
Central Sensitization and Psychological State Distinguishing Complex Regional Pain Syndrome from Other Chronic Limb Pain Conditions: A Cluster Analysis Model
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Disease Severity Measures
2.2.1. CRPS Severity Score
2.2.2. Short-Form McGill Pain Questionnaire (MPQ-SF)
2.3. Psychophysical Measures
2.3.1. Thermal and Pain Thresholds
2.3.2. Mechanical Hyperalgesia Intensity
2.3.3. Static Mechanical Allodynia Intensity
2.3.4. Dynamic Mechanical Allodynia Intensity
2.3.5. Dynamic Allodynia Area
2.3.6. Aftersensation Intensity
2.4. Psychological Self-Reported Measures
2.4.1. Pain Catastrophizing Scale (PCS) [35]
2.4.2. Tampa Scale of Kinesiophobia (TSK) [37]
2.4.3. Beck Depression Inventory (BDI-II) [39]
2.4.4. Brief Symptom Inventory (BSI) [41]
2.4.5. Cambridge Depersonalization Scale (CDS) [43]
2.4.6. The Bath Body Perception Disturbances Questionnaire (Bath-BPD) [45]
2.5. Biological Measures
Pro-Inflammatory Cytokines
2.6. Statistical Analysis
Missing Variables
2.7. The Study Protocol
3. Results
3.1. Patients
3.2. Thermal and Pain Thresholds Profile
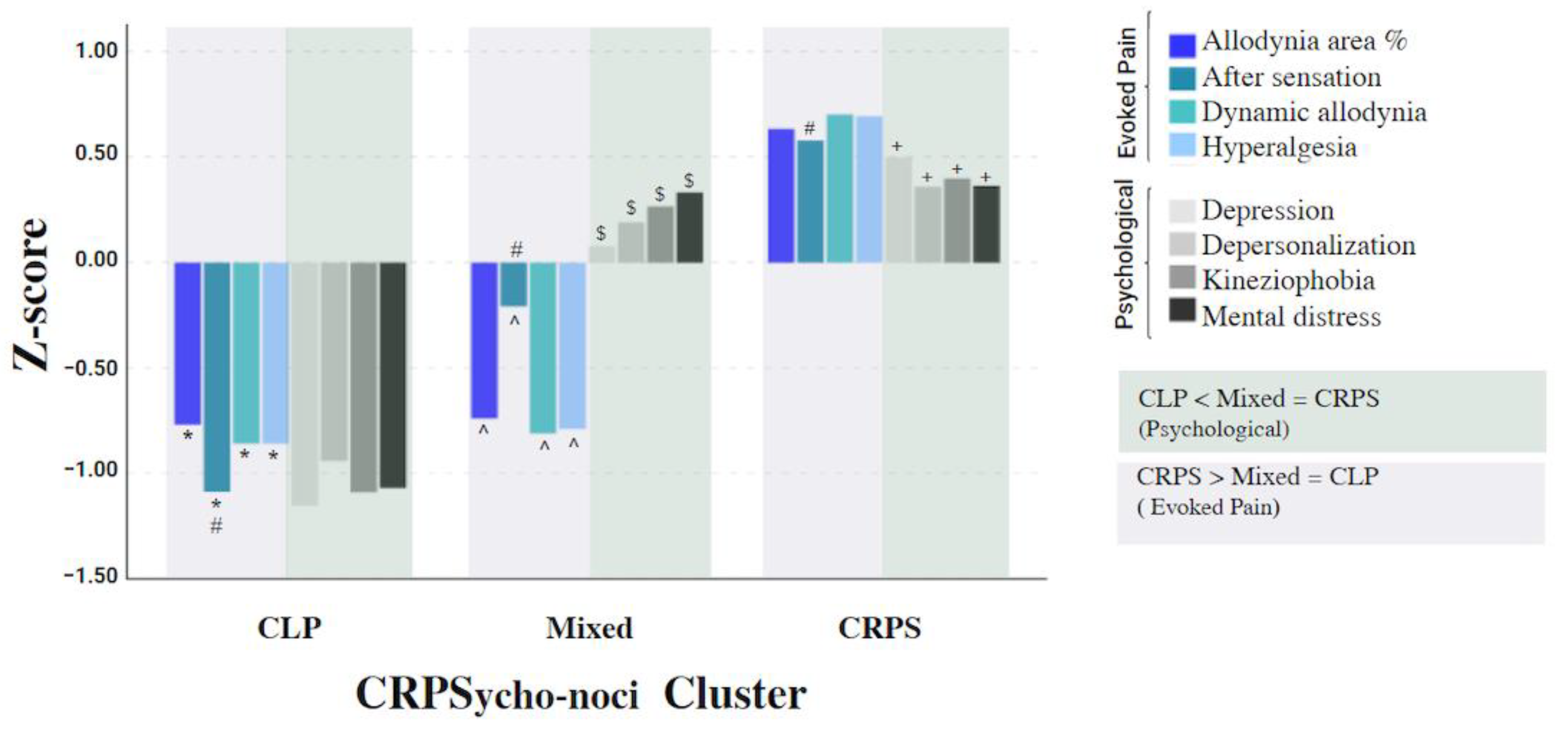
3.3. The Cluster Analysis Model
3.4. The Model Sensitivity
3.5. Correlation between the Pro-Inflammatory Cytokines and the Pain Measures
4. Discussion
4.1. Central Sensitization Processes That Differ between the Cluster Groups
4.2. Psychological State Differences between the Cluster Groups
4.3. The Mutual Association between Pain Hypersensitivity and Psychological State
4.4. TNF-α and Central Neuro-Inflammation Processes
4.5. BPD in CRPS
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harden, N.; McCabe, C.S.; Goebel, A.; Massey, M.; Suvar, T.; Grieve, S.; Bruehl, S. Complex Regional Pain Syndrome: Practical Diagnostic and Treatment Guidelines, 5th Edition. Pain Med. 2022, 23, S1–S53. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; McDonnell, P.; Gershwin, M.E. Complex regional pain syndrome—Autoimmune or functional neurologic syndrome. J. Transl. Autoimmun. 2021, 4, 100080. [Google Scholar] [CrossRef] [PubMed]
- Ott, S.; Maihöfner, C. Signs and Symptoms in 1,043 Patients with Complex Regional Pain Syndrome. J. Pain 2018, 19, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Harden, N.; Bruehl, S.; Perez, R.S.G.M.; Birklein, F.; Marinus, J.; Maihofner, C.; Lubenow, T.; Buvanendran, A.; Mackey, S.; Graciosa, J.; et al. Development of a severity score for CRPS. Pain 2010, 151, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, P.; Benrud-Larson, L.M.; Mcclelland, R.L.; Low, P.A. Complex regional pain syndrome type I: Incidence and prevalence in Olmsted county, a population-based study. Pain 2003, 103, 199–207. [Google Scholar] [CrossRef]
- De Mos, M.; de Bruijn, A.G.J.; Huygen, F.J.P.M.; Dieleman, J.P.; Stricker, B.H.C.; Sturkenboom, M.C.J.M. The incidence of complex regional pain syndrome: A population-based study. Pain 2007, 129, 12–20. [Google Scholar] [CrossRef]
- Kim, H.; Lee, C.H.; Kim, S.H.; Kim, Y.D. Epidemiology of complex regional pain syndrome in Korea: An electronic population health data study. PLoS ONE 2018, 13, e0198147. [Google Scholar] [CrossRef] [Green Version]
