
Observational Study to Compare Biological Drug Concentration Quantification Techniques and Immunogenicity in Patients with Immune-Mediated Diseases
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Samples Collection
2.3. Measurement of Biologic Drug Serum Levels
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Samples Characteristics
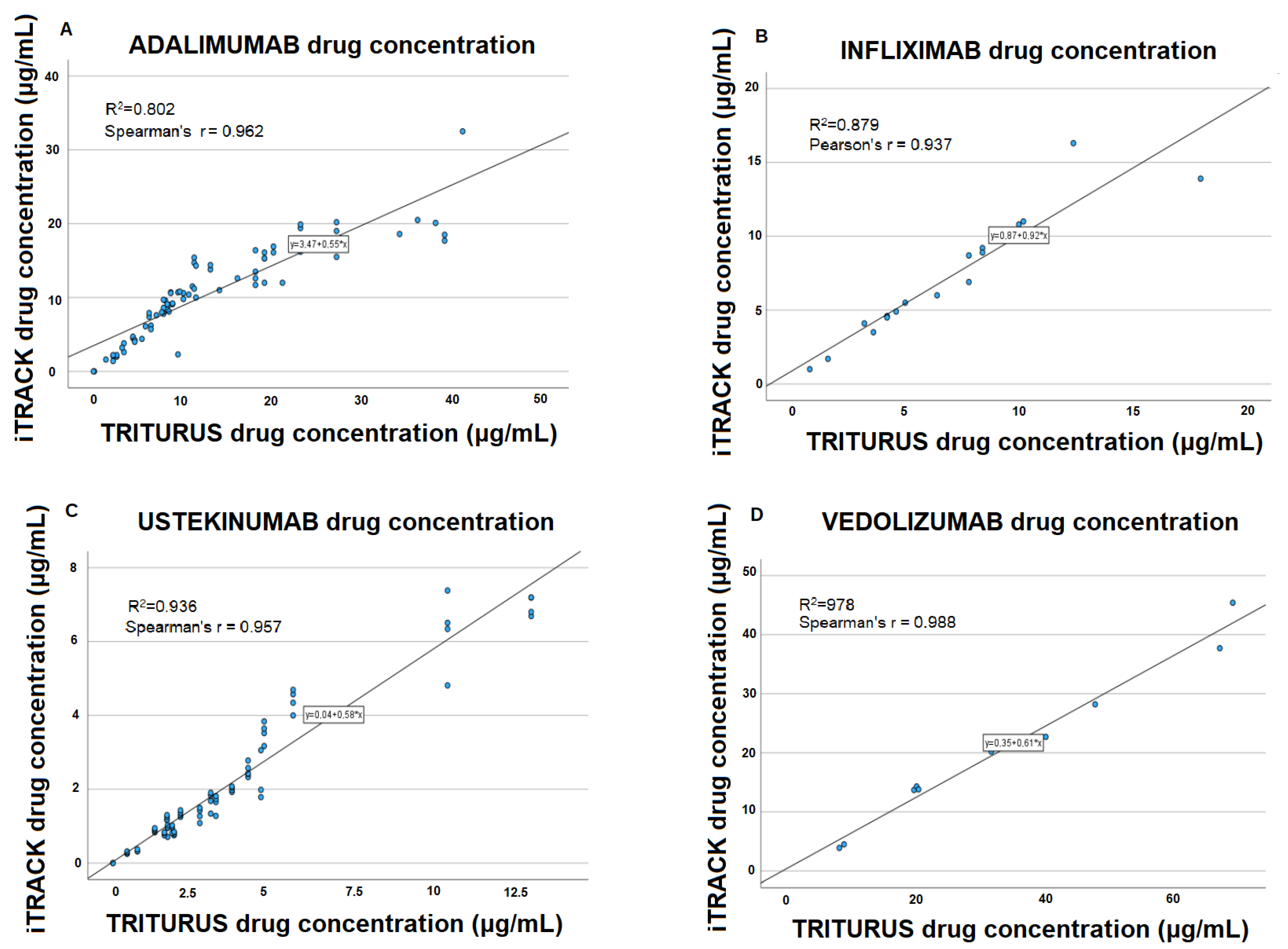
3.2. Data Correlation
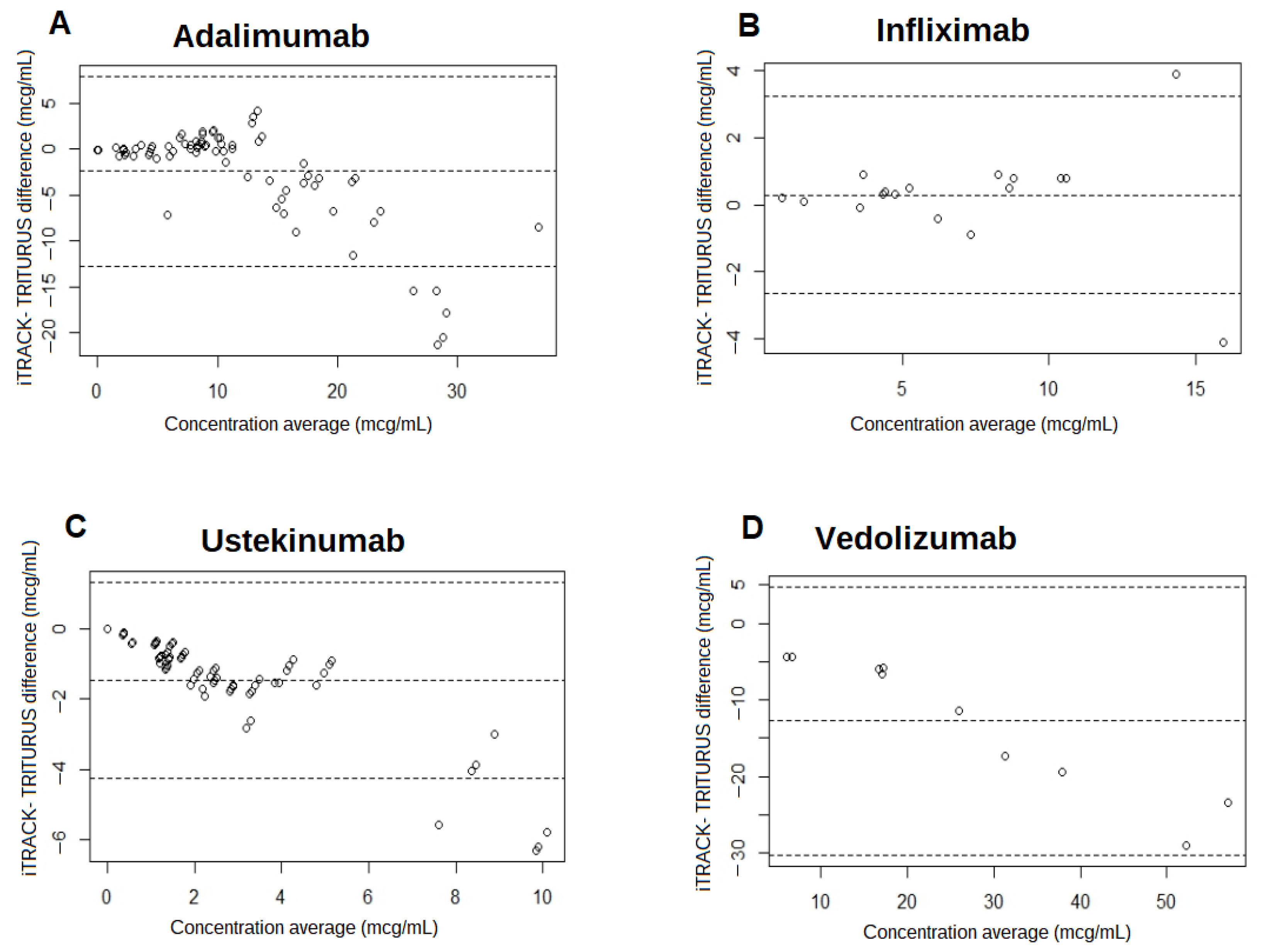
3.3. Data Agreement and Biases
3.3.1. Adalimumab
3.3.2. Infliximab
3.3.3. Ustekinumab
3.3.4. Vedolizumab
3.3.5. ADA Concentrations
3.4. Qualitative Analysis
4. Discussion
4.1. Drug Concentrations
4.2. ADAs Concentration
4.3. Limitations
4.4. Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elberdín Pazos, L.; Outeda Macías, M.; Salvador Garrido, P.; Martín Herranz, M.I. Pharmacokinetic monitoring as a new tool to individualize anti-TNF therapy. Farm. Hosp. Organo Of. Expr. Cient. Soc. Esp. Farm. Hosp. 2014, 38, 83–85. [Google Scholar]
- Restellini, S.; Afif, W. Update on TDM (Therapeutic Drug Monitoring) with Ustekinumab, Vedolizumab and Tofacitinib in Inflammatory Bowel Disease. J. Clin. Med. 2021, 10, 1242. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Vogelzang, E.H.; Lambert, J.; Wolbink, G.; Cheifetz, A.S. Therapeutic Drug Monitoring with Biologic Agents in Immune Mediated Inflammatory Diseases. Expert Rev. Clin. Immunol. 2019, 15, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Del Tedesco, E.; Marotte, H.; Rinaudo-Gaujous, M.; Moreau, A.; Phelip, J.-M.; Genin, C.; Peyrin-Biroulet, L.; Roblin, X. Therapeutic Drug Monitoring of Infliximab and Mucosal Healing in Inflammatory Bowel Disease: A Prospective Study. Inflamm. Bowel Dis. 2013, 19, 2568–2576. [Google Scholar] [CrossRef] [PubMed]
- Krieckaert, C.L.M.; Nair, S.C.; Nurmohamed, M.T.; van Dongen, C.J.J.; Lems, W.F.; Lafeber, F.P.J.G.; Bijlsma, J.W.J.; Koffijberg, H.; Wolbink, G.; Welsing, P.M.J. Personalised Treatment Using Serum Drug Levels of Adalimumab in Patients with Rheumatoid Arthritis: An Evaluation of Costs and Effects. Ann. Rheum. Dis. 2015, 74, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Amiot, A.; Hulin, A.; Belhassan, M.; Andre, C.; Gagniere, C.; Le Baleur, Y.; Farcet, J.