. Health Psychol. 2020, 25, 1176–1186. [Google Scholar] [CrossRef]
- Haack, M.; Scott-Sutherland, J.; Santangelo, G.; Simpson, N.S.; Sethna, N.; Mullington, J.M. Pain sensitivity and modulation in primary insomnia. Eur. J. Pain 2012, 16, 522–533. [Google Scholar] [CrossRef] [Green Version]
- Krause, A.J.; Prather, A.A.; Wager, T.D.; Lindquist, M.A.; Walker, M.P. The Pain of Sleep Loss: A Brain Characterization in Humans. J. Neurosci. 2019, 39, 2291–2300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theadom, A.; Cropley, M. Dysfunctional beliefs, stress and sleep disturbance in fibromyalgia. Sleep Med. 2008, 9, 376–381. [Google Scholar] [CrossRef]
- Valrie, C.R.; Bromberg, M.H.; Palermo, T.; Schanberg, L.E. A Systematic Review of Sleep in Pediatric Pain Populations. J. Dev. Behav. Pediatr. 2013, 34, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Husak, A.J.; Bair, M.J. Chronic Pain and Sleep Disturbances: A Pragmatic Review of Their Relationships, Comorbidities, and Treatments. Pain Med. 2020, 21, 1142–1152. [Google Scholar] [CrossRef]
- Jank, R.; Gallee, A.; Boeckle, M.; Fiegl, S.; Pieh, C. Chronic Pain and Sleep Disorders in Primary Care. Pain Res. Treat. 2017, 2017, 9081802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lautenbacher, S. Sleep and pain are definitely coupled—But how tight is this coupling? Pain 2018, 159, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.L.; Araujo, P.; Frange, C.; Tufik, S. Sleep Disturbance and Pain. Chest 2018, 154, 1249–1259. [Google Scholar] [CrossRef]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Herrero Babiloni, A.; De Koninck, B.P.; Beetz, G.; De Beaumont, L.; Martel, M.O.; Lavigne, G.J. Sleep and pain: Recent insights, mechanisms, and future directions in the investigation of this relationship. J. Neural Transm. 2020, 127, 647–660. [Google Scholar] [CrossRef]
- Hadlandsmyth, K.; Dailey, D.L.; Rakel, B.A.; Zimmerman, M.B.; Vance, C.G.; Merriwether, E.N.; Chimenti, R.L.; Geasland, K.M.; Crofford, L.J.; Sluka, K.A. Somatic symptom presentations in women with fibromyalgia are differentially associated with elevated depression and anxiety. J. Health Psychol. 2020, 25, 819–829. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; Reyes del Paso, G.A. Depression and trait-anxiety mediate the influence of clinical pain on health-related quality of life in fibromyalgia. J. Affect. Disord. 2020, 265, 486–495. [Google Scholar] [CrossRef]
- Mory, L.-N.; de Oliveira Fernandes, D.; Mancini, C.; Mouthon, M.; Chabwine, J.N. The Affective Dimension of Pain Appears to Be Determinant within a Pain–Insomnia–Anxiety Pathological Loop in Fibromyalgia: A Case-Control Study. J. Clin. Med. 2022, 11, 3296. [Google Scholar] [CrossRef]
- Rainville, P. Brain mechanisms of pain affect and pain modulation. Curr. Opin. Neurobiol. 2002, 12, 195–204. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Penacho, A. Viviendo Con Fibromialgia. La Vision del Afectado. In Fibromialgia y Promoción de la Salud. Herramientas de Intervención Psicosocial; Peñacoba, C., Ed.; Editorial Dykinson: Madrid, Spain, 2012; pp. 29–43. [Google Scholar]
- Fernandez-Mendoza, J.; Rodriguez-Muñoz, A.; Vela-Bueno, A.; Olavarrieta-Bernardino, S.; Calhoun, S.L.; Bixler, E.O.; Vgontzas, A.N. The Spanish version of the Insomnia Severity Index: A confirmatory factor analysis. Sleep Med. 2012, 13, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Turner, L.R.; Turner, J.A.; Romano, J.M. The use of multiple-item scales for pain intensity measurement in chronic pain patients. Pain 1996, 67, 35–40. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Fisher, L.D. Comparative reliability and validity of chronic pain intensity measures. Pain 1999, 83, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Salgueiro, M.; García-Leiva, J.M.; Ballesteros, J.; Hidalgo, J.; Molina, R.; Calandre, E.P. Validation of a Spanish version of the Revised Fibromyalgia Impact Questionnaire (FIQR). Health Qual. Life Outcomes 2013, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.A.; Arnold, L.M. Measures Applied to the Assessment of Fibromyalgia: Fibromyalgia Impact Questionnaire (FIQ), Brief Pain Inventory (BPI), the Multidimensional Fatigue Inventory (MFI-20), the MOS Sleep Scale, and the Multiple Ability Self-Report Questionnaire (MASQ; cognit. Arthritis Care Res. (Hoboken) 2011, 63, 86–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabrera, V.; Martín-Aragón, M.; del Carmen Terol, M.; Núñez, R.; Pastor, M.; de los, Á. La Escala de Ansiedad y Depresión Hospitalaria (HAD) en fibromialgia: Análisis de sensibilidad y especificidad. Ter. Psicológica 2015, 33, 181–193. