
The Significance of Selected Myokines in Predicting the Length of Rehabilitation of Patients after COVID-19 Infection
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
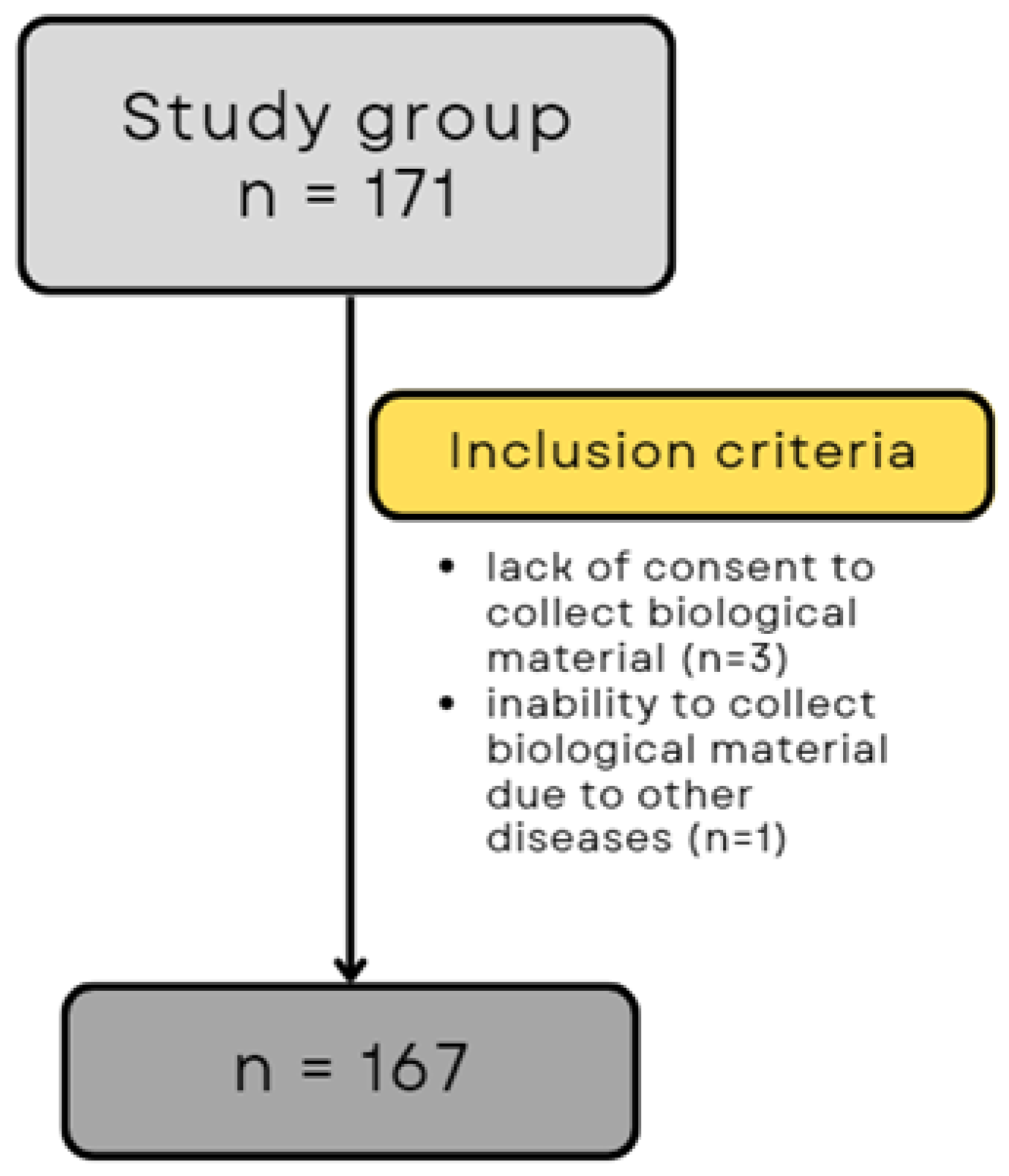
2.1. Patients
2.2. Study Process
- Breathing exercises (active breathing exercises, active breathing exercises with resistance, learning effective coughing, and clearing the airways, time: 30 min);
- Aerobic exercise (stair climbing, outdoor walking, continuous/interval exercise on a bicycle ergometer, assessment of exercise tolerance by monitoring oxygen saturation (pulse oximeter), and perceived exertion on the Borg scale; gradual increase in intensity by 5–10%, time: 90 min);
- Strength and endurance training (individualized training based on 1 repetition maximum (1 RM) and exercise tolerance (assessment of desaturation); load: 70–85% of 1RM; volume: 3 sets of 8–12 repetitions; rest: 1–2 min; progression: 60–70% of 1RM, time: 30 min).
