
Validating Brain Tumor Reporting and Data System (BT-RADS) as a Diagnostic Tool for Glioma Follow-Up after Surgery
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Ethical Statement
2.2. Eligibility Criteria
2.3. Postoperative Clinical Assessment
2.4. MRI Examination
2.5. MRI Image Analysis
2.6. Reference Standards
2.7. Reader Acceptance
2.8. Statistical Analysis
3. Results
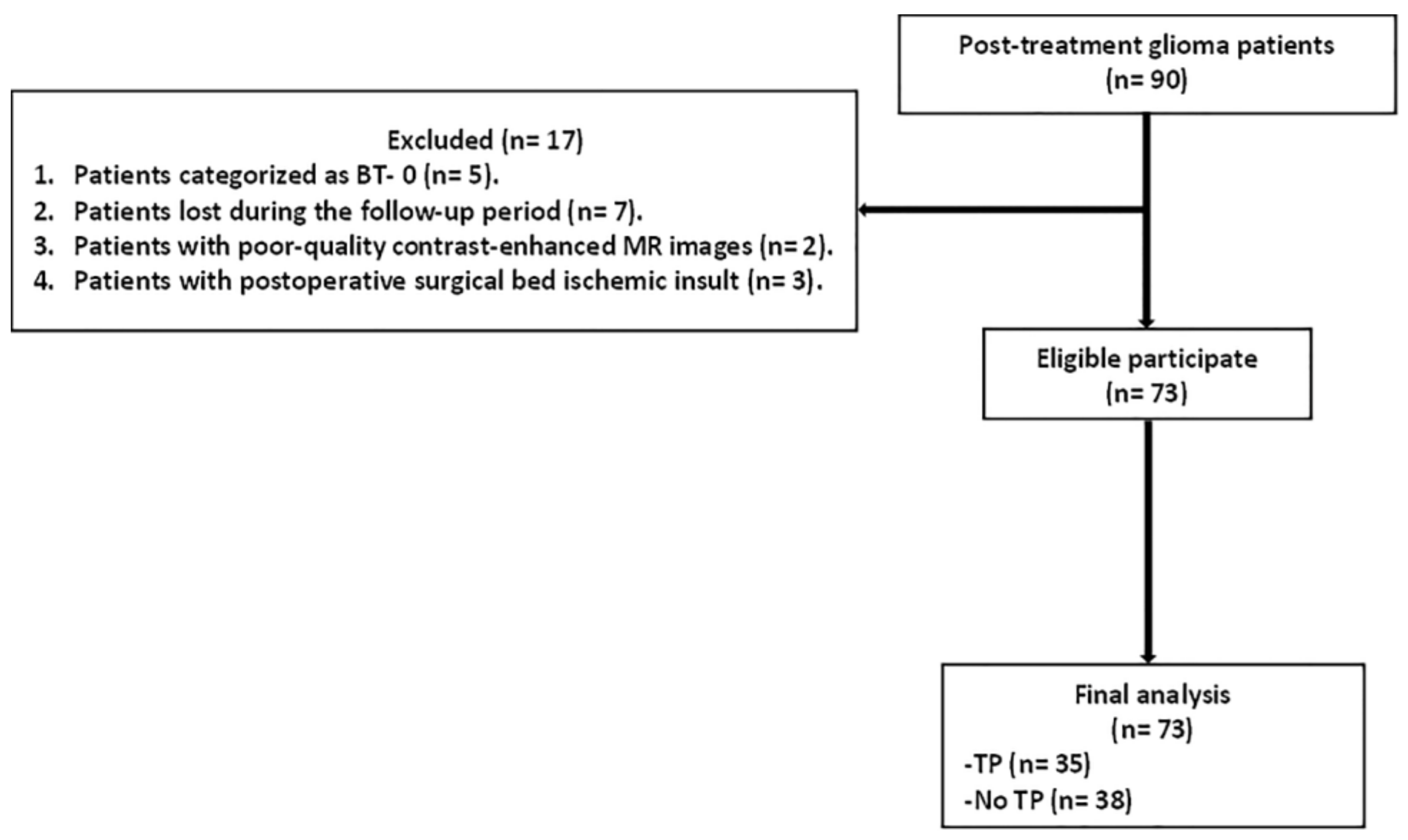
3.1. Patients and Glioma Characteristics
3.2. Distributions of BT-RADS Categories
3.3. Incidence of TP across BT-RADS Categories
3.4. Diagnostic Accuracy of BT-RADS
3.5. Inter-Reader Reliability of BT-RADS
3.6. Reader Acceptance of BT-RADS
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011–2015. Neuro Oncol. 2018, 20 (Suppl. S4), iv1–iv86. [Google Scholar] [CrossRef] [PubMed]
- Nieder, C.; Mehta, M.P.; Jalali, R. Combined radio- and chemotherapy of brain tumours in adult patients. Clin. Oncol. (R. Coll. Radiol.) 2009, 21, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.; Chang, S. Pediatric brain tumors: Current treatment strategies and future therapeutic approaches. Neurotherapeutics 2009, 6, 570–586. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Quant, E.C.; Wen, P.Y. Response assessment in neuro-oncology. Curr. Oncol. Rep. 2011, 13, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Parvez, K.; Parvez, A.; Zadeh, G. The diagnosis and treatment of pseudoprogression, radiation necrosis and brain tumor recurrence. Int. J. Mol. Sci. 2014, 15, 11832–11846. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.J.; Uitdehaag, B.M.; Barkhof, F.; Heimans, J.J.; Bitz-van der Zwan, A.E.; Gons, R.A.; van Waesberghe, J.H.; Polman, C.H. Interobserver variability in the radiological assessment of response to chemotherapy in glioma. Neurology 2003, 60, 826–830. [Google Scholar] [CrossRef] [PubMed]
- van den Bent, M.J.; Afra, D.; de Witte, O.; Ben Hassel, M.; Schraub, S.; Hoang-Xuan, K.; Malmström, P.O.; Hanzen, C.; Collette, L.; Piérart, M.; et al. Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: The EORTC 22845 randomised trial. Lancet 2005, 366, 985–990, Erratum in Lancet 2006, 367, 1818. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.Y.; Wen, P.Y. Response Assessment in Neuro-Oncology Criteria and Clinical Endpoints. Magn. Reson. Imaging Clin. N. Am. 2016, 24, 705–718. [Google Scholar] [CrossRef]
- Macdonald, D.R.; Cascino, T.L.; Schold, S.C., Jr.; Cairncross, J.G. Response criteria for phase II studies of supratentorial malignant glioma. J. Clin. Oncol. 1990, 8, 1277–1280. [Google Scholar] [CrossRef]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Rao, B.; Ikuta, I.; Mahajan, A.; Torskaya, V.; Patsalides, A.; Weinberg, B.D. Brain Tumor Reporting and Data System: A Pictorial Review. Neurographics 2021, 11, 175–185. [Google Scholar] [CrossRef]
- Weinberg, B.D. BT-RADS Brain Tumor Reporting & Data System. 2023. Available online: https://btrads.com/resources/ (accessed on 11 January 2023).
