
Adverse Events of Cabozantinib as a Potential Prognostic Factor in Metastatic Renal Cell Carcinoma Patients: Real-World Experience in a Single-Center Retrospective Study

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Collection
2.2. Data Collection
2.3. Adverse Events
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Libertino, J.; Gee, J. Renal Cancer Contemporary Management: Contemporary Management; Springer International Publishing: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Sharma, R.; Kadife, E.; Myers, M.; Kannourakis, G.; Prithviraj, P.; Ahmed, N. Determinants of Resistance to Vegf-Tki and Immune Checkpoint Inhibitors in Metastatic Renal Cell Carcinoma. J. Exp. Clin. Cancer Res. 2021, 40, 186. [Google Scholar] [CrossRef]
- Swiatek, M.; Jancewicz, I.; Kluebsoongnoen, J.; Zub, R.; Maassen, A.; Kubala, S.; Udomkit, A.; Siedlecki, J.A.; Sarnowski, T.J.; Sarnowska, E. Various Forms of Hif-1α Protein Characterize the Clear Cell Renal Cell Carcinoma Cell Lines. IUBMB Life 2020, 72, 1220–1232. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Escudier, B.; Powles, T.; Mainwaring, P.N.; Rini, B.I.; Donskov, F.; Hammers, H.; Hutson, T.E.; Lee, J.L.; Peltola, K.; et al. Cabozantinib Versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1814–1823. [Google Scholar] [CrossRef]
- Ott, P.A.; Hodi, F.S.; Buchbinder, E.I. Inhibition of Immune Checkpoints and Vascular Endothelial Growth Factor as Combination Therapy for Metastatic Melanoma: An Overview of Rationale, Preclinical Evidence, and Initial Clinical Data. Front. Oncol. 2015, 5, 202. [Google Scholar] [CrossRef]
- Voron, T.; Marcheteau, E.; Pernot, S.; Colussi, O.; Tartour, E.; Taieb, J.; Terme, M. Control of the Immune Response by Pro-Angiogenic Factors. Front. Oncol. 2014, 4, 70. [Google Scholar] [CrossRef]
- Apolo, A.B.; Nadal, R.; Tomita, Y.; Davarpanah, N.N.; Cordes, L.M.; Steinberg, S.M.; Cao, L.; Parnes, H.L.; Costello, R.; Merino, M.J.; et al. Cabozantinib in Patients with Platinum-Refractory Metastatic Urothelial Carcinoma: An Open-Label, Single-Centre, Phase 2 Trial. Lancet Oncol. 2020, 21, 1099–1109. [Google Scholar] [CrossRef]
- Kwilas, A.R.; Ardiani, A.; Donahue, R.N.; Aftab, D.T.; Hodge, J.W. Dual Effects of a Targeted Small-Molecule Inhibitor (Cabozantinib) on Immune-Mediated Killing of Tumor Cells and Immune Tumor Microenvironment Permissiveness When Combined with a Cancer Vaccine. J. Transl. Med. 2014, 12, 294. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Zurawski, B.; Oyervides Juárez, V.M.; Hsieh, J.J.; Basso, U.; Shah, A.Y.; et al. Nivolumab Plus Cabozantinib Versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 384, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Warren, M.A.; Golshayan, A.R.; Sahi, C.; Eigl, B.J.; Ruether, J.D.; Cheng, T.; North, S.; et al. Prognostic Factors for Overall Survival in Patients with Metastatic Renal Cell Carcinoma Treated with Vascular Endothelial Growth Factor-Targeted Agents: Results from a Large, Multicenter Study. J. Clin. Oncol. 2009, 27, 5794–5799. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Motzer, R.J.; Escudier, B.; Pal, S.; Kollmannsberger, C.; Pikiel, J.; Gurney, H.; Rha, S.Y.; Park, S.H.; Geertsen, P.F.; et al. Outcomes Based on Prior Therapy in the Phase 3 Meteor Trial of Cabozantinib Versus Everolimus in Advanced Renal Cell Carcinoma. Br. J. Cancer 2018, 119, 663–669. [Google Scholar] [CrossRef] [PubMed]
