
Donor-Derived Cell-Free DNA at 1 Month after Kidney Transplantation Relates to HLA Class II Eplet Mismatch Load

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients’ Information
2.2. dd-cfDNA Determination
2.3. Immunosuppressive Drugs Monitoring
2.4. Eplet Mismatch Examination
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
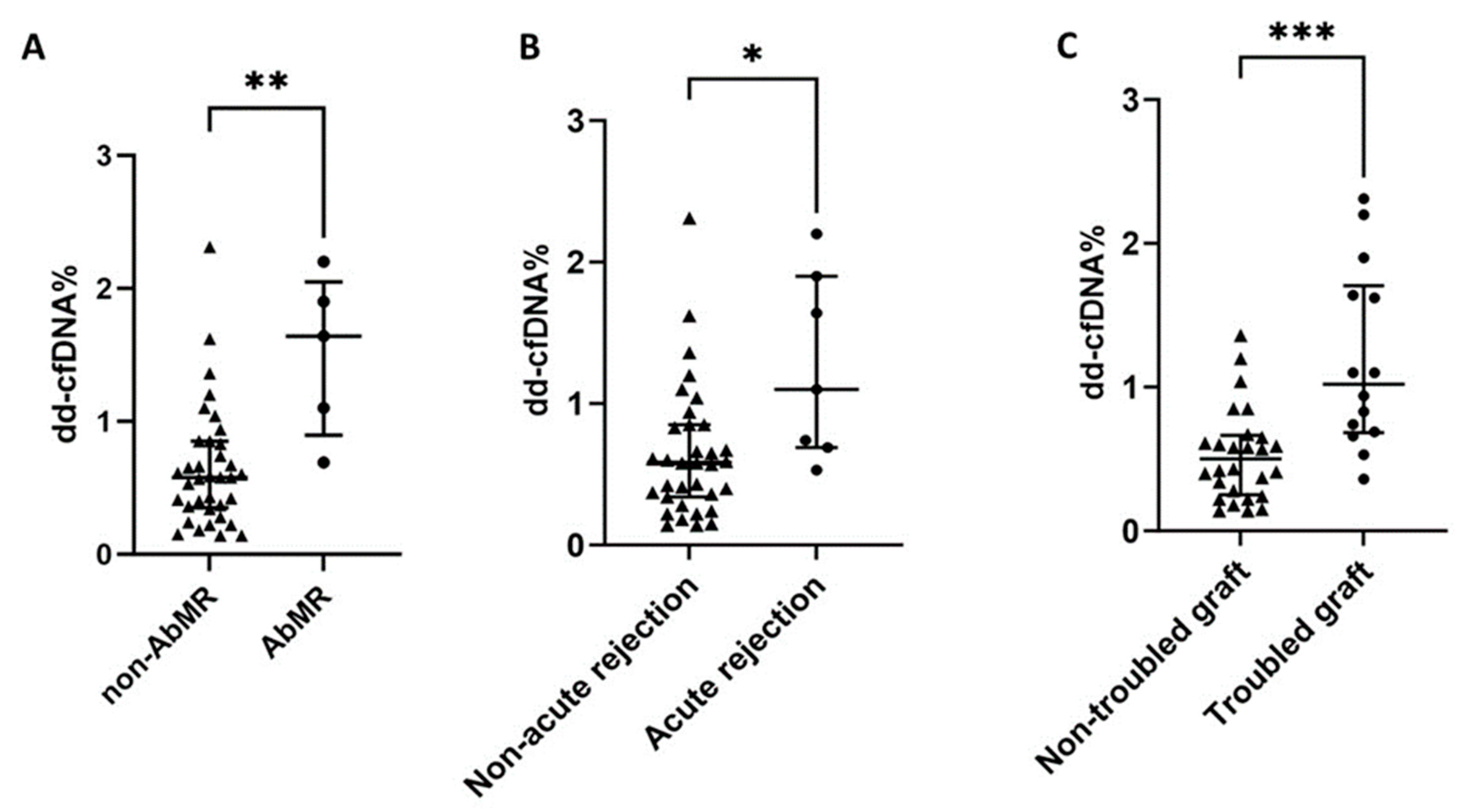
3.2. dd-cfDNA% and Troubled Graft Patients
3.3. dd-cfDNA% in AbMR Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lamb, K.E.; Lodhi, S.; Meier-Kriesche, H.U. Long-term renal allograft survival in the United States: A critical reappraisal. Am. J. Transpl. 2011, 11, 450–462. [Google Scholar] [CrossRef]
- Filippone, E.J.; Gulati, R.; Farber, J.L. Noninvasive Assessment of the Alloimmune Response in Kidney Transplantation. Adv. Chronic Kidney Dis. 2021, 28, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Petrányi, G.G. The complexity of immune and alloimmune response. Transpl. Immunol. 2002, 10, 91–100. [Google Scholar] [CrossRef]
- Lim, W.H.; Chadban, S.J.; Clayton, P.; Budgeon, C.A.; Murray, K.; Campbell, S.B.; Cohney, S.; Russ, G.R.; McDonald, S.P. Human leukocyte antigen mismatches associated with increased risk of rejection, graft failure, and death independent of initial immunosuppression in renal transplant recipients. Clin. Transpl. 2012, 26, E428–E437. [Google Scholar] [CrossRef] [PubMed]
- Sellarés, J.; de Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am. J. Transpl. 2012, 12, 388–399. [Google Scholar] [CrossRef]
- Parajuli, S.; Aziz, F.; Garg, N.; Panzer, S.E.; Joachim, E.; Muth, B.; Mohamed, M.; Blazel, J.; Zhong, W.; Astor, B.C.; et al. Histopathological characteristics and causes of kidney graft failure in the current era of immunosuppression. World J. Transpl. 2019, 9, 123–133. [Google Scholar] [CrossRef]
- Duquesnoy, R.J. HLAMatchmaker: A molecularly based algorithm for histocompatibility determination. I. Description of the algorithm. Hum. Immunol. 2002, 63, 339–352. [Google Scholar] [CrossRef]
- Duquesnoy, R.J.; Marrari, M. HLAMatchmaker: A molecularly based algorithm for histocompatibility determination. II. Verification of the algorithm and determination of the relative immunogenicity of amino acid triplet-defined epitopes. Hum. Immunol. 2002, 63, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Nickerson, P. Human leukocyte antigen mismatch and precision medicine in transplantation. Curr. Opin. Organ. Transpl. 2018, 23, 500–505. [Google Scholar] [CrossRef]
