
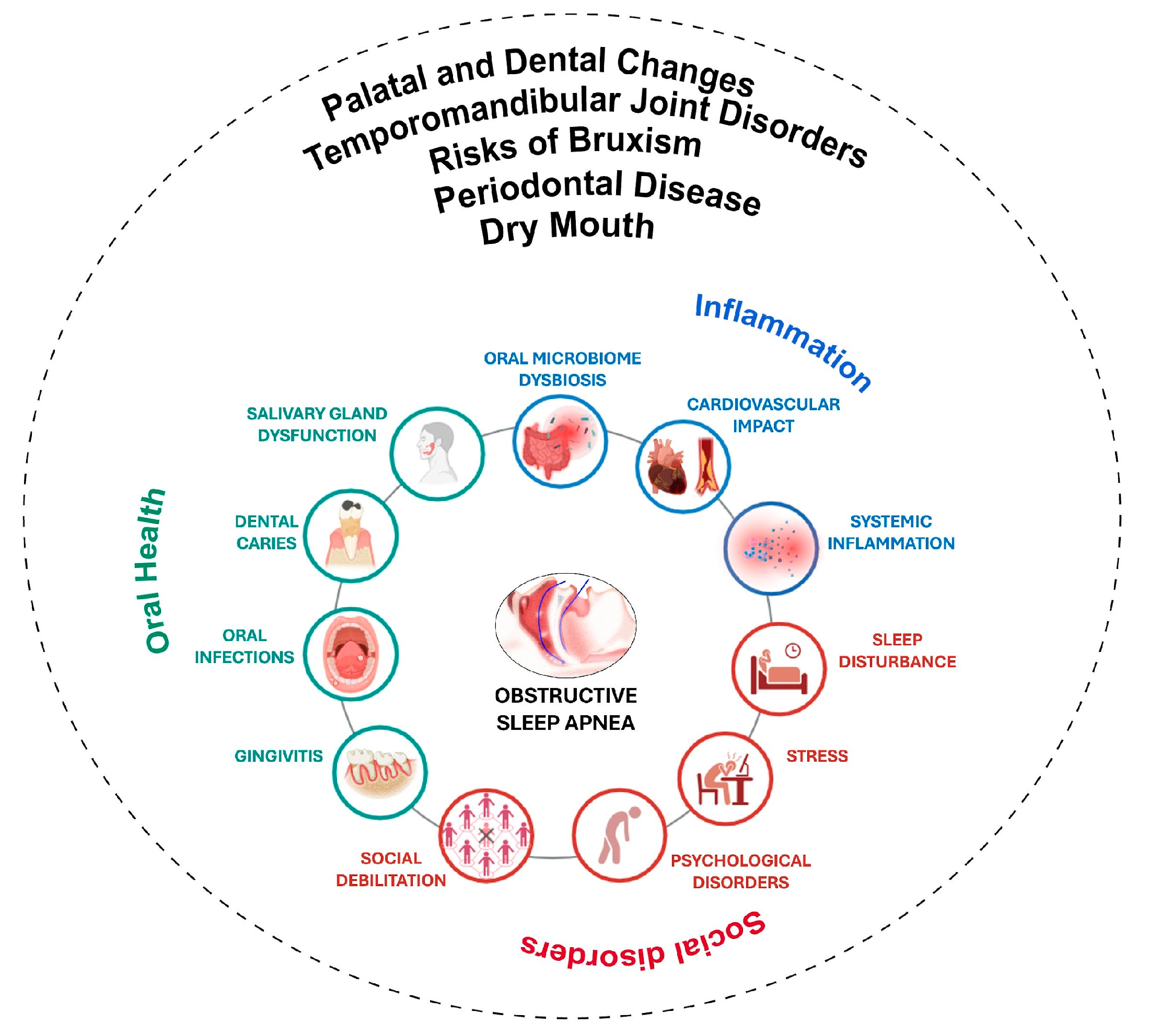
Oral Health Implications of Obstructive Sleep Apnea: A Literature Review

 ,
,  , ,
, ,  ,
,  , , , ,
, , , ,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Dry Mouth
3.2. Periodontal Disease
3.3. Risks of Bruxism
3.4. Temporomandibular Joint Disorders
3.5. Palatal and Dental Changes
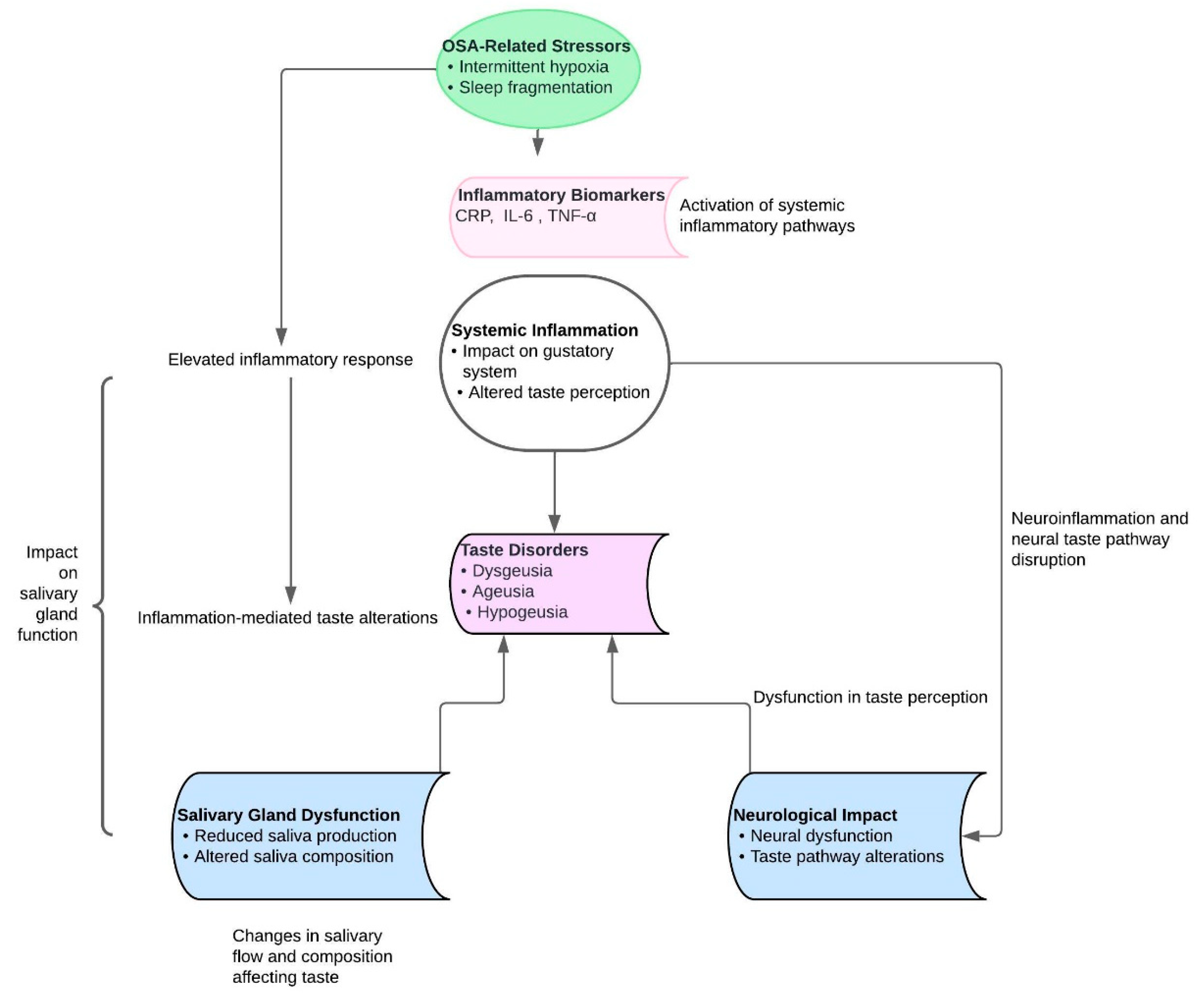
3.6. Taste Disorders
3.7. The Role of the Dentist in Addressing Obstructive Sleep Apnea
3.8. The Function of Maxillofacial Surgeons and Orthodontists
3.9. Oral Appliance Therapy and Dental Considerations, and Collaborative Approach
3.10. Risky Consequences of Untreated Obstructive Sleep Apnea Syndrome
3.11. Surgical and Conservative Methods of Treating Obstructive Sleep Apnea
4. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sampaio-Maia, B. The Oral Microbiome in Health and Its Implication in Oral and Systemic Diseases. Adv. Appl. Microbiol. 2016, 97, 171–210. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Li, Y.; Cao, Y.; Xue, J.; Zhou, X. The oral microbiome diversity and its relation to human diseases. Folia Microbiol. 2015, 60, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Kojima, Y.; Takayanagi, A.; Yoshino, K.; Ishizuka, Y.; Satou, R.; Takahashi, N.; Tazaki, M.; Kamijo, H.; Sugihara, N. Relationship between Obstructive Sleep Apnea and Self-assessed Oral Health Status: An Internet Survey. Bull. Tokyo Dent. Coll. 2016, 57, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Lévy, P.; Kohler, M.; McNicholas, W.T.; Barbé, F.; McEvoy, R.D.; Somers, V.K.; Lavie, L.; Pépin, J.L. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Primers 2015, 1, 15015. [Google Scholar] [CrossRef] [PubMed]
- Lv, R.; Liu, X.; Zhang, Y.; Dong, N.; Wang, X.; He, Y.; Yue, H.; Yin, Q. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct. Target. Ther. 2023, 8, 1–46. [Google Scholar] [CrossRef]
- Lee, J.J.; Sundar, K.M. Evaluation and Management of Adults with Obstructive Sleep Apnea Syndrome. Lung 2021, 199, 87–101. [Google Scholar] [CrossRef]
- Lopes, A.J.d.C.; Cunha, T.C.A.; Monteiro, M.C.M.; Serra-Negra, J.M.; Cabral, L.C.; Júnior, P.C.S. Is there an association between sleep bruxism and obstructive sleep apnea syndrome? A systematic review. Sleep Breath. 2020, 24, 913–921. [Google Scholar] [CrossRef]
- Ferreira, N.M.; Dos Santos, J.F.; dos Santos, M.B.; Marchini, L. Sleep bruxism associated with obstructive sleep apnea syndrome in children. Cranio 2015, 33, 251–255. [Google Scholar] [CrossRef]
- Alshahrani, A.A.; Alshadidi, A.A.F.; Alamri, M.A.A.; Alamri, A.A.A.; Alshehri, A.H.J.; Cicciù, M.; Isola, G.; Minervini, G. Prevalence of bruxism in obstructive sleep apnea syndrome (OSAS) patients: A systematic review conducted according to PRISMA guidelines and the Cochrane handbook for systematic reviews of interventions. J. Oral Rehabil. 2023, 50, 1362–1368. [Google Scholar] [CrossRef]
- Makeeva, I.M.; Budina, T.V.; Turkina, A.Y.; Poluektov, M.G.; Kondratiev, S.A.; Arakelyan, M.G.; Signore, A.; Amaroli, A. Xerostomia and hyposalivation in patients with obstructive sleep apnoea. Clin. Otolaryngol. 2021, 46, 782–787. [Google Scholar] [CrossRef]
- Apessos, I.; Andreadis, D.; Steiropoulos, P.; Tortopidis, D.; Angelis, L. Investigation of the relationship between sleep disorders and xerostomia. Clin. Oral Investig. 2020, 24, 1709–1716. [Google Scholar] [CrossRef]
- Molina, A.; Huck, O.; Herrera, D.; Montero, E. The association between respiratory diseases and periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2023, 50, 842–887. [Google Scholar] [CrossRef]
- Lembo, D.; Caroccia, F.; Lopes, C.; Moscagiuri, F.; Sinjari, B.; D’Attilio, M. Obstructive Sleep Apnea and Periodontal Disease: A Systematic Review. Medicina 2021, 57, 640. [Google Scholar] [CrossRef]
- Manfredini, D.; Thomas, D.C.; Lobbezoo, F. Temporomandibular Disorders Within the Context of Sleep Disorders. Dent. Clin. N. Am. 2023, 67, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Singhal, P.; Gupta, R.; Sharma, R.; Mishra, P. Association of naso-oro-pharyngeal structures with the sleep architecture in suspected obstructive sleep apnea. Indian J. Otolaryngol. Head Neck Surg. 2014, 66 (Suppl. 1), 81–87. [Google Scholar] [CrossRef]
- Zhao, T.; Ngan, P.; Hua, F.; Zheng, J.; Zhou, S.; Zhang, M.; Xiong, H.; He, H. Impact of pediatric obstructive sleep apnea on the development of Class II hyperdivergent patients receiving orthodontic treatment: A pilot study. Angle Orthod. 2018, 88, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Triplett, W.W.; Lund, B.A.; Westbrook, P.R.; Olsen, K.D. Obstructive sleep apnea syndrome in patients with class II malocclusion. Mayo Clin. Proc. 1989, 64, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Nabiev, F.K.; Dobrodeev, A.S.; Libin, P.V.; Kotov, I.I. Diagnostics and treatment of patients with II class malocclusion associated with obstructive sleep apnea syndrome. Stomatologiia 2014, 93, 74–77. (In Russian) [Google Scholar] [CrossRef]