- Nicholas, M.; Vlaeyen, J.W.S.; Rief, W.; Barke, A.; Aziz, Q.; Benoliel, R.; Cohen, M.; Evers, S.; Giamberardino, M.A.; Goebel, A.; et al. The IASP classification of chronic pain for ICD-11: Chronic primary pain. Pain 2019, 160, 28–37. [Google Scholar] [CrossRef]
- Fitzcharles, M.-A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef]
- Dimova, V.; Herrnberger, M.S.; Escolano-Lozano, F.; Rittner, H.L.; Vlckova, E.; Sommer, C.; Maihöfner, C.; Birklein, F. Clinical phenotypes and classification algorithm for complex regional pain syndrome. Neurology 2020, 94, e357–e367. [Google Scholar] [CrossRef]
- Bruehl, S.; Maihöfner, C.; Stanton-Hicks, M.; Perez, R.S.G.M.; Vatine, J.J.; Brunner, F.; Birklein, F.; Schlereth, T.; Mackey, S.; Mailis-Gagnon, A.; et al. Complex regional pain syndrome: Evidence for warm and cold subtypes in a large prospective clinical sample. Pain 2016, 157, 1674–1681. [Google Scholar] [CrossRef] [PubMed]
- Bruehl, S. Complex regional pain syndrome. BMJ 2015, 351, h2730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangnus, T.J.P.; Bharwani, K.D.; Dirckx, M.; Huygen, F.J.P.M. From a Symptom-Based to a Mechanism-Based Pharmacotherapeutic Treatment in Complex Regional Pain Syndrome. Drugs 2022, 82, 511–531. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.M.; Peterlin, B.L.; Perreault, M.J.; Grothusen, J.R.; Schwartzman, R.J. Changes in plasma cytokines and their soluble receptors in complex regional pain syndrome. J. Pain 2012, 13, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Libon, D.J.; Schwartzman, R.J.; Eppig, J.; Wambach, D.; Brahin, E.; Peterlin, B.L.; Alexander, G.; Kalanuria, A. Neuropsychological deficits associated with Complex Regional Pain Syndrome. J. Int. Neuropsychol. Soc. 2010, 16, 566–573. [Google Scholar] [CrossRef]
- Ten Brink, A.F.; Bultitude, J.H. Predictors of Self-Reported Neglect-like Symptoms and Involuntary Movements in Complex Regional Pain Syndrome Compared to Other Chronic Limb Pain Conditions. Pain Med. 2021, 22, 2337–2349. [Google Scholar] [CrossRef]
- Goebel, A.; Birklein, F.; Brunner, F.; Clark, J.D.; Gierthmühlen, J.; Harden, N.; Huygen, F.; Knudsen, L.; McCabe, C.; Lewis, J.; et al. The Valencia consensus-based adaptation of the IASP complex regional pain syndrome diagnostic criteria. Pain 2021, 162, 2346–2348. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Chronic primary musculoskeletal pain: A new concept of nonstructural regional pain. Pain Rep. 2022, 7, e1024. [Google Scholar] [CrossRef]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Perrot, S.; Cohen, M.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.-D.; IASP Taskforce for the Classification of Chronic Pain. The IASP classification of chronic pain for ICD-11: Chronic secondary musculoskeletal pain. Pain 2019, 160, 77–82. [Google Scholar] [CrossRef]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.-A.; Rice, A.S.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef] [PubMed]
- Dietz, C.; Müller, M.; Reinhold, A.K.; Karch, L.; Schwab, B.; Forer, L.; Vlckova, E.; Brede, E.-M.; Jakubietz, R.; Üçeyler, N.; et al. What is normal trauma healing and what is complex regional pain syndrome I? An analysis of clinical and experimental biomarkers. Pain 2019, 160, 2278–2289. [Google Scholar] [CrossRef] [PubMed]