- Ehlayel, A.; Simms, K.J.A.; Ashoor, I.F. Emerging monitoring technologies in kidney transplantation. Pediatr. Nephrol. 2021, 36, 3077–3087. [Google Scholar] [CrossRef]
- Mohammadhassanzadeh, H.; Oualkacha, K.; Zhang, W.; Klement, W.; Bourdiec, A.; Lamsatfi, J.; Yi, Y.; Foster, B.; Keown, P.; Gebel, H.M.; et al. On Path to Informing Hierarchy of Eplet Mismatches as Determinants of Kidney Transplant Loss. Kidney Int. Rep. 2021, 6, 1567–1579. [Google Scholar] [CrossRef]
- Daniëls, L.; Naesens, M.; Bosmans, J.L.; Abramowicz, D.; Nagler, E.; Van Laecke, S.; Peeters, P.; Kuypers, D.; Emonds, M.P. The clinical significance of epitope mismatch load in kidney transplantation: A multicentre study. Transpl. Immunol. 2018, 50, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Lachmann, N.; Niemann, M.; Reinke, P.; Budde, K.; Schmidt, D.; Halleck, F.; Pruß, A.; Schönemann, C.; Spierings, E.; Staeck, O. Donor-Recipient Matching Based on Predicted Indirectly Recognizable HLA Epitopes Independently Predicts the Incidence of De Novo Donor-Specific HLA Antibodies Following Renal Transplantation. Am. J. Transpl. 2017, 17, 3076–3086. [Google Scholar] [CrossRef]
- Bauer, A.C.; Franco, R.F.; Manfro, R.C. Immunosuppression in Kidney Transplantation: State of the Art and Current Protocols. Curr. Pharm. Des. 2020, 26, 3440–3450. [Google Scholar] [CrossRef] [PubMed]
- Briggs, J.D. Causes of death after renal transplantation. Nephrol. Dial. Transpl. 2001, 16, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- Bloom, R.D.; Bromberg, J.S.; Poggio, E.D.; Bunnapradist, S.; Langone, A.J.; Sood, P.; Matas, A.J.; Mehta, S.; Mannon, R.B.; Sharfuddin, A.; et al. Cell-Free DNA and Active Rejection in Kidney Allografts. J. Am. Soc. Nephrol. 2017, 28, 2221–2232. [Google Scholar] [CrossRef] [PubMed]
- Josephson, M.A. Monitoring and managing graft health in the kidney transplant recipient. Clin. J. Am. Soc. Nephrol. 2011, 6, 1774–1780. [Google Scholar] [CrossRef] [PubMed]
- Quaglia, M.; Merlotti, G.; Guglielmetti, G.; Castellano, G.; Cantaluppi, V. Recent Advances on Biomarkers of Early and Late Kidney Graft Dysfunction. Int. J. Mol. Sci. 2020, 21, 5404. [Google Scholar] [CrossRef]
- Loupy, A.; Haas, M.; Roufosse, C.; Naesens, M.; Adam, B.; Afrouzian, M.; Akalin, E.; Alachkar, N.; Bagnasco, S.; Becker, J.U.; et al. The Banff 2019 Kidney Meeting Report (I): Updates on and clarification of criteria for T cell- and antibody-mediated rejection. Am. J. Transpl. 2020, 20, 2318–2331. [Google Scholar] [CrossRef]