- Neelapu, B.C.; Kharbanda, O.P.; Sardana, H.K.; Balachandran, R.; Sardana, V.; Kapoor, P.; Gupta, A.; Vasamsetti, S. Craniofacial and upper airway morphology in adult obstructive sleep apnea patients: A systematic review and meta-analysis of cephalometric studies. Sleep Med. Rev. 2017, 31, 79–90. [Google Scholar] [CrossRef]
- Kang, J.H.; Kim, H.J.; Song, S.I. Obstructive sleep apnea and anatomical structures of the nasomaxillary complex in adolescents. PLoS ONE 2022, 17, e0272262. [Google Scholar] [CrossRef]
- Tranfić Duplančić, M.; Pecotić, R.; Lušić Kalcina, L.; Pavlinac Dodig, I.; Valić, M.; Roguljić, M.; Rogić, D.; Lapić, I.; Grdiša, K.; Peroš, K.; et al. Salivary parameters and periodontal inflammation in obstructive sleep apnoea patients. Sci. Rep. 2022, 12, 19387. [Google Scholar] [CrossRef]
- Pico-Orozco, J.; Carrasco-Llatas, M.; Silvestre, F.J.; Silvestre-Rangil, J. Xerostomia in patients with sleep apnea-hypopnea syndrome: A prospective case-control study. J. Clin. Exp. Dent. 2020, 12, e708–e712. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhou, N.; Chattrattrai, T.; van Selms, M.K.A.; de Vries, R.; Hilgevoord, A.A.J.; de Vries, N.; Aarab, G.; Lobbezoo, F. Associations between snoring and dental sleep conditions: A systematic review. J. Oral Rehabil. 2023, 50, 416–428. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhou, N.; Lobbezoo, F.; Almeida, F.R.; Cistulli, P.A.; Dieltjens, M.; Huynh, N.T.; Kato, T.; Lavigne, G.J.; Masse, J.F.; et al. Dental sleep-related conditions and the role of oral healthcare providers: A scoping review. Sleep Med. Rev. 2023, 67, 101721. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Shen, Y.; Liping, F.; Ma, J.; Wang, G.F. The role of dry mouth in screening sleep apnea. Postgrad. Med. J. 2021, 97, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Tanasiewicz, M.; Hildebrandt, T.; Obersztyn, I. Xerostomia of Various Etiologies: A Review of the Literature. Adv. Clin. Exp. Med. 2016, 25, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Millsop, J.W.; Wang, E.A.; Fazel, N. Etiology, evaluation, and management of xerostomia. Clin. Dermatol. 2017, 35, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Guggenheimer, J.; Moore, P.A. Xerostomia: Etiology, recognition and treatment. J. Am. Dent. Assoc. 2003, 134, 61–69; quiz 118–119. [Google Scholar] [CrossRef] [PubMed]
- Melvin, J.E. Saliva and dental diseases. Curr. Opin. Dent. 1991, 1, 795–801. [Google Scholar]
- Farnaud, S.J.; Kosti, O.; Getting, S.J.; Renshaw, D. Saliva: Physiology and diagnostic potential in health and disease. Sci. World J. 2010, 10, 434–456. [Google Scholar] [CrossRef]
- Kaplan, M.D.; Baum, B.J. The functions of saliva. Dysphagia 1993, 8, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Edgar, W.M. Saliva: Its secretion, composition and functions. Br. Dent. J. 1992, 172, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Téllez-Corral, M.A.; Herrera-Daza, E.; Cuervo-Jimenez, H.K.; Arango-Jimenez, N.; Morales-Vera, D.Z.; Velosa-Porras, J.; Latorre-Uriza, C.; Escobar-Arregoces, F.M.; Hidalgo-Martinez, P.; Cortés, M.E.; et al. Patients with obstructive sleep apnea can favor the predisposing factors of periodontitis by the presence of P. melaninogenica and C. albicans, increasing the severity of the periodontal disease. Front. Cell. Infect. Microbiol. 2022, 12, 934298. [Google Scholar] [CrossRef] [PubMed]
- Téllez Corral, M.A.; Daza, E.H.; Jimenez, N.A.; Morales Vera, D.Z.; Velosa Porras, J.; Latorre Uriza, C.; Escobar Arregoces, F.M.; Martinez, P.H.; Cortés, M.E.; Otero, L.; et al. Biomarkers for the severity of periodontal disease in patients with obstructive sleep apnea:IL-1 β, IL-6, IL-17A, and IL-33. Heliyon 2023, 9, e14340. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, J.; Fu, R.; Liu, J.; Wen, X.; Zhang, L. Halitosis: Etiology, prevention, and the role of microbiota. Clin. Oral Investig. 2023, 27, 6383–6393. [Google Scholar] [CrossRef] [PubMed]
- Edgar, W.M.; Higham, S.M.; Manning, R.H. Saliva stimulation and caries prevention. Adv. Dent. Res. 1994, 8, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Wick, J.Y. Xerostomia: Causes and treatment. Consult. Pharm. 2007, 22, 985–992. [Google Scholar] [CrossRef] [PubMed]
- van der Reijden, W.A.; Veerman, E.C.; van Nieuw Amerongen, A. Speeksel en speekselsubstituten [Saliva and saliva substitutes]. Ned. Tijdschr. Tandheelkd. 1993, 100, 351–354. (In Dutch) [Google Scholar] [PubMed]
- Shimazaki, Y.; Fu, B.; Yonemoto, K.; Akifusa, S.; Shibata, Y.; Takeshita, T.; Ninomiya, T.; Kiyohara, Y.; Yamashita, Y. Stimulated salivary flow rate and oral health status. J. Oral Sci. 2017, 59, 55–62. [Google Scholar] [CrossRef]