- McGregor, B.A.; Lalani, A.A.; Xie, W.; Steinharter, J.A.; Bakouny, Z.E.; Martini, D.J.; Fleischer, J.H.; Abou-Alaiwi, S.; Nassar, A.; Nuzzo, P.V.; et al. Activity of Cabozantinib after Immune Checkpoint Blockade in Metastatic Clear-Cell Renal Cell Carcinoma. Eur. J. Cancer 2020, 135, 203–210. [Google Scholar] [CrossRef]
- Navani, V.; Wells, J.C.; Boyne, D.J.; Cheung, W.Y.; Brenner, D.M.; McGregor, B.A.; Labaki, C.; Schmidt, A.L.; McKay, R.R.; Meza, L.; et al. Caboseq: The Effectiveness of Cabozantinib in Patients with Treatment Refractory Advanced Renal Cell Carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium (Imdc). Clin. Genitourin. Cancer 2023, 21, 106.e1–106.e8. [Google Scholar] [CrossRef]
- Shah, A.Y.; Kotecha, R.R.; Lemke, E.A.; Chandramohan, A.; Chaim, J.L.; Msaouel, P.; Xiao, L.; Gao, J.; Campbell, M.T.; Zurita, A.J.; et al. Outcomes of Patients with Metastatic Clear-Cell Renal Cell Carcinoma Treated with Second-Line Vegfr-Tki after First-Line Immune Checkpoint Inhibitors. Eur. J. Cancer 2019, 114, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Bedke, J.; Albiges, L.; Capitanio, U.; Giles, R.H.; Hora, M.; Lam, T.B.; Ljungberg, B.; Marconi, L.; Klatte, T.; Volpe, A.; et al. Updated European Association of Urology Guidelines on Renal Cell Carcinoma: Nivolumab Plus Cabozantinib Joins Immune Checkpoint Inhibition Combination Therapies for Treatment-Naïve Metastatic Clear-Cell Renal Cell Carcinoma. Eur. Urol. 2021, 79, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Rathmell, W.K.; Rumble, R.B.; Van Veldhuizen, P.J.; Al-Ahmadie, H.; Emamekhoo, H.; Hauke, R.J.; Louie, A.V.; Milowsky, M.I.; Molina, A.M.; Rose, T.L.; et al. Management of Metastatic Clear Cell Renal Cell Carcinoma: Asco Guideline. J. Clin. Oncol. 2022, 40, 2957–2995. [Google Scholar] [CrossRef] [PubMed]
- Kucharz, J.; Budnik, M.; Dumnicka, P.; Pastuszczak, M.; Kuśnierz-Cabala, B.; Demkow, T.; Popko, K.; Wiechno, P. Hand-Foot Syndrome and Progression-Free Survival in Patients Treated with Sunitinib for Metastatic Clear Cell Renal Cell Carcinoma. Adv. Exp. Med. Biol. 2019, 1133, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, J.D.; Wolfe, N.K.; Rich, M.W. Perioperative Care of the Geriatric Patient for Noncardiac Surgery. Clin. Cardiol. 2020, 43, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.; Brenner, B.M. The Aging Kidney: Structure, Function, Mechanisms, and Therapeutic Implications. J. Am. Geriatr. Soc. 1987, 35, 590–593. [Google Scholar] [CrossRef]
- European Medicines Agency. Summmary of Product Characteristics Cabozantinib. 2021. Available online: https://Www.Ema.Europa.Eu/En/Documents/Product-Information/Cabometyx-Epar-Product-Information_En.Pdf (accessed on 11 November 2023).
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (Ctcae) Version 5.0. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 20 December 2023).