-P.; Delchier, J.-C.; Hüe, S. Therapeutic Drug Monitoring Is Predictive of Loss of Response after De-Escalation of Infliximab Therapy in Patients with Inflammatory Bowel Disease in Clinical Remission. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Diz-Lois Palomares, M.T.; Porta Sánchez, Á.; Elberdin Pazos, L.; González Conde, B.; Outeda Macías, M.; Vázquez Rey, M.T.; Estévez Prieto, E.; Martín Herranz, I.; Alonso Aguirre, P. Pharmacokinetic and Clinical Monitoring through Posologic Change in Adalimumab Intensification Regimen from 40 Mg Every Week to 80 Mg Every Other Week. Rev. Esp. Enfermedades Dig. Organo Of. Soc. Esp. Patol. Dig. 2022, 114, 708. [Google Scholar] [CrossRef]
- Ben-Horin, S.; Chowers, Y. Tailoring Anti-TNF Therapy in IBD: Drug Levels and Disease Activity. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 243–255. [Google Scholar] [CrossRef]
- Vande Casteele, N.; Herfarth, H.; Katz, J.; Falck-Ytter, Y.; Singh, S. American Gastroenterological Association Institute Technical Review on the Role of Therapeutic Drug Monitoring in the Management of Inflammatory Bowel Diseases. Gastroenterology 2017, 153, 835–857. [Google Scholar] [CrossRef]
- Cheifetz, A.S.; Abreu, M.T.; Afif, W.; Cross, R.K.; Dubinsky, M.C.; Loftus, E.V.; Osterman, M.T.; Saroufim, A.; Siegel, C.A.; Yarur, A.J.; et al. A Comprehensive Literature Review and Expert Consensus Statement on Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2021, 116, 2014–2025. [Google Scholar] [CrossRef]
- Lázár-Molnár, E.; Delgado, J.C. Immunogenicity Assessment of Tumor Necrosis Factor Antagonists in the Clinical Laboratory. Clin. Chem. 2016, 62, 1186–1198. [Google Scholar] [CrossRef]
- Bader, L.I.; Solberg, S.M.; Kaada, S.H.; Bolstad, N.; Warren, D.J.; Gavasso, S.; Gjesdal, C.G.; Vedeler, C.A. Assays for Infliximab Drug Levels and Antibodies: A Matter of Scales and Categories. Scand. J. Immunol. 2017, 86, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Nasser, Y.; Labetoulle, R.; Harzallah, I.; Berger, A.-E.; Roblin, X.; Paul, S. Comparison of Point-of-Care and Classical Immunoassays for the Monitoring Infliximab and Antibodies Against Infliximab in IBD. Dig. Dis. Sci. 2018, 63, 2714–2721. [Google Scholar] [CrossRef]
