Investigating Modifiable Risk Factors Across Dementia Subtypes: Insights from the UK Biobank


Abstract
1. Introduction
2. Materials and Methods
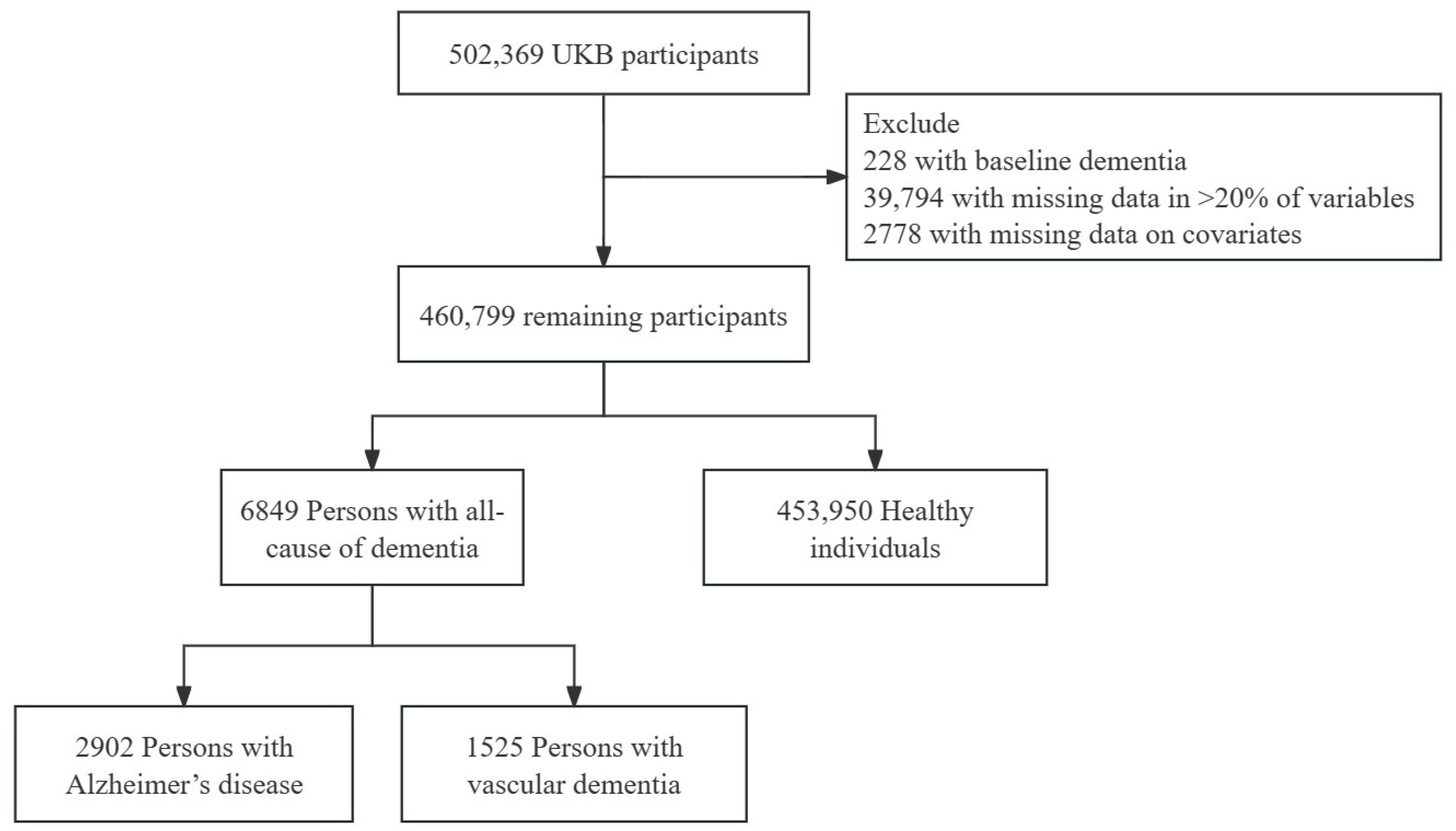
2.1. Study Population
2.2. Dementia Diagnosis
2.3. Modifiable Factors
2.4. Statistical Analyses
3. Results
3.1. Risk Factors for Dementia
3.2. Joint Effects of Risk Factors on Dementia
3.3. PAF Estimates for the Seven Domains in Dementia Prevention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malik, I.; Iqbal, A.; Gu, Y.H.; Al-antari, M.A. Deep Learning for Alzheimer’s Disease Prediction: A Comprehensive Review. Diagnostics 2024, 14, 1281. [Google Scholar] [CrossRef]
- Browning, C.A.; Thompson, C.L.; Kochan, N.A.; Brodaty, H.; Sachdev, P.S.; Henry, J.D. Prospective Memory Function Predicts Future Cognitive Decline and Incident Dementia. J. Gerontol. Ser. B 2023, 78, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Mathias, J.L.; Burke, J. Cognitive Functioning in Alzheimer’s and Vascular Dementia: A Meta-Analysis. Neuropsychology 2009, 23, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, G.; Danti, S.; Picchi, L.; Nuti, A.; Fiorino, M.D. Daily Functioning and Dementia. Dement. Neuropsychol. 2020, 14, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Sun, S.; Kang, W.; Wu, S.; Lin, L. A Review of Neuroimaging-Based Data-Driven Approach for Alzheimer’s Disease Heterogeneity Analysis. Rev. Neurosci. 2024, 35, 121–139. [Google Scholar] [PubMed]
- Swerdlow, R.H. Pathogenesis of Alzheimer’s Disease. Clin. Interv. Aging 2007, 2, 347–359. [Google Scholar]
- Hadjichrysanthou, C.; Ower, A.K.; De Wolf, F.; Anderson, R.M.; for the Alzheimer’s Disease Neuroimaging Initiative. The Development of a Stochastic Mathematical Model of Alzheimer’s Disease to Help Improve the Design of Clinical Trials of Potential Treatments. PLoS ONE 2018, 13, e0190615. [Google Scholar] [CrossRef]
- Pennese, F.; Del Re, M.L.; Esposito, F.; Zito, M.; Abate, G. Clinical and Tomographic Findings in Vascular Dementia. Aging Clin. Exp. Res. 1994, 6, 57–64. [Google Scholar]
- Mulkey, M. Understanding Frontotemporal Disease Progression and Management Strategies. Nurs. Clin. N. Am. 2019, 54, 437–448. [Google Scholar] [CrossRef]
- McKeith, I.G. Dementia with Lewy Bodies. Br. J. Psychiatry 2002, 180, 144–147. [Google Scholar] [CrossRef]
- Khan, M.; Jaiswal, A.; Wandile, B. A Comprehensive Review of Modifiable Cardiovascular Risk Factors and Genetic Influences in Dementia Prevention. Cureus 2023, 15, e48430. [Google Scholar] [CrossRef]
- Zhang, B.; Lin, L.; Wu, S. A Review of Brain Atrophy Subtypes Definition and Analysis for Alzheimer’s Disease Heterogeneity Studies. JAD 2021, 80, 1339–1352. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, T.; Ly, A.; Schnier, C.; Rannikmäe, K.; Bush, K.; Brayne, C.; Quinn, T.J.; Sudlow, C.L.M.; on behalf of the UK Biobank Neurodegenerative Outcomes Group and Dementias Platform UK. Identifying Dementia Cases with Routinely Collected Health Data: A Systematic Review. Alzheimers Amp Dement. 2018, 14, 1038–1051. [Google Scholar] [CrossRef] [PubMed]
- Juárez-Cedillo, T.; Martínez-Rodríguez, N.; Fragoso, J.M.; Islas-Pérez, V.; lópez-Martínez, A.; Valle-Medina, A. Multifactor Dimensionality Reduction Analysis to Evaluate the Association of Dopamine Beta-Hydroxylase (DΒH) Polymorphisms with Susceptibility to Dementia (SADEM Study). Mol. Neurobiol. 2023, 60, 4731–4737. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Hoshide, S.; Kario, K. Hypertension and Dementia. Am. J. Hypertens. 2010, 23, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Maslow, K. Dementia, Diabetes and Family Caregiving. Aging Ment. Health 2011, 15, 933–935. [Google Scholar] [CrossRef]