- Alam, O.H.; Zaidi, B.; Pierce, J.; Moser, S.E.; Hilliard, P.E.; Golmirzaie, G.; Brummett, C.M. Phenotypic features of patients with complex regional pain syndrome compared with those with neuropathic pain. Reg. Anesth. Pain Med. 2019, 44, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Michal, M.; Adler, J.; Reiner, I.; Wermke, A.; Ackermann, T.; Schlereth, T.; Birklein, F. Association of Neglect-Like Symptoms with Anxiety, Somatization, and Depersonalization in Complex Regional Pain Syndrome. Pain Med. 2017, 18, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Farzad, M.; MacDermid, J.C.; Packham, T.; Khodabandeh, B.; Vahedi, M.; Shafiee, E. Factors associated with disability and pain intensity in patients with complex regional pain syndrome. Disabil. Rehabil. 2022, 44, 8243–8251. [Google Scholar] [CrossRef]
- Bean, D.J.; Johnson, M.H.; Kydd, R.R. Relationships Between Psychological Factors, Pain, and Disability in Complex Regional Pain Syndrome and Low Back Pain. Clin. J. Pain 2014, 30, 647–653. [Google Scholar] [CrossRef] [Green Version]
- Harden, N.; Maihofner, C.; Abousaad, E.; Vatine, J.J.; Kirsling, A.; Perez, R.S.G.M.; Kuroda, M.; Brunner, F.; Stanton-Hicks, M.; Marinus, J.; et al. A prospective, multisite, international validation of the Complex Regional Pain Syndrome Severity Score. Pain 2017, 158, 1430–1436. [Google Scholar] [CrossRef]
- Melzack, R. The short-form McGill pain questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef]
- Sloman, R.; Rosen, G.; Rom, M.; Shir, Y. Nurses’ assessment of pain in surgical patients. J. Adv. Nurs. 2005, 52, 125–132. [Google Scholar] [CrossRef]
- Treede, R.D.; Magerl, W. Multiple mechanisms of secondary hyperalgesia. Prog. Brain Res. 2000, 129, 331–341. [Google Scholar] [CrossRef]
- Rolke, R.; Magerl, W.; Campbell, K.A.; Schalber, C.; Caspari, S.; Birklein, F.; Treede, R.-D. Quantitative sensory testing: A comprehensive protocol for clinical trials. Eur. J. Pain 2006, 10, 77. [Google Scholar] [CrossRef] [PubMed]
- Packham, T.L.; Spicher, C.J.; MacDermid, J.C.; Michlovitz, S.; Buckley, D.N. Somatosensory rehabilitation for allodynia in complex regional pain syndrome of the upper limb: A retrospective cohort study. J. Hand Ther. 2018, 31, 10–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karpin, H.; Shmueli, S.; Turgeman, N.; Weissman-Fogel, I.; Vatin, J.J. A new allodynography quantification method for somatosensory rehabilitation in Complex Regional Pain Syndrome. In Proceedings of the 11th Congress of the European Pain Federation, Valencia, Spain, 4–7 September 2019. [Google Scholar]
- Lund, C.C.; Browder, N.C. The estimation of areas of burns. Surg. Gynecol. Obst. 1944, 79, 352–358. [Google Scholar]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Granot, M.; Ferber, S.G. The Roles of Pain Catastrophizing and Anxiety in the Prediction of Postoperative Pain Intensity—A Prospective Study. Pain 2005, 21, 439–445. [Google Scholar] [CrossRef]
- Miller, R.P.; Kori, S.H.; Todd, D.D. Miller, R.P.; Kori, S.H.; Todd, D.D. The Tampa Scale—A measiure of kinesiophobia. Clin. J. Pain 1991, 7, 51. [Google Scholar] [CrossRef]
- Sarig Bahat, H.; Weiss, P.L.T.; Sprecher, E.; Krasovsky, A.; Laufer, Y. Do neck kinematics correlate with pain intensity, neck disability or with fear of motion? Man. Ther. 2014, 19, 252–258. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G. Beck Depression Inventory–II (BDI-II). Psychol. Assess. 1996, 67, 588–597. [Google Scholar]
