

Application of Inflatable Video-Assisted Mediastinoscopic Transhiatal Esophagectomy in Individualized Treatment of Esophageal Cancer


Abstract
:1. Introduction
2. Indications for IVMTE of Esophageal Cancer
3. Contraindications for IVMTE of Esophageal Cancer
4. Surgical Methods
4.1. Conventional IVMTE Mode
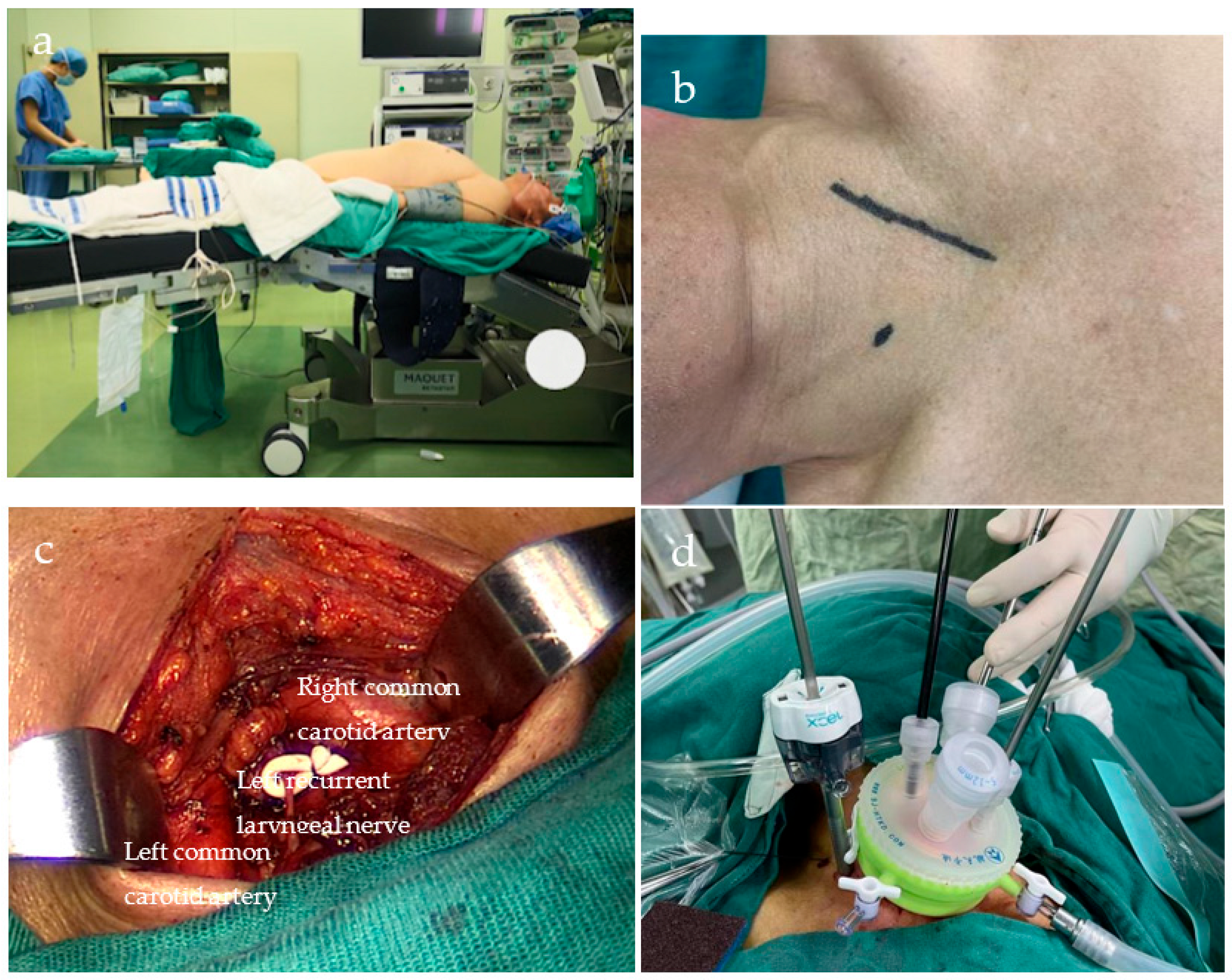
4.1.1. Cervical Procedures
4.1.2. Transcervical Mediastinal Procedures
4.1.3. Abdominal Procedures
4.1.4. Transabdominal Mediastinal Procedures
4.2. Modified IVMTE Mode
4.2.1. Cervical Procedures
4.2.2. Mediastinal Procedures
4.3. West China Hospital IVMTE Model
5. Perioperative Outcomes
5.1. Operation Time
5.2. Pulmonary Complications
5.3. RLN Injury
5.4. Number of Dissected Lymph Nodes
5.5. Hemorrhage
5.6. Thoracic Duct Injury
5.7. Anastomotic Leakage
5.8. Inflammatory Responses
5.9. Definition of Complications
6. Long-Term Outcomes
7. Potential Advantages and Challenges of IVMTE
7.1. Advantages of IVMTE
- One-lung ventilation is not required, and its advantages are more evident in some patients with cardiopulmonary insufficiency.
