

Prior Appendicectomy and Gut Microbiota Re-Establishment in Adults after Bowel Preparation and Colonoscopy
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants and Setting
2.3. Data Collection
2.4. Intervention
2.5. Outcome Measures
2.6. Covariates
2.7. DNA Extraction
2.8. Sequencing and Annotation
2.9. Pre-Processing
2.10. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Between-Group Differences in Gut Microbiota Composition at Baseline and Follow Up
3.3. Within-Group Changes in Gut Microbiota Composition Post-Procedure
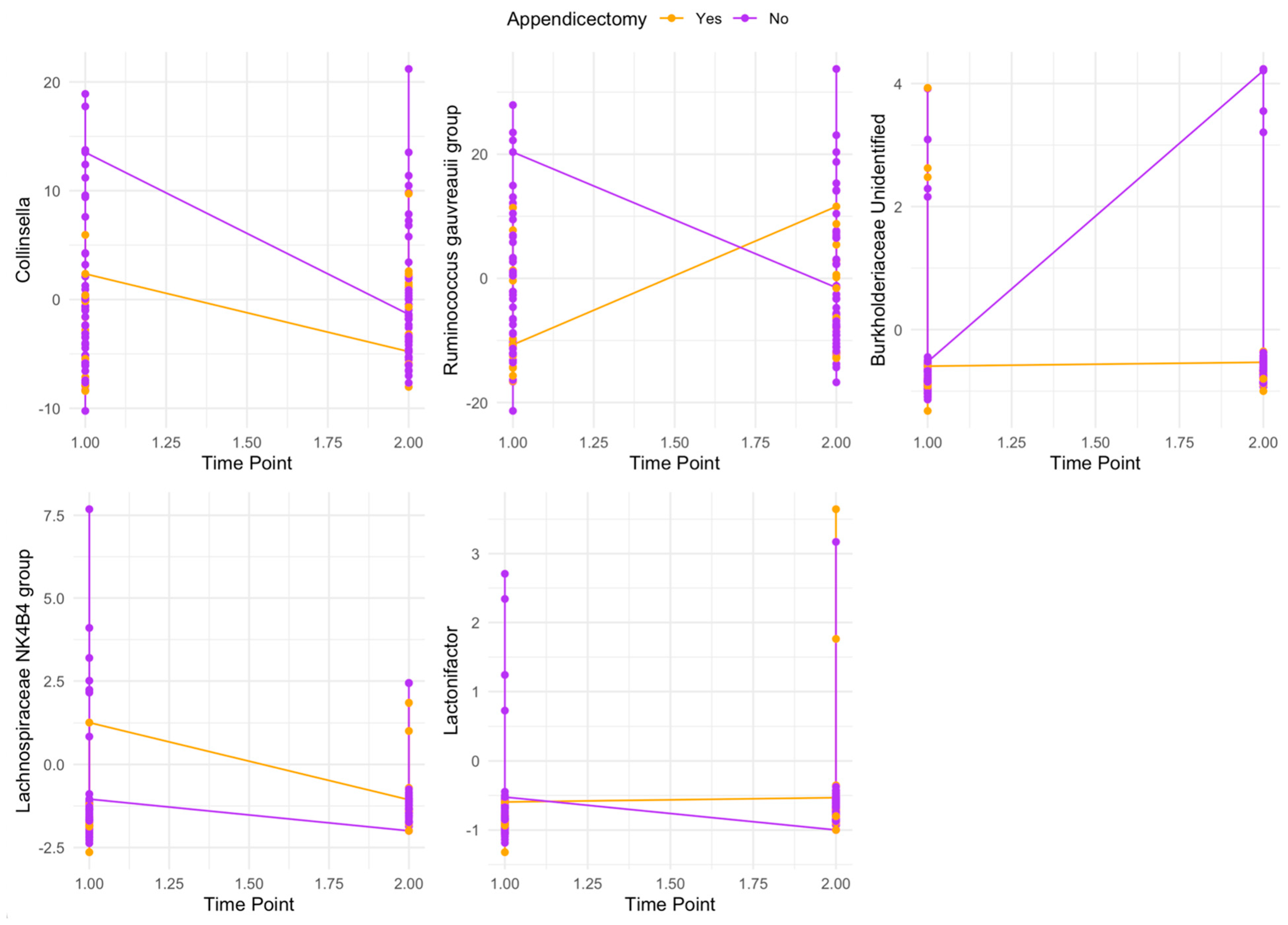
3.4. Post Hoc Analyses of Appendicectomy as an Effect Modifier of Genus Re-Establishment
4. Discussion
4.1. Summary of Findings
4.2. Potential Clinical Implications
4.3. Challenges to Studying the Potential Function of the Human Appendix
4.4. Limitations of the Present Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Girard-Madoux, M.J.H.; Gomez de Aguero, M.; Ganal-Vonarburg, S.C.; Mooser, C.; Belz, G.T.; Macpherson, A.J.; Vivier, E. The immunological functions of the Appendix: An example of redundancy? Semin. Immunol. 2018, 36, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Kooij, I.A.; Sahami, S.; Meijer, S.L.; Buskens, C.J.; Te Velde, A.A. The immunology of the vermiform appendix: A review of the literature. Clin. Exp. Immunol. 2016, 186, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L.; Chen, J.; Clarke, S. The vermiform appendix: An immunological organ sustaining a microbiome inoculum. Clin. Sci. 2019, 133, 1–8. [Google Scholar] [CrossRef]
- Laurin, M.; Everett, M.L.; Parker, W. The cecal appendix: One more immune component with a function disturbed by post-industrial culture. Anat. Rec. 2011, 294, 567–579. [Google Scholar] [CrossRef]
- Spencer, J.; Finn, T.; Isaacson, P.G. Gut associated lymphoid tissue: A morphological and immunocytochemical study of the human appendix. Gut 1985, 26, 672–679. [Google Scholar] [CrossRef]
- Schumpelick, V.; Dreuw, B.; Ophoff, K.; Prescher, A. Appendix and cecum. Embryology, anatomy, and surgical applications. Surg. Clin. N. Am. 2000, 80, 295–318. [Google Scholar] [CrossRef] [PubMed]
- Vieira, E.d.P.L.; Bonato, L.M.; Silva, G.G.P.d.; Gurgel, J.L. Congenital abnormalities and anatomical variations of the vermiform appendix and mesoappendix. J. Coloproctol. 2019, 39, 279–287. [Google Scholar] [CrossRef]