- BDI-II Guide, 2nd ed.; Psyctech: Jerusalem, Israel, 2010.
- Derogatis, L.R.; Melisaratos, N. The brief symptom inventory: An introductory report. Psychol. Med. 1983, 13, 595–605. [Google Scholar] [CrossRef] [Green Version]
- Canetti, L.; Kaplan De-Nour, A.; Shalev, A.Y. Israeli adolescents’ norms of the Brief Symptom Inventory (BSI). Isr. J. Psychiatry Relat. Sci. 1994, 31, 13–18. [Google Scholar]
- Sierra, M.; Berrios, G.E. The Cambridge Depersonalisation Scale: A new instrument for the measurement of depersonalisation. Psychiatry Res. 2000, 93, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.; McCabe, C. Body perception disturbance (BPD) in CRPS. Pract. Pain Manag. 2010, 60–66. [Google Scholar]
- Vallerand, R.J.; Pelletier, L.G.; Blais, M.R.; Briere, N.M.; Senecal, C.; Vallieres, E.F. The Academic Motivation Scale: A measure of intrinsic, extrinsic, and amotivation in education. Educ. Psychol. Meas. 1992, 52, 1003–1017. [Google Scholar] [CrossRef]
- Lewis, J.S.; Schweinhardt, P. Perceptions of the painful body: The relationship between body perception disturbance, pain and tactile discrimination in complex regional pain syndrome. Eur. J. Pain 2012, 16, 1320–1330. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Tkaczynski, A. Segmentation using two-step cluster analysis. In Segmentation in Social Marketing; Springer: Singapore, 2017; pp. 109–125. [Google Scholar]
- Schwarz, G. Estimating the Dimension of a Model. Ann. Stat. 1978, 6, 261–464. [Google Scholar] [CrossRef]
- Rousseeuw, P.J. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. J. Comput. Appl. Math. 1987, 20, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Baraldi, A.N.; Enders, C.K. An introduction to modern missing data analyses. J. Sch. Psychol. 2010, 48, 5–37. [Google Scholar] [CrossRef] [PubMed]
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: Definitions, diagnosis, and management. Lancet 2000, 356, 1255–1259. [Google Scholar] [CrossRef]
- Woolf, C.J.; Warner, D.S.; Ch, B. Central Sensitization Uncovering the Relation between Pain and Plasticity. Anesthesiology 2007, 106, 864–867. [Google Scholar] [CrossRef] [Green Version]
- Seifert, F.; Kiefer, G.; Decol, R.; Schmelz, M.; Maihöfner, C. Differential endogenous pain modulation in complex-regional pain syndrome. Brain 2009, 132, 788–800. [Google Scholar] [CrossRef]
- Nijs, J.; Lahousse, A.; Kapreli, E.; Bilika, P.; Saraçoğlu, İ.; Malfliet, A.; Coppieters, I.; De Baets, L.; Leysen, L.; Roose, E.; et al. Nociplastic pain criteria or recognition of central sensitization? Pain phenotyping in the past, present and future. J. Clin. Med. 2021, 10, 3203. [Google Scholar] [CrossRef]
- Yarnitsky, D. Role of endogenous pain modulation in chronic pain mechanisms and treatment. Pain 2015, 156, S24–S31. [Google Scholar] [CrossRef] [PubMed]
- Yarnitsky, D.; Granot, M.; Granovsky, Y. Pain modulation profile and pain therapy: Between pro- and antinociception. Pain 2014, 155, 663–665. [Google Scholar] [CrossRef]
- Birklein, F.; Ajit, S.K.; Goebel, A.; Perez, R.S.G.M.; Sommer, C. Complex regional pain syndrome-phenotypic characteristics and potential biomarkers. Nat. Rev. Neurol. 2018, 14, 272–284. [Google Scholar] [CrossRef]