- Arnoldussen, I.A.C.; Kiliaan, A.J.; Gustafson, D.R. Obesity and Dementia: Adipokines Interact with the Brain. Eur. Neuropsychopharmacol. 2014, 24, 1982–1999. [Google Scholar] [CrossRef]
- Elbejjani, M.; Auer, R.; Dolui, S.; Jacobs, D.R.; Haight, T.; Goff, D.C.; Detre, J.A.; Davatzikos, C.; Bryan, R.N.; Launer, L.J. Cigarette Smoking and Cerebral Blood Flow in a Cohort of Middle-Aged Adults. J. Cereb. Blood Flow Metab. 2019, 39, 1247–1257. [Google Scholar] [CrossRef]
- Licher, S.; Ahmad, S.; Karamujić-Čomić, H.; Voortman, T.; Leening, M.J.G.; Ikram, M.A.; Ikram, M.K. Genetic Predisposition, Modifiable-Risk-Factor Profile and Long-Term Dementia Risk in the General Population. Nat. Med. 2019, 25, 1364–1369. [Google Scholar] [CrossRef]
- Oudin, A.; Forsberg, B.; Adolfsson, A.N.; Lind, N.; Modig, L.; Nordin, M.; Nordin, S.; Adolfsson, R.; Nilsson, L.-G. Traffic-Related Air Pollution and Dementia Incidence in Northern Sweden: A Longitudinal Study. Environ. Health Perspect. 2016, 124, 306–312. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Fayosse, A.; Sabia, S.; Canonico, M.; Bobak, M.; Elbaz, A.; Kivimäki, M.; Dugravot, A. Atrial Fibrillation as a Risk Factor for Cognitive Decline and Dementia. Eur. Heart J. 2017, 38, 2612–2618. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Flicker, L. Depression as a Modifiable Factor to Decrease the Risk of Dementia. Transl. Psychiatry 2017, 7, e1117. [Google Scholar] [CrossRef] [PubMed]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK Biobank: An Open Access Resource for Identifying the Causes of a Wide Range of Complex Diseases of Middle and Old Age. PLoS Med 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed]
- Fry, A.; Littlejohns, T.J.; Sudlow, C.; Doherty, N.; Allen, N.E. OP41 The Representativeness of the UK Biobank Cohort on a Range of Sociodemographic, Physical, Lifestyle and Health-Related Characteristics. J. Epidemiol. Community Health 2016, 70, A26. [Google Scholar]
- Glynn, P.; Greenland, P. Contributions of the UK Biobank High Impact Papers in the Era of Precision Medicine. Eur. J. Epidemiol. 2020, 35, 5–10. [Google Scholar] [CrossRef]
- Lourida, I.; Hannon, E.; Littlejohns, T.J.; Langa, K.M.; Hyppönen, E.; Kuźma, E.; Llewellyn, D.J. Association of Lifestyle and Genetic Risk With Incidence of Dementia. JAMA 2019, 322, 430–437. [Google Scholar] [CrossRef]
- Liu, W.; Wang, T.; Zhu, M.; Jin, G. Healthy Diet, Polygenic Risk Score, and Upper Gastrointestinal Cancer Risk: A Prospective Study from UK Biobank. Nutrients 2023, 15, 1344. [Google Scholar] [CrossRef]
- Yuan, S.; Ma, W.; Yang, R.; Xu, F.; Han, D.; Huang, T.; Peng, M.; Xu, A.; Lyu, J. Sleep Duration, Genetic Susceptibility, and Alzheimer’s Disease: A Longitudinal UK Biobank-Based Study. BMC Geriatr. 2022, 22, 638. [Google Scholar] [CrossRef]
- Elovainio, M.; Lahti, J.; Pirinen, M.; Pulkki-Råback, L.; Malmberg, A.; Lipsanen, J.; Virtanen, M.; Kivimäki, M.; Hakulinen, C. Association of Social Isolation, Loneliness and Genetic Risk with Incidence of Dementia: UK Biobank Cohort Study. BMJ Open 2022, 12, e053936. [Google Scholar] [CrossRef]
- He, X.-Y.; Kuo, K.; Yang, L.; Zhang, Y.-R.; Wu, B.-S.; Chen, S.-D.; Cheng, W.; Feng, J.-F.; Yu, J.-T. Serum Clinical Laboratory Tests and Risk of Incident Dementia: A Prospective Cohort Study of 407,190 Individuals. Transl. Psychiatry 2022, 12, 312. [Google Scholar] [CrossRef]