- Magro, F.; Afonso, J.; Lopes, S.; Coelho, R.; Gonçalves, R.; Caldeira, P.; Lago, P.; de Sousa, H.T.; Ramos, J.; Gonçalves, A.R.; et al. Clinical Performance of an Infliximab Rapid Quantification Assay. Ther. Adv. Gastroenterol. 2017, 10, 651–660. [Google Scholar] [CrossRef]
- Berger, A.E.; Gleizes, A.; Waeckel, L.; Roblin, X.; Krzysiek, R.; Hacein-Bey-Abina, S.; Soriano, A.; Paul, S. Validation Study of a New Random-Access Chemiluminescence Immunoassay Analyzer i-TRACK10® to Monitor Infliximab and Adalimumab Serum Trough Levels and Anti-Drug Antibodies. Int. J. Mol. Sci. 2022, 23, 9561. [Google Scholar] [CrossRef] [PubMed]
- Cherry, M.; Dutzer, D.; Nasser, Y.; Berger, A.-E.; Roblin, X.; Paul, S. Point-of-Care Assays Could Be Useful for Therapeutic Drug Monitoring of IBD Patients in a Proactive Strategy with Adalimumab. J. Clin. Med. 2020, 9, 2739. [Google Scholar] [CrossRef]
- Laserna-Mendieta, E.J.; Salvador-Martín, S.; Marín-Jiménez, I.; Menchén, L.A.; López-Cauce, B.; López-Fernández, L.A.; Lucendo, A.J. Comparison of a New Rapid Method for Determination of Serum Anti-Adalimumab and Anti-Infliximab Antibodies with Two Established ELISA Kits. J. Pharm. Biomed. Anal. 2021, 198, 114003. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.H.; Aluzaite, K.; Schultz, M.; Casey, P. Infliximab Trough Levels: A Comparison between the Quantum Blue Infliximab Assay and the Established ELISA. J. Gastroenterol. Hepatol. 2020, 35, 1302–1306. [Google Scholar] [CrossRef]
- Facchin, S.; Buda, A.; Cardin, R.; Agbariah, N.; Zingone, F.; De Bona, M.; Zaetta, D.; Bertani, L.; Ghisa, M.; Barberio, B.; et al. Rapid Point-of-Care Anti-Infliximab Antibodies Detection in Clinical Practice: Comparison with ELISA and Potential for Improving Therapeutic Drug Monitoring in IBD Patients. Ther. Adv. Gastroenterol. 2021, 14, 1756284821999902. [Google Scholar] [CrossRef]
- Noguier, G.; Montaillier, C.; Daviere, S.; Yang, Y.; Colombeau, L.; Parussini, E. Development and Evaluation of I-Tracker Ustekinumab and i-Tracker Anti-Ustekinumab Kits: Fast and Innovative Chemiluminescent Assays for the Monitoring of Patients Treated with Ustekinumab. J. Crohns Colitis 2021, 15 (Suppl. S1), S191. [Google Scholar] [CrossRef]