- No damage to the intercostal nerves, good patient comfort, and fast postoperative recovery.
- There is no need to change the body position, and mediastinal and abdominal surgeries can be performed simultaneously, which shortens the operation and anesthesia time.
- The azygos vein and bronchial artery are preserved during surgery, thus preventing liver injury in patients with hepatic insufficiency and reducing the probability of postoperative coughing.
- It is suitable for patients with chest wall lesions who present difficulty for the surgical device when entering the chest through the intercostal space.
7.2. Challenges faced by IVMTE
7.3. Disadvantages of IVMTE
- The narrow operating space poses a risk of damage to the surrounding tissues and limits the ability to handle unforeseen circumstances during surgery.
- There remains a gap between lymph node dissection and VATE.
- Compared to VATE, the risk of RLN injury is higher.
- The absence of a chest drainage tube increases the likelihood of postoperative pleural effusion, which may necessitate a thoracentesis.
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Lu, S.W.; Pai, C.P.; Yang, T.H.; Lu, J.X.; Hsiao, C.H.; Yen, C.C. Clinical characteristics and risk factors for 30-day mortality in esophageal cancer patients with upper gastrointestinal bleeding: A multicenter study. Front. Oncol. 2023, 13, 11847100. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Ho, C.M.; Wu, M.S.; Hsu, W.H.; Wang, W.Y.; Yuan, S.F.; Hsieh, H.M.; Wu, I.C. Effect of esophageal cancer screening on mortality among patients with oral cancer and second primary esophageal cancer in Taiwan. Am. J. Otolaryngol. 2023, 44, 103856. [Google Scholar] [CrossRef]
- Ma, L.; Li, X.; Wang, M.; Zhang, Y.; Wu, J.; He, Y.; Fan, X.; Zhang, B.; Zhou, X. The Incidence, Mortality, and DALYs Trends Associated with Esophageal Cancer-China, 1990–2019. China CDC Wkly 2022, 4, 956–961. [Google Scholar] [CrossRef]
- Li, F.; Li, H.; Su, X.; Liang, H.; Wei, L.; Shi, D.; Zhang, J.; Wang, Z. Trends in incidence and mortality of esophageal cancer in China 1990–2019: A joinpoint and age-period-cohort analysis. Front. Oncol. 2022, 12, 887011. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Chen, P.; Wu, J.; Wen, Z.; Zhao, C. The association between statin use and prognosis in esophageal cancer patients: A meta-analysis. Medicine 2023, 102, e33359. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Wu, B.; Li, H.; Xiong, J. Influence of adverse effects of neoadjuvant chemoradiotherapy on the prognosis of patients with early-stage esophageal cancer (cT1b-cT2N0M0) based on the SEER database. Front. Surg. 2023, 10, 1131385. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.; Yang, Q.; Yin, H.; Wei, N.; Wang, W.; Yu, B. Comprehensive analysis of ZNF family genes in prognosis, immunity, and treatment of esophageal cancer. BMC Cancer 2023, 23, 301. [Google Scholar] [CrossRef]
- Huang, Z.N.; Liu, C.Q.; Guo, M.F.; Xu, M.Q.; Sun, X.H.; Wang, G.X.; Xie, M.R. Clinical analysis of inflatable video-assisted mediastinoscopic transhiatal esophagectomy combined with laparoscopy. Zhonghua Wai Ke Za Zhi Chin. J. Surg. 2023, 61, 48–53. [Google Scholar]