- Weinberg, B.D.; Gore, A.; Shu, H.G.; Olson, J.J.; Mu, Y.; Lindell, P.K.; Cogswell, P.M.; Wawrzynczak, C.J.; Johnson, J.D.; Wang, K.J.; et al. Management-Based Structured Reporting of Posttreatment Glioma Response with the Brain Tumor Reporting and Data System. J. Am. Coll. Radiol. 2018, 15, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Gore, A.; Hoch, M.J.; Shu, H.G.; Lindell, P.K.; Weinberg, B.D. Institutional Implementation of a Structured Reporting System: Our Experience with the Brain Tumor Reporting and Data System. Acad. Radiol. 2019, 26, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Y.; Weinberg, B.D.; Hu, R.; Gore, A.; Shu, H.G.; Olson, J.J.; Lindell, P.K.; Wawrzynczak, C.J.; Cogswell, P.M.; Wang, K.J.; et al. Quantitative Improvement in Brain Tumor MRI Through Structured Reporting (BT-RADS). Acad. Radiol. 2020, 27, 780–784. [Google Scholar] [CrossRef]
- Nayak, L.; DeAngelis, L.M.; Brandes, A.A.; Peereboom, D.M.; Galanis, E.; Lin, N.U.; Soffietti, R.; Short, S.C.; Deangelis, L.M.; Chamberlain, M.C.; et al. The Neurologic Assessment in Neuro-Oncology (NANO) scale: A tool to assess neurologic function for integration into the Response Assessment in Neuro-Oncology (RANO) criteria. Neuro Oncol. 2017, 19, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.; Blakeley, J.O.; Hong, X.; Yu, Y.; Zou, J.; Zhang, W.; Zhang, M.; van Zijl, P.C.; Mori, S.; Jiang, S.; et al. Applying amide proton transfer-weighted MRI to distinguish pseudoprogression from true progression in malignant gliomas. J. Magn. Reson. Imaging 2016, 44, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.K.; Jensen, R.L. Treatment-related brain tumor imaging changes: So-called “pseudoprogression” vs. tumor progression: Review and future research opportunities. Surg. Neurol. Int. 2013, 4 (Suppl. S3), S129–S135. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Martinez-Lage, M.; Sakai, Y.; Chawla, S.; Woo, D.C.V.; Alonso-Basanta, M.; Shadowitz, S.; Carralero, J.D.; Desai, A.; Prah, M.; et al. Differentiating Tumor Progression from Pseudoprogression in Patients with Glioblastomas Using Diffusion Tensor Imaging and Dynamic Susceptibility Contrast MRI. AJNR Am. J. Neuroradiol. 2016, 37, 28–36. [Google Scholar] [CrossRef]
- Kim, S.; Hoch, M.J.; Peng, L.; Shao, J.; Go, J.L.; Akers, A.; Moon, J.J.; Cha, Y.J.; Choi, S.W.; Ivanidze, J.; et al. A brain tumor reporting and data system to optimize imaging surveillance and prognostication in high-grade gliomas. J. Neuroimaging 2022, 32, 1185–1192. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, Y.; Wu, X.; Liu, J.; Lin, N.; Xu, Y.; Cheng, L.; Jiang, Y.; Wang, T.; Lv, X.; et al. Adding DSC PWI and DWI to BT-RADS can help identify postoperative recurrence in patients with high-grade gliomas. J. Neurooncol. 2020, 146, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Metwally, M.I.; Hafez, F.F.; Ibrahim, S.A.; Amin, D.H.; EL-Saied, W.E.F.F.; Amer, A.M. The value of adding DWI and FLAIR signal changes in the resection cavity on the diagnostic performance of BT-RADS category 3 for tumor progression prediction in post-treated glioma patients: A prospective pilot study. Egypt. J. Radiol. Nucl. Med. 2023, 54, 52. [Google Scholar] [CrossRef]