- Naesens, M.; Friedewald, J.; Mas, V.; Kaplan, B.; Abecassis, M.M. A Practical Guide to the Clinical Implementation of Biomarkers for Subclinical Rejection Following Kidney Transplantation. Transplantation 2020, 104, 700–707. [Google Scholar] [CrossRef]
- Edwards, R.L.; Menteer, J.; Lestz, R.M.; Baxter-Lowe, L.A. Cell-free DNA as a solid-organ transplant biomarker: Technologies and approaches. Biomark. Med. 2022, 16, 401–415. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Vaitla, P.; Craici, I.M.; Leeaphorn, N.; Hansrivijit, P.; Salim, S.A.; Bathini, T.; Rivera, F.H.C.; Cheungpasitporn, W. The Use of Donor-Derived Cell-Free DNA for Assessment of Allograft Rejection and Injury Status. J. Clin. Med. 2020, 9, 1480. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, E.; Auinger, L.; Speicher, M.R. Cell-Free DNA and Apoptosis: How Dead Cells Inform About the Living. Trends Mol. Med. 2020, 26, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Sigdel, T.K.; Archila, F.A.; Constantin, T.; Prins, S.A.; Liberto, J.; Damm, I.; Towfighi, P.; Navarro, S.; Kirkizlar, E.; Demko, Z.P.; et al. Optimizing Detection of Kidney Transplant Injury by Assessment of Donor-Derived Cell-Free DNA via Massively Multiplex PCR. J. Clin. Med. 2018, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Zhou, Y.; Chen, Y.; Li, X.; Lei, W.; Ge, J.; Peng, W.; Wu, J.; Liu, G.; Yang, G.; et al. Dynamics of early post-operative plasma ddcfDNA levels in kidney transplantation: A single-center pilot study. Transpl. Int. 2019, 32, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Oellerich, M.; Shipkova, M.; Asendorf, T.; Walson, P.D.; Schauerte, V.; Mettenmeyer, N.; Kabakchiev, M.; Hasche, G.; Gröne, H.J.; Friede, T.; et al. Absolute quantification of donor-derived cell-free DNA as a marker of rejection and graft injury in kidney transplantation: Results from a prospective observational study. Am. J. Transpl. 2019, 19, 3087–3099. [Google Scholar] [CrossRef] [PubMed]
- Khush, K.K.; De Vlaminck, I.; Luikart, H.; Ross, D.J.; Nicolls, M.R. Donor-derived, cell-free DNA levels by next-generation targeted sequencing are elevated in allograft rejection after lung transplantation. ERJ Open Res. 2021, 7, 00462–2020. [Google Scholar] [CrossRef]
- Khush, K.K.; Patel, J.; Pinney, S.; Kao, A.; Alharethi, R.; DePasquale, E.; Ewald, G.; Berman, P.; Kanwar, M.; Hiller, D.; et al. Noninvasive detection of graft injury after heart transplant using donor-derived cell-free DNA: A prospective multicenter study. Am. J. Transpl. 2019, 19, 2889–2899. [Google Scholar] [CrossRef]