- Moseley, G.L.; Herbert, R.D.; Parsons, T.; Lucas, S.; van Hilten, J.J.; Marinus, J. Intense pain soon after wrist fracture strongly predicts who will develop complex regional pain syndrome: Prospective cohort study. J. Pain 2014, 15, 16–23. [Google Scholar] [CrossRef]
- Harden, R.N.; Oaklander, A.L.; Burton, A.W.; Perez, R.S.G.M.; Richardson, M.K.; Swan, O.M.; Barthel, M.J.; Costa, C.B.; Graciosa, B.J.R.; Bruehl, S. Complex Regional Pain Syndrome: Practical Diagnostic and Treatment Guidelines, 4th Edition. Pain Med. 2013, 14, 180–229. [Google Scholar] [CrossRef] [Green Version]
- Ji, R.-R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and central sensitization in chronic and widespread pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef]
- Bharwani, K.D.; Dik, W.A.; Dirckx, M.; Huygen, F.J.P.M. Highlighting the Role of Biomarkers of Inflammation in the Diagnosis and Management of Complex Regional Pain Syndrome. Mol. Diagn. Ther. 2019, 23, 615–626. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R. Medical Hypotheses Individual differences in endogenous pain modulation as a risk factor for chronic pain. Neurology 2005, 65, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Zaslansky, R.; Yarnitsky, D. Clinical applications of quantitative sensory testing (QST). J. Neurol. Sci. 1998, 153, 215–238. [Google Scholar] [CrossRef]
- Gottrup, H.; Kristensen, A.D.; Bach, F.W.; Jensen, T.S. Aftersensations in experimental and clinical hypersensitivity. Pain 2003, 103, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Morisset, V.; Nagy, F. Plateau potential-dependent windup of the response to primary afferent stimuli in rat dorsal horn neurons. Eur. J. Neurosci. 2000, 12, 3087–3095. [Google Scholar] [CrossRef]
- Monteiro, C.; Lima, D.; Galhardo, V. Switching-on and -off of bistable spontaneous discharges in rat spinal deep dorsal horn neurons. Neurosci. Lett. 2006, 398, 258–263. [Google Scholar] [CrossRef]
- Wolanin, M.W.; Schwartzman, R.J.; Alexander, G.; Grothusen, J. Loss of Surround Inhibition and After Sensation as Diagnostic Parameters of Complex Regional Pain Syndrome. Neurosci. Med. 2012, 03, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Sheng, J.; Liu, S.; Wang, Y.; Cui, R.; Zhang, X. The Link between Depression and Chronic Pain: Neural Mechanisms in the Brain. Neural. Plast. 2017, 2017, 9724371. [Google Scholar] [CrossRef] [Green Version]
- Yin, C.; Jia, T.; Luan, Y.; Zhang, X.; Xiao, C.; Zhou, C. A nigra–subthalamic circuit is involved in acute and chronic pain states. Pain 2022, 163, 1952–1966. [Google Scholar] [CrossRef]
- Margalit, D.; ben Har, L.; Brill, S.; Vatine, J.J. Complex regional pain syndrome, alexithymia, and psychological distress. J. Psychosom. Res. 2014, 77, 273–277. [Google Scholar] [CrossRef]
- Park, H.Y.; Jang, Y.E.; Oh, S.; Lee, P.B. Psychological characteristics in patients with chronic complex regional pain syndrome: Comparisons with patients with major depressive disorder and other types of chronic pain. J. Pain Res. 2020, 13, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Bean, D.J.; Johnson, M.H.; Heiss-Dunlop, W.; Kydd, R.R. Extent of recovery in the first 12 months of complex regional pain syndrome type-1: A prospective study. Eur. J. Pain 2016, 20, 884–894. [Google Scholar] [CrossRef]