2.3. Blood Sampling
2.4. ELISA Tests
2.5. Statistical Analyses
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barbalho, S.M.; Minniti, G.; Miola, V.F.B.; Haber, J.F.D.S.; Bueno, P.C.D.S.; Haber, L.S.d.A.; Girio, R.S.J.; Detregiachi, C.R.P.; Dall’antonia, C.T.; Rodrigues, V.D.; et al. Organokines in COVID-19: A Systematic Review. Cells 2023, 12, 1349. [Google Scholar] [CrossRef] [PubMed]
- Filgueira, T.O.; Castoldi, A.; Santos, L.E.R.; de Amorim, G.J.; de Sousa Fernandes, M.S.; Anastácio, W.d.L.D.N.; Campos, E.Z.; Santos, T.M.; Souto, F.O. The Relevance of a Physical Active Lifestyle and Physical Fitness on Immune Defense: Mitigating Disease Burden, With Focus on COVID-19 Consequences. Front. Immunol. 2021, 12, 587146. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J.; et al. Skeletal muscle alterations in patients with acute COVID-19 and post-acute sequelae of COVID-19. J. Cachexia Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Ragab, D.; Salah Eldin, H.; Taeimah, M.; Khattab, R.; Salem, R. The COVID-19 Cytokine Storm; What We Know So Far. Front. Immunol. 2020, 11, 1446. [Google Scholar] [CrossRef] [PubMed]
- Soares-Schanoski, A.; Sauerwald, N.; Goforth, C.W.; Periasamy, S.; Weir, D.L.; Lizewski, S.; Lizewski, R.; Ge, Y.; Kuzmina, N.A.; Nair, V.D.; et al. Asymptomatic SARS-CoV-2 Infection Is Associated with Higher Levels of Serum IL-17C, Matrix Metalloproteinase 10 and Fibroblast Growth Factors Than Mild Symptomatic COVID-19. Front. Immunol. 2022, 13, 821730. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; Sciorati, C.; Capobianco, A.; Lorè, N.I.; Giustina, A.; Manfredi, A.A.; Rovere-Querini, P.; Conte, C. Adiponectin to leptin ratio reflects inflammatory burden and survival in COVID-19. Diabetes Metab. 2021, 47, 101268. [Google Scholar] [CrossRef] [PubMed]
- Aryana, I.; Setiati, S.; Rini, S.S. Molecular Mechanism of -Acute Sarcopenia in Elderly Patient with COVID-19. Acta Med. Indones. 2021, 53, 481–492. [Google Scholar] [PubMed]
- Pedersen, B.K.; Åkerström, T.C.A.; Nielsen, A.R.; Fischer, C.P. Role of Myokines in Exercise and Metabolism. J. Appl. Physiol. 2007, 103, 1093–1098. [Google Scholar] [CrossRef]
- Pedersen, B.K. Muscle as a secretory organ. Compr. Physiol. 2013, 3, 1337–1362. [Google Scholar] [CrossRef]
- Choi, K.M. The impact of organokines on insulin resistance, inflammation, and atherosclerosis. Endocrinol. Metab. 2016, 31, 1–6. [Google Scholar] [CrossRef]
- Coelho-Junior, H.J.; Picca, A.; Calvani, R.; Uchida, M.C.; Marzetti, E. If my muscle could talk: Myokines as a biomarker of frailty. Exp. Gerontol. 2019, 127, 110715. [Google Scholar] [CrossRef]
- Severinsen, M.C.K.; Pedersen, B.K. Muscle-Organ Crosstalk: The Emerging Roles of Myokines. Endocr. Rev. 2020, 41, 594–609. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.U.; Ghafoor, S. Myokines: Discovery challenges and therapeutic impediments. J. Pak. Med. Assoc. 2019, 69, 1014–1017. [Google Scholar] [PubMed]