- Rochefort, M. A minimally invasive esophagectomy; by any means necessary. J. Surg. Oncol. 2023, 127, 1089–1091. [Google Scholar] [CrossRef]
- Dabsha, A.; Elkharbotly, I.; Yaghmour, M.; Badr, A.; Badie, F.; Khairallah, S.; Esmail, Y.M.; Shmushkevich, S.; Hossny, M.; Rizk, A.; et al. ASO Visual Abstract: Novel Mediastinoscope-Assisted Minimally Invasive Esophagectomy for Esophageal Cancer: A Systematic Review and Meta-analysis. Ann. Surg. Oncol. 2023, 30, 4042–4043. [Google Scholar] [CrossRef]
- Vincke, A.; Miftode, S.; Alfarawan, F.; Bockhorn, M.; El-Sourani, N. Hybrid Minimally Invasive Esophagectomy vs. Open Esophagectomy: A Retrospective Propensity Score Matched Comparison. Medicina 2023, 59, 434. [Google Scholar] [CrossRef] [PubMed]
- Lewis, I. The surgical treatment of carcinoma of the oesophagus; with special reference to a new operation for growths of the middle third. Br. J. Surg. 1946, 34, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Buess, G.; Becker, H.D. Minimally invasive surgery in tumors of the esophagus. Langenbecks Arch. Fur Chirurgie. Suppl. II Verh. Der Dtsch. Ges. Fur Chirurgie. Dtsch. Ges. Fur Chirurgie. Kongr. 1990, 1990, 1355–1360. [Google Scholar]
- Daiko, H.; Fujita, T.; Ohgara, T.; Yamazaki, N.; Fujii, S.; Ohno, Y.; Yano, T. Minimally invasive hybrid surgery combined with endoscopic and thoracoscopic approaches for submucosal tumor originating from thoracic esophagus. World J. Surg. Oncol. 2015, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, H.; Shiozaki, A.; Konishi, H.; Kosuga, T.; Komatsu, S.; Ichikawa, D.; Okamoto, K.; Otsuji, E. Single-Port Mediastinoscopic Lymphadenectomy Along the Left Recurrent Laryngeal Nerve. Ann. Thorac. Surg. 2015, 100, 1115–1117. [Google Scholar] [CrossRef] [PubMed]
- Gong, S.; Rao, X.; Yuan, Y.; Yao, X.; Li, G.; Wang, N.; Li, D.; Jiang, L. Clinical-pathological features and perioperative outcomes of mediastinoscopy vs. thoracoscopy esophagectomy in esophageal cancer: A meta-analysis. Front. Surg. 2023, 10, 1039615. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Guo, X.; Zhao, H.; Yu, X.; Wang, C.; Du, L.; Wang, F.; Mu, J. Mediastinoscopy-assisted transhiatal esophagectomy versus thoraco-laparoscopic esophagectomy for esophageal cancer: A single-center initial experience. J. Thorac. Dis. 2020, 12, 4908–4914. [Google Scholar] [CrossRef]
- Lemmens, J.; Klarenbeek, B.; Verstegen, M.; van Workum, F.; Hannink, G.; Ubels, S.; Rosman, C. Performance of a consensus-based algorithm for diagnosing anastomotic leak after minimally invasive esophagectomy for esophageal cancer. Dis. Esophagus 2023, 36, doad016. [Google Scholar] [CrossRef]
- Yu, W.Q.; Zhai, L.X.; Shi, G.D.; Tang, J.Y.; Gao, H.J.; Wei, Y.C. Short-term outcome of totally minimally invasive versus hybrid minimally invasive Ivor-Lewis esophagectomy. Asian J. Surg. 2023, 46, 3727–3733. [Google Scholar] [CrossRef]
- Daiko, H.; Oguma, J.; Fujiwara, H.; Ishiyama, K.; Kurita, D.; Sato, T.; Sato, K.; Faiz, Z.; Fujita, T. Novel universally applicable technique for performing bilateral transcervical mediastinoscopic-assisted transhiatal laparoscopic esophagectomy: A truly minimally invasive procedure. Surg. Endosc. 2021, 35, 5186–5192. [Google Scholar] [CrossRef]