- De Jong, J.R.; Vlaeyen, J.W.S.; de Gelder, J.M.; Patijn, J. Pain-related fear, perceived harmfulness of activities, and functional limitations in complex regional pain syndrome type I. J. Pain 2011, 12, 1209–1218. [Google Scholar] [CrossRef]
- Marinus, J.; Perez, R.S.; van Eijs, F.; van Gestel, M.A.; Geurts, J.J.; Huygen, F.J.; Bauer, M.C.; van Hilten, J.J. The Role of Pain Coping and Kinesiophobia in Patients with Complex Regional Pain Syndrome Type 1 of the Legs. Clin. J. Pain 2013, 29, 563–569. [Google Scholar] [CrossRef]
- Luque-Suarez, A.; Martinez-Calderon, J.; Falla, D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: A systematic review. Br. J. Sport. Med. 2019, 53, 554–559. [Google Scholar] [CrossRef]
- Antunovich, D.R.; Horne, J.C.; Tuck, N.L.; Bean, D.J. Are Illness Perceptions Associated with Pain and Disability in Complex Regional Pain Syndrome? A Cross-Sectional Study. Pain Med. 2021, 22, 100–111. [Google Scholar] [CrossRef]
- Mansour, A.R.; Farmer, M.A.; Baliki, M.N.; Apkarian, A.V. Chronic pain: The role of learning and brain plasticity. Restor. Neurol. Neurosci. 2014, 32, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.M.; Neugebauer, V. Amygdala Plasticity and Pain. Pain Res. Manag. 2017, 2017, 8296501. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Chang, M.C. Chronic pain: Structural and functional changes in brain structures and associated negative affective states. Int. J. Mol. Sci. 2019, 20, 3130. [Google Scholar] [CrossRef] [Green Version]
- Maihöfner, C.; Handwerker, H.O.; Birklein, F. Functional imaging of allodynia in complex regional pain syndrome. Neurology 2006, 66, 711–717. [Google Scholar] [CrossRef]
- Maihfner, C.; Forster, C.; Birklein, F.; Neundörfer, B.; Handwerker, H.O. Brain processing during mechanical hyperalgesia in complex regional pain syndrome: A functional MRI study. Pain 2005, 114, 93–103. [Google Scholar] [CrossRef]
- Gilam, G.; Gross, J.J.; Wager, T.D.; Keefe, F.J.; Mackey, S.C. What Is the Relationship between Pain and Emotion? Bridging Constructs and Communities. Neuron 2020, 107, 17–21. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Latremoliere, A.; Woolf, C.J. Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef] [Green Version]
- Harte, S.E.; Harris, R.E.; Clauw, D.J. The neurobiology of central sensitization. J. Appl. Biobehav. Res. 2018, 23, e12137. [Google Scholar] [CrossRef]
- Adams, L.M.; Turk, D.C. Central sensitization and the biopsychosocial approach to understanding pain. J. Appl. Biobehav. Res. 2018, 23, e12125. [Google Scholar] [CrossRef]
- Baral, P.; Udit, S.; Chiu, I.M. Pain and immunity: Implications for host defence. Nat. Rev. Immunol. 2019, 19, 433–447. [Google Scholar] [CrossRef]
- Reimer, M.; Rempe, T.; Diedrichs, C.; Baron, R.; Gierthmühlen, J. Sensitization of the nociceptive system in complex regional pain syndrome. PLoS ONE 2016, 11, e0154553. [Google Scholar] [CrossRef] [Green Version]
- Li, W.W.; Guo, T.Z.; Shi, X.; Sun, Y.; Wei, T.; Clark, D.J.; Kingery, W. Substance P spinal signaling induces glial activation and nociceptive sensitization after fracture. Neuroscience 2015, 310, 73–90. [Google Scholar] [CrossRef] [Green Version]
