

Radiological Imaging Findings of Adrenal Abnormalities in TAFRO Syndrome: A Systematic Review
 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Literature Search
- (TAFRO) AND (adrenal) on PubMed;
- TAFRO on the Cochrane Library;
- TAFRO AND adrenal on the Web of Science Core Collection.
- The article includes patients with TAFRO syndrome with adrenal abnormalities, namely, adrenal ischemia/infarction, adrenal hemorrhage, and/or adrenomegaly.
- CT or MRI were performed.
- Each patient’s demographic and clinical information was available.
- CT or MRI images of the adrenal glands could not be evaluated.
2.2. Criteria for TAFRO Syndrome
2.3. Data Analyses
2.4. Collected Data
- Patient’s age;
- Sex;
- Histopathological diagnosis of lymph nodes (presence or absence).
- Abdominal pain during the course of the disease (presence or absence);
- Abdominal pain at onset (presence or absence);
- Type of adrenal abnormalities (adrenal ischemia/infarction, adrenal hemorrhage, and/or adrenomegaly) within the articles of the study;
- Side of the affected adrenal gland (unilateral or bilateral).
- Adrenal ischemia/infarction;
- Adrenal hemorrhage;
- Adrenomegaly;
- Adrenal calcification over time (presence or absence).
2.5. Quality Assessment
3. Results
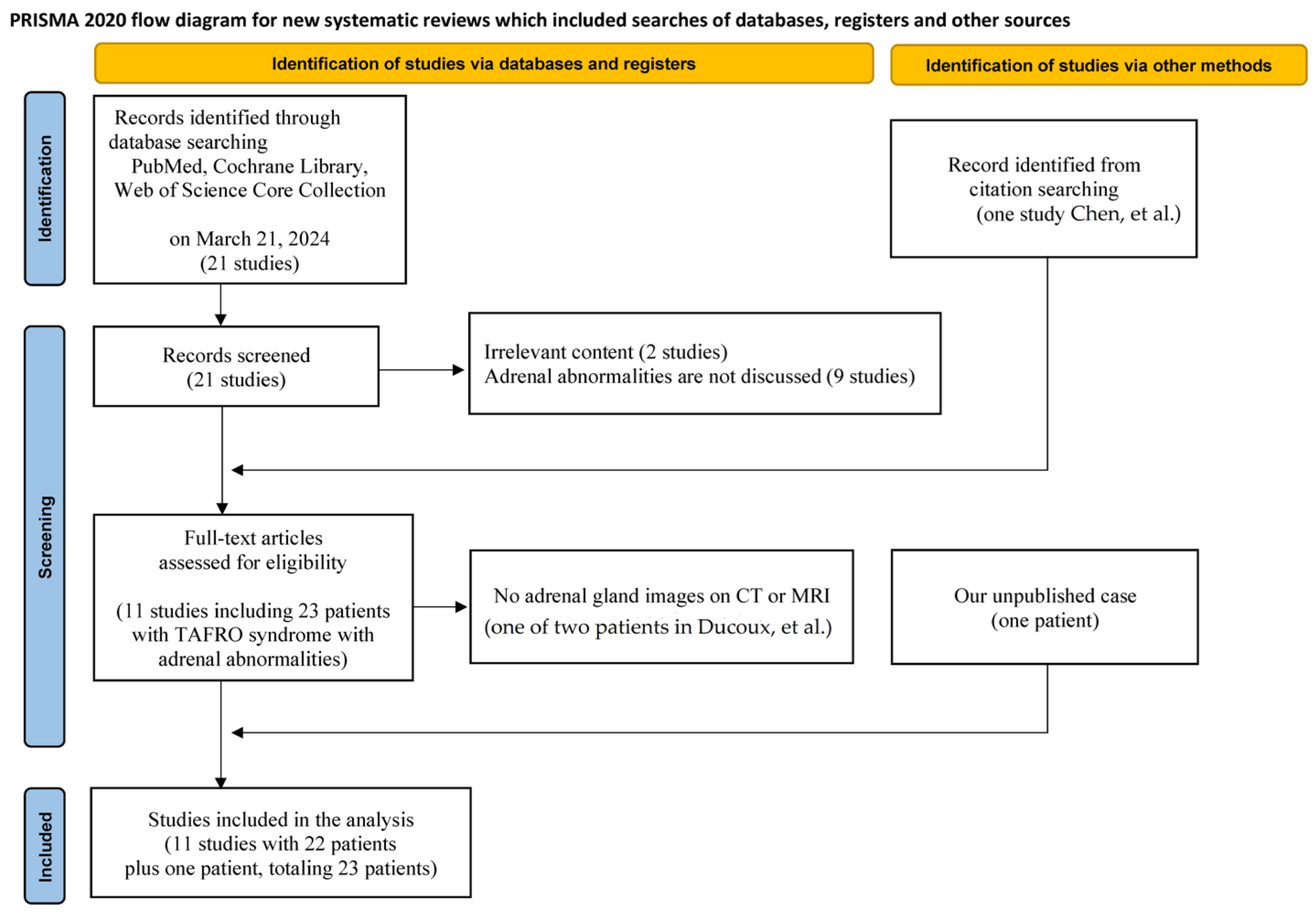
3.1. Study Selection
3.2. Risk of Bias Assessment
3.3. Demographic and Clinical Data

| Study | Age [Year] Mean ± Standard Deviation | Sex | Histopathological Diagnosis of Lymph Node | Adrenal Findings | Unilateral or Bilateral | Concurrent Adrenomegaly in Ischemia/Infarction or Hemorrhage | Calcification Over Time | Abdominal Pain | Abdominal Pain at Disease Onset |
|---|---|---|---|---|---|---|---|---|---|
| 47.0 ± 12.6 | Male = 20, Female = 3 | YES = 15, NO = 8 | Ischemia/infarction = 11, Hemorrhage = 9 *, Adrenomegaly without evidence of adrenal ischemia/infarction or hemorrhage = 4 * | Bilateral = 17, Unilateral = 6 | YES = 20, NO = 0, Unknown = 0 | YES = 9, NO = 5, Unknown = 9 | YES = 15, NO = 8 | YES = 15, NO = 8 | |
| Kurokawa [7] | 24 | Female | YES | Ischemia/infarction | Bilateral | YES | YES | YES | YES |