- Wong, S.H.; Yu, J. Gut microbiota in colorectal cancer: Mechanisms of action and clinical applications. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 690–704. [Google Scholar] [CrossRef]
- Pinart, M.; Dotsch, A.; Schlicht, K.; Laudes, M.; Bouwman, J.; Forslund, S.K.; Pischon, T.; Nimptsch, K. Gut Microbiome Composition in Obese and Non-Obese Persons: A Systematic Review and Meta-Analysis. Nutrients 2021, 14, 12. [Google Scholar] [CrossRef]
- McGuinness, A.J.; Davis, J.A.; Dawson, S.L.; Loughman, A.; Collier, F.; O’Hely, M.; Simpson, C.A.; Green, J.; Marx, W.; Hair, C.; et al. A systematic review of gut microbiota composition in observational studies of major depressive disorder, bipolar disorder and schizophrenia. Mol. Psychiatry 2022, 27, 1920–1935. [Google Scholar] [CrossRef]
- Guinane, C.M.; Tadrous, A.; Fouhy, F.; Ryan, C.A.; Dempsey, E.M.; Murphy, B.; Andrews, E.; Cotter, P.D.; Stanton, C.; Ross, R.P. Microbial composition of human appendices from patients following appendectomy. mBio 2013, 4, e00366-12. [Google Scholar] [CrossRef] [PubMed]
- Randal Bollinger, R.; Barbas, A.S.; Bush, E.L.; Lin, S.S.; Parker, W. Biofilms in the large bowel suggest an apparent function of the human vermiform appendix. J. Theor. Biol. 2007, 249, 826–831. [Google Scholar] [CrossRef]
- Palestrant, D.; Holzknecht, Z.E.; Collins, B.H.; Parker, W.; Miller, S.E.; Bollinger, R.R. Microbial biofilms in the gut: Visualization by electron microscopy and by acridine orange staining. Ultrastruct. Pathol. 2004, 28, 23–27. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Mirzayi, C.; Renson, A.; Genomic Standards Consortium; Massive Analysis and Quality Control Society Furlanello Cesare 31 Sansone Susanna-Assunta 84; Zohra, F.; Elsafoury, S.; Geistlinger, L.; Kasselman, L.J.; Eckenrode, K.; van de Wijgert, J.; et al. Reporting guidelines for human microbiome research: The STORMS checklist. Nat. Med. 2021, 27, 1885–1892. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.J.; Calderwood, A.H.; Doros, G.; Fix, O.K.; Jacobson, B.C. The Boston bowel preparation scale: A valid and reliable instrument for colonoscopy-oriented research. Gastrointest. Endosc. 2009, 69, 620–625. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 2033.0.55.001—Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA), Australia, 2016; Australian Bureau of Statistics: Belconnen, Australia, 2018.