- Noguier, G.; Montaillier, C.; Daviere, S.; Colombeau, L.; Parussini, E. Development and Evaluation of I-TRACKER Infliximab and i-TRACKER Anti-Infliximab Kits: Fast and Innovative Chemiluminescent Assays for the Monitoring of Patients Treated with Infliximab. J. Crohns Colitis 2020, 14 (Suppl. S1), S563. [Google Scholar] [CrossRef]
- Noguier, G.; Montaillier, C.; Daviere, S.; Colombeau, L.; Parussini, E. Development and Evaluation of I-Tracker Adalimumab and i-Tracker Anti-Adalimumab Kits: Fast Innovative Chemiluminescent Assays for the Monitoring of Patients Treated with Adalimumab. Gastroenterology 2020, 158, S-471. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial Diagnosis, Monitoring of Known IBD, Detection of Complications. J. Crohns Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef] [PubMed]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology Consensus Guidelines on the Management of Inflammatory Bowel Disease in Adults. Gut 2019, 68 (Suppl. S3), s1–s106. [Google Scholar] [CrossRef] [PubMed]
- Vande Casteele, N.; Ferrante, M.; Van Assche, G.; Ballet, V.; Compernolle, G.; Van Steen, K.; Simoens, S.; Rutgeerts, P.; Gils, A.; Vermeire, S. Trough Concentrations of Infliximab Guide Dosing for Patients with Inflammatory Bowel Disease. Gastroenterology 2015, 148, 1320–1329. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Rissel, F.; Cazaubon, Y.; Saffar, S.; Altwegg, R.; Artasone, M.; Lozano, C.; Vincent, T.; Jentzer, A. Comparative Evaluation of Four Commercially Available Immunoassays for Therapeutic Drug Monitoring of Infliximab and Adalimumab. Int. J. Mol. Sci. 2023, 24, 10379. [Google Scholar] [CrossRef] [PubMed]
- Restellini, S.; Khanna, R.; Afif, W. Therapeutic Drug Monitoring With Ustekinumab and Vedolizumab in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2018, 24, 2165–2172. [Google Scholar] [CrossRef] [PubMed]
- Verdon, C.; Vande Casteele, N.; Heron, V.; Germain, P.; Afif, W. Comparison of Serum Concentrations of Ustekinumab Obtained by Three Commercial Assays in Patients with Crohn’s Disease. J. Can. Assoc. Gastroenterol. 2021, 4, 73–77. [Google Scholar] [CrossRef]