- Duchowny, K.A.; Ackley, S.F.; Brenowitz, W.D.; Wang, J.; Zimmerman, S.C.; Caunca, M.R.; Glymour, M.M. Associations Between Handgrip Strength and Dementia Risk, Cognition, and Neuroimaging Outcomes in the UK Biobank Cohort Study. JAMA Netw. Open 2022, 5, e2218314. [Google Scholar] [CrossRef]
- Hendriks, S.; Ranson, J.M.; Peetoom, K.; Lourida, I.; Tai, X.Y.; De Vugt, M.; Llewellyn, D.J.; Köhler, S. Risk Factors for Young-Onset Dementia in the UK Biobank. JAMA Neurol. 2024, 81, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, S.-D.; Deng, Y.-T.; You, J.; He, X.-Y.; Wu, X.-R.; Wu, B.-S.; Yang, L.; Zhang, Y.-R.; Kuo, K.; et al. Identifying Modifiable Factors and Their Joint Effect on Dementia Risk in the UK Biobank. Nat. Hum. Behav. 2023, 7, 1185–1195. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Sun, D.; Zhou, T.; Heianza, Y.; Lv, J.; Li, L.; Qi, L. Sleep Patterns, Genetic Susceptibility, and Incident Cardiovascular Disease: A Prospective Study of 385 292 UK Biobank Participants. Eur. Heart J. 2020, 41, 1182–1189. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Ritchie, K.; Carriere, I.; Ritchie, C.W.; Berr, C.; Artero, S.; Ancelin, M.-L. Designing Prevention Programmes to Reduce Incidence of Dementia: Prospective Cohort Study of Modifiable Risk Factors. BMJ 2010, 341, c3885. [Google Scholar] [CrossRef]
- Sjölander, A. Estimation of Causal Effect Measures with the R-Package stdReg. Eur. J. Epidemiol. 2018, 33, 847–858. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia Prevention, Intervention, and Care: 2020 Report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Liu, L.; Lin, L.; Sun, S.; Wu, S. Elucidating Multimodal Imaging Patterns in Accelerated Brain Aging: Heterogeneity through a Discriminant Analysis Approach Using the UK Biobank Dataset. Bioengineering 2024, 11, 124. [Google Scholar] [CrossRef]
- Joy Mathew, C.; Jose, M.T.; Elshaikh, A.O.; Shah, L.; Lee, R.; Cancarevic, I. Is Hyperthyroidism a Possible Etiology of Early Onset Dementia? Cureus 2020, 12, e10603. [Google Scholar] [CrossRef]
- Sakaniwa, R.; Shirai, K.; Cadar, D.; Saito, T.; Kondo, K.; Kawachi, I.; Steptoe, A.; Iso, H. Socioeconomic Status Transition Throughout Life and Risk of Dementia. JAMA Netw. Open 2024, 7, e2412303. [Google Scholar] [CrossRef]
- He, P.; Zhou, C.; Ye, Z.; Liu, M.; Zhang, Y.; Wu, Q.; Zhang, Y.; Yang, S.; Xiaoqin, G.; Qin, X. Walking Pace, Handgrip Strength, Age, APOE Genotypes, and New-Onset Dementia: The UK Biobank Prospective Cohort Study. Alzheimers Res. Ther. 2023, 15, 9. [Google Scholar] [CrossRef] [PubMed]
- Sattler, C.; Toro, P.; Schönknecht, P.; Schröder, J. Cognitive Activity, Education and Socioeconomic Status as Preventive Factors for Mild Cognitive Impairment and Alzheimer’s Disease. Psychiatry Res. 2012, 196, 90–95. [Google Scholar] [CrossRef]
- Caffò, A.O.; Spano, G.; Tinella, L.; Lopez, A.; Ricciardi, E.; Stasolla, F.; Bosco, A. The Prevalence of Amnestic and Non-Amnestic Mild Cognitive Impairment and Its Association with Different Lifestyle Factors in a South Italian Elderly Population. Int. J. Environ. Res. Public Health 2022, 19, 3097. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Zhu, M.; Jiao, H.; Song, Y.; et al. Prevalence, Risk Factors, and Management of Dementia and Mild Cognitive Impairment in Adults Aged 60 Years or Older in China: A Cross-Sectional Study. Lancet Public Health 2020, 5, e661–e671. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Jin, Y.; Xiong, M.; Wu, S.; Sun, S. The Protective Power of Cognitive Reserve: Examining White Matter Integrity and Cognitive Function in the Aging Brain for Sustainable Cognitive Health. Sustainability 2023, 15, 11336. [Google Scholar] [CrossRef]