- Ahmad, N.E.; Sanders, A.E.; Sheats, R.; Brame, J.L.; Essick, G.K. Obstructive sleep apnea in association with periodontitis: A case-control study. J. Dent. Hyg. 2013, 87, 188–199. [Google Scholar]
- Chen, Y.; Metz, J.E.; Gao, H.; Gao, X. Association between obstructive sleep apnea and periodontitis in Chinese male adults: A cross-sectional study. J. Prosthet. Dent. 2023, 130, 80–86. [Google Scholar] [CrossRef]
- Keller, J.J.; Wu, C.S.; Chen, Y.H.; Lin, H.C. Association between obstructive sleep apnoea and chronic periodontitis: A population-based study. J. Clin. Periodontol. 2013, 40, 111–117. [Google Scholar] [CrossRef]
- Nizam, N.; Basoglu, O.K.; Tasbakan, M.S.; Holthöfer, A.; Tervahartiala, T.; Sorsa, T.; Buduneli, N. Do salivary and serum collagenases have a role in an association between obstructive sleep apnea syndrome and periodontal disease? A preliminary case-control study. Arch. Oral Biol. 2015, 60, 134–143. [Google Scholar] [CrossRef]
- Trombone, A.P.F.; Cardoso, C.R.; Repeke, C.E.; Ferreira, S.B., Jr.; Martins, W., Jr.; Campanelli, A.P.; Avila-Campos, M.J.; Trevilatto, P.C.; Silva, J.S.; Garlet, G.P. Tumor necrosis factor-α-308G/A single nucleotide polymorphism and red-complex periodontopathogens are independently associated with increased levels of tumor necrosis factor-alpha in diseased periodontal tissues. J. Periodontal Res. 2009, 44, 598–608. [Google Scholar] [CrossRef]
- Latorre, C.; Escobar, F.; Velosa, J.; Rubiano, D.; Hidalgo-Martinez, P.; Otero, L. Association between obstructive sleep apnea and comorbidities with periodontal disease in adults. J. Indian Soc. Periodontol. 2018, 22, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Arango Jimenez, N.; Morales Vera, D.Z.; Latorre Uriza, C.; Velosa-Porras, J.; Téllez Corral, M.A.; Escobar Arregocés, F.M. Relationship of obstructive sleep apnea with periodontal condition and its local and systemic risk factors. Clin. Oral Investig. 2023, 27, 2823–2832. [Google Scholar] [CrossRef]
- Li, D.; Kuang, B.; Lobbezoo, F.; de Vries, N.; Hilgevoord, A.; Aarab, G. Sleep bruxism is highly prevalent in adults with obstructive sleep apnea: A large-scale polysomnographic study. J. Clin. Sleep Med. 2023, 19, 443–451. [Google Scholar] [CrossRef]
- Wali, S.O.; Abalkhail, B.; Krayem, A. Prevalence and risk factors of obstructive sleep apnea syndrome in a Saudi Arabian population. Ann. Thorac. Med. 2017, 12, 88–94. [Google Scholar] [CrossRef]
- Alqahtani, N.D.; Algowaifly, M.I.; Almehizia, F.A.; Alraddadi, Z.A.; Al-Sehaibany, F.S.; Almosa, N.A.; Albarakati, S.F.; Bahammam, A.S. The characteristics of dental occlusion in patients with moderate to severe obstructive sleep apnea in Saudi Arabia. Saudi Med. J. 2018, 39, 928–934. [Google Scholar] [CrossRef] [PubMed]
- Martynowicz, H.; Gac, P.; Brzecka, A.; Poreba, R.; Wojakowska, A.; Mazur, G.; Smardz, J.; Wieckiewicz, M. The Relationship between Sleep Bruxism and Obstructive Sleep Apnea Based on Polysomnographic Findings. J. Clin. Med. 2019, 8, 1653. [Google Scholar] [CrossRef] [PubMed]
- Inana, R.; Benbir, G.; Karadeniz, D.; Yavlal, F.; Kiziltanb, M.E. Sleep bruxism is related to decreased inhibitory control of trigeminal motoneurons, but not with reticulobulbar system. Neurol. Sci. 2017, 38, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Han, K.; Lee, S.Y. Associations between obstructive sleep apnea and dental pain and chewing discomfort in Korean adults: A nationwide cross-sectional study. Sci. Rep. 2023, 13, 12768. [Google Scholar] [CrossRef] [PubMed]
- Ning, R.; Chen, J.; Lu, Y.; Guo, J. Obstructive sleep apnea: A follow-up program in its relation to temporomandibular joint disorder, sleep bruxism and orofacial pain. BMC Oral Health 2023, 23, 578. [Google Scholar] [CrossRef] [PubMed]
- Klasser, G.D.; Rei, N.; Lavigne, G.J. Sleep bruxism etiology: The evolution of a changing paradigm. J. Can. Dent. Assoc. 2015, 81, f2. [Google Scholar] [PubMed]
- Ciavarella, D.; Campobasso, A.; Conte, E.; Burlon, G.; Guida, L.; Montaruli, G.; Cassano, M.; Laurenziello, M.; Illuzzi, G.; Tepedino, M. Correlation between dental arch form and OSA severity in adult patients: An observational study. Prog. Orthod. 2023, 24, 19. [Google Scholar] [CrossRef] [PubMed]