- Huang, E.; Sethi, S.; Peng, A.; Najjar, R.; Mirocha, J.; Haas, M.; Vo, A.; Jordan, S.C. Early clinical experience using donor-derived cell-free DNA to detect rejection in kidney transplant recipients. Am. J. Transpl. 2019, 19, 1663–1670. [Google Scholar] [CrossRef]
- Zhang, H.; Zheng, C.; Li, X.; Fu, Q.; Li, J.; Su, Q.; Zeng, L.; Liu, Z.; Wang, J.; Huang, H.; et al. Diagnostic Performance of Donor-Derived Plasma Cell-Free DNA Fraction for Antibody-Mediated Rejection in Post Renal Transplant Recipients: A Prospective Observational Study. Front. Immunol. 2020, 11, 342. [Google Scholar] [CrossRef]
- Gielis, E.M.; Ledeganck, K.J.; Dendooven, A.; Meysman, P.; Beirnaert, C.; Laukens, K.; De Schrijver, J.; Van Laecke, S.; Van Biesen, W.; Emonds, M.P.; et al. The use of plasma donor-derived, cell-free DNA to monitor acute rejection after kidney transplantation. Nephrol. Dial. Transpl. 2020, 35, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Osmanodja, B.; Akifova, A.; Budde, K.; Choi, M.; Oellerich, M.; Schütz, E.; Beck, J. Absolute or Relative Quantification of Donor-derived Cell-free DNA in Kidney Transplant Recipients: Case Series. Transpl. Direct 2021, 7, e778. [Google Scholar] [CrossRef] [PubMed]
- Whitlam, J.B.; Ling, L.; Skene, A.; Kanellis, J.; Ierino, F.L.; Slater, H.R.; Bruno, D.L.; Power, D.A. Diagnostic application of kidney allograft-derived absolute cell-free DNA levels during transplant dysfunction. Am. J. Transplant. 2019, 19, 1037–1049. [Google Scholar] [CrossRef] [PubMed]
- Wijtvliet, V.; Plaeke, P.; Abrams, S.; Hens, N.; Gielis, E.M.; Hellemans, R.; Massart, A.; Hesselink, D.A.; De Winter, B.Y.; Abramowicz, D.; et al. Donor-derived cell-free DNA as a biomarker for rejection after kidney transplantation: A systematic review and meta-analysis. Transpl. Int. 2020, 33, 1626–1642. [Google Scholar] [CrossRef]
- Agbor-Enoh, S.; Tunc, I.; De Vlaminck, I.; Fideli, U.; Davis, A.; Cuttin, K.; Bhatti, K.; Marishta, A.; Solomon, M.A.; Jackson, A.; et al. Applying rigor and reproducibility standards to assay donor-derived cell-free DNA as a non-invasive method for detection of acute rejection and graft injury after heart transplantation. J. Heart Lung Transpl. 2017, 36, 1004–1012. [Google Scholar] [CrossRef]
- Agbor-Enoh, S. 2018 ATS BEAR Cage Winning Proposal: Cell-Free DNA to Improve Lung Transplant Outcomes. Am. J. Respir. Crit. Care Med. 2019, 199, 1058–1060. [Google Scholar] [CrossRef]