- Jin, Y.; Lin, L.; Xiong, M.; Sun, S.; Wu, S. Moderating Effects of Cognitive Reserve on the Relationship between Brain Structure and Cognitive Abilities in Middle-Aged and Older Adults. Neurobiol. Aging 2023, 128, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Carret, N.L.; Auriacombe, S.; Letenneur, L.; Bergua, V.; Dartigues, J.-F.; Fabrigoule, C. Influence of Education on the Pattern of Cognitive Deterioration in AD Patients: The Cognitive Reserve Hypothesis. Brain Cogn. 2005, 57, 120–126. [Google Scholar] [CrossRef]
- Bennett, D.A.; Wilson, R.S.; Schneider, J.A.; Evans, D.A.; Mendes de Leon, C.F.; Arnold, S.E.; Barnes, L.L.; Bienias, J.L. Education Modifies the Relation of AD Pathology to Level of Cognitive Function in Older Persons. Neurology 2003, 60, 1909–1915. [Google Scholar] [CrossRef]
- Rehm, J.; Hasan, O.S.M.; Black, S.E.; Shield, K.D.; Schwarzinger, M. Alcohol Use and Dementia: A Systematic Scoping Review. Alzheimers Res. Ther. 2019, 11, 1. [Google Scholar] [CrossRef]
- Piano, M.R. Alcohol’s Effects on the Cardiovascular System. Alcohol Res. 2017, 38, 219–241. [Google Scholar] [PubMed]
- Xu, X.; Lin, L.; Wu, S.; Sun, S. Exploring Successful Cognitive Aging: Insights Regarding Brain Structure, Function, and Demographics. Brain Sci. 2023, 13, 1651. [Google Scholar] [CrossRef]
- Lin, L.; Xiong, M.; Jin, Y.; Kang, W.; Wu, S.; Sun, S.; Fu, Z. Quantifying Brain and Cognitive Maintenance as Key Indicators for Sustainable Cognitive Aging: Insights from the UK Biobank. Sustainability 2023, 15, 9620. [Google Scholar] [CrossRef]
- Javanshiri, K.; Waldö, M.L.; Friberg, N.; Sjövall, F.; Wickerström, K.; Haglund, M.; Englund, E. Atherosclerosis, Hypertension, and Diabetes in Alzheimer’s Disease, Vascular Dementia, and Mixed Dementia: Prevalence and Presentation. J. Alzheimers Dis. 2018, 65, 1247–1258. [Google Scholar] [CrossRef]
- Liu, C.-H.; Sung, P.-S.; Li, Y.-R.; Huang, W.-K.; Lee, T.-W.; Huang, C.-C.; Lee, T.-H.; Chen, T.-H.; Wei, Y.-C. Telmisartan Use and Risk of Dementia in Type 2 Diabetes Patients with Hypertension: A Population-Based Cohort Study. PLoS Med. 2021, 18, e1003707. [Google Scholar] [CrossRef]
- Luan, Y.; Yao, Y. The Clinical Significance and Potential Role of C-Reactive Protein in Chronic Inflammatory and Neurodegenerative Diseases. Front. Immunol. 2018, 9, 1302. [Google Scholar] [CrossRef]
- Spangenberg, E.E.; Green, K.N. Inflammation in Alzheimer’s Disease: Lessons Learned from Microglia-Depletion Models. Brain Behav. Immun. 2017, 61, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, M.; Elkind, M.S.; Godoy, D.A.; Singh, P.; Papa, F.; Popa-Wagner, A. Role of C-Reactive Protein in Cerebrovascular Disease: A Critical Review. Expert Rev. Cardiovasc. Ther. 2011, 9, 1565–1584. [Google Scholar] [CrossRef]
- O’Brien, J.T.; Thomas, A. Vascular Dementia. Lancet 2015, 386, 1698–1706. [Google Scholar] [CrossRef]
- Hugon, J. Rheumatoid Arthritis and Cognitive Decline. Jt. Bone Spine 2022, 89, 105346. [Google Scholar] [CrossRef]
- Crowson, C.S.; Liao, K.P.; Davis, J.M.; Solomon, D.H.; Matteson, E.L.; Knutson, K.L.; Hlatky, M.A.; Gabriel, S.E. Rheumatoid Arthritis and Cardiovascular Disease. Am. Heart J. 2013, 166, 622–628.e1. [Google Scholar] [CrossRef] [PubMed]