- Magliulo, G.; De Vincentiis, M.; Iannella, G.; Ciofalo, A.; Pasquariello, B.; Manno, A.; Angeletti, D.; Polimeni, A. Olfactory evaluation in obstructive sleep apnoea patients. ACTA Otorhinolaryngol. Ital. 2018, 38, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Yenigun, A.; Degirmenci, N.; Goktas, S.S.; Dogan, R.; Ozturan, O. Investigation of smell and taste function in patients with obstructive sleep apnoea syndrome. J. Laryngol. Otol. 2019, 133, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Fang, F.; Zhan, X.; Yao, L.; Wei, Y. The impact of obstructive apnea sleep syndrome on chemical function. Sleep Breath. 2020, 24, 1549–1555. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, E.; Segù, M.; Toffoli, A.; Razzini, G.; Macaluso, G.M.; Manfredi, E. Relationship between periodontal disease and obstructive sleep apnea in adults: A systematic review. Dent. Res. J. 2024, 21, 15. [Google Scholar] [CrossRef]
- Loke, W.; Girvan, T.; Ingmundson, P.; Verrett, R.; Schoolfield, J.; Mealey, B.L. Investigating the association between obstructive sleep apnea and periodontitis. J. Periodontol. 2015, 86, 232–243. [Google Scholar] [CrossRef]
- Kim, S.R.; Son, M.; Kim, Y.R. Risk of chronic periodontitis in patients with obstructive sleep apnea in Korea: A nationwide retrospective cohort study. Epidemiol. Health 2023, 45, e2023032. [Google Scholar] [CrossRef] [PubMed]
- Takedachi, M.; Shimabukuro, Y.; Sawada, K.; Koshimizu, M.; Shinada, K.; Asai, H.; Mizoguchi, A.; Hayashi, Y.; Tsukamoto, A.; Miyago, M.; et al. Evaluation of periodontitis-related tooth loss according to the new 2018 classification of periodontitis. Sci. Rep. 2022, 12, 11893. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Sanz, M.; Shapira, L.; Brotons, C.; Chapple, I.; Frese, T.; Graziani, F.; Hobbs, F.D.R.; Huck, O.; Hummers, E.; et al. Association between periodontal diseases and cardiovascular diseases, diabetes and respiratory diseases: Consensus report of the Joint Workshop by the European Federation of Periodontology (EFP) and the European arm of the World Organization of Family Doctors (WONCA Europe). J. Clin. Periodontol. 2023, 50, 819–841. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, C.; Watt, R.; Hamer, M. Toothbrushing, inflammation, and risk of cardiovascular disease: Results from Scottish Health Survey. BMJ 2010, 34, c2451. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Sanz, M.; Shapira, L.; Brotons, C.; Chapple, I.; Frese, T.; Graziani, F.; Hobbs, F.D.R.; Huck, O.; Hummers, E.; et al. Periodontal diseases and cardiovascular diseases, diabetes, and respiratory diseases: Summary of the consensus report by the European Federation of Periodontology and WONCA Europe. Eur. J. Gen. Pract. 2024, 30, 2320120. [Google Scholar] [CrossRef] [PubMed]
- Yonel, Z.; Sharma, P. The Role of the Dental Team in the Prevention of Systemic Disease: The Importance of Considering Oral Health As Part of Overall Health. Prim. Dent. J. 2017, 6, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Berggren, K.; Broström, A.; Firestone, A.; Wright, B.; Josefsson, E.; Lindmark, U. Oral health problems linked to obstructive sleep apnea are not always recognized within dental care-As described by dental professionals. Clin. Exp. Dent. Res. 2022, 8, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Schames, S.E.; Schames, J.; Schames, M.; Chagall-Gungur, S.S. Sleep bruxism, an autonomic self-regulating response by triggering the trigeminal cardiac reflex. J. Calif. Dent. Assoc. 2012, 40, 670–676. [Google Scholar] [CrossRef] [PubMed]
- González González, A.; Montero, J.; Gómez Polo, C. Sleep Apnea-Hypopnea Syndrome and Sleep Bruxism: A Systematic Review. J. Clin. Med. 2023, 12, 910. [Google Scholar] [CrossRef]
- Palmer, J.; Durham, J. Temporomandibular disorders. BJA Educ. 2021, 21, 44–50. [Google Scholar] [CrossRef]
- Magalhães, B.G.; Freitas, J.L.d.M.; Barbosa, A.C.d.S.; Gueiros, M.C.S.N.; Gomes, S.G.F.; Rosenblatt, A.; Júnior, A.d.F.C. Temporomandibular disorder: Otologic implications and its relationship to sleep bruxism. Braz. J. Otorhinolaryngol. 2018, 84, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Durán-Cantolla, J.; Alkhraisat, M.H.; Martínez-Null, C.; Aguirre, J.J.; Guinea, E.R.; Anitua, E. Frequency of obstructive sleep apnea syndrome in dental patients with tooth wear. J. Clin. Sleep Med. 2015, 11, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Alessandri-Bonetti, A.; Bortolotti, F.; Moreno-Hay, I.; Michelotti, A.; Cordaro, M.; Alessandri-Bonetti, G.; Okeson, J.P. Effects of mandibular advancement device for obstructive sleep apnea on temporomandibular disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 48, 101211. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, M.L.; Bortolotti, F.; Pelligra, I.; Stipa, C.; Sorrenti, G.; Incerti-Parenti, S.; Alessandri-Bonetti, G. Prevalence of temporomandibular disorders in adult obstructive sleep apnoea patients: A cross-sectional controlled study. J. Oral Rehabil. 2023, 50, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.E.; Quinnell, T. Mandibular Advancement Devices for OSA: An Alternative to CPAP? Pulm. Ther. 2021, 7, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Langaliya, A.; Alam, M.K.; Hegde, U.; Panakaje, M.S.; Cervino, G.; Minervini, G. Occurrence of Temporomandibular Disorders among patients undergoing treatment for Obstructive Sleep Apnoea Syndrome (OSAS) using Mandibular Advancement Device (MAD): A Systematic Review conducted according to PRISMA guidelines and the Cochrane handbook for systematic reviews of interventions. J. Oral Rehabil. 2023, 50, 1554–1563. [Google Scholar] [CrossRef] [PubMed]