- van Dijken, B.R.J.; van Laar, P.J.; Holtman, G.A.; van der Hoorn, A. Diagnostic accuracy of magnetic resonance imaging techniques for treatment response evaluation in patients with high-grade glioma, a systematic review and meta-analysis. Eur Radiol. 2017, 27, 4129–4144. [Google Scholar] [CrossRef] [PubMed]
- Da Cruz, L.H.; Rodriguez, I.; Domingues, R.C.; Gasparetto, E.L.; Sorensen, A.G. Pseudoprogression and pseudoresponse: Imaging challenges in the assessment of posttreatment glioma. AJNR Am. J. Neuroradiol. 2011, 32, 1978–1985. [Google Scholar] [CrossRef] [PubMed]
- Delgado-López, P.D.; Riñones-Mena, E.; Corrales-García, E.M. Treatment-related changes in glioblastoma: A review on the controversies in response assessment criteria and the concepts of true progression, pseudoprogression, pseudoresponse and radionecrosis. Clin. Transl. Oncol. 2018, 20, 939–953. [Google Scholar] [CrossRef] [PubMed]
- Zikou, A.; Sioka, C.; Alexiou, G.A.; Fotopoulos, A.; Voulgaris, S.; Argyropoulou, M.I. Radiation Necrosis, Pseudoprogression, Pseudoresponse, and Tumor Recurrence: Imaging Challenges for the Evaluation of Treated Gliomas. Contrast Media Mol. Imaging 2018, 2018, 6828396. [Google Scholar] [CrossRef] [PubMed]
- Parillo, M.; Mallio, C.A.; Pileri, M.; Salicone, E.; Bandi, N.; Mazzanti, G.; Perocchio, F.; Rabni, M.; Viale, M.; Laino, M.; et al. Interrater reliability of Brain Tumor Reporting and Data System (BT-RADS) in the follow up of adult primary brain tumors: A single institution experience in Italy. Quant. Imaging Med. Surg. 2023, 13, 7423–7431. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.; Hoch, M.; Abidi, S.; Mathura, G.; Almero, J.; Nasr, K.; Pantel, P.; Reddy, V.; Naemi, A.; Davis, M. Brain tumor mri structured reporting allows calculation of interrater agreement of patients reviewed at tumor board. Neuro Oncol. 2019, 21 (Suppl. S6), vi163. [Google Scholar] [CrossRef]
- Wen, P.Y.; van den Bent, M.; Youssef, G.; Cloughesy, T.F.; Ellingson, B.M.; Weller, M.; Galanis, E.; Barboriak, D.P.; de Groot, J.; Gilbert, M.R.; et al. RANO 2.0: Update to the Response Assessment in Neuro-Oncology Criteria for High- and Low-Grade Gliomas in Adults. J. Clin. Oncol. 2023, 41, 5187–5199. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Description | Imaging Patterns | Management Recommendation |
|---|---|---|---|
| BT-RADS-0 | No score. | New baseline, incomplete study, or inability to categorize. | Continued follow-up, no change. |
| BT-RADS-1a | Improvement suspected due to a decrease in TP and/or treatment effects. Clinically stable or improved. | Reduction in enhancing component, FLAIR component, mass effect, or resolution of lesions compared with prior MRI. | Continued follow-up, no change. |