- Piovezana Bossolani, G.D.; Silva, B.T.; Colombo Martins Perles, J.V.; Lima, M.M.; Vieira Frez, F.C.; Garcia De Souza, S.R.; Sehaber-Sierakowski, C.C.; Bersani-Amado, C.A.; Zanoni, J.N. Rheumatoid Arthritis Induces Enteric Neurodegeneration and Jejunal Inflammation, and Quercetin Promotes Neuroprotective and Anti-Inflammatory Actions. Life Sci. 2019, 238, 116956. [Google Scholar] [CrossRef]
- McInnes, I.B.; Gravallese, E.M. Immune-Mediated Inflammatory Disease Therapeutics: Past, Present and Future. Nat. Rev. Immunol. 2021, 21, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Allais, G.; Chiarle, G.; Sinigaglia, S.; Airola, G.; Schiapparelli, P.; Benedetto, C. Estrogen, Migraine, and Vascular Risk. Neurol. Sci. 2018, 39, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhang, M.; Duan, J.; Li, L.; Du, J.; Cheng, H.; Zhang, S.; Zhai, Y.; An, X.; Li, Q.; et al. Maternal Prepregnancy 5-Hydroxytryptamine Exposure Affects the Early Development of the Fetus. Front. Physiol. 2022, 13, 761357. [Google Scholar] [CrossRef]
- Khan, T.K.; Alkon, D.L. Peripheral Biomarkers of Alzheimer’s Disease. J. Alzheimers Dis. 2015, 44, 729–744. [Google Scholar] [CrossRef]
- Westwood, A.J.; Beiser, A.; DeCarli, C.; Harris, T.B.; Chen, T.C.; He, X.; Roubenoff, R.; Pikula, A.; Au, R.; Braverman, L.E.; et al. Insulin-like Growth Factor-1 and Risk of Alzheimer Dementia and Brain Atrophy. Neurol. 2014, 82, 1613–1619. [Google Scholar] [CrossRef]
- Laron, Z.; Kauli, R. Fifty Seven Years of Follow-up of the Israeli Cohort of Laron Syndrome Patients—From Discovery to Treatment. Growth Horm. IGF Res. 2016, 28, 53–56. [Google Scholar] [CrossRef]
- Ashpole, N.M.; Sanders, J.E.; Hodges, E.L.; Yan, H.; Sonntag, W.E. Growth Hormone, Insulin-like Growth Factor-1 and the Aging Brain. Exp. Gerontol. 2015, 68, 76–81. [Google Scholar] [CrossRef]
- Piriz, J.; Muller, A.; Trejo, J.L.; Torres-Aleman, I. IGF-I and the Aging Mammalian Brain. Exp. Gerontol. 2011, 46, 96–99. [Google Scholar] [CrossRef]
- Bartke, A.; Sun, L.Y.; Longo, V. Somatotropic Signaling: Trade-Offs Between Growth, Reproductive Development, and Longevity. Physiol. Rev. 2013, 93, 571–598. [Google Scholar] [CrossRef] [PubMed]
- Frater, J.; Lie, D.; Bartlett, P.; McGrath, J.J. Insulin-like Growth Factor 1 (IGF-1) as a Marker of Cognitive Decline in Normal Ageing: A Review. Ageing Res. Rev. 2018, 42, 14–27. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Domains | ACD | AD | VD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | p for Trend | HR (95% CI) | p | p for Trend | HR (95% CI) | p | p for Trend | |
| Sociodemographic factors | |||||||||
| Favorable | 1(reference) | *** | 1(reference) | *** | 1(reference) | *** | |||
| Intermediate | 1.08(0.99–1.17) | . | 1.27(1.12–1.45) | *** | 1.21(1.02–1.45) | * | |||
| Unfavorable | 1.15(1.09–1.22) | *** | 1.65(1.46–1.87) | *** | 1.58(1.34–1.86) | *** | |||
| Lifestyles | |||||||||
| Favorable | 1(reference) | *** | 1(reference) | *** | 1(reference) | *** | |||
| Intermediate | 1.16(1.08–1.23) | *** | 1.17(1.07–1.29) | ** | 1.13(0.98–1.29) | . | |||
| Unfavorable | 1.37(1.29–1.46) | *** | 1.43(1.27–1.62) | *** | 1.49(1.30–1.70) | *** | |||
| Environment | |||||||||
| Favorable | 1(reference) | *** | 1(reference) | *** | 1(reference) | * | |||
| Intermediate | 1.11(1.04–1.18) | ** | 1.19(1.08–1.32) | *** | 1.20(1.01–1.42) | * | |||
| Unfavorable | 1.15(1.08–1.22) | *** | 1.25(1.13–1.38) | *** | 1.19(1.03–1.37) | * | |||
| Physical measures | |||||||||