- Choueiri, T.K.; Escudier, B.; Powles, T.; Tannir, N.M.; Mainwaring, P.N.; Rini, B.I.; Hammers, H.J.; Donskov, F.; Roth, B.J.; Peltola, K.; et al. Cabozantinib Versus Everolimus in Advanced Renal Cell Carcinoma (Meteor): Final Results from a Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2016, 17, 917–927. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Halabi, S.; Sanford, B.L.; Hahn, O.; Michaelson, M.D.; Walsh, M.K.; Feldman, D.R.; Olencki, T.; Picus, J.; Small, E.J.; et al. Cabozantinib Versus Sunitinib as Initial Targeted Therapy for Patients with Metastatic Renal Cell Carcinoma of Poor or Intermediate Risk: The Alliance A031203 Cabosun Trial. J. Clin. Oncol. 2017, 35, 591–597. [Google Scholar] [CrossRef]
- Bodnar, L.; Kopczyńska, A.; Żołnierek, J.; Wieczorek-Rutkowska, M.; Chrom, P.; Tomczak, P. Real-World Experience of Cabozantinib as Second- or Subsequent Line Treatment in Patients with Metastatic Renal Cell Carcinoma: Data from the Polish Managed Access Program. Clin. Genitourin. Cancer 2019, 17, e556–e564. [Google Scholar] [CrossRef]
- Iinuma, K.; Tomioka-Inagawa, R.; Kameyama, K.; Taniguchi, T.; Kawada, K.; Ishida, T.; Nagai, S.; Enomoto, T.; Ueda, S.; Kawase, M.; et al. Efficacy and Safety of Cabozantinib in Patients with Advanced or Metastatic Renal Cell Carcinoma: A Multicenter Retrospective Cohort Study. Biomedicines 2022, 10, 3172. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.D.; Li, J.; Ly, N.; Faggioni, R.; Roskos, L. Cabozantinib Exposure-Response Analysis for the Phase 3 Checkmate 9er Trial of Nivolumab Plus Cabozantinib Versus Sunitinib in First-Line Advanced Renal Cell Carcinoma. Cancer Chemother. Pharmacol. 2023, 91, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Buda-Nowak, A.; Kucharz, J.; Dumnicka, P.; Kuzniewski, M.; Herman, R.M.; Zygulska, A.L.; Kusnierz-Cabala, B. Sunitinib-Induced Hypothyroidism Predicts Progression-Free Survival in Metastatic Renal Cell Carcinoma Patients. Med. Oncol. 2017, 34, 68. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Gu, J. Hand-Foot Skin Reaction with Vascular Endothelial Growth Factor Receptor Tyrosine Kinase Inhibitors in Cancer Patients: A Systematic Review and Meta-Analysis. Crit. Rev. Oncol. Hematol. 2017, 119, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Bono, P.; Rautiola, J.; Utriainen, T.; Joensuu, H. Hypertension as Predictor of Sunitinib Treatment Outcome in Metastatic Renal Cell Carcinoma. Acta Oncol. 2011, 50, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Belum, V.R.; Serna-Tamayo, C.; Wu, S.; Lacouture, M.E. Incidence and Risk of Hand-Foot Skin Reaction with Cabozantinib, a Novel Multikinase Inhibitor: A Meta-Analysis. Clin. Exp. Dermatol. 2016, 41, 8–15. [Google Scholar] [CrossRef]