| BT-RADS-1b | Improvement potentially due to treatment effect. Clinically stable or improved. | Reduction in enhancing component, FLAIR component, mass effect, or resolution of lesions compared with prior MRI. | Continued follow-up, no change. |
| BT-RADS-2 | No significant change. Clinically stable. | No substantial change in enhancing component, FLAIR component, mass effect, or new lesions compared with prior MRI. | Continued follow-up, no change. |
| BT-RADS-3a | Worsening may represent the treatment effect. Clinically stable. | Mild increase (<25%) in enhancing component, FLAIR component, or mass effect compared with prior MRI. | Decreased time interval of follow-up. |
| BT-RADS-3b | Indeterminate. Worsening may be a mix of TP and treatment effects. Clinically stable. | Moderate increase in enhancing component, FLAIR component, mass effect, or new lesion compared with prior MRI. | Decreased time interval of follow-up. |
| BT-RADS-3c | Worsening favors TP. Clinically worsening. | Significant increase (>25%) in enhancing component, FLAIR component, mass effect, or definite new lesion compared with prior MRI. | Change in management vs. decreased time interval of follow-up. |
| BT-RADS-4 | Worsening, highly suspicious for TP. Clinically worsening. | Substantial increase in enhancing component, FLAIR component, mass effect, and/or multiple new lesions compared with prior MRI. | Change in management. |
| Characteristic | Value |
|---|---|
| Total No. of patients | 73 |
| Age, (years), mean ± SD (range) | 43.2 ± 12.9 (31–67) |
| Sex | |
| Male | 49 (67.1) |
| Female | 24 (32.9) |
| Total No. of MRI | 322 |
| Follow-up period (months), mean ± SD (range) | 15.3± 4.8 (8–25) |
| Mean interval to the first postoperative MRI scan (months), mean ± SD (range) | 4.3± 1.5 (1–10) |
| Mean interval between first and second postoperative MRI scan (months), mean ± SD (range) | 3.8± 0.9 (2–7) |
| Maximum tumor diameter (mm), mean ± SD (range) | 57.5 ± 17.8 (28–90) |
| Primary surgery | |
| Total resection | 60 (82.2) |
| Subtotal resection | 13 (17.8) |
| Tumor grade | |
| Grade III | 31 (42.5) |
| Grade IV | 42 (57.5) |
| Treatment | |
| Cortisone intake | 28 (38.4) |
| Radiotherapy | 73 (100) |
| Chemotherapy | 62 (84.9) |
| Methods of final diagnosis | |
| Repeat surgical resection | 27 (37) |
| Clinical/imaging follow-up | 46 (63) |
| Final diagnosis | |
| TP | 35 (47.9) |
| No TP | 38 (52.1) |
| Category | R 1 | R 2 | R 3 | R 4 | R 5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| TP | No TP | TP | No TP | TP | No TP | TP | No TP | TP | No TP | |
| 1a | 1 (2.9) | 6 (15.8) | 0 (0) | 8 (21.1) | 2 (5.7) | 9 (23.7) | 1 (2.9) | 8 (21.1) | 0 (0) | 10 (26.3) |
| 1b | 3 (8.6) | 9 (23.7) | 1 (2.9) | 8 (21.1) | 1 (2.9) | 8 (21.1) | 1 (2.9) | 10 (26.3) | 2 (5.7) | 9 (23.7) |
| 2 | 2 (5.7) | 12 (31.6) | 3 (8.6) | 9 (23.7) | 3 (8.6) | 9 (23.7) | 4 (11.4) | 9 (23.7) | 2 (5.7) | 11 (28.9) |
| 3a | 5 (14.3) | 7 (18.4) | 3 (8.6) | 8 (21.1) | 4 (2.9) | 6 (15.8) | 3 (8.6) | 8 (21.1) | 1 (2.9) | 3 (7.9) |