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef]
- Dawson, S.L.; Mohebbi, M.; Craig, J.M.; Dawson, P.; Clarke, G.; Tang, M.L.; Jacka, F.N. Targeting the perinatal diet to modulate the gut microbiota increases dietary variety and prebiotic and probiotic food intakes: Results from a randomised controlled trial. Public Health Nutr. 2021, 24, 1129–1141. [Google Scholar] [CrossRef]
- Mostafa, R. Rome III: The functional gastrointestinal disorders, third edition, 2006. World J. Gastroenterol. 2008, 14, 2124–2125. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Richardson, J.; Iezzi, A.; Khan, M.A.; Maxwell, A. Validity and reliability of the Assessment of Quality of Life (AQoL)-8D multi-attribute utility instrument. Patient 2014, 7, 85–96. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Author Correction: Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 1091. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef]
- Bokulich, N.A.; Dillon, M.R.; Zhang, Y.; Rideout, J.R.; Bolyen, E.; Li, H.; Albert, P.S.; Caporaso, J.G. q2-longitudinal: Longitudinal and Paired-Sample Analyses of Microbiome Data. mSystems 2018, 3, e00219-18. [Google Scholar] [CrossRef] [PubMed]
- Callahan, B.J.; Sankaran, K.; Fukuyama, J.A.; McMurdie, P.J.; Holmes, S.P. Bioconductor Workflow for Microbiome Data Analysis: From raw reads to community analyses. F1000Research 2016, 5, 1492. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development Environment for R; RStudio, PBC: Boston, MA, USA, 2022; Available online: http://www.rstudio.com/ (accessed on 18 August 2024).
- Cai, S.; Fan, Y.; Zhang, B.; Lin, J.; Yang, X.; Liu, Y.; Liu, J.; Ren, J.; Xu, H. Appendectomy Is Associated with Alteration of Human Gut Bacterial and Fungal Communities. Front. Microbiol. 2021, 12, 724980. [Google Scholar] [CrossRef]
- Goedert, J.J.; Hua, X.; Yu, G.; Shi, J. Diversity and composition of the adult fecal microbiome associated with history of cesarean birth or appendectomy: Analysis of the American Gut Project. EBioMedicine 2014, 1, 167–172. [Google Scholar] [CrossRef]
- Sanchez-Alcoholado, L.; Fernandez-Garcia, J.C.; Gutierrez-Repiso, C.; Bernal-Lopez, M.R.; Ocana-Wilhelmi, L.; Garcia-Fuentes, E.; Moreno-Indias, I.; Tinahones, F.J. Incidental Prophylactic Appendectomy Is Associated with a Profound Microbial Dysbiosis in the Long-Term. Microorganisms 2020, 8, 609. [Google Scholar] [CrossRef]
- Chung, W.S.; Chung, S.; Hsu, C.Y.; Lin, C.L. Risk of Inflammatory Bowel Disease Following Appendectomy in Adulthood. Front. Med. 2021, 8, 661752. [Google Scholar] [CrossRef] [PubMed]
- Radford-Smith, G.L.; Edwards, J.E.; Purdie, D.M.; Pandeya, N.; Watson, M.; Martin, N.G.; Green, A.; Newman, B.; Florin, T.H. Protective role of appendicectomy on onset and severity of ulcerative colitis and Crohn’s disease. Gut 2002, 51, 808–813. [Google Scholar] [CrossRef]
- Koutroubakis, I.E.; Vlachonikolis, I.G.; Kouroumalis, E.A. Role of appendicitis and appendectomy in the pathogenesis of ulcerative colitis: A critical review. Inflamm. Bowel Dis. 2002, 8, 277–286. [Google Scholar] [CrossRef]