- Di Nunno, V.; Frega, G.; Gatto, L.; Brandi, G.; Massari, F. Hypothyroidism in Patients with Hepatocellular Carcinoma Receiving Cabozantinib: An Unassessed Issue. Future Oncol. 2019, 15, 563–565. [Google Scholar] [CrossRef]
- Peverelli, G.; Raimondi, A.; Ratta, R.; Verzoni, E.; Bregni, M.; Cortesi, E.; Cartenì, G.; Fornarini, G.; Facchini, G.; Buti, S.; et al. Cabozantinib in Renal Cell Carcinoma with Brain Metastases: Safety and Efficacy in a Real-World Population. Clin. Genitourin. Cancer 2019, 17, 291–298. [Google Scholar] [CrossRef]
- Janusch, M.; Fischer, M.; Marsch, W.; Holzhausen, H.J.; Kegel, T.; Helmbold, P. The Hand-Foot Syndrome—A Frequent Secondary Manifestation in Antineoplastic Chemotherapy. Eur. J. Dermatol. 2006, 16, 494–499. [Google Scholar]
- Escudier, B.; Eisen, T.; Stadler, W.M.; Szczylik, C.; Oudard, S.; Siebels, M.; Negrier, S.; Chevreau, C.; Solska, E.; Desai, A.A.; et al. Sorafenib in Advanced Clear-Cell Renal-Cell Carcinoma. N. Engl. J. Med. 2007, 356, 125–134. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib Versus Interferon Alfa in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef]
- Pożarowska, D.; Pożarowski, P. The Era of Anti-Vascular Endothelial Growth Factor (Vegf) Drugs in Ophthalmology, Vegf and Anti-Vegf Therapy. Cent. Eur. J. Immunol. 2016, 41, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, A.D.; Robert, C.; Zhu, A.X. Hand-Foot Syndrome (Hand-Foot Skin Reaction, Palmar-Plantar Erythrodysesthesia): Focus on Sorafenib and Sunitinib. Oncology 2009, 77, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Michaelson, M.D.; Cohen, D.P.; Li, S.; Motzer, R.; Escudier, B.J.; Barrios, C.H.; Burnett, P.; Puzanov, I. Hand-Foot Syndrome (Hfs) as a Potential Biomarker of Efficacy in Patients (Pts) with Metastatic Renal Cell Carcinoma (Mrcc) Treated with Sunitinib (Su). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29 (Suppl. S7), 320. [Google Scholar] [CrossRef]