| 3b | 8 (22.9) | 1 (2.6) | 11 (31.4) | 4 (10.5) | 8 (22.9) | 5 (13.2) | 7 (20) | 1 (2.6) | 11 (31.4) | 3 (7.9) |
| 3c | 5 (14.3) | 2 (5.3) | 10 (28.6) | 1 (2.6) | 8 (22.9) | 1 (2.6) | 6 (17.1) | 2 (5.3) | 3 (8.6) | 1 (2.6) |
| 4 | 11 (31.4) | 1 (2.6) | 7 (20) | 0 (0) | 9 (25.7) | 0 (0) | 13 (37.1) | 0 (0) | 16 (45.7) | 1 (2.6) |
| Category | Sensitivity | Specificity |
|---|---|---|
| ≥BT-RADS-1a | 100 | 0.0 |
| >BT-RADS-1a | 94.3–100 | 15.8–26.3 |
| >BT-RADS-1b | 88.6–97.1 | 39.5–50.0 |
| >BT-RADS-2 | 68.6–88.6 | 65.8–79.0 |
| >BT-RADS-3a * | 68.6–85.7 | 84.2–92.1 |
| >BT-RADS-3b | 45.7–54.3 | 92.1–97.4 |
| >BT-RADS-3c | 17.1–45.7 | 94.7–97.4 |
| >BT-RADS-4 | 0.0 | 100.0 |
| Parameters | R 1 | R 2 | R 3 | R 4 | R 5 |
|---|---|---|---|---|---|
| Cutoff | >BT-RADS-3a | >BT-RADS-3a | >BT-RADS-3a | >BT-RADS-3a | >BT-RADS-3a |
| True-positive findings (n) | 24 | 28 | 25 | 26 | 30 |
| False-negative findings (n) | 11 | 7 | 10 | 9 | 5 |
| False-positive findings (n) | 4 | 5 | 6 | 3 | 5 |
| True-negative findings (n) | 34 | 33 | 32 | 35 | 33 |
| Accuracy (%) | 79.5 (58/73) [68.4–88.0] | 83.6 (61/73) [73.1–91.2] | 78.1 (57/73) [66.9–86.9] | 83.6 (61/73) [73.1–91.2] | 86.3 (63/73) [76.3–93.2] |
| Sensitivity (%) | 68.6 (24/35) [50.7–83.2] | 80.0 (28/35) [63.1–91.6] | 71.4 (25/35) [53.7–85.4] | 74.3 (26/35) [56.7–87.5] | 85.7 (30/35) [69.7–95.2] |
| Specificity (%) | 89.5 (34/38) [75.2–97.1] | 86.8 (33/38) [71.9–95.6] | 84.2 (32/38) [68.8–94.0] | 92.1 (35/38) [78.6–98.3] | 86.8 (33/38) [71.9–95.6] |
| Positive predictive value (%) | 85.7 (24/28) [69.8–94.0] | 84.8 (28/33) [70.8–92.8] | 80.6 (25/31) [66.0–89.9] | 89.7 (26/29) [74.2–96.3] | 85.7 (30/35) [72.4–93.2] |
| Negative predictive value (%) | 75.6 (34/45) [65.2–83.6] | 82.5 (33/40) [70.6–90.2] | 76.2 (32/42) [65.1–84.6] | 79.6 (35/44) [68.7–87.3] | 86.8 (33/38) [74.4–93.8] |
| Readers | Features | R 2 | R 3 | R 4 | R 5 | Overall |
|---|---|---|---|---|---|---|
| R 1 | Enhanced component | 0.28 (0.15–0.40) | 0.24 (0.07–0.42) | 0.29 (0.13–0.44) | 0.36 (0.23–0.50) | |
| FLAIR component | 0.60 (0.46–0.74) | 0.43 (0.27–0.60) | 0.56 (0.41–0.71) | 0.68 (0.56–0.80) | ||
| Mass effect | 0.62 (0.46–0.79) | 0.70 (0.55–0.84) | 0.64 (0.48–0.79) | 0.82 (0.70–0.95) | ||
| New lesion | 0.79 (0.59–0.99) | 1.00 (1.00–1.00) | 0.79 (0.51–1.00) | 1.00 (1.00–1.00) | ||
| BT-RADS | 0.57 (0.46–0.67) | 0.51 (0.38–0.64) | 0.54 (0.43–0.66) | 0.70 (0.58–0.81) | ||
| R 2 | Enhanced component | 0.33 (0.17–0.50) | 0.26 (0.08–0.44) | 0.65 (0.51–0.80) | ||
| FLAIR component | 0.59 (0.44–0.73) | 0.65 (0.51–0.80) | 0.69 (0.57–0.82) | |||
| Mass effect | 0.73 (0.58–0.88) | 0.79 (0.65–0.93) | 0.68 (0.52–0.84) | |||
| New lesion | 0.79 (0.59–0.99) | 0.65 (0.38–0.93) | 0.79 (0.59–0.99) | |||
| BT-RADS | 0.51 (0.41–0.62) | 0.60 (0.49–0.70) | 0.72 (0.63–0.80) | |||
| R 3 | Enhanced component | 0.28 (0.11–0.45) | 0.44 (0.29–0.59) | |||
| FLAIR component | 0.46 (0.29–0.63) | 0.57 (0.42–0.71) | ||||
| Mass effect | 0.71 (0.56–0.86) | 0.73 (0.58–0.87) | ||||