- Shen, J.; Guo, L.; Yan, P.; Zhou, J.; Zhou, Q.; Lei, W.; Liu, H.; Liu, G.; Lv, J.; Liu, F.; et al. Prognostic value of the donor-derived cell-free DNA assay in acute renal rejection therapy: A prospective cohort study. Clin. Transpl. 2020, 34, e14053. [Google Scholar] [CrossRef]
- Oellerich, M.; Budde, K.; Osmanodja, B.; Bornemann-Kolatzki, K.; Beck, J.; Schütz, E.; Walson, P.D. Donor-Derived Cell-free DNA for Personalized Immunosuppression in Renal Transplantation. Ther. Drug Monit. 2023, 45, 20–25. [Google Scholar] [CrossRef]
- Goussous, N.; Xie, W.; Dawany, N.; Scalea, J.R.; Bartosic, A.; Haririan, A.; Kalil, R.; Drachenberg, C.; Costa, N.; Weir, M.R.; et al. Donor-derived Cell-free DNA in Infections in Kidney Transplant Recipients: Case Series. Transpl. Direct 2020, 6, e568. [Google Scholar] [CrossRef]
- Berger, P.M.; Diamond, J.R. Ureteral obstruction as a complication of renal transplantation: A review. J. Nephrol. 1998, 11, 20–23. [Google Scholar]
- Larkins, N.G.; Wong, G.; Taverniti, A.; Lim, W.H. Epitope matching in kidney transplantation: Recent advances and current limitations. Curr. Opin. Organ. Transpl. 2019, 24, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Leeaphorn, N.; Pena, J.R.A.; Thamcharoen, N.; Khankin, E.V.; Pavlakis, M.; Cardarelli, F. HLA-DQ Mismatching and Kidney Transplant Outcomes. Clin. J. Am. Soc. Nephrol. 2018, 13, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Senev, A.; Coemans, M.; Lerut, E.; Van Sandt, V.; Kerkhofs, J.; Daniëls, L.; Driessche, M.V.; Compernolle, V.; Sprangers, B.; Van Loon, E.; et al. Eplet Mismatch Load and De Novo Occurrence of Donor-Specific Anti-HLA Antibodies, Rejection, and Graft Failure after Kidney Transplantation: An Observational Cohort Study. J. Am. Soc. Nephrol. 2020, 31, 2193–2204. [Google Scholar] [CrossRef] [PubMed]
- Kishikawa, H.; Kinoshita, T.; Hashimoto, M.; Fukae, S.; Taniguchi, A.; Yamanaka, K.; Nakagawa, M.; Nishimura, K. Class II HLA Eplet Mismatch Is a Risk Factor for De Novo Donor-Specific Antibody Development and Antibody-mediated Rejection in Kidney Transplantation Recipients. Transpl. Proc. 2018, 50, 2388–2391. [Google Scholar] [CrossRef] [PubMed]
- Tafulo, S.; Malheiro, J.; Santos, S.; Dias, L.; Almeida, M.; Martins, S.; Pedroso, S.; Mendes, C.; Lobato, L.; Castro-Henriques, A. Degree of HLA class II eplet mismatch load improves prediction of antibody-mediated rejection in living donor kidney transplantation. Hum. Immunol. 2019, 80, 966–975. [Google Scholar] [CrossRef]