| 50 | Male | NO | Ischemia/infarction | Unilateral | YES | NO | NO | NO | |
| 71 | Male | YES | Hemorrhage | Bilateral | YES ** | NO | YES | YES | |
| 33 | Male | NO | Ischemia/infarction | Bilateral | YES | NO | YES | YES | |
| 55 | Male | NO | Ischemia/infarction | Bilateral | YES | NO | NO | NO | |
| 53 | Male | YES | Ischemia/infarction | Bilateral | YES | YES | NO | NO | |
| 35 | Male | YES | Adrenomegaly | Bilateral | NO | NO | NO | ||
| Fujimi [14] | 54 | Male | YES | Adrenomegaly | Bilateral | Unknown | YES | YES | |
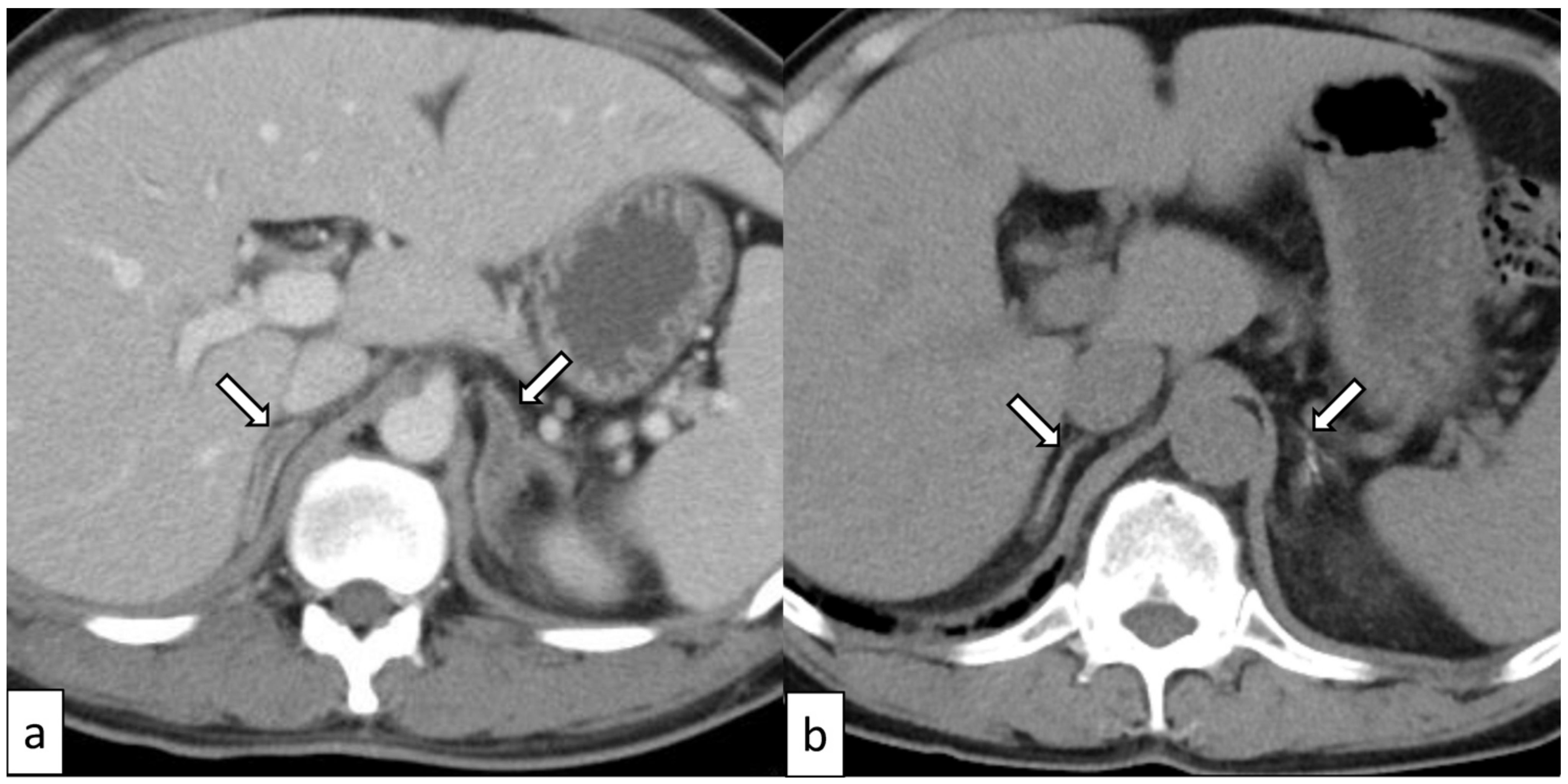
| Our case | 38 (Figure 2) | Male | YES | Ischemia/infarction | Bilateral | YES | YES | YES | YES |
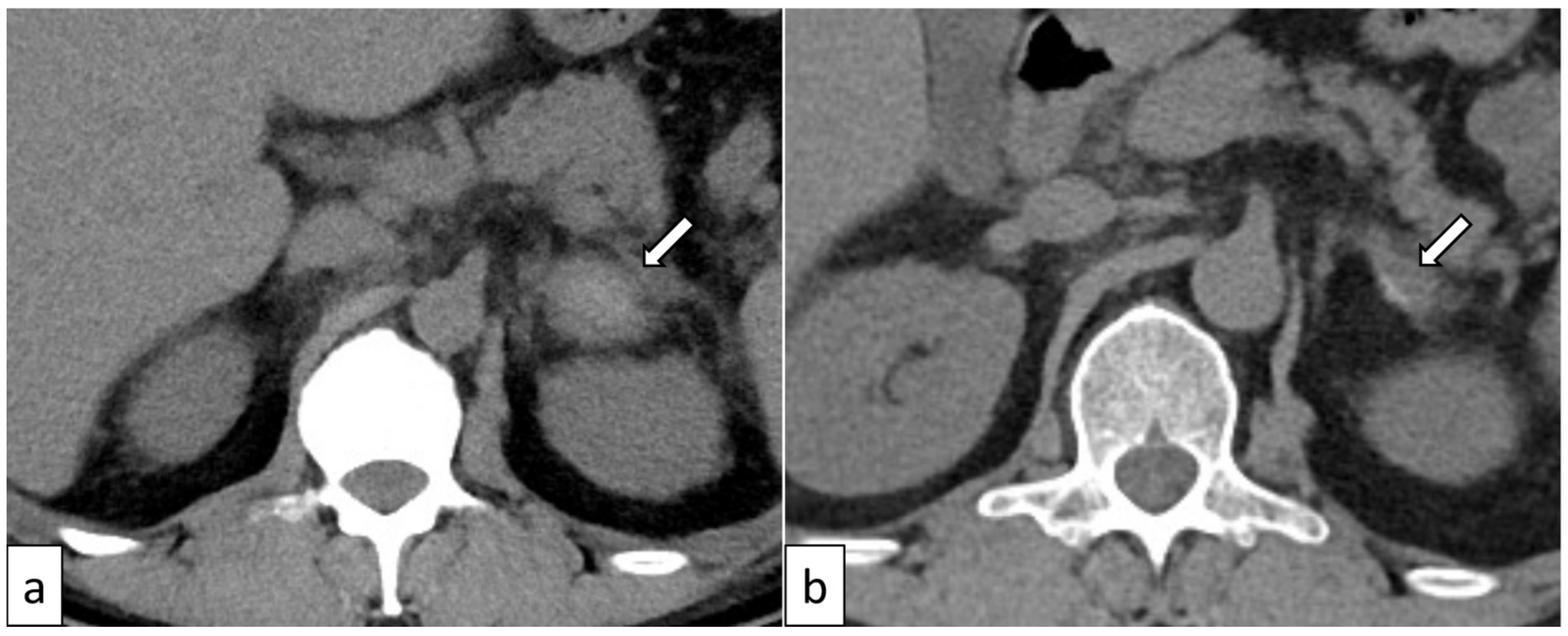
| Kano [15] | 50 (Figure 3) | Male | NO | Hemorrhage and contralateral adrenomegaly * | Bilateral | YES | YES | YES | YES |
| 66 | Male | YES | Hemorrhage | Bilateral | YES | YES | NO | NO | |
| 45 | Male | NO | Adrenomegaly | Bilateral | YES | NO | NO | ||
| 43 | Male | NO | Hemorrhage | Bilateral | YES ** | YES | YES | YES | |
| 41 | Male | NO | Hemorrhage | Bilateral | YES | YES | YES | YES | |
| 51 | Male | YES | Ischemia/infarction | Bilateral | YES | YES | YES | YES | |
| Yonezaki [16] | 53 | Female | YES | Ischemia/infarction | Bilateral | YES | Unknown | YES | YES |
| Ono [17] | 43 | Male | YES | Ischemia/infarction | Unilateral | YES | Unknown | YES | YES |
| Okamoto [18] | 70 | Female | NO | Hemorrhage | Unilateral | YES | Unknown | YES | YES |
| Ducoux G [19] | 19 | Male | YES | Hemorrhage | Bilateral | YES | Unknown | YES | YES |
| Fujiwara [20] | 46 | Male | YES | Ischemia/infarction | Unilateral | YES | Unknown | YES | YES |
| Ito [21] | 48 | Male | YES | Hemorrhage | Bilateral | YES | Unknown | NO | NO |
| Nara [22] | 48 | Male | YES | Hemorrhage | Unilateral | YES | Unknown | NO | NO |
| Chen [23] | 46 | Male | YES | Ischemia/infarction | Unilateral | YES | Unknown | YES | YES |
3.4. Adrenal Ischemia/Infarction
3.5. Adrenal Hemorrhage
3.6. Adrenomegaly