- Poprach, A.; Pavlik, T.; Melichar, B.; Puzanov, I.; Dusek, L.; Bortlicek, Z.; Vyzula, R.; Abrahamova, J.; Buchler, T. Skin Toxicity and Efficacy of Sunitinib and Sorafenib in Metastatic Renal Cell Carcinoma: A National Registry-Based Study. Ann. Oncol. 2012, 23, 3137–3143. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Huang, H. Acquired Hypothyroidism in Patients with Metastatic Renal Cell Carcinoma Treated with Tyrosine Kinase Inhibitors. Drug Des. Dev. Ther. 2020, 14, 3977–3982. [Google Scholar] [CrossRef] [PubMed]
- Makita, N.; Iiri, T. Tyrosine Kinase Inhibitor-Induced Thyroid Disorders: A Review and Hypothesis. Thyroid 2013, 23, 151–159. [Google Scholar] [CrossRef]
- Makita, N.; Miyakawa, M.; Fujita, T.; Iiri, T. Sunitinib Induces Hypothyroidism with a Markedly Reduced Vascularity. Thyroid Off. J. Am. Thyroid Assoc. 2010, 20, 323–326. [Google Scholar] [CrossRef]
- Wolter, P.; Stefan, C.; Decallonne, B.; Dumez, H.; Fieuws, S.; Wildiers, H.; Clement, P.; Debaere, D.; Van Oosterom, A.; Schöffski, P. Evaluation of Thyroid Dysfunction as a Candidate Surrogate Marker for Efficacy of Sunitinib in Patients (Pts) with Advanced Renal Cell Cancer (Rcc). J. Clin. Oncol. 2008, 26, 5126. [Google Scholar] [CrossRef]
- Kust, D.; Prpić, M.; Murgić, J.; Jazvić, M.; Jakšić, B.; Krilić, D.; Bolanča, A.; Kusić, Z. Hypothyroidism as a Predictive Clinical Marker of Better Treatment Response to Sunitinib Therapy. Anticancer Res. 2014, 34, 3177–3184. [Google Scholar]
- Kucharz, J.; Dumnicka, P.; Kusnierz-Cabala, B.; Demkow, T.; Wiechno, P. The Correlation between the Incidence of Adverse Events and Progression-Free Survival in Patients Treated with Cabozantinib for Metastatic Renal Cell Carcinoma (Mrcc). Med. Oncol. 2019, 36, 19. [Google Scholar] [CrossRef]
- Riesenbeck, L.M.; Bierer, S.; Hoffmeister, I.; Köpke, T.; Papavassilis, P.; Hertle, L.; Thielen, B.; Herrmann, E. Hypothyroidism Correlates with a Better Prognosis in Metastatic Renal Cancer Patients Treated with Sorafenib or Sunitinib. World J. Urol. 2011, 29, 807–813. [Google Scholar] [CrossRef]
- Pinto, F.A.I.; Pereira, A.A.R.; Formiga, M.N.; Fanelli, M.F.; Chinen, L.T.D.; Lima, V.C.; De Melo Gagliato, D.; Santos, E.S.; Dettino, A.A.; Sousa, C.E.P.; et al. Association of Hypothyroidism with Improved Outcomes in First-Line Treatment of Renal Cell Carcinoma with Sunitinib. J. Clin. Oncol. 2012, 30, 466. [Google Scholar] [CrossRef]
- Schmidinger, M.; Vogl, U.M.; Bojic, M.; Lamm, W.; Heinzl, H.; Haitel, A.; Clodi, M.; Kramer, G.; Zielinski, C.C. Hypothyroidism in Patients with Renal Cell Carcinoma: Blessing or Curse? Cancer 2011, 117, 534–544. [Google Scholar] [CrossRef]