- Delezie, J.; Handschin, C. Endocrine Crosstalk Between Skeletal Muscle and the Brain. Front. Neurol. 2018, 9, 698. [Google Scholar] [CrossRef]
- Boström, P.; Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Rasbach, K.A.; Boström, E.A.; Choi, J.H.; Long, J.Z.; et al. A PGC1α-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature 2012, 481, 463–468. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Anastasilakis, A.D.; Efstathiadou, Z.A.; Makras, P.; Perakakis, N.; Kountouras, J.; Mantzoros, C.S. Irisin in Metabolic Diseases. Endocrine 2018, 59, 260–274. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, M.; De Sibio, M.T.; Mathias, L.S.; Rodrigues, B.M.; Sakalem, M.E.; Nogueira, C.R. Irisin modulates genes associated with severe coronavirus disease (COVID-19) outcome in human subcutaneous adipocytes cell culture. Mol. Cell Endocrinol. 2020, 515, 110917. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Zhang, Z.; Wang, X.; Zhang, J.; Ren, C.; Li, Y.; Gao, L.; Liang, X.; Wang, P.; Ma, C. Palmitoylation of SARS-CoV-2 S protein is essential for viral infectivity. Signal Transduct. Target. Ther. 2021, 6, 231. [Google Scholar] [CrossRef] [PubMed]
- Seldin, M.M.; Peterson, J.M.; Byerly, M.S.; Wei, Z.; Wong, G.W. Myonectin (CTRP15), a novel myokine that links skeletal muscle to systemic lipid homeostasis. J. Biol. Chem. 2012, 287, 11968–11980. [Google Scholar] [CrossRef]
- Little, H.C.; Rodriguez, S.; Lei, X.; Tan, S.Y.; Stewart, A.N.; Sahagun, A.; Sarver, D.C.; Wong, G.W. Myonectin deletion promotes adipose fat storage and reduces liver steatosis. FASEB J. 2019, 33, 8666–8687. [Google Scholar] [CrossRef]
- Schäffler, A.; Buechler, C. CTRP family: Linking immunity to metabolism. Trends Endocrinol. Metab. 2012, 23, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Gros, K.; Matkovič, U.; Parato, G.; Miš, K.; Luin, E.; Bernareggi, A.; Sciancalepore, M.; Marš, T.; Lorenzon, P.; Pirkmajer, S. Neuronal Agrin Promotes Proliferation of Primary Human Myoblasts in an Age-Dependent Manner. Int. J. Mol. Sci. 2022, 23, 11784. [Google Scholar] [CrossRef] [PubMed]
- Consitt, L.A.; Clark, B.C. The vicious cycle of myostatin signaling in sarcopenic obesity: Myostatin role in skeletal muscle growth, insulin signaling and implications for clinical trials. J. Frailty Aging 2018, 7, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.L.; Hittel, D.S.; McPherron, A.C. Expression and Function of Myostatin in Obesity, Diabetes, and Exercise Adaptation. Med. Sci. Sports Exerc. 2011, 43, 1828–1835. [Google Scholar] [CrossRef] [PubMed]
- Hittel, D.S.; Berggren, J.R.; Shearer, J.; Boyle, K.; Houmard, J.A. Increased Secretion and Expression of Myostatin in Skeletal Muscle from Extremely Obese Women. Diabetes 2009, 58, 30–38. [Google Scholar] [CrossRef]
- Order of the President of the National Health Fund No. 172/2021/DSOZ of 18 October 2021. Available online: https://baw.nfz.gov.pl/NFZ/tabBrowser/mainPage (accessed on 9 March 2023).