- San Segundo, D.; Guiral-Foz, S.A.; Benito-Hernández, A.; Fernández, A.R.; Arnau, A.; Valero, R.; Ramos-Barrón, M.A.; García-Unzueta, M.T.; Gómez-Ortega, J.M.; López-Hoyos, M.; et al. Urinary CXCL10 specifically relates to HLA-DQ eplet mismatch load in kidney transplant recipients. Transpl. Immunol. 2022, 70, 101494. [Google Scholar] [CrossRef]
- Montgomery, R.A.; Tatapudi, V.S.; Leffell, M.S.; Zachary, A.A. HLA in transplantation. Nat. Rev. Nephrol. 2018, 14, 558–570. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Total (n = 42) | dd-cfDNA ≥ 1.0% (n = 11) | dd-cfDNA < 1.0% (n = 31) | p |
|---|---|---|---|---|
| Recipient age (years) | 59.0 [47.8–67.5] | 60.0 [48.0–73.0] | 59.0 [47.0–66.0] | 0.572 |
| Recipient gender (male) | 76.2% | 63.6% | 80.6% | 0.255 |
| Diabetic nephropathy | 23.8% | 18.2% | 25.8% | 0.610 |
| Time in renal replacement therapy (months) | 13.5 [3.9–38.7] | 24.5 [10.5–108.7] | 10.7 [0.0–32.6] | 0.062 |
| Retransplant | 19.0% | 36.4% | 12.9% | 0.089 |
| Preemptive transplantation | 21.4% | 18.2% | 22.6% | 0.760 |
| Donor age (years) | 58.5 [47.0–65.0] | 61.0 [47.0–65.0] | 58.0 [47.0–65.0] | 0.910 |
| Cold ischemia time (hours) | 21.5 [17.8–24.0] | 20.0 [18.0–24.0] | 22.0 [17.0–24.0] | 0.822 |
| Induction | 66.7% | 72.7% | 64.5% | 0.620 |
| 1-month acute rejection | 16.7% | 36.4% | 9.7% | 0.041 |
| 1-month AbMR | 11.9% | 36.4% | 3.2% | 0.004 |
| 1-month troubled graft | 33.3% | 63.6% | 22.6% | 0.013 |
| First year acute rejection (RAPreM12) | 21.4% | 36.4% | 16.1% | 0.160 |
| First month eGFR (mL/min/1.73 m2) | 49.5 [40.5–70.0] | 43.0 [28.0–54.0] | 51.0 [42.0–72.0] | 0.138 |
| First month albuminuria (mg/g) | 55.0 [23.5–150.5] | 57.5 [34.5–485.8] | 53.0 [22.5–135.5] | 0.524 |
| 1-year eGFR (mL/min/1.73 m2) | 50.0 [38.0–68.0] | 45.0 [38.0–49.0] | 50.0 [38.0–71.8] | 0.514 |
| dd-cfDNA (%) | 0.61 [0.34–1.06] | - | - | 0.396 |
| Data of immunosuppressive therapy | ||||
| TTR 8–12 at month 1 (%) | 45.7 [29.3–61.3] | 50.9 [37.0–60.4] | 45.5 [25.0–61.4] | 0.396 |
| TTR > 12 at month 1 (%) | 47.3 [34.0–65.2] | 49.1 [39.6–63.0] | 44.8 [33.6–75.0] | 1.000 |
| Mean tacrolimus trough level throughout month 1 (ng/mL) | 12.5 [11.3–14.3] | 12.5 [11.4–14.3] | 12.3 [11.2–14.2] | 0.822 |
| Tacrolimus trough level at month 1 (ng/mL) | 12.1 [10.0–14.0] | 13.0 [10.0–15.0] | 12.0 [9.0–14.0] | 0.233 |
| Mycophenolic acid trough level at month 1 (ng/mL) | 2.0 [1.0–3.0] | 2.0 [1.8–4.0] | 2.0 [1.0–3.0] | 0.569 |
| Any tacrolimus level < 5 at month 1 | 7.1% | 0.0% | 9.7% | 0.284 |
| Any tacrolimus level < 6 at month 1 | 11.9% | 0.0% | 16.1% | 0.156 |
| Coefficient of variability at month 1 (%) | 28.1 [19.4–34.2] | 21.8 [16.1–61.5] | 28.6 [19.8–37.2] | 0.257 |