- Gil-Martínez, A.; Paris-Alemany, A.; López-de-Uralde-Villanueva, I.; La Touche, R. Management of pain in patients with temporomandibular disorder (TMD): Challenges and solutions. J. Pain Res. 2018, 11, 571–587. [Google Scholar] [CrossRef]
- Sutherland, K.; Cistulli, P.A. Oral Appliance Therapy for Obstructive Sleep Apnoea: State of the Art. J. Clin. Med. 2019, 8, 2121. [Google Scholar] [CrossRef]
- Kecik, D. Three-dimensional analyses of palatal morphology and its relation to upper airway area in obstructive sleep apnea. Angle Orthod. 2017, 87, 300–306. [Google Scholar] [CrossRef]
- Bajrovic, N.; Nakas, E.; Dzemidzic, V.; Tiro, A. The Link Between Obstructive Sleep Apnea and Orthodontic Anomalies in Obese Adult Population. Mater Sociomed. 2021, 33, 65–69. [Google Scholar] [CrossRef]
- Ishida, E.; Kunimatsu, R.; Medina, C.C.; Iwai, K.; Miura, S.; Tsuka, Y.; Tanimoto, K. Dental and Occlusal Changes during Mandibular Advancement Device Therapy in Japanese Patients with Obstructive Sleep Apnea: Four Years Follow-Up. J. Clin. Med. 2022, 11, 7539. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatric Dentistry. Management of the Developing Dentition and Occlusion in Pediatric Dentistry. Pediatr. Dent. 2017, 39, 334–347. [Google Scholar]
- Manrikyan, G.E.; Vardanyan, I.F.; Markaryan, M.M.; Manrikyan, M.E.; Badeyan, E.H.; Manukyan, A.H.; Gevorgyan, M.A.; Khachatryan, S.G. Association between the Obstructive Sleep Apnea and Cephalometric Parameters in Teenagers. J. Clin. Med. 2023, 12, 6851. [Google Scholar] [CrossRef] [PubMed]
- Lavalle, S.; Masiello, E.; Iannella, G.; Magliulo, G.; Pace, A.; Lechien, J.R.; Calvo-Henriquez, C.; Cocuzza, S.; Parisi, F.M.; Favier, V.; et al. Unraveling the Complexities of Oxidative Stress and Inflammation Biomarkers in Obstructive Sleep Apnea Syndrome: A Comprehensive Review. Life 2024, 14, 425. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, H.; Almeida, F.R.; Tsuda, T.; Moritsuchi, Y.; Lowe, A.A. Craniofacial changes after 2 years of nasal continuous positive airway pressure use in patients with obstructive sleep apnea. Chest 2010, 138, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Ghadiri, M.; Grunstein, R.R. Clinical side effects of continuous positive airway pressure in patients with obstructive sleep apnoea. Respirology 2020, 25, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Johal, A.; Hamoda, M.M.; Almeida, F.R.; Marklund, M.; Tallamraju, H. The role of oral appliance therapy in obstructive sleep apnoea. Eur. Respir. Rev. 2023, 32, 220257. [Google Scholar] [CrossRef] [PubMed]
- Fagundes, N.C.F.; Perez-Garcia, A.; Graf, D.; Flores-Mir, C.; Heo, G. Orthodontic interventions as a management option for children with residual obstructive sleep apnea: A cohort study protocol. BMJ Open. 2022, 12, e061651. [Google Scholar] [CrossRef] [PubMed]
- Sforza, E.; Roche, F. Chronic intermittent hypoxia and obstructive sleep apnea: An experimental and clinical approach. Hypoxia 2016, 4, 99–108. [Google Scholar] [CrossRef]
- Binar, M.; Gokgoz, M.C. Olfactory function in patients with obstructive sleep apnea and the effect of positive airway pressure treatment: A systematic review and meta-analysis. Sleep Breath. 2021, 25, 1791–1802. [Google Scholar] [CrossRef]
- Sahib, A.; Roy, B.; Kang, D.; Aysola, R.S.; Wen, E.; Kumar, R. Relationships between brain tissue damage, oxygen desaturation, and disease severity in obstructive sleep apnea evaluated by diffusion tensor imaging. J. Clin. Sleep Med. 2022, 18, 2713–2721, Erratum in J. Clin. Sleep Med. 2023, 19, 1167. [Google Scholar] [CrossRef]
- Lin, H.C.; Hwang, M.S.; Liao, C.C.; Friedman, M. Taste disturbance following tongue base resection for OSA. Laryngoscope 2016, 126, 1009–1013. [Google Scholar] [CrossRef] [PubMed]
- Uchida, H.; Ovitt, C.E. Novel impacts of saliva with regard to oral health. J. Prosthet. Dent. 2022, 127, 383–391. [Google Scholar] [CrossRef]
- Müller, F.; Chebib, N.; Maniewicz, S.; Genton, L. The Impact of Xerostomia on Food Choices—A Review with Clinical Recommendations. J. Clin. Med. 2023, 12, 4592. [Google Scholar] [CrossRef] [PubMed]