- Klok, F.A.; Boon, G.J.A.M.; Barco, S.; Endres, M.; Geelhoed, J.J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status scale: A tool to measure functional status over time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef]
- Paternostro-Sluga, T.; Grim-Stieger, M.; Posch, M.; Schuhfried, O.; Vacariu, G.; Mittermaier, C.; Bittner, C.; Fialka-Moser, V. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J. Rehabil. Med. 2008, 40, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Hayata, A.; Minakata, Y.; Matsunaga, K.; Nakanishi, M.; Yamamoto, N. Differences in physical activity according to mMRC grade in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2203–2208. [Google Scholar] [PubMed]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, V.; Hernandes, N.A.; Mitchell, K.E.; Hill, C.J.; Lee, A.L.; Camillo, C.A.; Troosters, T.; Spruit, M.A.; et al. An official systematic review of the European Respiratory Society/American Thoracic Society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef]
- Intarakamhang, P.; Wangjongmeechaikul, P. The assessment of dyspnea during the vigorous intensity exercise by three Dyspnea Rating Scales in inactive medical personnel. Glob. J. Health Sci. 2013, 5, 19–29. [Google Scholar] [CrossRef]
- Alhanbali, S.; AlJasser, A.; Aboudi, O.; Alaqrabawi, W.; Munro, K.J. Establishing the reliability and the validity of the Arabic translated versions of the Effort Assessment Scale and the Fatigue Assessment Scale. Int. J. Audiol. 2023, 62, 853–858. [Google Scholar] [CrossRef]
- Udina, C.; Ars, J.; Morandi, A.; Vilaró, J.; Cáceres, C.; Inzitari, M. Rehabilitation in adult post-COVID-19 patients in post-acute care with Therapeutic Exercise. J. Frailty Aging 2021, 10, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Wittmer, V.L.; Paro, F.M.; Duarte, H.; Capellini, V.K.; Barbalho-Moulim, M.C. Early mobilization and physical exercise in patients with COVID-19: A narrative literature review. Complement. Ther. Clin. Pract. 2021, 43, 101364. [Google Scholar] [CrossRef]
- Lugo-Agudelo, L.H.; Cruz Sarmiento, K.M.; Spir Brunal, M.A.; Velásquez Correa, J.C.; Posada Borrero, A.M.; Franco, L.; Ianini, R.; Lis, P.; Vélez, C.; Lugo, D.; et al. Adaptations for rehabilitation services during the COVID-19 pandemic proposed by scientific organizations and rehabilitation professionals. J. Rehabil. Med. 2021, 53, jrm00228. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Loboda, D.; Gibinski, M.; Wilczek, J.; Paradowska-Nowakowska, E.; Ekiert, K.; Rybicka, E.; Sarecka-Hujar, B.; Szoltysek-Boldys, I.; Zielinska-Danch, W.; Golba, K.S. Effectiveness of cardiopulmonary rehabilitation after COVID-19 in Poland. Pol. Arch. Intern. Med. 2023, 133, 16341. [Google Scholar] [CrossRef]
- Hermann, M.; Pekacka-Egli, A.M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary Rehabilitation After COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Hockele, L.F.; Sachet Affonso, J.V.; Rossi, D.; Eibel, B. Pulmonary and Functional Rehabilitation Improves Functional Capacity, Pulmonary Function and Respiratory Muscle Strength in Post COVID-19 Patients: Pilot Clinical Trial. Int. J. Environ. Res. Public. Health. 2022, 19, 14899. [Google Scholar] [CrossRef]
- Alizadeh Pahlavani, H. Exercise Therapy for People With Sarcopenic Obesity: Myokines and Adipokines as Effective Actors. Front. Endocrinol 2022, 13, 811751. [Google Scholar] [CrossRef]