| Tacrolimus trough level/dose at month 1 | 1.7 [1.3–2.5] | 1.8 [1.3–2.5] | 1.7 [1.1–2.7] | 0.778 |
| Fast tacrolimus metabolizers | 11.9% | 9.1% | 12.9% | 0.737 |
| Variable | Total (n = 42) | dd-cfDNA ≥ 1.0% (n = 11) | dd-cfDNA < 1.0% (n = 31) | p |
|---|---|---|---|---|
| Antigen HLA class I and II mismatches | 7.5 [6.0–9.0] | 8.0 [7.0–9.0] | 7.0 [5.0–9.0] | 0.233 |
| All HLA class I eplet mismatch load | 18.0 [13.0–22.0] | 20.0 [16.0–22.0] | 16.0 [13.0–22.0] | 0.553 |
| All HLA class II eplet mismatch load | 23.5 [14.8–51.5] | 46.0 [22.0–69.0] | 21.0 [11.0–39.0] | 0.022 |
| HLA-DRB1 eplet mismatch load | 9.0 [4.0–14.0] | 10.0 [7.0–14.0] | 9.0 [3.0–13.0] | 0.245 |
| HLA-DQB1 eplet mismatch load | 7.0 [2.8–9.3] | 9.0 [7.0–11.0] | 7.0 [2.0–9.0] | 0.041 |
| HLA-DQA1 eplet mismatch load | 1.0 [0.0–5.0] | 3.0 [0.0–5.0] | 1.0 [0.0–4.0] | 0.445 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-López, E.; Ocejo-Vinyals, J.G.; Renuncio-García, M.; Roa-Bautista, A.; San Segundo Arribas, D.; Escagedo, C.; García-Saiz, M.d.M.; Valero, R.; García-Berbel, P.; Ruíz San Millán, J.C.; et al. Donor-Derived Cell-Free DNA at 1 Month after Kidney Transplantation Relates to HLA Class II Eplet Mismatch Load. Biomedicines 2023, 11, 2741. https://doi.org/10.3390/biomedicines11102741
González-López E, Ocejo-Vinyals JG, Renuncio-García M, Roa-Bautista A, San Segundo Arribas D, Escagedo C, García-Saiz MdM, Valero R, García-Berbel P, Ruíz San Millán JC, et al. Donor-Derived Cell-Free DNA at 1 Month after Kidney Transplantation Relates to HLA Class II Eplet Mismatch Load. Biomedicines. 2023; 11(10):2741. https://doi.org/10.3390/biomedicines11102741
Chicago/Turabian StyleGonzález-López, Elena, Javier Gonzalo Ocejo-Vinyals, Mónica Renuncio-García, Adriel Roa-Bautista, David San Segundo Arribas, Clara Escagedo, María del Mar García-Saiz, Rosalía Valero, Pilar García-Berbel, Juan Carlos Ruíz San Millán, and et al. 2023. "Donor-Derived Cell-Free DNA at 1 Month after Kidney Transplantation Relates to HLA Class II Eplet Mismatch Load" Biomedicines 11, no. 10: 2741. https://doi.org/10.3390/biomedicines11102741
APA StyleGonzález-López, E., Ocejo-Vinyals, J. G., Renuncio-García, M., Roa-Bautista, A., San Segundo Arribas, D., Escagedo, C., García-Saiz, M. d. M., Valero, R., García-Berbel, P., Ruíz San Millán, J. C., & Rodrigo, E. (2023). Donor-Derived Cell-Free DNA at 1 Month after Kidney Transplantation Relates to HLA Class II Eplet Mismatch Load. Biomedicines, 11(10), 2741. https://doi.org/10.3390/biomedicines11102741