- Fan, X.; Wang, J.; Xia, L.; Qiu, H.; Tian, Y.; Zhangcai, Y.; Luo, X.; Gao, Y.; Li, C.; Wu, Y.; et al. Efficacy of endoscopic therapy for T1b esophageal cancer and construction of prognosis prediction model: A retrospective cohort study. Int. J. Surg. 2023, 109, 1708–1719. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Kozuki, R. Esophagectomy and Perioperative Management in Elderly Patients with Esophageal Cancer. Kyobu geka. Jpn. J. Thorac. Surg. 2020, 73, 870–875. [Google Scholar]
- Koide, N.; Takeuchi, D.; Suzuki, A.; Miyagawa, S. Mediastinoscopy-assisted esophagectomy for esophageal cancer in patients with serious comorbidities. Surg. Today 2012, 42, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Nomura, T.; Matsutani, T.; Hagiwara, N.; Fujita, I.; Nakamura, Y.; Makino, H.; Miyashita, M.; Uchida, E. Mediastinoscopy-assisted Transhiatal Esophagectomy for Esophageal Cancer: A Single-Institutional Cohort Study. Surg. Laparosc. Endosc. Percutan. Tech. 2016, 26, e153–e156. [Google Scholar] [CrossRef]
- Koide, N.; Hiraguri, M.; Nishio, A.; Igarashi, J.; Watanabe, H.; Adachi, W.; Amano, J. Three elderly patients with lower esophageal cancer successfully treated by transhiatal esophagectomy assisted by mediastinoscopy. Surg. Laparosc. Endosc. Percutan. Tech. 2000, 10, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Mimatsu, K.; Oida, T.; Kawasaki, A.; Aramaki, O.; Kuboi, Y.; Kanou, H.; Amano, S. Mediastinoscopy-assisted esophagectomy is useful technique for poor surgical-risk patients with thoracic esophageal cancer. Surg. Laparosc. Endosc. Percutaneous Tech. 2009, 19, e17–e20. [Google Scholar] [CrossRef]
- Jin, Y.; Lu, X.; Xue, L.; Zhao, X. Retrospective Comparison of Two Minimally Invasive Esophagectomy in the Treatment of Esophageal Cancer: Pneumatic Mediastinoscopy Versus Thoracoscopy. J. Laparoendosc. Adv. Surg. Tech. Part A 2019, 29, 638–642. [Google Scholar] [CrossRef]
- Li, G.S. Prof. Qingdong Cao: Single-port inflatable mediastinoscopy combined with laparoscopy for the radical treatment of esophageal cancer. J. Thorac. Dis. 2016, 8, E1108–E1109. [Google Scholar] [CrossRef]
- Akovbiantz, A.; Aeberhard, P.; Linder, E. Mediastinoscopy in the Evaluation of Operability of Esophageal Cancer. Schweiz Med. Wochenschr. 1965, 95, 168–170. [Google Scholar]
- Hu, W.; Yuan, P.; Yuan, Y.; Chen, L.; Hu, Y. Learning curve for inflatable mediastinoscopic and laparoscopic-assisted esophagectomy. Surg. Endosc. 2023, 37, 4486–4494. [Google Scholar] [CrossRef]
- Ma, J.; Wang, W.; Zhang, B.; Li, X.; Wu, J.; Wu, Z. Minimally invasive esophagectomy via Sweet approach in combination with cervical mediastinoscopy is a valuable approach for surgical treatment of esophageal cancer. Zhong Nan Da Xue Xue Bao Yi Xue Ban J. Cent. South Univ. Med. Sci. 2021, 46, 60–68. [Google Scholar]