- Marini, J.C.; Gils, A.; Shankar, G.; Peeters, M.; Brouwers, E.; Van Iperen, P.; Le Bars, M.; Bevalander, G.S.; Sattin, B.; Sloan, S. Comparison of the KU Leuven Ustekinumab Concentration Assay and the Antibodies-to-Ustekinumab Assay with Assays Developed at Janssen R&D and Used in Clinical Studies of IBD Patients. J. Crohns Colitis 2018, 12 (Suppl. S1), S439. [Google Scholar] [CrossRef]
- Pouillon, L.; Rousseau, H.; Busby-Venner, H.; De Carvalho Bittencourt, M.; Choukour, M.; Gauchotte, G.; Zallot, C.; Danese, S.; Baumann, C.; Peyrin-Biroulet, L. Vedolizumab Trough Levels and Histological Healing During Maintenance Therapy in Ulcerative Colitis. J. Crohns Colitis 2019, 13, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Vande Casteele, N.; Yang, L.; Dobler, I.; Agboton, C.; McRorie Osborn, T.; Suri, A.; Lindner, D.; Smithson, G.M. Measuring Serum Vedolizumab and Vedolizumab Antibodies: Comparison of Commercial Assays with the Vedolizumab Clinical Development Assay. Ther. Drug Monit. 2023, 45, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Wyant, T.; Yang, L.; Rosario, M. Comparison of the ELISA and ECL Assay for Vedolizumab Anti-Drug Antibodies: Assessing the Impact on Pharmacokinetics and Safety Outcomes of the Phase 3 GEMINI Trials. AAPS J. 2020, 23, 3. [Google Scholar] [CrossRef] [PubMed]
- Steenholdt, C.; Ainsworth, M.A.; Tovey, M.; Klausen, T.W.; Thomsen, O.O.; Brynskov, J.; Bendtzen, K. Comparison of Techniques for Monitoring Infliximab and Antibodies against Infliximab in Crohn’s Disease. Ther. Drug Monit. 2013, 35, 530–538. [Google Scholar] [CrossRef]
- Pérez, I.; Fernández, L.; Sánchez-Ramón, S.; Alba, C.; Zatarain, A.; Cañas, M.; López, O.N.; Olivares, D.; Rey, E.; Taxonera, C. Reliability Evaluation of Four Different Assays for Therapeutic Drug Monitoring of Infliximab Levels. Ther. Adv. Gastroenterol. 2018, 11, 1756284818783613. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ADALIMUMAB | ITRACK Drug Concentration | Total | |||
| Triturus drug concentration | <5 μg/mL | (5–8) μg/mL | >8 μg/mL | ||
| <5 μg/mL | 15 | 0 | 0 | 15 | |
| (5–8) μg/mL | 1 | 8 | 3 | 12 | |
| >8 μg/mL | 1 | 0 | 47 | 48 | |
| Total | 17 | 8 | 50 | 75 | |
| Kappa value: 0.87 (CI: 95%: 0.76–0.98) | |||||