- Wang, H.E.; Muntner, P.; Chertow, G.M.; Warnock, D.G. Acute Kidney Injury and Mortality in Hospitalized Patients. Am. J. Nephrol. 2012, 35, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Allinovi, M.; Sessa, F.; Villa, G.; Cocci, A.; Innocenti, S.; Zanazzi, M.; Tofani, L.; Paparella, L.; Curi, D.; Cirami, C.L.; et al. Novel Biomarkers for Early Detection of Acute Kidney Injury and Prediction of Long-Term Kidney Function Decline after Partial Nephrectomy. Biomedicines 2023, 11, 1046. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, T.; Takemura, K.; Hayashida, M.; Suyama, K.; Urakami, S.; Miura, Y. Cabozantinib-Induced Serum Creatine Kinase Elevation and Rhabdomyolysis: A Retrospective Case Series. Cancer Chemother. Pharmacol. 2023, 92, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Schmidinger, M.; Danesi, R. Management of Adverse Events Associated with Cabozantinib Therapy in Renal Cell Carcinoma. Oncologist 2018, 23, 306–315. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Values Observed in mRCC Patients (n = 71) |
|---|---|
| male sex, n (%) | 46 (65) |
| mean age (SD), years | 63 (9) |
| median time from RCC diagnosis (Q1; Q3), years | 4.3 (2.0; 8.2) |
| mean BMI (SD), kg/m2 | 28.1 (5.9) |
| morphology | |
| clear cell, n (%) | 69 (97) |
| non-clear cell, n (%) | 6 (8) |
| sarcomatoid differentiation, n (%) | 11 (14) |
| nephrectomy, n (%) | 69 (97) |
| Fuhrman grade | |
| 1, n (%) | 6 (8) |
| 2, n (%) | 33 (46) |
| 3, n (%) | 21 (30) |
| 4, n (%) | 11 (15) |
| MSKCC score | |
| 0, n (%) | 19 (27) |
| 1, n (%) | 36 (51) |
| 2, n (%) | 15 (21) |
| 3, n (%) | 1 (1) |
| IMDC prognostic score | |
| 0, n (%) | 16 (23) |
| 1, n (%) | 30 (42) |
| 2, n (%) | 15 (21) |
| 3, n (%) | 7 (10) |
| 4, n (%) | 3 (4) |
| metastases | |
| lungs, n (%) | 53 (75) |
| bone, n (%) | 24 (34) |
| liver, n (%) | 12 (17) |
| pancreas, n (%) | 6 (8) |
| other sites, n (%) | 31 (44) |
| median number of sites (Q1; Q3) | 2 (2; 3) |
| ECOG performance score | |
| 0, n (%) | 19 (27) |
| 1, n (%) | 42 (59) |
| 2, n (%) | 9 (13) |
| 3, n (%) | 1 (1) |
| Karnofsky performance scale | |
| 100, n (%) | 10 (14) |
| 90, n (%) | 21 (30) |
| 80, n (%) | 37 (52) |
| <80, n (%) | 3 (4) |
| cabozantinib as 2nd-line treatment, n (%) | 30 (42) |
| cabozantinib as 3rd-line treatment, n (%) | 36 (50) |
| cabozantinib as 4th- or 5th-line treatment, n (%) | 5 (7) |
| n (%) | |
|---|---|
| 1st-line treatment | |