- Invitto, S.; Calcagnì, A.; Piraino, G.; Ciccarese, V.; Balconi, M.; De Tommaso, M.; Toraldo, D.M. Obstructive sleep apnea syndrome and olfactory perception: An OERP study. Respir. Physiol. Neurobiol. 2019, 259, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Boerner, B.; Tini, G.M.; Fachinger, P.; Graber, S.M.; Irani, S. Significant improvement of olfactory performance in sleep apnea patients after three months of nasal CPAP therapy—Observational study and randomized trial. PLoS ONE 2017, 12, e0171087. [Google Scholar] [CrossRef]
- Wallace, E.S.; Carberry, J.C.; Toson, B.; Eckert, D.J. A systematic review and meta-analysis of upper airway sensation in obstructive sleep apnea—Implications for pathogenesis, treatment and future research directions. Sleep Med. Rev. 2022, 62, 101589. [Google Scholar] [CrossRef] [PubMed]
- Walliczek-Dworschak, U.; Cassel, W.; Mittendorf, L.; Pellegrino, R.; Koehler, U.; Güldner, C.; Dworschak, P.O.G.; Hildebrandt, O.; Daniel, H.; Günzel, T.; et al. Continuous positive air pressure improves orthonasal olfactory function of patients with obstructive sleep apnea. Sleep Med. 2017, 34, 24–29. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Ahlberg, J.; Manfredini, D.; Winocur, E. Are bruxism and the bite causally related? J. Oral Rehabil. 2012, 39, 489–501. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Aarab, G. Increasing the visibility of dental sleep medicine. Sleep Med. Clin. 2019, 14, 155–156. [Google Scholar]
- Koyano, K.; Tsukiyama, Y.; Ichiki, R.; Kuwata, T. Assessment of bruxism in the clinic. J. Oral Rehabil. 2008, 35, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Ruangsri, S.; Jorns, T.P.; Puasiri, S.; Luecha, T.; Chaithap, C.; Sawanyawisuth, K. Which oropharyngeal factors are significant risk factors for obstructive sleep apnea? An age-matched study and dentist perspectives. Nat. Sci. Sleep 2016, 8, 215–219. [Google Scholar] [PubMed]
- Al-Jewair, T.S.; Al-Jasser, R.; Almas, K. Periodontitis and obstructive sleep apnea’s bidirectional relationship: A systematic review and meta-analysis. Sleep Breath. 2015, 19, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Jonas, D.E.; Amick, H.R.; Feltner, C.; Weber, R.P.; Arvanitis, M.; Stine, A.; Lux, L.; Middleton, J.C.; Voisin, C.; Harris, R.P. Screening for Obstructive Sleep Apnea in Adults: An Evidence Review for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2017. [Google Scholar]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar] [PubMed]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 11, 773–827. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, K.; Vanderveken, O.M.; Tsuda, H.; Marklund, M.; Gagnadoux, F.; Kushida, C.A.; Cistulli, P.A. Oral appliance treatment for obstructive sleep apnea: An update. J. Clin. Sleep Med. 2014, 10, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Benoist, L.; de Ruiter, M.; de Lange, J.; de Vries, N. A randomized, controlled trial of positional therapy versus oral appliance therapy for position-dependent sleep apnea. Sleep Med. 2017, 34, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Marklund, M. Update on oral appliance therapy for OSA. Curr. Sleep Med. Rep. 2017, 3, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Sheats, R.D.; Schell, T.G.; Blanton, A.O.; Braga, P.M.; Demko, B.G.; Dort, L.C.; Farquhar, D.; Katz, S.G.; Masse, J.-F.; Rogers, R.R.; et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J. Dent. Sleep Med. 2017, 4, 111–125. [Google Scholar] [CrossRef]
- Marchetti, E.; Petro, E.; Gaggioli, F.; Lardani, L.; Mancini, L.; Marzo, G. The dentist’s role in diagnosis and treatment of obstructive sleep apnea syndrome: A literature review. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 1), 173–180. [Google Scholar]
- Levendowski, D.J.; Morgan, T.; Westbrook, P. Initial evaluation of a titration appliance for temporary treatment of obstructive sleep apnea. J. Sleep Disord. Ther. 2012, 1, 101. [Google Scholar] [CrossRef] [PubMed]
- Padma, A.; Ramakrishnan, N.; Narayanan, V. Management of obstructive sleep apnea: A dental perspective. Indian J. Dent. Res. 2007, 18, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Conley, R.S. Evidence for dental and dental specialty treatment of obstructive sleep apnoea. Part 1: The adult OSA patient and Part 2: The paediatric and adolescent patient. J. Oral Rehabil. 2011, 38, 136–156. [Google Scholar] [CrossRef] [PubMed]
- Zucconi, M.; Caprioglio, A.; Calori, G.; Ferini-Strambi, L.; Oldani, A.; Castronovo, C.; Smirne, S. Craniofacial modifications in children with habitual snoring and obstructive sleep apnoea: A case-control study. Eur. Respir. J. 1999, 13, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Guarda-Nardini, L.; Manfredini, D.; Mion, M.; Heir, G.; Marchese-Ragona, R. Anatomically Based Outcome Predictors of Treatment for Obstructive Sleep Apnea with Intraoral Splint Devices: A Systematic Review of Cephalometric Studies. J. Clin. Sleep Med. 2015, 11, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Vale, F.; Albergaria, M.; Carrilho, E.; Francisco, I.; Guimarães, A.; Caramelo, F.; Maló, L. Efficacy of Rapid Maxillary Expansion in the Treatment of Obstructive Sleep Apnea Syndrome: A Systematic Review With Meta-analysis. J. Evid.-Based Dent. Pract. 2017, 17, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.; Chang, E.T.; Song, S.A.; Abdullatif, J.; Zaghi, S.; Pirelli, P.; Certal, V.; Guilleminault, C. Rapid maxillary expansion for pediatric obstructive sleep apnea: A systematic review and meta-analysis. Laryngoscope 2017, 127, 1712–1719. [Google Scholar] [CrossRef]