| Favorable | 1(reference) | *** | 1(reference) | *** | 1(reference) | ** | |||
| Intermediate | 1.25(1.17–1.33) | *** | 1.14(1.00–1.30) | * | 1.19(1.01–1.40) | * | |||
| Unfavorable | 1.18(1.09–1.28) | *** | 1.28(1.13–1.44) | *** | 1.23(1.07–1.40) | ** | |||
| Blood markers | |||||||||
| Favorable | 1(reference) | *** | 1(reference) | *** | 1(reference) | *** | |||
| Intermediate | 1.19(1.10–1.27) | *** | 1.33(1.20–1.48) | *** | 1.15(0.96–1.38) | ||||
| Unfavorable | 1.44(1.35–1.54) | *** | 1.29(1.17–1.42) | *** | 1.61(1.37–1.90) | *** | |||
| Medical history | |||||||||
| Favorable | 1(reference) | *** | 1(reference) | *** | 1(reference) | *** | |||
| Intermediate | 1.29(1.20–1.40) | *** | 1.27(1.13–1.43) | *** | 1.56(1.25–1.95) | *** | |||
| Unfavorable | 1.88(1.74–2.03) | *** | 1.80(1.54–2.10) | *** | 2.39(2.10–2.71) | *** | |||
| Psychiatric factors | |||||||||
| Favorable | 1(reference) | *** | 1(reference) | *** | 1(reference) | *** | |||
| Intermediate | 1.23(1.07–1.42) | ** | 1.47(1.25–1.72) | *** | |||||
| Unfavorable | 1.61(1.38–1.89) | *** | 1.50(1.18–1.91) | *** | 1.75(1.21–2.53) | ** | |||
| Domains | Age < 65 | Age ≥ 65 | p1 | Female (Aged 56.3 ± 8.0) | Male (Aged 56.7 ± 8.2) | p2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |||
| Sociodemographic factors | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.06 (0.93–1.20) | 1.10 (0.99–1.22) | . | 1.05 (0.93–1.18) | 1.12 (1.00–1.26) | * | ||||
| Unfavorable | 1.20 (1.10–1.31) | *** | 1.13 (1.05–1.22) | ** | 1.24 (1.14–1.34) | *** | 1.08 (1.00–1.17) | * | * | |
| Lifestyles | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.23 (1.11–1.37) | *** | 1.10 (1.01–1.20) | * | * | 1.16 (1.05–1.27) | ** | 1.15 (1.05–1.26) | ** | |
| Unfavorable | 1.52 (1.38–1.67) | *** | 1.26 (1.17–1.37) | *** | *** | 1.39 (1.27–1.52) | *** | 1.34 (1.23–1.46) | *** | |
| Environment | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.03 (0.93–1.15) | 1.15 (1.05–1.25) | ** | 1.10 (1.00–1.21) | * | 1.10 (1.01–1.21) | * | |||
| Unfavorable | 1.14 (1.04–1.25) | ** | 1.15 (1.06–1.24) | *** | 1.22 (1.12–1.33) | *** | 1.08 (1.00–1.18) | . | ||
| Physical measures | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.34 (1.21–1.49) | *** | 1.20 (1.10–1.30) | *** | 1.15 (1.01–1.30) | * | 1.32 (1.22–1.43) | *** | ||
| Unfavorable | 1.28 (1.13–1.45) | *** | 1.13 (1.02–1.25) | * | 1.09 (0.95–1.25) | 1.19 (1.06–1.33) | ** | |||
| Blood markers | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.25 (1.12–1.39) | *** | 1.13 (1.03–1.24) | * | 1.17 (1.05–1.30) | ** | 1.21 (1.10–1.33) | *** | ||
| Unfavorable | 1.60 (1.44–1.78) | *** | 1.33 (1.22–1.46) | *** | . | 1.40 (1.27–1.55) | *** | 1.50 (1.37–1.64) | *** | |
| Medical history | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.48 (1.31–1.67) | *** | 1.20 (1.09–1.32) | *** | ** | 1.36 (1.22–1.52) | *** | 1.23 (1.11–1.37) | *** | |
| Unfavorable | 2.09 (1.85–2.36) | *** | 1.78 (1.61–1.95) | *** | *** | 2.19 (1.95–2.46) | *** | 1.69 (1.53–1.87) | *** | *** |
| Psychiatric factors | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.28 (1.04–1.57) | * | 1.18 (0.96–1.44) | 1.26 (1.05–1.53) | * | 1.17 (0.94–1.47) | ||||
| Unfavorable | 1.72 (1.38–2.16) | *** | 1.48 (1.18–1.86) | *** | . | 1.72 (1.39–2.11) | *** | 1.48 (1.15–1.89) | ** | |
| Domains | Age < 65 | Age ≥ 65 | p1 | Female (Aged 56.3 ± 8.0) | Male (Aged 56.7 ± 8.2) | p2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |||