| TKI (sunitinib, pazopanib, sorafenib), n (%) | 65 (92) |
| other (immunotherapy), n (%) | 6 (8) |
| 2nd-line treatment | |
| TKI (axitinib, sunitinib, pazopanib, sorafenib), n (%) | 20 (28) |
| everolimus, temsirolimus, n (%) | 18 (25) |
| nivolumab, n (%) | 3 (4) |
| 3rd-line treatment | |
| TKI (sorafenib, pazopanib), n (%) | 4 (6) |
| nivolumab, n (%) | 1 (1) |
| 4th-line treatment (nivolumab), n (%) | 1 (1) |
| Laboratory Test | Values Observed in mRCC Patients (n = 71) |
|---|---|
| median hemoglobin (Q1; Q3), g/dL | 13.1 (11.0; 14.4) |
| median neutrophils (Q1; Q3), G/L | 3.80 (3.20; 5.30) |
| median lymphocytes (Q1; Q3), G/L | 1.73 (1.26; 2.30) |
| median platelets (Q1; Q3), G/L | 252 (198; 343) |
| median NLR (Q1; Q3) | 2.46 (1.53; 3.63) |
| median PLR (Q1; Q3) | 137 (98; 214) |
| Variable | Values Observed in mRCC Patients (n = 71) |
|---|---|
| any adverse event, n (%) | 65 (92) |
| hypothyroidism, n (%) | 35 (49) |
| hand–foot syndrome, n (%) | 33 (46) |
| hypertension, n (%) | 28 (39) |
| diarrhea, n (%) | 28 (39) |
| asthenia, n (%) | 24 (34) |
| liver toxicity, n (%) | 11 (15) |
| >1 reported adverse event, n (%) | 39 (55) |
| median number of adverse events (Q1, Q3) | 2 (1–4) |
| dose reduction | 35 (49) |
| Variable | Simple Analysis | Multiple Model | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| cabozantinib in 3rd line or further (vs. 2nd) | 0.50 (0.28–0.89) | 0.019 | 0.49 (0.24–0.97) | 0.041 |
| time from RCC diagnosis, per 1 year | 0.91 (0.85–0.99) | 0.031 | not included | |
| IMDC (score 3 or 4) | 2.99 (1.41–6.35) | 0.004 | 2.23 (1.00–5.02) | 0.51 |
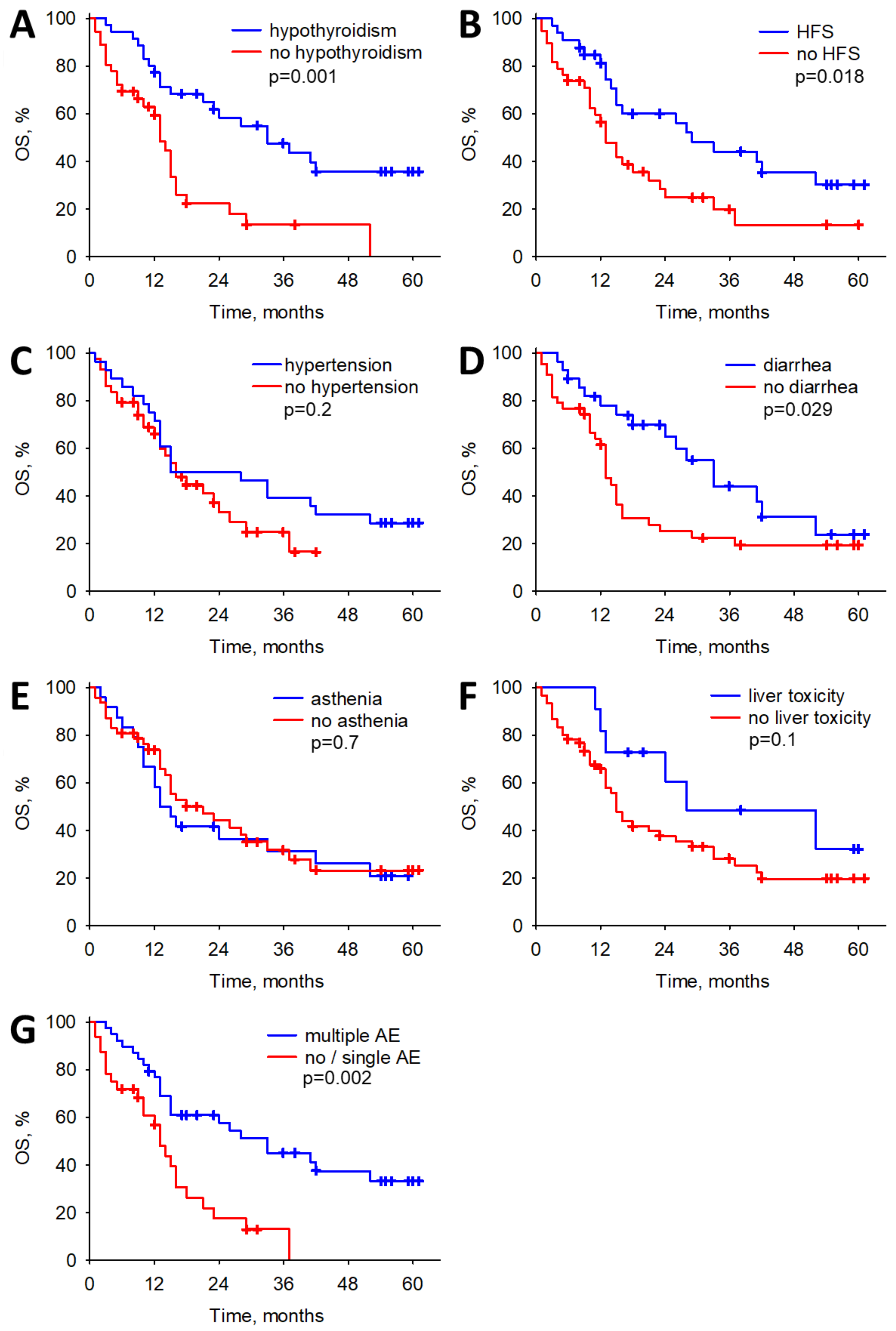
| hypothyroidism | 0.35 (0.19–0.65) | <0.001 | 0.31 (0.15–0.62) | 0.001 |
| hand–foot syndrome | 0.49 (0.27–0.90) | 0.020 | 0.46 (0.24–0.89) | 0.021 |
| diarrhea | 0.53 (0.29–0.97) | 0.039 | not included | |
| number of adverse events, per 1 event | 0.71 (0.57–0.88) | 0.002 | not included | |
| multiple adverse events | 0.36 (0.19–0.66) | 0.001 | not included | |
| hemoglobin, per 1 g/dL | 0.81 (0.70–0.93) | 0.003 | not included | |
| neutrophils, per 1 G/L | 1.20 (1.03–1.40) | 0.017 | not included | |
| platelets, per 100 G/L | 1.45 (1.12–1.87) | 0.005 | not included | |
| NLR | 1.19 (1.05–1.35) | 0.007 | 1.29 (1.12–1.48) | <0.001 |
| PLR | 1.005 (1.003–1.008) | <0.001 | not included | |
| Variable | Simple Analysis | Multiple Model | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| cabozantinib in 3rd line or further (vs. 2nd) | 0.34 (0.20–0.59) | <0.001 | 0.29 (0.16–0.53) | <0.001 |