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Takai, K.; Nikkuni, K.; Momoi, A.; Nagai, K.; Igarashi, N.; Saeki, T. Thrombocytopenia with Reticulin Fibrosis Accompanied by Fever, Anasarca and Hepatosplenomegaly: A Clinical Report of Five Cases. J. Clin. Exp. Hematop. 2013, 53, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Iwaki, N.; Fajgenbaum, D.C.; Nabel, C.S.; Gion, Y.; Kondo, E.; Kawano, M.; Masunari, T.; Yoshida, I.; Moro, H.; Nikkuni, K.; et al. Clinicopathologic Analysis of TAFRO Syndrome Demonstrates a Distinct Subtype of HHV-8-Negative Multicentric Castleman Disease. Am. J. Hematol. 2016, 91, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Dispenzieri, A.; Fajgenbaum, D.C. Overview of Castleman Disease. Blood 2020, 135, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Masaki, Y.; Kawabata, H.; Takai, K.; Kojima, M.; Tsukamoto, N.; Ishigaki, Y.; Kurose, N.; Ide, M.; Murakami, J.; Nara, K.; et al. Proposed Diagnostic Criteria, Disease Severity Classification and Treatment Strategy for TAFRO Syndrome, 2015 Version. Int. J. Hematol. 2016, 103, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Masaki, Y.; Kawabata, H.; Takai, K.; Tsukamoto, N.; Fujimoto, S.; Ishigaki, Y.; Kurose, N.; Miura, K.; Nakamura, S.; Aoki, S.; et al. 2019 Updated Diagnostic Criteria and Disease Severity Classification for TAFRO Syndrome. Int. J. Hematol. 2020, 111, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, T.; Sato, C.; Takai, K.; Nakai, Y.; Kaneko, Y.; Matsuki, M. CT Findings in 11 Patients with TAFRO Syndrome: A Variant of Multicentric Castleman’s Disease. Clin. Radiol. 2017, 72, 905.e1–905.e5. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, R.; Gonoi, W.; Yokota, H.; Isshiki, S.; Ohira, K.; Mizuno, H.; Kiguchi, T.; Inui, S.; Kurokawa, M.; Kato, S.; et al. Computed Tomography Findings of Early-Stage TAFRO Syndrome and Associated Adrenal Abnormalities. Eur. Radiol. 2020, 30, 5588–5598. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological Quality and Synthesis of Case Series and Case Reports. BMJ Evid. Based. Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, R.; Baba, A.; Kurokawa, M.; Ota, Y.; Hassan, O.; Capizzano, A.; Kim, J.; Johnson, T.; Srinivasan, A.; Moritani, T. Neuroimaging of Astroblastomas: A Case Series and Systematic Review. J. Neuroimaging 2022, 32, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, R.; Baba, A.; Emile, P.; Kurokawa, M.; Ota, Y.; Kim, J.; Capizzano, A.; Srinivasan, A.; Moritani, T. Neuroimaging Features of Angiocentric Glioma: A Case Series and Systematic Review. J. Neuroimaging 2022, 32, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, M.; Kurokawa, R.; Capizzano, A.A.; Baba, A.; Ota, Y.; Pinarbasi, E.; Johnson, T.; Srinivasan, A.; Moritani, T. Neuroradiological Features of the Polymorphous Low-Grade Neuroepithelial Tumor of the Young: Five New Cases with a Systematic Review of the Literature. Neuroradiology 2022, 64, 1255–1264. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, R.; Baba, A.; Kurokawa, M.; Pinarbasi, E.S.; Makise, N.; Ota, Y.; Kim, J.; Srinivasan, A.; Moritani, T. Neuroimaging Features of Diffuse Hemispheric Glioma, H3 G34-Mutant: A Case Series and Systematic Review. J. Neuroimaging 2021, 32, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Fujimi, A.; Nagamachi, Y.; Yamauchi, N.; Onoyama, N.; Matsuno, T.; Miyajima, N.; Koike, K.; Goto, Y.; Ihara, K.; Nishisato, T.; et al. Acute Abdomen and Adrenal Swelling as the First Manifestations of TAFRO Syndrome. Intern. Med. 2023, 62, 1675–1681. [Google Scholar] [CrossRef] [PubMed]
- Kano, R.; Igarashi, T.; Kikuchi, R.; Ojiri, H.; Katsube, A.; Yano, S. Evaluation of the Correlation between Multiple Organ Calcification on CT and Disease Severity in Patients with TAFRO Syndrome. Jpn. J. Radiol. 2023, 41, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Yonezaki, S.; Nagasaki, K.; Yamaguchi, H.; Kobayashi, H. Bilateral Adrenal Infarctions as an Initial Manifestation of TAFRO Syndrome: A Case Report and Review of the Literature. Intern. Med. 2022, 61, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Yoshimoto, K.; Nishimura, N.; Yoneima, R.; Kawashima, H.; Kobayashi, T.; Tai, Y.; Miyamoto, M.; Tsushima, E.; Yada, N.; et al. Complete Resolution of a Case of TAFRO Syndrome Accompanied by Mediastinal Panniculitis, Adrenal Lesion, and Liver Damage with Hyperbilirubinemia. Intern. Med. 2021, 60, 1303–1309. [Google Scholar] [CrossRef]