- Pohóczky, K.; Kun, J.; Szentes, N.; Aczél, T.; Urbán, P.; Gyenesei, A.; Bölcskei, K.; Szőke, É.; Sensi, S.; Dénes, Á.; et al. Discovery of novel targets in a complex regional pain syndrome mouse model by transcriptomics: TNF and JAK-STAT pathways. Pharmacol. Res. 2022, 182, 106347. [Google Scholar] [CrossRef]
- Sommer, C.; Leinders, M.; Üçeyler, N. Inflammation in the pathophysiology of neuropathic pain. Pain 2018, 159, 595–602. [Google Scholar] [CrossRef]
- Parkitny, L.; McAuley, J.H.; di Pietro, F.; Stanton, T.R.; O’Connell, N.E.; Marinus, J.; Van Hilten, J.J.; Moseley, G.L. Inflammation in complex regional pain syndrome A systematic review and meta-analysis. Am. Acad. Neurol. 2013, 80, 106–117. [Google Scholar] [CrossRef] [Green Version]
- Hall, J.; Llewellyn, A.; Palmer, S.; Rowett-Harris, J.; Atkins, R.M.; McCabe, C.S. Sensorimotor dysfunction after limb fracture—An exploratory study. Eur. J. Pain 2016, 20, 1402–1412. [Google Scholar] [CrossRef]
- Frettlöh, J.; Hüppe, M.; Maier, C. Severity and specificity of neglect-like symptoms in patients with complex regional pain syndrome (CRPS) compared to chronic limb pain of other origins. Pain 2006, 124, 184–189. [Google Scholar] [CrossRef]
- Reinersmann, A.; Landwehrt, J.; Krumova, E.K.; Ocklenburg, S.; Güntürkün, O.; Maier, C. Impaired spatial body representation in complex regional pain syndrome type 1 (CRPS I). Pain 2012, 153, 2174–2181. [Google Scholar] [CrossRef]
- Punt, T.D.; Cooper, L.; Hey, M.; Johnson, M.I. Neglect-like symptoms in complex regional pain syndrome: Learned nonuse by another name? Pain 2013, 154, 200–203. [Google Scholar] [CrossRef]
- Kuttikat, A.; Noreika, V.; Shenker, N.; Chennu, S.; Bekinschtein, T.; Brown, C.A. Neurocognitive and neuroplastic mechanisms of novel clinical signs in CRPS. Front. Hum. Neurosci. 2016, 10, 16. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variables | CRPS | CLP | p |
|---|---|---|---|
| Patients, n | 61 | 31 | |
| Age (years), mean (SD) | 34.69 (11.52) | 39.0 (15.09) | 0.164 |
| Sex (female/male), n (%) | 32/29 (52.5/47.5) | 23/8 (74.2/25.8) | 0.044 |
| Education (years), mean (SD) | 12.93 (2.14) | 13.71 (2.25) | 0.111 |
| Disease duration (days), mean (SD) | 728.62 (903.96) | 775.81 (843.25) | 0.809 |
| Work status, n (%) | |||
| Working | 15 (24.59) | 13 (41.93) | |
| Not working | 43 (70.49) | 14 (45.16) | |
| Soldier | 3 (4.91) | 4 (12.90) | |
| Type of injury, n (%): | |||
| Fracture | 31(50.81) | 14(45.16) | |
| Trauma | 27 (44.26) | 15 (48.38) | |
| Other | 3 (4.91) | 2 (6.45) | |
| Limb involved, n (%):HandLeg | |||
| 24 (39.35) | 12 (38.7) | ||
| 37 (60.65) | 19 (61.29) | ||
| Side involved, n (%): | |||
| Rt. | 31 (50.81) | 12 (38.71) | |
| Lt. | 30 (49.19) | 19 (61.29) | |
| Nerve injury, n (%) | 38 (62.35) | 16 (51.61) | |
| Pain characteristics, mean (SD): | |||
| NRPS—Current | 7.15 (1.5) | 4.29 (2.59) | <0.001 |
| NRPS—24 H | 7.42 (1.38) | 5.11 (2.57) | <0.001 |
| Comorbid diagnosis n (%): | |||
| Cardiovascular/Hematology | 5 (8.19) | 3 (9.66) | |
| Endocrine diseases | 5 (8.19) | 1 (3.22) | |
| Enzyme deficiency/Allergies | 4 (6.55) | 1 (3.22) | |
| Neurodevelopmental disorder | 3 (4.91) | 2 (6.45) | |
| Missing | 1 (1.63) | 6 (19.35) |
| Variables, Mean (SD) | CRPS (n = 33) | CLP (n = 25) | F (1, 56) | p | η2 | ||