| New lesion | 0.79 (0.51–1.00) | 1.00 (1.00–1.00) | ||||
| BT-RADS | 0.54 (0.42–0.66) | 0.72 (0.62–0.81) | ||||
| R 4 | Enhanced component | 0.46 (0.29–0.63) | ||||
| FLAIR component | 0.67 (0.53–0.81) | |||||
| Mass effect | 0.63 (0.47–0.80) | |||||
| New lesion | 0.79 (0.51–1.00) | |||||
| BT-RADS | 0.73 (0.64–0.83) | |||||
| Overall | Enhanced component | 0.45 (0.34–0.56) | ||||
| FLAIR component | 0.67 (0.58–0.76) | |||||
| Mass effect | 0.69 (0.60–0.77) | |||||
| New lesion | 0.89 (0.86–0.93) | |||||
| BT-RADS | 0.75 (0.68–0.82) |
| Questions | Score |
|---|---|
| Reporting of post-treatment glioma imaging should follow a structured format | 24 |
| Radiology reports following BT-RADS clarify the significant findings | 17 |
| The structured reporting template of BT-RADS maintains the consistency of the reports | 24 |
| The application of BT-RADS constrains radiologists’ and clinicians’ communication | 23 |
| The application of BT-RADS enables a more understandable and concise report | 21 |
| Much training is required before the application of BT-RADS | 21 |
| BT-RADS is an easily applicable system by both junior and senior radiologists | 16 |
| The application of BT-RAD needs highly experienced radiologists | 21 |
| Reporting using BT-RADS helps trainee education | 20 |
| Using a structured reporting template of BT-RADS saves time for radiologists | 18 |
| BT-RADS promotes confidence in the final categorization of post-glioma imaging | 16 |
| BT-RADS enables the determination of appropriate management strategy | 19 |
| Some post-glioma imaging was difficult to interpret by BT-RADS | 22 |
| BT-RADS is equivalent to other ACR reporting systems, such as BI-RADS and LI-RADS | 14 |
| The current BT-RADS system is satisfied | 15 |
| BT-RADS needs further modification | 24 |
| The application of BT-RADS should be encouraged | 25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almalki, Y.E.; Basha, M.A.A.; Metwally, M.I.; Zeed, N.A.; Nada, M.G.; Alduraibi, S.K.; Morsy, A.A.; Balata, R.; Al Attar, A.Z.; Amer, M.M.; et al. Validating Brain Tumor Reporting and Data System (BT-RADS) as a Diagnostic Tool for Glioma Follow-Up after Surgery. Biomedicines 2024, 12, 887. https://doi.org/10.3390/biomedicines12040887
Almalki YE, Basha MAA, Metwally MI, Zeed NA, Nada MG, Alduraibi SK, Morsy AA, Balata R, Al Attar AZ, Amer MM, et al. Validating Brain Tumor Reporting and Data System (BT-RADS) as a Diagnostic Tool for Glioma Follow-Up after Surgery. Biomedicines. 2024; 12(4):887. https://doi.org/10.3390/biomedicines12040887
Chicago/Turabian StyleAlmalki, Yassir Edrees, Mohammad Abd Alkhalik Basha, Maha Ibrahim Metwally, Nesma Adel Zeed, Mohamad Gamal Nada, Sharifa Khalid Alduraibi, Ahmed A. Morsy, Rawda Balata, Ahmed Z. Al Attar, Mona M. Amer, and et al. 2024. "Validating Brain Tumor Reporting and Data System (BT-RADS) as a Diagnostic Tool for Glioma Follow-Up after Surgery" Biomedicines 12, no. 4: 887. https://doi.org/10.3390/biomedicines12040887