- Okamoto, T.; Ochi, S.; Motokawa, Y.; Azumi, H.; Kobayashi, S.; Nakamura, F.; Nakatani, T.; Yagi, H. Fatal Case of TAFRO Syndrome with Unilateral Adrenal Hemorrhage in Early-Stage Disease. J. Clin. Exp. Hematop. 2021, 61, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Ducoux, G.; Guerber, A.; Durel, C.-A.; Asli, B.; Fadlallah, J.; Hot, A. Thrombocytopenia, Anasarca, Fever, Reticulin Fibrosis/Renal Failure, and Organomegaly (TAFRO) Syndrome with Bilateral Adrenal Hemorrhage in Two Caucasian Patients. Am. J. Case Rep. 2020, 21, e919536. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Ito, K.; Takamura, A.; Nagata, K. The First Case of Thrombocytopenia, Anasarca, Fever, Renal Impairment or Reticulin Fibrosis, and Organomegaly (TAFRO) Syndrome with Unilateral Adrenal Necrosis: A Case Report. J. Med. Case Rep. 2018, 12, 295. [Google Scholar] [CrossRef] [PubMed]
- Ito, F.; Kameoka, Y.; Nara, M.; Ubukawa, K.; Fujishima, M.; Yoshioka, T.; Fujishima, N.; Takahashi, N. TAFRO syndrome with bilateral adrenal hemorrhage. Nihon Naika Gakkai Zasshi 2017, 106, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Nara, M.; Komatsuda, A.; Itoh, F.; Kaga, H.; Saitoh, M.; Togashi, M.; Kameoka, Y.; Wakui, H.; Takahashi, N. Two Cases of Thrombocytopenia, Anasarca, Fever, Reticulin Fibrosis/Renal Failure, and Organomegaly (TAFRO) Syndrome with High Serum Procalcitonin Levels, Including the First Case Complicated with Adrenal Hemorrhaging. Intern. Med. 2017, 56, 1247–1252. [Google Scholar] [CrossRef]
- Chen, L.Y.C.; Skinnider, B.F.; Wilson, D.; Fajgenbaum, D.C. Adrenalitis and Anasarca in Idiopathic Multicentric Castleman’s Disease. Lancet 2021, 397, 1749. [Google Scholar] [CrossRef] [PubMed]
- Finocchietto, P.; Contardo, D.; Uehara, T.; Papini, C.; Deligiannis, N.; Darderes, E.; Castroagudin, A.; Cabral, C.; di Fonzo, H. TAFRO Syndrome in a Patient of South-American Descent. Eur. J. Case Rep. Intern. Med. 2015, 2. [Google Scholar] [CrossRef]