- Andersson, R.E.; Olaison, G.; Tysk, C.; Ekbom, A. Appendectomy and protection against ulcerative colitis. N. Engl. J. Med. 2001, 344, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Cosnes, J.; Carbonnel, F.; Beaugerie, L.; Blain, A.; Reijasse, D.; Gendre, J.P. Effects of appendicectomy on the course of ulcerative colitis. Gut 2002, 51, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.G.; Pedersen, B.V.; Andersson, R.E.; Sands, B.E.; Korzenik, J.; Frisch, M. The risk of developing Crohn’s disease after an appendectomy: A population-based cohort study in Sweden and Denmark. Gut 2007, 56, 1387–1392. [Google Scholar] [CrossRef]
- Essrani, R.; Saturno, D.; Mehershahi, S.; Essrani, R.K.; Hossain, M.R.; Ravi, S.J.K.; Berger, A.; Mehmood, A. The Impact of Appendectomy in Clostridium difficile Infection and Length of Hospital Stay. Cureus 2020, 12, e10342. [Google Scholar] [CrossRef]
- Im, G.Y.; Modayil, R.J.; Lin, C.T.; Geier, S.J.; Katz, D.S.; Feuerman, M.; Grendell, J.H. The appendix may protect against Clostridium difficile recurrence. Clin. Gastroenterol. Hepatol. 2011, 9, 1072–1077. [Google Scholar] [CrossRef]
- Fujii, L.; Fasolino, J.; Crowell, M.D.; DiBaise, J.K. Appendectomy and Risk of Clostridium difficile Recurrence. Infect. Dis. Clin. Pract. 2013, 21, 28–32. [Google Scholar] [CrossRef]
- Merchant, R.; Mower, W.R.; Ourian, A.; Abrahamian, F.M.; Moran, G.J.; Krishnadasan, A.; Talan, D.A. Association between Appendectomy and Clostridium difficile Infection. J. Clin. Med. Res. 2012, 4, 17. [Google Scholar] [CrossRef]
- Wu, S.-C.; Chen, W.T.-L.; Muo, C.-H.; Ke, T.-W.; Fang, C.-W.; Sung, F.-C. Association between Appendectomy and Subsequent Colorectal Cancer Development: An Asian Population Study. PLoS ONE 2015, 10, e0118411. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.Y.; Lee, K.Y.; Oh, S.T.; Park, S.H.; Han, K.D.; Lee, J. A link between appendectomy and gastrointestinal cancers: A large-scale population-based cohort study in Korea. Sci. Rep. 2020, 10, 15670. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, J.A.; Mori, N.; Artaud, F.; Fournier, A.; Conte, M.; Boutron-Ruault, M.C.; Chan, S.S.M.; Gunter, M.J.; Murphy, N.; Severi, G. Colorectal cancer risk following appendectomy: A pooled analysis of three large prospective cohort studies. Cancer Commun. 2022, 42, 486–489. [Google Scholar] [CrossRef]
- Skoldberg, F.; Olen, O.; Ekbom, A.; Schmidt, P.T. Appendectomy and Risk of Subsequent Diverticular Disease Requiring Hospitalization: A Population-Based Case-Control Study. Dis. Colon Rectum 2018, 61, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Tsai, M.C.; Lin, H.C.; Lee, H.C.; Lee, C.Z.; Chung, S.D. Appendectomy increased the risk of ischemic heart disease. J. Surg. Res. 2015, 199, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Janszky, I.; Mukamal, K.J.; Dalman, C.; Hammar, N.; Ahnve, S. Childhood appendectomy, tonsillectomy, and risk for premature acute myocardial infarction--a nationwide population-based cohort study. Eur. Heart J. 2011, 32, 2290–2296. [Google Scholar] [CrossRef]
- Tzeng, Y.M.; Kao, L.T.; Kao, S.; Lin, H.C.; Tsai, M.C.; Lee, C.Z. An appendectomy increases the risk of rheumatoid arthritis: A five-year follow-up study. PLoS ONE 2015, 10, e0126816. [Google Scholar] [CrossRef]