- Sasaki, K.; Tsuruda, Y.; Shimonosono, M.; Noda, M.; Uchikado, Y.; Arigami, T.; Matsushita, D.; Kita, Y.; Mori, S.; Kurahara, H.; et al. A comparison of the surgical invasiveness and short-term outcomes between thoracoscopic and pneumatic mediastinoscopic esophagectomy for esophageal cancer. Surg. Today 2022, 52, 1759–1765. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Huang, K.; Wei, R.; Liu, C.; Fang, Y.; Wu, B.; Xu, Z.; Ding, X.; Tang, H. Transcervical inflatable mediastinoscopic esophagectomy versus thoracoscopic esophagectomy for local early- and intermediate-stage esophageal squamous cell carcinoma: A propensity score-matched analysis. J. Surg. Oncol. 2022, 125, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Tandon, S.; Batchelor, A.; Bullock, R.; Gascoigne, A.; Griffin, M.; Hayes, N.; Hing, J.; Shaw, I.; Warnell, I.; Baudouin, S.V. Peri-operative risk factors for acute lung injury after elective oesophagectomy. Br. J. Anaesth. 2001, 86, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Hamada, J.; Konishi, H.; Shiozaki, A.; Fujiwara, H.; Shoda, K.; Kosuga, T.; Kubota, T.; Okamoto, K.; Arita, T.; Morimura, R.; et al. Management of Pleural Effusion After Mediastinoscopic Radical Esophagectomy. Anticancer. Res. 2018, 38, 6919–6925. [Google Scholar] [CrossRef] [PubMed]
- Hisakura, K.; Ogawa, K.; Akashi, Y.; Kim, J.; Moue, S.; Ohara, Y.; Owada, Y.; Hashimoto, S.; Enomoto, T.; Oda, T. Transhiatal chest drainage in mediastinoscope and laparoscope-assisted esophagectomy for esophageal cancer: A retrospective study. J. Cardiothorac. Surg. 2022, 17, 200. [Google Scholar] [CrossRef]
- Wang, X.; Li, X.; Cheng, H.; Zhang, B.; Zhong, H.; Wang, R.; Zhong, B.; Cao, Q. Single-Port Inflatable Mediastinoscopy Combined With Laparoscopic-Assisted Small Incision Surgery for Radical Esophagectomy Is an Effective and Safe Treatment for Esophageal Cancer. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2019, 23, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, H.; Yokota, K.; Utsunomiya, M.; Namikawa, T.; Kobayashi, M.; Hanazaki, K. A descriptive comparison of postoperative outcomes between hybrid mediastino-thoracoscopic approach and conventional thoracoscopic esophagectomy for esophageal cancer. Surg. Endosc. 2023, 37, 2949–2957. [Google Scholar] [CrossRef]
- Yoshino, S.; Takeda, S.; Nishimura, T.; Tokunou, K.; Oka, M. A case of esophageal cancer with recurrent lymph-node metastasis successfully treated with chemo-radiotherapy after mediastinoscopy-assisted transhiatal esophagectomy. Gan Kagaku Ryoho Cancer Chemother. 2008, 35, 2039–2041. [Google Scholar]
- Li, Z.; Gai, C.; Zhang, Y.; Wen, S.; Lv, H.; Xu, Y.; Huang, C.; Zhao, B.; Tian, Z. Comparisons of minimally invasive esophagectomy and open esophagectomy in lymph node metastasis/dissection for thoracic esophageal cancer. Chin. Med. J. 2022, 135, 2446–2452. [Google Scholar] [CrossRef]
- Xu, B.; Chen, H.; Zhang, Q.; Chen, P.; Liu, Q.; Chen, M. Value of subcarinal lymph node dissection in esophageal cancer surgery: A case-control study. Medicine 2022, 101, e31593. [Google Scholar] [CrossRef] [PubMed]