| Sociodemographic factors | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.50 (1.26–1.78) | *** | 0.99 (0.82–1.19) | *** | 1.21 (1.00–1.46) | * | 1.34 (1.13–1.60) | ** | ||
| Unfavorable | 1.86 (1.58–2.20) | *** | 1.31 (1.10–1.57) | ** | *** | 1.64 (1.38–1.96) | *** | 1.67 (1.41–1.99) | *** | |
| Lifestyles | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.14 (0.98–1.32) | 1.19 (1.05–1.34) | ** | 1.15 (1.00–1.31) | * | 1.20 (1.05–1.37) | ** | |||
| Unfavorable | 1.50 (1.22–1.83) | *** | 1.41 (1.21–1.64) | *** | 1.37 (1.17–1.61) | *** | 1.50 (1.23–1.83) | *** | ||
| Environment | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.12 (0.96–1.31) | 1.25 (1.10–1.41) | *** | 1.18 (1.03–1.35) | * | 1.21 (1.06–1.39) | ** | |||
| Unfavorable | 1.24 (1.06–1.46) | ** | 1.26 (1.11–1.44) | *** | 1.35 (1.18–1.55) | *** | 1.14 (0.99–1.33) | . | ||
| Physical measures | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.20 (0.97–1.48) | . | 1.12 (0.95–1.32) | 2.66 (0.66–10.68) | 1.20 (1.03–1.40) | * | ||||
| Unfavorable | 1.41 (1.16–1.71) | *** | 1.22 (1.05–1.43) | * | 3.07 (0.77–12.31) | 1.26 (1.10–1.44) | *** | |||
| Blood markers | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.34 (1.14–1.58) | *** | 1.34 (1.17–1.52) | *** | 1.35 (1.18–1.54) | *** | 1.37 (1.15–1.64) | *** | ||
| Unfavorable | 1.27 (1.09–1.48) | ** | 1.30 (1.15–1.47) | *** | 1.37 (1.19–1.57) | *** | 1.24 (1.09–1.42) | ** | ||
| Medical history | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.38 (1.14–1.69) | ** | 1.22 (1.05–1.40) | ** | 1.32 (1.12–1.56) | *** | 1.21 (1.03–1.43) | * | ||
| Unfavorable | 1.88 (1.43–2.46) | *** | 1.79 (1.48–2.16) | *** | 2.28 (1.84–2.82) | *** | 1.44 (1.15–1.81) | ** | ** | |
| Psychiatric factors | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Unfavorable | 1.82 (1.26–2.64) | ** | 1.30 (0.95–1.78) | 1.48 (1.10–2.00) | ** | 1.54 (1.03–2.30) | * | |||
| Domains | Age < 65 | Age ≥ 65 | p1 | Female (Aged 56.3 ± 8.0) | Male (Aged 56.7 ± 8.2) | p2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |||
| Sociodemographic factors | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.31 (1.00–1.71) | * | 1.00 (0.80–1.27) | 1.29 (0.96–1.73) | . | 1.19 (0.95–1.48) | ||||
| Unfavorable | 1.95 (1.54–2.47) | *** | 1.22 (0.98–1.51) | . | *** | 1.57 (1.20–2.06) | *** | 1.60 (1.30–1.97) | *** | |
| Lifestyles | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.08 (0.85–1.38) | 1.15 (0.97–1.36) | 1.23 (0.99–1.53) | . | 1.05 (0.87–1.26) | |||||
| Unfavorable | 1.59 (1.27–2.00) | *** | 1.39 (1.17–1.65) | *** | 1.54 (1.24–1.90) | *** | 1.44 (1.21–1.72) | *** | ||
| Environment | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.14 (0.85–1.53) | 1.24 (1.00–1.53) | * | 1.07 (0.82–1.39) | 1.32 (1.06–1.66) | * | ||||
| Unfavorable | 1.19 (0.93–1.52) | 1.19 (0.99–1.43) | . | 1.11 (0.89–1.38) | 1.26 (1.03–1.53) | * | ||||
| Physical measures | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.04 (0.77–1.40) | 1.27 (1.04–1.54) | * | * | 0.95 (0.71–1.26) | 1.31 (1.07–1.60) | ** | |||
| Unfavorable | 1.34 (1.07–1.68) | * | 1.18 (0.99–1.40) | . | 0.98 (0.79–1.21) | 1.42 (1.19–1.69) | *** | ** | ||
| Blood markers | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.31 (0.97–1.77) | . | 1.05 (0.84–1.31) | . | 0.94 (0.72–1.23) | 1.37 (1.07–1.75) | * | . | ||
| Unfavorable | 1.97 (1.50–2.60) | *** | 1.41 (1.15–1.72) | *** | * | 1.51 (1.19–1.92) | *** | 1.74 (1.38–2.18) | *** | |
| Medical history | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.71 (1.18–2.49) | ** | 1.48 (1.12–1.95) | ** | 1.48 (1.04–2.11) | * | 1.64 (1.23–2.18) | *** | ||