- Riddell, A.M.; Khalili, K. Sequential Adrenal Infarction without MRI-Detectable Hemorrhage in Primary Antiphospholipid-Antibody Syndrome. AJR Am. J. Roentgenol. 2004, 183, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Karwacka, I.M.; Obołończyk, Ł.; Sworczak, K. Adrenal Hemorrhage: A Single Center Experience and Literature Review. Adv. Clin. Exp. Med. 2018, 27, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ren, Y.; Ma, L.; Li, J.; Zhu, Y.; Zhao, L.; Tian, H.; Chen, T. Clinical Features of 50 Patients with Primary Adrenal Lymphoma. Front. Endocrinol. 2020, 11, 595. [Google Scholar] [CrossRef] [PubMed]
- Arivazhagan, S.; Parthiban, G.P.; Patterson, C.; Reddy, K. Acute Adrenal Hemorrhage as the Initial Manifestation of Metastatic Lung Adenocarcinoma: A Cautionary Tale. Case Rep. Oncol. Med. 2022, 2022, 2864773. [Google Scholar] [CrossRef] [PubMed]
- Jordan, E.; Poder, L.; Courtier, J.; Sai, V.; Jung, A.; Coakley, F.V. Imaging of Nontraumatic Adrenal Hemorrhage. AJR Am. J. Roentgenol. 2012, 199, W91–W98. [Google Scholar] [CrossRef] [PubMed]
- Merklin, R.J. Suprarenal Gland Lymphatic Drainage. Am. J. Anat. 1966, 119, 359–374. [Google Scholar] [CrossRef]
- Tokiwa, K.; Nakamura, K.; Ogita, S.; Iwai, N.; Hagiwara, A.; Takahashi, T. Lymphatic Drainage of Adrenal Neuroblastoma. J. Pediatr. Surg. 1993, 28, 927–929. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Inoue, A.; Tanaka, T.; Sato, Y.; Potretzke, T.A.; Masuoka, S.; Takahashi, N.; Minami, M.; Kawashima, A. Imaging of Perirenal and Intrarenal Lymphatic Vessels: Anatomy-Based Approach. Radiographics 2024, 44, e230065. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Mori, H.; Kiyonaga, M.; Yamada, Y.; Takaji, R.; Sato, F.; Mimata, H.; Hijiya, N.; Moriyama, M.; Tanoue, R.; et al. Perirenal Lymphatic Systems: Evaluation Using Spectral Presaturation with Inversion Recovery T2 -Weighted MR Images with 3D Volume Isotropic Turbo Spin-Echo Acquisition at 3.0T. J. Magn. Reson. Imaging 2016, 44, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Minomo, S.; Fujiwara, Y.; Sakashita, S.; Takamura, A.; Nagata, K. A Severe Case of Thrombocytopenia, Anasarca, Fever, Renal Insufficiency or Reticulin Fibrosis, and Organomegaly Syndrome with Myocardial and Skeletal Muscle Calcification