| INFLIXIMAB | ITRACK drug concentration | Total | |||
| Triturus drug concentration | <3 μg/mL | (3–7) μg/mL | >7 μg/mL | ||
| <3 μg/mL | 2 | 0 | 0 | 2 | |
| (3–7) μg/mL | 0 | 7 | 0 | 7 | |
| >7 μg/mL | 0 | 1 | 7 | 8 | |
| Total | 2 | 8 | 7 | 17 | |
| Kappa value: 0.902 (CI: 95%: 0.715–1.089) | |||||
| USTEKINUMAB | ITRACK drug concentration | Total | |||
| Triturus drug concentration | <1 μg/mL | (1–4.5) μg/mL | >4.5 μg/mL | ||
| <1 μg/mL | 9 | 0 | 0 | 9 | |
| (1–4.5) μg/mL | 17 | 31 | 0 | 48 | |
| >4.5 μg/mL | 0 | 9 | 10 | 19 | |
| Total | 26 | 40 | 10 | 76 | |
| Kappa value: 0.424 (CI: 95%: 0.245–0.604) | |||||
| VEDOLIZUMAB | ITRACK drug concentration | Total | |||
| Triturus drug concentration | <25 μg/mL | >25 μg/mL | |||
| <25 μg/mL | 5 | 0 | 5 | ||
| >25 μg/mL | 2 | 3 | 5 | ||
| Total | 7 | 3 | 10 | ||
| Kappa value: 0.424 (CI: 95%: –0.072–0.920) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Pradeda, A.; Elberdín, L.; Porta-Sánchez, Á.; Outeda, M.; Diz-Lois Palomares, M.T.; Vázquez-Rey, T.; González-Conde, B.; Estévez-Prieto, E.; Gómez-Besteiro, M.I.; Martín-Herranz, I. Observational Study to Compare Biological Drug Concentration Quantification Techniques and Immunogenicity in Patients with Immune-Mediated Diseases. Biomedicines 2024, 12, 839. https://doi.org/10.3390/biomedicines12040839
Martínez-Pradeda A, Elberdín L, Porta-Sánchez Á, Outeda M, Diz-Lois Palomares MT, Vázquez-Rey T, González-Conde B, Estévez-Prieto E, Gómez-Besteiro MI, Martín-Herranz I. Observational Study to Compare Biological Drug Concentration Quantification Techniques and Immunogenicity in Patients with Immune-Mediated Diseases. Biomedicines. 2024; 12(4):839. https://doi.org/10.3390/biomedicines12040839
Chicago/Turabian StyleMartínez-Pradeda, Alejandro, Laida Elberdín, Ángeles Porta-Sánchez, María Outeda, Mª Teresa Diz-Lois Palomares, Teresa Vázquez-Rey, Benito González-Conde, Emilio Estévez-Prieto, María I. Gómez-Besteiro, and Isabel Martín-Herranz. 2024. "Observational Study to Compare Biological Drug Concentration Quantification Techniques and Immunogenicity in Patients with Immune-Mediated Diseases" Biomedicines 12, no. 4: 839. https://doi.org/10.3390/biomedicines12040839