- Furuke, H.; Konishi, H.; Fujiwara, H.; Shiozaki, A.; Ohashi, T.; Shimizu, H.; Arita, T.; Yamamoto, Y.; Morimura, R.; Kuriu, Y.; et al. Predictors of the difficulty of transcervical subcarinal lymph node dissection for esophageal cancer. Esophagus Off. J. Jpn. Esophageal Soc. 2023, 20, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Kanemura, T.; Miyata, H.; Takeoka, T.; Sugase, T.; Sugimura, K.; Yamashita, K.; Tanaka, K.; Makino, T.; Ota, M.; Yagi, K.; et al. Significance of dissection in each regional lymph-node station of esophageal cancer based on efficacy index and recurrence patterns after curative esophagectomy. Esophagus Off. J. Jpn. Esophageal Soc. 2023, 20, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Vagliasindi, A.; Franco, F.D.; Degiuli, M.; Papis, D.; Migliore, M. Extension of lymph node dissection in the surgical treatment of esophageal and gastroesophageal junction cancer: Seven questions and answers. Future Oncol. 2023, 19, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.L.; Chen, C.M.; Hung, W.H.; Cheng, Y.F.; Hong, R.P.; Wang, B.Y.; Cheng, C.Y. Clinical Outcome of Intraoperative Recurrent Laryngeal Nerve Monitoring during Thoracoscopic Esophagectomy and Mediastinal Lymph Node Dissection for Esophageal Cancer. J. Clin. Med. 2022, 11, 4949. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Liu, Z.; Gao, C. Relationship Between CD8+ T Cells and Prognosis of Esophageal Cancer Patients: A Systematic Review and Meta-analysis. Mol. Biotechnol. 2023, 1–13. [Google Scholar] [CrossRef]
- Shang, Q.X.; Wang, Y.C.; Yang, Y.S.; Hu, W.P.; Chen, L.Q. Pattern of subcarinal lymph node metastasis and dissection strategy for thoracic esophageal cancer. J. Thorac. Dis. 2020, 12, 5667–5677. [Google Scholar] [CrossRef] [PubMed]
- Hosogi, H.; Yagi, D.; Sakaguchi, M.; Akagawa, S.; Tokoro, Y.; Kanaya, S. Upper mediastinal lymph node dissection based on mesenteric excision in esophageal cancer surgery: Confirmation by near-infrared image-guided lymphatic mapping and the impact on locoregional control. Esophagus Off. J. Jpn. Esophageal Soc. 2021, 18, 219–227. [Google Scholar] [CrossRef]
- Shi, K.; Qian, R.; Zhang, X.; Jin, Z.; Lin, T.; Lang, B.; Wang, G.; Cui, D.; Zhang, B.; Hua, X. Video-assisted mediastinoscopic and laparoscopic transhiatal esophagectomy for esophageal cancer. Surg. Endosc. 2022, 36, 4207–4214. [Google Scholar] [CrossRef]
- Feng, M.X.; Wang, H.; Zhang, Y.; Tan, L.J.; Xu, Z.L.; Qun, W. Minimally invasive esophagectomy for esophageal squamous cell carcinoma: A case-control study of thoracoscope versus mediastinoscope assistance. Surg. Endosc. 2012, 26, 1573–1578. [Google Scholar] [CrossRef]
- Wang, Q.Y.; Li, J.P.; Zhang, L.; Jiang, N.Q.; Wang, Z.L.; Zhang, X.Y. Mediastinoscopic esophagectomy for patients with early esophageal cancer. J. Thorac. Dis. 2015, 7, 1235–1240. [Google Scholar]
- Fujiwara, H.; Shiozaki, A.; Konishi, H.; Kosuga, T.; Komatsu, S.; Ichikawa, D.; Okamoto, K.; Otsuji, E. Perioperative outcomes of single-port mediastinoscope-assisted transhiatal esophagectomy for thoracic esophageal cancer. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2017, 30, 1–8. [Google Scholar] [CrossRef]
- Wang, G.; Sun, X.; Li, T.; Xu, M.; Guo, M.; Liu, C.; Xie, M. Study of the short-term quality of life of patients with esophageal cancer after inflatable videoassisted mediastinoscopic transhiatal esophagectomy. Front. Surg. 2022, 9, 981576. [Google Scholar] [CrossRef]