- Ishizuka, M.; Shibuya, N.; Takagi, K.; Hachiya, H.; Tago, K.; Suda, K.; Aoki, T.; Kubota, K. Appendectomy Does Not Increase the Risk of Future Emergence of Parkinson’s Disease: A Meta-analysis. Am. Surg. 2021, 87, 1802–1808. [Google Scholar] [CrossRef]
- Ekstrom, L.D.; Ekstrom, H.; Dal, H.; Kosidou, K.; Gustafsson, U.O. Childhood appendectomy and adult mental disorders: A population-based cohort study. Depress. Anxiety 2020, 37, 1108–1117. [Google Scholar] [CrossRef]
- Shi, F.; Liu, G.; Lin, Y.; Guo, C.l.; Han, J.; Chu, E.S.H.; Shi, C.; Li, Y.; Zhang, H.; Hu, C.; et al. Altered gut microbiome composition by appendectomy contributes to colorectal cancer. Oncogene 2023, 42, 530–540. [Google Scholar] [CrossRef]

{kind=link}
| Variable | With Appendix | Without Appendix |
|---|---|---|
| Participants, n (%) | 45 (78%) | 13 (22%) |
| Age, mean (SD) | 58.4 (11.1) | 60.5 (9.9) |
| Sex, female n (%) | 26 (58%) | 5 (39%) |
| BMI, mean (SD) | 30.9 (6.5) | 26.0 (4.8) |
| Currently smoking, yes n (%) | 5 (11%) | 1 (8%) |
| IBS, yes n (%) | 11 (24%) | 2 (15%) |
| Missing | 1 (2.2%) | 0 (0%) |
| Diet quality ‡, mean (SD) | 44.2 (11.5) | 48.9 (11.4) |
| Depression symptomatology, mean (SD) | 4.13 (3.31) | 2.15 (1.21) |
| Depression severity, mean (SD) | 4.29 (5.88) | 1.15 (2.15) |
| Anxiety symptomatology, mean (SD) | 5.78 (3.98) | 3.92 (2.56) |
| Physical quality of life, mean (SD) | 0.689 (0.178) | 0.790 (0.103) |
| Psychosocial quality of life, mean (SD) | 0.456 (0.213) | 0.581 (0.173) |
| Overall quality of life, mean (SD) | 0.746 (0.199) | 0.868 (0.106) |
| Gastrointestinal medications, yes n (%) | ||
| Hyperacidity/reflux medication, | 19 (42%) | 3 (23%) |
| Digestive supplements/cholelitholytics | 1 (2%) | 1 (8%) |
| Self-reported prior gastrointestinal disease, yes n (%) | ||
| Hiatus hernia/oesophageal reflux | 5 (11%) | 1 (8%) |
| Chronic diarrhoea | 3 (7%) | 0 (0%) |
| Chronic gastritis | 1 (2%) | 0 (0%) |
| Bowel cancer § | 1 (2%) | 0 (0%) |
| Peptic ulcer disease § | 0 (0%) | 1 (8%) |
| History of sleeve gastrectomy | 1 (2%) | 0 (0%) |
| Missing | 1 (2%) | 1 (8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGuinness, A.J.; O’Hely, M.; Stupart, D.; Watters, D.; Dawson, S.L.; Hair, C.; Berk, M.; Mohebbi, M.; Loughman, A.; Guest, G.; et al. Prior Appendicectomy and Gut Microbiota Re-Establishment in Adults after Bowel Preparation and Colonoscopy. Biomedicines 2024, 12, 1938. https://doi.org/10.3390/biomedicines12091938
McGuinness AJ, O’Hely M, Stupart D, Watters D, Dawson SL, Hair C, Berk M, Mohebbi M, Loughman A, Guest G, et al. Prior Appendicectomy and Gut Microbiota Re-Establishment in Adults after Bowel Preparation and Colonoscopy. Biomedicines. 2024; 12(9):1938. https://doi.org/10.3390/biomedicines12091938
Chicago/Turabian StyleMcGuinness, Amelia J., Martin O’Hely, Douglas Stupart, David Watters, Samantha L. Dawson, Christopher Hair, Michael Berk, Mohammadreza Mohebbi, Amy Loughman, Glenn Guest, and et al. 2024. "Prior Appendicectomy and Gut Microbiota Re-Establishment in Adults after Bowel Preparation and Colonoscopy" Biomedicines 12, no. 9: 1938. https://doi.org/10.3390/biomedicines12091938