| IMDC–poor risk (score 3 or 4) | 2.13 (1.03–4.41) | 0.042 | 1.58 (0.73–3.41) | 0.2 |
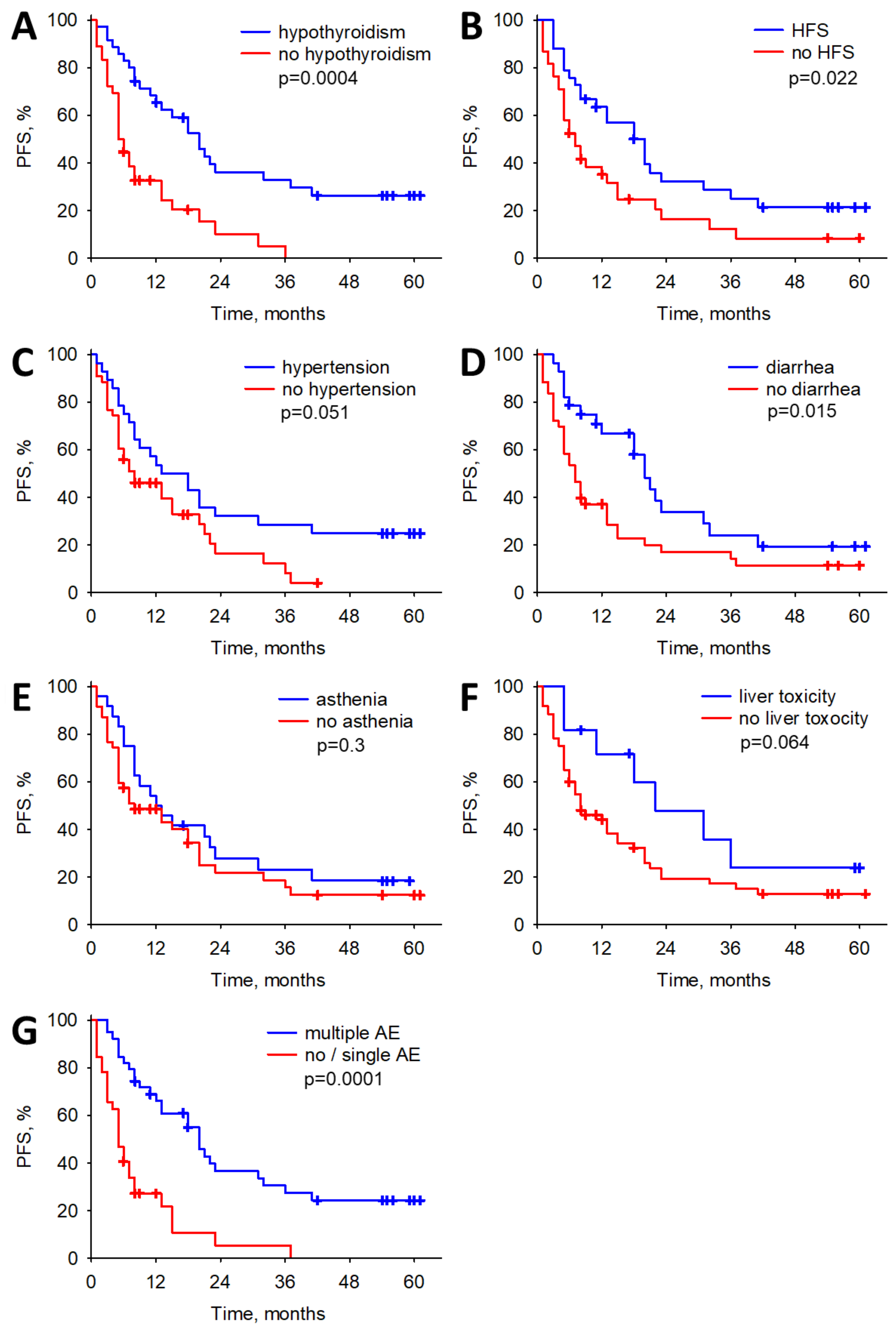
| hypothyroidism | 0.35 (0.20–0.62) | <0.001 | 0.34 (0.18–0.65) | <0.001 |
| hand–foot syndrome | 0.54 (0.31–0.93) | 0.026 | not included | |
| diarrhea | 0.52 (0.30–0.92) | 0.024 | not included | |
| number of adverse events, per 1 event | 0.68 (0.55–0.83) | <0.001 | not included | |
| multiple adverse events | 0.30 (0.17–0.53) | <0.001 | not included | |
| hemoglobin, per 1 g/dL | 0.80 (0.70–0.91) | <0.001 | 0.82 (0.70–0.97) | 0.017 |
| platelets, per 100 G/L | 1.26 (1.001–1.58) | 0.049 | not included | |
| PLR | 1.004 (1.002–1.007) | <0.001 | 1.004 (1.001–1.007) | 0.016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domański, P.; Piętak, M.; Kruczyk, B.; Jarosińska, J.; Mydlak, A.; Demkow, T.; Darewicz, M.; Sikora-Kupis, B.; Dumnicka, P.; Kamzol, W.; et al. Adverse Events of Cabozantinib as a Potential Prognostic Factor in Metastatic Renal Cell Carcinoma Patients: Real-World Experience in a Single-Center Retrospective Study. Biomedicines 2024, 12, 413. https://doi.org/10.3390/biomedicines12020413
Domański P, Piętak M, Kruczyk B, Jarosińska J, Mydlak A, Demkow T, Darewicz M, Sikora-Kupis B, Dumnicka P, Kamzol W, et al. Adverse Events of Cabozantinib as a Potential Prognostic Factor in Metastatic Renal Cell Carcinoma Patients: Real-World Experience in a Single-Center Retrospective Study. Biomedicines. 2024; 12(2):413. https://doi.org/10.3390/biomedicines12020413
Chicago/Turabian StyleDomański, Piotr, Mateusz Piętak, Barbara Kruczyk, Jadwiga Jarosińska, Anna Mydlak, Tomasz Demkow, Marta Darewicz, Bożena Sikora-Kupis, Paulina Dumnicka, Wojciech Kamzol, and et al. 2024. "Adverse Events of Cabozantinib as a Potential Prognostic Factor in Metastatic Renal Cell Carcinoma Patients: Real-World Experience in a Single-Center Retrospective Study" Biomedicines 12, no. 2: 413. https://doi.org/10.3390/biomedicines12020413
APA StyleDomański, P., Piętak, M., Kruczyk, B., Jarosińska, J., Mydlak, A., Demkow, T., Darewicz, M., Sikora-Kupis, B., Dumnicka, P., Kamzol, W., & Kucharz, J. (2024). Adverse Events of Cabozantinib as a Potential Prognostic Factor in Metastatic Renal Cell Carcinoma Patients: Real-World Experience in a Single-Center Retrospective Study. Biomedicines, 12(2), 413. https://doi.org/10.3390/biomedicines12020413