- Tokunbo, O.; Abayomi, T.; Adekomi, D.; Oyeyipo, I. COVID-19: Sitting is the new smoking; the role of exercise in augmenting the immune system among the elderly. Afr. Health Sci. 2021, 21, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.-P.; Maggi, S.; Ecarnot, F. Raising awareness of the needs of older COVID patients after hospital discharge. Aging Clin. Exp. Res. 2020, 32, 1595–1598. [Google Scholar] [CrossRef] [PubMed]
- Stam, H.J.; Stucki, G.; Bickenbach, J. European Academy of Rehabilitation Medicine COVID-19 and post intensive care syndrome: A call for action. J. Rehabil. Med. 2020, 52, jrm00044. [Google Scholar] [CrossRef] [PubMed]
- Kozłowska-Flis, M.; Rodziewicz-Flis, E.; Micielska, K.; Kortas, J.; Jaworska, J.; Borkowska, A.; Sansoni, V.; Perego, S.; Lombardi, G.; Ziemann, E. Short and long-term effects of high-intensity interval training applied alone or with whole-body cryostimulation on glucose homeostasis and myokine levels in overweight to obese subjects. Front. Biosci. 2021, 26, 1132–1146. [Google Scholar] [CrossRef]
- Kirwan, R.; McCullough, D.; Butler, T.; de Heredia, F.P.; Davies, I.G.; Stewart, C. Sarcopenia during COVID-19 lockdown restrictions: Long-term health effects of short-term muscle loss. GeroScience 2020, 42, 1547–1578. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Liu, P.; Wu, H.; Zhou, X. Relation between serum myostatin with BMI and PaO2/PaCO2 in patients with chronic obstructive pulmonary disease. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2014, 39, 807–810. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-Z.; Ma, J.-D.; Yang, L.-J.; Zou, Y.-W.; Zhang, X.-P.; Pan, J.; Li, Q.-H.; Li, H.-G.; Yang, Z.-H.; Wu, T.; et al. Myokine Myostatin Is a Novel Predictor of One-Year Radiographic Progression in Patients with Rheumatoid Arthritis: A Prospective Cohort Study. Front. Immunol. 2022, 13, 1005161. [Google Scholar] [CrossRef] [PubMed]
- Grunow, J.J.; Reiher, K.; Carbon, N.M.; Engelhardt, L.J.; Mai, K.; Koch, S.; Schefold, J.C.; Z’graggen, W.; Schaller, S.J.; Fielitz, J.; et al. Muscular Myostatin Gene Expression and Plasma Concentrations Are Decreased in Critically Ill Patients. Crit. Care Lond. Engl. 2022, 26, 237. [Google Scholar] [CrossRef]
- Escobar, J.; Van Alstine, W.G.; Baker, D.H.; Johnson, R.W. Decreased Protein Accretion in Pigs with Viral and Bacterial Pneumonia Is Associated with Increased Myostatin Expression in Muscle. J. Nutr. 2004, 134, 3047–3053. [Google Scholar] [CrossRef]


{kind=link}
| Variable | n | % | |
|---|---|---|---|
| Sex | Female | 91 | 53.2 |
| Male | 76 | 46.8 | |
| Age | <60 years | 46 | 26.9 |
| >60 years | 121 | 73.1 | |
| Nutritional status (BMI) | 18.5–24.99 (norm) | 36 | 21.1 |
| 25.0–29.9 (overweight) | 60 | 35.1 | |
| 30.0–34.99 (1st degree obesity). | 48 | 28.1 | |
| 35.0–39.99 (2nd degree obesity). | 18 | 10.5 | |
| over 40 (3rd degree obesity) | 5 | 2.9 | |
| Hospitalization | Yes | 117 | 68.4 |
| No | 44 | 25.7 | |
| Length of hospitalization | 1–5 days | 5 | 2.9 |
| 6–10 days | 18 | 7.6 | |
| 11–15 days | 31 | 18.1 | |
| 16–20 days | 18 | 10.5 | |
| More than 20 days | 50 | 29.2 | |
| Pneumonia during COVID-19 infection | Yes | 128 | 74.8 |
| No | 34 | 19.9 | |
| Oxygen therapy during hospitalization | Yes | 106 | 61.9 |
| No | 38 | 22.2 | |
| The duration of rehabilitation | 2–3 weeks | 75 | 43.8 |
| 3–4 weeks | 23 | 13.5 | |
| 4–5 weeks | 16 | 9.4 | |
| 5–6 weeks | 51 | 29.8 | |
| Comorbidities | Diabetes | 50 | 29.2 |
| Hypertension | 113 | 66.1 | |
| Asthma | 19 | 11.1 | |
| COPD | 9 | 5.3 | |
| Smoking status | Yes | 15 | 8.8 |
| No | 146 | 85.4 | |
| Concentration of myokines | Me ± SD | ||