- Sheats, R.D. Management of side effects of oral appliance therapy for sleep-disordered breathing: Summary of American Academy of Dental Sleep Medicine recommendations. J. Clin. Sleep Med. 2020, 16, 835. [Google Scholar] [CrossRef] [PubMed]
- Zaghi, S.; Holty, J.-E.C.; Certal, V.; Abdullatif, J.; Guilleminault, C.; Powell, N.B.; Riley, R.W.; Camacho, M. Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea: A Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 58–66. [Google Scholar] [CrossRef]
- Camacho, M.; Liu, S.Y.; Certal, V.; Capasso, R.; Powell, N.B.; Riley, R.W. Large maxillomandibular advancements for obstructive sleep apnea: An operative technique evolved over 30 years. J. Cranio-Maxillofac. Surg. 2015, 43, 1113–1118. [Google Scholar] [CrossRef]
- Handler, E.; Hamans, E.; Goldberg, A.N.; Mickelson, S. Tongue suspension: An evidence-based review and comparison to hypopharyngeal surgery for OSA. Laryngoscope 2014, 124, 329–336. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, Y.; Wang, Z.; Zhao, G.; Liu, L.; Bi, Y. Obstructive sleep apnea and risk of cardiovascular disease and all-cause mortality: A meta-analysis of prospective cohort studies. Int. J. Cardiol. 2013, 169, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Javaheri, S.; Barbe, F.; Campos-Rodriguez, F.; Dempsey, J.A.; Khayat, R.; Javaheri, S.; Malhotra, A.; Martinez-Garcia, M.A.; Mehra, R.; Pack, A.I.; et al. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequences. J. Am. Coll. Cardiol. 2017, 69, 841–858. [Google Scholar] [CrossRef]
- Leng, Y.; McEvoy, C.T.; Allen, I.E.; Yaffe, K. Association of Sleep-Disordered Breathing With Cognitive Function and Risk of Cognitive Impairment: A Systematic Review and Meta-analysis. JAMA Neurol. 2017, 74, 1237–1245. [Google Scholar] [CrossRef]
- Rosenzweig, I.; Glasser, M.; Polsek, D.; Leschziner, G.D.; Williams, S.C.; Morrell, M.J. Sleep apnoea and the brain: A complex relationship. Lancet Respir. Med. 2015, 3, 404–414. [Google Scholar] [CrossRef]
- Ong, C.W.; O’Driscoll, D.M.; Truby, H.; Naughton, M.T.; Hamilton, G.S. The reciprocal interaction between obesity and obstructive sleep apnoea. Sleep Med. Rev. 2013, 17, 123–131. [Google Scholar] [CrossRef]
- Framnes, S.N.; Arble, D.M. The Bidirectional Relationship Between Obstructive Sleep Apnea and Metabolic Disease. Front. Endocrinol. 2018, 9, 440. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Guglielmi, O.; Sanna, A.; Mancardi, G.L.; Magnavita, N. Risk of Occupational Accidents in Workers with Obstructive Sleep Apnea: Systematic Review and Meta-analysis. Sleep 2016, 39, 1211–1218. [Google Scholar] [CrossRef]
- Gupta, M.A.; Simpson, F.C. Obstructive sleep apnea and psychiatric disorders: A systematic review. J. Clin. Sleep Med. 2015, 11, 165–175. [Google Scholar] [CrossRef]
- Araghi, M.H.; Chen, Y.-F.; Jagielski, A.; Choudhury, S.; Banerjee, D.; Hussain, S.; Thomas, G.N.; Taheri, S. Effectiveness of lifestyle interventions on obstructive sleep apnea (OSA): Systematic review and meta-analysis. Sleep 2013, 36, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.E.; Issa, F.G.; Berthon-Jones, M.; Eves, L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865. [Google Scholar] [CrossRef]
- Weaver, T.E.; Grunstein, R.R. Adherence to continuous positive airway pressure therapy: The challenge to effective treatment. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Marklund, M.; Verbraecken, J.; Randerath, W. Non-CPAP therapies in obstructive sleep apnoea: Mandibular advancement device therapy. Eur. Respir. J. 2012, 39, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, B.; Hsia, J.; Capasso, R. Surgical therapy of obstructive sleep apnea: A review. Neurotherapeutics 2012, 9, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.A.; Anttila, H.; Axelsson, S.; Gislason, T.; Maasilta, P.; Myhre, K.I.; Rehnqvist, N. Effects and side-effects of surgery for snoring and obstructive sleep apnea—A systematic review. Sleep 2009, 32, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, S.; Lim, J.; Lasserson, T.J. Surgery for obstructive sleep apnoea in adults. Cochrane Database Syst. Rev. 2005, CD001004. [Google Scholar] [CrossRef]