- Zhang, W.; Cui, D.; Shi, K.; Chen, M.; Zhang, B.; Qian, R. Feasibility and safety of expandable mediastinoscopic and laparoscopic radical esophagectomy. Front. Oncol. 2023, 13, 1110962. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| IVMTE | VATE | |
|---|---|---|
| Indications | Advanced age | Any age |
| Severe pleural adhesion | Except severe pleural adhesion | |
| Emphysema with FEV1 < 70% and vital capacity < 80% | Sufficient lung function to tolerate one-lung ventilation | |
| Histopathology confirms esophageal cancer that can be treated with R0 resection | ||
| Contraindications | No definite pathological diagnosis | |
| Severe organ dysfunction | ||
| Presence of distant metastasis | ||
| Absence of replacement organs for the digestive tract | ||
| Factors that cause tight operating space: severe spinal deformity, tumor stage T4, large primary tumor, significant lymphadenopathy, distant lymph node metastasis, and tissue swelling and adhesion resulting from adjuvant chemotherapy or radiotherapy | Unresectable with invasion of adjacent tissues | |
| Pathology (Cases) | Complication (%) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Authors | Year | Ref | Country | N (Cases) | SCC | Adeno. | Other | Definition of Complication | Pneumonia | Arrhythmia | Leakage | Chylothorax | RLNP |
| 1 | Feng | 2012 | [50] | China | 27 | 27 | 0 | 0 | 25.9 | 18.5 | 0 | 18.5 | ||
| 2 | Wang | 2015 | [51] | China | 194 | 194 | 0 | 0 | 6.2 | 3.6 | 4.6 | 4.6 | ||
| 3 | Fujiwara | 2017 | [52] | Japan | 60 | 58 | 2 | 0 | CD, ECCG | 6.7 | 15 | 0 | 33.3 | |
| 4 | Chen | 2022 | [33] | China | 59 | 59 | 0 | 0 | 8.5 | 13.6 | 1.7 | |||
| 5 | Sasaki | 2022 | [32] | Japan | 34 | 32 | 0 | 2 | CD | 17.7 | 17.7 | 5.9 | 38.2 | |
| 6 | Shi | 2022 | [49] | China | 100 | 100 | 0 | 0 | ECCG | 7 | 6 | 11 | 12 | |
| 7 | Huang | 2023 | [8] | China | 38 | CD | 7.9 | 7.9 | 5.3 | 2.6 | ||||
| 8 | wang | 2023 | [53] | China | 30 | 30 | 0 | 0 | CD | 10 | 6.7 | 6.7 | 0 | 3.3 |
| 9 | Zhang | 2023 | [54] | China | 106 | 106 | 0 | 0 | CD | 3.77 | 14.15 | 2.83 | 1.89 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, S.; Shen, C.; Hu, Y.; He, Y.; Yuan, Y.; Xu, Y. Application of Inflatable Video-Assisted Mediastinoscopic Transhiatal Esophagectomy in Individualized Treatment of Esophageal Cancer. Biomedicines 2023, 11, 2750. https://doi.org/10.3390/biomedicines11102750
Song S, Shen C, Hu Y, He Y, Yuan Y, Xu Y. Application of Inflatable Video-Assisted Mediastinoscopic Transhiatal Esophagectomy in Individualized Treatment of Esophageal Cancer. Biomedicines. 2023; 11(10):2750. https://doi.org/10.3390/biomedicines11102750
Chicago/Turabian StyleSong, Shangqi, Cheng Shen, Yang Hu, Yazhou He, Yong Yuan, and Yuyang Xu. 2023. "Application of Inflatable Video-Assisted Mediastinoscopic Transhiatal Esophagectomy in Individualized Treatment of Esophageal Cancer" Biomedicines 11, no. 10: 2750. https://doi.org/10.3390/biomedicines11102750
APA StyleSong, S., Shen, C., Hu, Y., He, Y., Yuan, Y., & Xu, Y. (2023). Application of Inflatable Video-Assisted Mediastinoscopic Transhiatal Esophagectomy in Individualized Treatment of Esophageal Cancer. Biomedicines, 11(10), 2750. https://doi.org/10.3390/biomedicines11102750