|---|---|---|---|---|---|---|---|
| Involved | Not involved | Involved | Not involved | ||||
| CDT | −1.74 (1.87) | −1.39 (1.45) | −2.21 (1.26) | −1.61 (1.19) | 4.08 | 0.048 | 0.068 |
| WDT | −1.26 (1.82) | −0.82 (1.55) | −1.82 (1.18) | −0.96 (1.35) | 7.27 | 0.009 | 0.115 |
| CPT | 1.19 (1.16) | 0.33 (1.21) | 0.68 (1.18) | 0.29 (1.19) | 10.74 | 0.002 | 0.161 |
| HPT | 1.15 (2.11) | 0.43 (1.61) | −0.02 (1.60) | 0−.03 (1.30) | 1.55 | ns | |
| Variables, Mean (SD) | Cluster ‘CRPS’ (n = 50) | Cluster ‘Mixed’ (n = 19) | Cluster ‘CLP’ (n = 23) | F (2, 89) | Multiple pairwise comparisons | η2 |
|---|---|---|---|---|---|---|
| Dynamic allodynia | 7.32 (1.53) | 2.11 (2.92) | 1.94 (2.78) | 64.96 * | CLP = Mixed < CRPS | 0.59 |
| Hyperalgesia | 7.72 (2.58) | 2.86 (2.99) | 2.63 (2.38) | 61.67 * | CLP = Mixed < CRPS | 0.58 |
| After-sensation | 7.66 (1.39) | 5.11 (3.47) | 2.23 (2.85) | 42.97 * | CRPS > Mixed > CLP | 0.49 |
| Allodynia area % | 5.84 (3.03) | 0.97 (1.54) | 0.87 (2.11) | 41.64 * | CLP = Mixed < CRPS | 0.48 |
| Depression | 28.55 (10.06) | 23.63 (7.11) | 9.29 (5.42) | 40.01 * | CRPS = Mixed > CLP | 0.47 |
| Kinesiophobia | 42.89 (6.08) | 41.79 (6.62) | 30.43 (7.44) | 29.89 * | CRPS = Mixed > CLP | 0.40 |
| Mental distress | 2.64 (0.57) | 2.62 (0.45) | 1.72 (0.39) | 27.81 * | CRPS = Mixed > CLP | 0.38 |
| De-personalization | 76.61 (47.29) | 68.31 (45.51) | 12.66 (18.09) | 19.21 * | CRPS = Mixed > CLP | 0.30 |
| Variables, Mean (SD) | Cluster ‘CRPS’ (n = 50) | Cluster ‘Mixed’ (n = 19) | Cluster ‘CLP’ (n = 23) | F (2, 89) | Multiple pairwise comparisons | η2 |
| CSS Score | 12.08 (2.54) | 8.93 (2.83) | 6.16 (3.28) | 36.74 ** | CRPS > Mixed > CLP | 0.45 |
| MPQ-SF | 27.22 (9.01) | 22.21 (9.63) | 10.61 (7.41) | 28.2 ** | CRPS = Mixed > CLP | 0.38 |
| Bath-BPD | 25.61 (10.07) | 21.36 (7.17) | 12.93 (10.54) | 13.49 ** | CRPS = Mixed > CLP | 0.23 |
| Variables, Median (Interquartile range) | Cluster CRPS (n = 17) | Cluster Mixed (n = 7) | Cluster CLP (n = 9) | H (2) | Multiple pairwise comparisons | r |
| TNF-α (pg/mL) | 1.27 (0.50) | 1.77 (1.28) | 0.61 (0.42) | 6.28 * | CRPS = Mixed > CLP | -0.53 |
| IL-6 (pg/mL) | 1.97 (2.48) | 1.39 (0.85) | 3.73 (1.63) | 4.15 | ns | -0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karpin, H.; Vatine, J.-J.; Bachar Kirshenboim, Y.; Markezana, A.; Weissman-Fogel, I. Central Sensitization and Psychological State Distinguishing Complex Regional Pain Syndrome from Other Chronic Limb Pain Conditions: A Cluster Analysis Model. Biomedicines 2023, 11, 89. https://doi.org/10.3390/biomedicines11010089
Karpin H, Vatine J-J, Bachar Kirshenboim Y, Markezana A, Weissman-Fogel I. Central Sensitization and Psychological State Distinguishing Complex Regional Pain Syndrome from Other Chronic Limb Pain Conditions: A Cluster Analysis Model. Biomedicines. 2023; 11(1):89. https://doi.org/10.3390/biomedicines11010089
Chicago/Turabian StyleKarpin, Hana, Jean-Jacques Vatine, Yishai Bachar Kirshenboim, Aurelia Markezana, and Irit Weissman-Fogel. 2023. "Central Sensitization and Psychological State Distinguishing Complex Regional Pain Syndrome from Other Chronic Limb Pain Conditions: A Cluster Analysis Model" Biomedicines 11, no. 1: 89. https://doi.org/10.3390/biomedicines11010089