| Myostatin (ng/mL) | 326.8 ± 316.2 | ||
| Agrin (ng/mL) | 3.5 ± 3.2 | ||
| Irisin (ng/mL) | 13.1 ± 17.9 | ||
| Myonectin (ng/mL) | 5.0 ± 4.7 | ||
| Variable | Before Rehabilitation | After Rehabilitation | p |
|---|---|---|---|
| M (±SD) | M (±SD) | ||
| 6MWT distance (m) | 370.03 (±122.63) | 490.47 (±144.26) | <0.001 * |
| 6MWT distance (%predicted). | 74.61 (±23.53) | 98.44 (±24.89) | <0.001 * |
| Borg’s scale (6–20) | 12.26 (±2.28) | 10.39 (±2.61) | <0.001 * |
| FVC (% predicted) | 83.39 (±22.71) | 89.71 ± 21.47 | 0.016 * |
| FEV1 (% predicted) | 86.36 (±24.01) | 96.81 (21.46) | <0.001 * |
| FEV1/FVC (%) | 86.32 (13.23) | 87.39 (9.91) | 0.071 |
| mMRC | 2.55 (0.66) | 0.73 (0.72) | <0.001 * |
| FAS scale | 28.21 (9.05) | 20.68 (6.63) | <0.001 * |
| Clamping force (kg) | 27.23 (10.84) | 29.69 (10.91) | <0.001 * |
| Variable | Myostatin | Agrin | Irisin | Myonectin | |||||
|---|---|---|---|---|---|---|---|---|---|
| M ± SD | p | M ± SD | p | M ± SD | p | M ± SD | p | ||
| Sex | Female | 315.83 ± 301.14 | 0.878 | 3.33 ± 3.12 | 0.362 | 14.71 ± 18.92 | 0.08 | 5.52 ± 5.23 | 0.166 |
| Male | 339.62 ± 334.60 | 3.68 ± 3.31 | 11.07 ± 16.67 | 4.37 ± 3.96 | |||||
| Age | <65 | 318.34 ± 270.99 | 0.694 | 4.27 ± 3.75 | 0.121 | 14.66 ± 20.28 | 0.785 | 5.75 ± 4.95 | 0.072 |
| >65 | 329.83 ± 331.87 | 3.18 ± 2.91 | 12.41 ± 17.03 | 4.72 ± 4.62 | |||||
| BMI | <25 | 423.48 ± 400.46 | 0.042 * | 3.25 ± 2.52 | 0.469 | 15.31 ± 21.70 | 0.917 | 5.23 ± 4.34 | 0.331 |
| ≥25 | 374.34 ± 350.33 | 3.52 ± 2.91 | 12.61 ± 17.65 | 4.35 ± 3.90 | |||||
| ≤30 | 238.73 ± 199.09 | 3.57 ± 3.67 | 12.29 ± 16.27 | 5.43 ± 5.48 | |||||
| Hospitalization | Yes | 325.96 ± 325.11 | 0.645 | 3.23 ± 2.97 | 0.284 | 12.12 ± 16.83 | 0.287 | 4.92 ± 4.71 | 0.427 |
| No | 326.21 ± 302.71 | 4.15 ± 3.79 | 15.02 ± 19.59 | 4.94 ± 4.77 | |||||
| Diabetes | Yes | 341.61 ± 299.32 | 0.548 | 3.46 ± 3.42 | 0.530 | 12.17 ± 17.29 | 0.581 | 4.42 ± 4.49 | 0.142 |
| No | 297.38 ± 326.57 | 3.51 ± 3.15 | 13.77 ± 18.58 | 5.24 ± 4.87 | |||||
| Hypertension | Yes | 309.31 ± 316.51 | 0.062 | 3.31 ± 2.97 | 0.542 | 13.26 ± 17.77 | 0.357 | 5.02 ± 4.93 | 0.623 |
| No | 374.11 ± 320.39 | 3.94 ± 3.76 | 13.29 ± 19.17 | 4.94 ± 4.38 | |||||
| Variable | R | p | |
|---|---|---|---|
| Duration of hospitalization | Myostatin | 0.24713 | 0.008 * |
| Agrin | 0.06777 | 0.469 | |
| Irisin | 0.02055 | 0.825 | |
| Myonectin | −0.10978 | 0.241 | |
| Variable | R | p | |
|---|---|---|---|
| Rehabilitation time | Myostatin | 0.17618 | 0.029 * |
| Agrin | −0.07789 | 0.323 | |
| Irisin | −0.24241 | 0.002 * | |
| Myonectin | −0.24592 | 0.001 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mińko, A.; Turoń-Skrzypińska, A.; Rył, A.; Mańkowska, K.; Cymbaluk-Płoska, A.; Rotter, I. The Significance of Selected Myokines in Predicting the Length of Rehabilitation of Patients after COVID-19 Infection. Biomedicines 2024, 12, 836. https://doi.org/10.3390/biomedicines12040836
Mińko A, Turoń-Skrzypińska A, Rył A, Mańkowska K, Cymbaluk-Płoska A, Rotter I. The Significance of Selected Myokines in Predicting the Length of Rehabilitation of Patients after COVID-19 Infection. Biomedicines. 2024; 12(4):836. https://doi.org/10.3390/biomedicines12040836
Chicago/Turabian StyleMińko, Alicja, Agnieszka Turoń-Skrzypińska, Aleksandra Rył, Katarzyna Mańkowska, Aneta Cymbaluk-Płoska, and Iwona Rotter. 2024. "The Significance of Selected Myokines in Predicting the Length of Rehabilitation of Patients after COVID-19 Infection" Biomedicines 12, no. 4: 836. https://doi.org/10.3390/biomedicines12040836