| Unfavorable | 3.15 (2.56–3.89) | *** | 2.06 (1.76–2.41) | *** | *** | 2.61 (2.14–3.17) | *** | 2.26 (1.91–2.66) | *** | |
| Psychiatric factors | ||||||||||
| Favorable | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||||
| Intermediate | 1.41 (1.11–1.81) | ** | 1.48 (1.20–1.82) | *** | 1.65 (1.33–2.06) | *** | 1.32 (1.05–1.67) | * | ||
| Unfavorable | 1.97 (1.23–3.16) | ** | 1.30 (0.71–2.36) | *** | 4.32 (2.57–7.26) | *** | 1.05 (0.63–1.76) | * | *** | |
| Domains | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| Unweighted PAF | Communality | Weighted_ PAF | Unweighted PAF | Communality | Weighted_ PAF | |
| Sociodemographic factors | 0.097 | 0.016 | 0.059 | 0.118 | 0.185 | 0.059 |
| Lifestyle | 0.123 | 0.277 | 0.075 | 0.198 | 0.183 | 0.099 |
| Environment | 0.050 | 0.034 | 0.031 | 0.086 | 0.095 | 0.043 |
| Physical measures | 0.035 | 0.190 | 0.021 | 0.148 | 0.388 | 0.074 |
| Blood markers | 0.152 | 0.423 | 0.093 | 0.242 | 0.349 | 0.121 |
| Medical history | 0.080 | 0.404 | 0.049 | 0.119 | 0.292 | 0.059 |
| Psychiatric factors | 0.022 | 0.658 | 0.014 | 0.216 | 0.509 | 0.108 |
| Overall PAF | 0.342 | 0.562 | ||||
| Domains | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| Unweighted PAF | Communality | Weighted_ PAF | Unweighted PAF | Communality | Weighted_ PAF | |
| Sociodemographic factors | 0.177 | 0.287 | 0.112 | 0.292 | 0.394 | 0.155 |
| Lifestyle | 0.045 | 0.291 | 0.029 | 0.099 | 0.159 | 0.052 |
| Environment | 0.054 | 0.056 | 0.034 | 0.090 | 0.008 | 0.048 |
| Physical measures | 0.082 | 0.321 | 0.052 | 0.137 | 0.460 | 0.072 |
| Blood markers | 0.029 | 0.497 | 0.018 | 0.091 | 0.465 | 0.048 |
| Medical history | 0.036 | 0.407 | 0.023 | 0.065 | 0.383 | 0.035 |
| Psychiatric factors | 0.344 | 0.141 | 0.218 | 0.344 | 0.131 | 0.183 |
| Overall PAF | 0.485 | 0.592 | ||||
| Domains | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| Unweighted PAF | Communality | Weighted_ PAF | Unweighted PAF | Communality | Weighted_ PAF | |
| Sociodemographic factors | 0.224 | 0.186 | 0.117 | 0.322 | 0.268 | 0.144 |
| Lifestyle | 0.161 | 0.305 | 0.084 | 0.248 | 0.305 | 0.111 |
| Environment | 0.086 | 0.234 | 0.045 | 0.213 | 0.186 | 0.096 |
| Physical measures | 0.141 | 0.277 | 0.073 | 0.184 | 0.170 | 0.082 |
| Blood markers | 0.295 | 0.308 | 0.153 | 0.389 | 0.267 | 0.174 |
| Medical history | 0.220 | 0.300 | 0.114 | 0.255 | 0.311 | 0.115 |
| Psychiatric factors | 0.014 | 0.390 | 0.007 | 0.052 | 0.493 | 0.023 |
| Overall PAF | 0.593 | 0.746 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, X.; Gao, H.; Wu, Y.; Zhu, X.; Wu, S.; Lin, L. Investigating Modifiable Risk Factors Across Dementia Subtypes: Insights from the UK Biobank. Biomedicines 2024, 12, 1967. https://doi.org/10.3390/biomedicines12091967
Ma X, Gao H, Wu Y, Zhu X, Wu S, Lin L. Investigating Modifiable Risk Factors Across Dementia Subtypes: Insights from the UK Biobank. Biomedicines. 2024; 12(9):1967. https://doi.org/10.3390/biomedicines12091967
Chicago/Turabian StyleMa, Xiangge, Hongjian Gao, Yutong Wu, Xinyu Zhu, Shuicai Wu, and Lan Lin. 2024. "Investigating Modifiable Risk Factors Across Dementia Subtypes: Insights from the UK Biobank" Biomedicines 12, no. 9: 1967. https://doi.org/10.3390/biomedicines12091967
APA StyleMa, X., Gao, H., Wu, Y., Zhu, X., Wu, S., & Lin, L. (2024). Investigating Modifiable Risk Factors Across Dementia Subtypes: Insights from the UK Biobank. Biomedicines, 12(9), 1967. https://doi.org/10.3390/biomedicines12091967