despite Hypocalcemia: A Case Report. J. Med. Case Rep. 2021, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Raja, A.; Malik, K.; Mahalingam, S. Adrenal Castleman’s Disease: Case Report and Review of Literature. J. Indian Assoc. Pediatr. Surg. 2022, 27, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.S.M. Unicentric Castleman Disease. Hematol. Oncol. Clin. North Am. 2018, 32, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Butzmann, A.; Kumar, J.; Sridhar, K.; Gollapudi, S.; Ohgami, R.S. A Review of Genetic Abnormalities in Unicentric and Multicentric Castleman Disease. Biology 2021, 10, 251. [Google Scholar] [CrossRef] [PubMed]
- Saeed-Abdul-Rahman, I.; Al-Amri, A.M. Castleman Disease. Korean J. Hematol. 2012, 47, 163–177. [Google Scholar] [CrossRef]
- Nishimura, Y.; Hanayama, Y.; Fujii, N.; Kondo, E.; Otsuka, F. Comparison of the Clinical Characteristics of TAFRO Syndrome and Idiopathic Multicentric Castleman Disease in General Internal Medicine: A 6-Year Retrospective Study. Intern. Med. J. 2020, 50, 184–191. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurokawa, R.; Baba, A.; Kano, R.; Kaneko, Y.; Kurokawa, M.; Gonoi, W.; Abe, O. Radiological Imaging Findings of Adrenal Abnormalities in TAFRO Syndrome: A Systematic Review. Biomedicines 2024, 12, 837. https://doi.org/10.3390/biomedicines12040837
Kurokawa R, Baba A, Kano R, Kaneko Y, Kurokawa M, Gonoi W, Abe O. Radiological Imaging Findings of Adrenal Abnormalities in TAFRO Syndrome: A Systematic Review. Biomedicines. 2024; 12(4):837. https://doi.org/10.3390/biomedicines12040837
Chicago/Turabian StyleKurokawa, Ryo, Akira Baba, Rui Kano, Yo Kaneko, Mariko Kurokawa, Wataru Gonoi, and Osamu Abe. 2024. "Radiological Imaging Findings of Adrenal Abnormalities in TAFRO Syndrome: A Systematic Review" Biomedicines 12, no. 4: 837. https://doi.org/10.3390/biomedicines12040837
APA StyleKurokawa, R., Baba, A., Kano, R., Kaneko, Y., Kurokawa, M., Gonoi, W., & Abe, O. (2024). Radiological Imaging Findings of Adrenal Abnormalities in TAFRO Syndrome: A Systematic Review. Biomedicines, 12(4), 837. https://doi.org/10.3390/biomedicines12040837