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM Corp IBM SPSS Statistics for Windows, Version 22.0; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Hu, L.; Bentler, P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternative. Struct Equ. Model 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods, Instruments, Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- de Souza, J.B.; Goffaux, P.; Julien, N.; Potvin, S.; Charest, J.; Marchand, S. Fibromyalgia subgroups: Profiling distinct subgroups using the Fibromyalgia Impact Questionnaire. A preliminary study. Rheumatol. Int. 2009, 29, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Angarita-Osorio, N.; Pérez-Aranda, A.; Feliu-Soler, A.; Andrés-Rodríguez, L.; Borràs, X.; Suso-Ribera, C.; Slim, M.; Herrera-Mercadal, P.; Fernández-Vergel, R.; Blanco, M.E.; et al. Patients With Fibromyalgia Reporting Severe Pain but Low Impact of the Syndrome: Clinical and Pain-Related Cognitive Features. Pain Pract. 2019, 20, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Córdoba-Torrecilla, S.; Aparicio, V.A.; Soriano-Maldonado, A.; Estévez-López, F.; Segura-Jiménez, V.; Álvarez-Gallardo, I.; Femia, P.; Delgado-Fernández, M. Physical fitness is associated with anxiety levels in women with fibromyalgia: The al-Ándalus project. Qual. Life Res. 2016, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- McCrae, C.S.; Craggs, J.G.; Curtis, A.F.; Nair, N.; Kay, D.; Staud, R.; Berry, R.B.; Robinson, M.E. Neural activation changes in response to pain following cognitive behavioral therapy for patients with comorbid fibromyalgia and insomnia: A pilot study. J. Clin. Sleep Med. 2022, 18, 203–215. [Google Scholar] [CrossRef]
- Serdaroglu Beyazal, M.; Tufekci, A.; Kirbas, S.; Topaloglu, M.S. The Impact of Fibromyalgia on Disability, Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Migraine. Noro Psikiyatr. Ars. 2016, 55, 140–145. [Google Scholar] [CrossRef]
- Wiffen, P.J.; Derry, S.; Moore, R.A.; Aldington, D.; Cole, P.; Rice, A.S.; Lunn, M.P.; Hamunen, K.; Haanpaa, M.; Kalso, E.A. Antiepileptic drugs for neuropathic pain and fibromyalgia-an overview of Cochrane reviews. Cochrane Database Syst. Rev. 2013, CD010567. [Google Scholar] [CrossRef]
- Geiger-Brown, J.M.; Rogers, V.E.; Liu, W.; Ludeman, E.M.; Downton, K.D.; Diaz-Abad, M. Cognitive behavioral therapy in persons with comorbid insomnia: A meta-analysis. Sleep Med. Rev. 2015, 23, 54–67. [Google Scholar] [CrossRef]
- Lewandowski, A.S.; Palermo, T.M.; De la Motte, S.; Fu, R. Temporal daily associations between pain and sleep in adolescents with chronic pain versus healthy adolescents. Pain 2010, 151, 220–225. [Google Scholar] [CrossRef] [Green Version]
- Affleck, G.; Urrows, S.; Tennen, H.; Higgins, P.; Abeles, M. Sequential daily relations of sleep, pain intensity, and attention to pain among women with fibromyalgia. Pain 1996, 68, 363–368. [Google Scholar] [CrossRef]


{kind=link}
| Model | Predictor (X) | Mediator | Outcome (Y) |
|---|---|---|---|
| 1 | Insomnia | Pain severity | Anxiety |
| 2 | Insomnia | Anxiety | Pain severity |
| 3 | Pain severity | Insomnia | Anxiety |
| 4 | Pain severity | Anxiety | Insomnia |
| 5 | Anxiety | Pain severity | Insomnia |
| 6 | Anxiety | Insomnia | Pain severity |
| Mean (SD) | Range Sample | 2 | 3 | 4 | |
|---|---|---|---|---|---|
| 1. Pain severity | 7.23 (1.49) | 1–10 | 0.22 ** | 0.34 ** | 0.58 ** |
| 2. Anxiety | 12.17 (3.69) | 4–21 | 0.23 ** | 0.37 ** | |
| 3. Insomnia | 8.85 (2.35) | 0–11 | 0.58 ** | ||
| 4. Fibromyalgia impact | 75.21 (18.42) | 6–110 |
| Model | Effect | SE | Boot LLCI | Boot LLCI |
|---|---|---|---|---|
| 1 | 0.011 | 0.007 | 0.001 | 0.036 |
| 2 | 0.066 | 0.053 | −0.019 | 0.189 |
| 3 | 0.036 | 0.048 | −0.040 | 0.153 |
| 4 | 0.006 | 0.010 | −0.012 | 0.018 |
| 5 | 0.300 | 0.184 | −0.001 | 0.694 |
| 6 | 0.041 | 0.012 | −0.002 | 0.044 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalá, P.; Gutiérrez, L.; Écija, C.; Peñacoba, C. Pathological Cycle between Pain, Insomnia, and Anxiety in Women with Fibromyalgia and its Association with Disease Impact. Biomedicines 2023, 11, 148. https://doi.org/10.3390/biomedicines11010148
Catalá P, Gutiérrez L, Écija C, Peñacoba C. Pathological Cycle between Pain, Insomnia, and Anxiety in Women with Fibromyalgia and its Association with Disease Impact. Biomedicines. 2023; 11(1):148. https://doi.org/10.3390/biomedicines11010148
Chicago/Turabian StyleCatalá, Patricia, Lorena Gutiérrez, Carmen Écija, and Cecilia Peñacoba. 2023. "Pathological Cycle between Pain, Insomnia, and Anxiety in Women with Fibromyalgia and its Association with Disease Impact" Biomedicines 11, no. 1: 148. https://doi.org/10.3390/biomedicines11010148
APA StyleCatalá, P., Gutiérrez, L., Écija, C., & Peñacoba, C. (2023). Pathological Cycle between Pain, Insomnia, and Anxiety in Women with Fibromyalgia and its Association with Disease Impact. Biomedicines, 11(1), 148. https://doi.org/10.3390/biomedicines11010148