- Doff, M.H.J.; Hoekema, A.; Wijkstra, P.J.; van der Hoeven, J.H.; Slater, J.J.R.H.; de Bont, L.G.M.; Stegenga, B. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: A 2-year follow-up. Sleep 2013, 36, 1289–1296. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Reference | Author(s) | Year | Key Contents |
|---|---|---|---|
| Xerostomia | |||
| [10,11] | Makeeva IM et al. | 2021 | Associated with xerostomia, reduced salivary flow, and worsening of oral health disorders |
| Apessos I et al. | 2020 | ||
| [22,23,24,25] | Pico-Orozco J et al. | 2020 | Decreased salivary flow related to OSA due to mouth breathing during sleep |
| Huang Z et al. | 2023 | ||
| Huang Z et al. | 2023 | ||
| Zhang C et al. | 2021 | ||
| [26,27,28] | Tanasiewicz M et al. | 2016 | Demonstration that xerostomia is an uncomfortable symptom that can worsen oral health disorders |
| Millsop JW et al. | 2017 | ||
| Guggenheimer J et al. | 2003 | ||
| Periodontal disease | |||
| [33,34] | Téllez-Corral MA et al. | 2022 | Risks of dental caries, periodontal disease, and oral infections correlated with reduced saliva production in OSA patients |
| Téllez-Corral MA et al. | 2023 | ||
| [39] | Shimazaki Y et al. | 2017 | Regular oral hygiene practices to reduce risks associated with reduced saliva flow and promote adequate hydration in OSA patients |
| [40,41,42,43] | Ahmad NE et al. | 2013 | Correlation between periodontal disease and OSA, with an increased inflammatory response |
| Chen Y et al. | 2023 | ||
| Keller JJ et al. | 2013 | ||
| Nizam N et al. | 2015 | ||
| Inflammatory cytokines | |||
| [42] | Keller JJ et al. | 2013 | Essential role of inflammatory cytokines in the pathogenesis of both disorders |
| [44] | Trombone C et al. | 2009 | Correlation between TNF-α levels and various indicators of oral health, including worsened attachment loss |
| [45] | Latorre C et al. | 2018 | Significant correlation between periodontitis and OSA, with activation of pro-inflammatory molecules |
| [46] | Arango Jimenez N et al. | 2023 | Tendency for patients with periodontitis to exhibit more severe obstructive sleep apnea |
| Bruxism | |||
| [47,48,49] | Li D et al. | 2023 | Prevalence of bruxism in OSA patients, suggesting a physiological relationship between the two |
| Wali SO et al. | 2017 | ||
| Alqahtani ND et al. | 2018 | ||
| [50] | Martynowicz H et al. | 2019 | Bruxism as a potential cause of sleep disturbances |
| [51] | Inana R et al. | 2017 | Association of bruxism with increased sympathetic activity and compromised modulation of the brainstem inhibitory circuit |
| [52] | Lee JH et al. | 2023 | Harmful effects of bruxism related to periodontal health and tooth sensitivity |
| Temporomandibular Joint Disorders Palatal and Dental Changes | |||
| [53] | Ning R et al. | 2023 | Common symptom of TMD correlated with obstructive sleep apnea |
| [54] | Klasser GD et al. | 2015 | Frequent association between bruxism and OSA, with an impact on the patient’s quality of life |
| [55] | Ciavarella D et al. | 2023 | Importance of palatal and dental alterations in the severity and course of OSA |
| Taste Disorders | |||
| [56] | Magliulo G et al. | 2018 | Changes in taste perception as a significant concern in OSA |
| [57] | Yenigun A et al. | 2019 | Significant differences in olfactory and taste perception tests between individuals with and without OSA |
| [58] | Liu Y et al. | 2020 | Significant variations in taste perception among patients with different severities of OSA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maniaci, A.; Lavalle, S.; Anzalone, R.; Lo Giudice, A.; Cocuzza, S.; Parisi, F.M.; Torrisi, F.; Iannella, G.; Sireci, F.; Fadda, G.; et al. Oral Health Implications of Obstructive Sleep Apnea: A Literature Review. Biomedicines 2024, 12, 1382. https://doi.org/10.3390/biomedicines12071382
Maniaci A, Lavalle S, Anzalone R, Lo Giudice A, Cocuzza S, Parisi FM, Torrisi F, Iannella G, Sireci F, Fadda G, et al. Oral Health Implications of Obstructive Sleep Apnea: A Literature Review. Biomedicines. 2024; 12(7):1382. https://doi.org/10.3390/biomedicines12071382
Chicago/Turabian StyleManiaci, Antonino, Salvatore Lavalle, Riccardo Anzalone, Antonino Lo Giudice, Salvatore Cocuzza, Federica Maria Parisi, Filippo Torrisi, Giannicola Iannella, Federico Sireci, Gianluca Fadda, and et al. 2024. "Oral Health Implications of Obstructive Sleep Apnea: A Literature Review" Biomedicines 12, no. 7: 1382. https://doi.org/10.3390/biomedicines12071382
APA StyleManiaci, A., Lavalle, S., Anzalone, R., Lo Giudice, A., Cocuzza, S., Parisi, F. M., Torrisi, F., Iannella, G., Sireci, F., Fadda, G., Lentini, M., Masiello, E., & La Via, L. (2024). Oral Health Implications of Obstructive Sleep Apnea: A Literature Review. Biomedicines, 12(7), 1382. https://doi.org/10.3390/biomedicines12071382