1. Introduction
Gamma-glutamyltransferase (γ-GT) is a glycoprotein located on the plasma membranes of most cells and organ tissues, especially of hepatocytes. It is involved in the extracellular catabolism of glutathione, recognized as the major thiol antioxidant in humans and other mammals. An increase in serum γ-GT levels >50 IU/mL is seen as a consequence of liver injury or bile ducts blockage. In clinical practice, serum γ-GT levels are routinely measured when hepatic/biliary disease and/or alcohol abuse are suspected [
1], and it has recently been recognized as a risk factor for metabolic alterations [
2], and chronic renal [
3] and cardiovascular diseases (CV) [
4,
5,
6,
7]. These effects seem to be mediated by the capacity of γ-GT to increase the production of reactive oxygen species (ROS) in the presence of some transition metal such as iron [
4,
8]. Thus, on the basis of these findings and of other epidemiological studies, it was suggested to consider γ-GT, within its normal range, as an early and sensitive biomarker of oxidative stress [
9]. In fact, subclinical inflammation related to oxidative stress is considered as the main pathogenetic mechanism involved in several cardio-metabolic diseases [
10].
It is well established that endothelial dysfunction, an early event in the atherogenic process, is associated with some metabolic and hemodynamic [
11,
12,
13,
14] risk factors (i.e., arterial hypertension, obesity, etc.) sharing the same pathogenetic mechanisms, represented by an increased oxidative stress and subclinical inflammation. The activation of these pro-oxidant and pro-inflammatory pathways leads to the activation and progression of atherosclerotic disease by reducing nitric oxide (NO) bioavailability and its protective effect on vascular function [
15,
16]. In addition, it is important to remark that endothelial dysfunction has been demonstrated to predict the progression of subclinical target organ damage [
17,
18,
19]; on this basis, it is possible to affirm that endothelial dysfunction has a key role in the pathogenetic mechanisms of CV diseases and associated outcomes [
14]. Even if the association between essential hypertension and endothelial dysfunction is well established, to our knowledge there are no data testing a possible relationship between serum γ-GT concentrations and endothelial function in this setting of patients. Thus, we designed the present study to evaluate a possible association between serum γ-GT concentrations, within its normal range, and endothelium-dependent vasodilation, evaluated by strain-gauge plethysmography, in a large population of newly diagnosed, never-treated hypertensive patients.
2. Experimental Section
For this study we enrolled 500 Caucasian hypertensive outpatients (256 men and 244 women; mean age, 47 ± 11 years) referred to the Hypertension Clinic of the University Hospital of Catanzaro, Italy. Exclusion criteria were secondary forms of hypertension, clinical evidence or previous history of coronary artery disease, valvular heart disease, peripheral artery disease, diabetes mellitus, hypercholesterolemia, liver diseases, impaired renal function (defined as an estimated glomerular filtration rate [e-GFR] <60 mL/min per 1.73 m2), coagulopathies, vasculitis and/or Raynaud’s phenomenon, history of alcohol and/or drug abuse, and the use of drugs interfering with liver enzyme concentrations. To enter the study protocol, all subjects had to have serum values of alanine aminotransferase (ALT), aspartate aminotransferase (AST), and γ-GT in the normal range; in particular, we considered 50 IU/mL as the upper normal limit for all these three variables, as established by our laboratory. At the first evaluation, all subjects underwent routine blood tests, assessment of risk factors for atherosclerosis, and evaluation of vascular function through strain-gauge plethysmography. ALT and AST were measured by pyridoxal phosphate activated (liquid reagent) (COBAS Integra 800—Roche Diagnostics GmbH, Mannheim, Germany; normal values 0–50 UI/L), γ-GT was evaluated by standardized against Szasz (COBAS Integra 800—Roche Diagnostics GmbH, Mannheim, Germany; normal values 8–50 UI/L).
High-sensitivity C-reactive protein (hs-CRP) was measured by a high-sensitivity turbidimetric immunoassay (Cardio-Phase hs-CRP, Siemens Healthcare Diagnostics GmbH, Marburg, Germany) in a subgroup of 400 patients representative of the whole study population with regard to the variables listed in
Table 1.
The local ethics committee approved the study (approval number 2012.63, 23 October 2012—Comitato Etico Azienda Ospedaliero-Universitaria Mater Domini of Catanzaro, Italy), and all participants gave written informed consent for all procedures. All the study procedures were conducted according to the Declaration of Helsinki.
2.1. Vascular Function Evaluation
Vascular function evaluation was made at 09:00 a.m. in a quiet and air-conditioned room (22–24 °C) with the fasting subjects lying supine. Forearm volume was determined by water displacement. A 20-gauge polyethylene catheter (Vasculon 2; Baxter Healthcare, Deerfield, IL, USA), introduced into the brachial artery of the non-dominant arm, was used for evaluation of blood pressure (BP) and for drug administration. Measurement of percent change in forearm volume was obtained by a mercury-filled silastic strain gauge placed on the widest part of the forearm, connected to a plethysmograph (model EC-4; DE Hokanson, Issaquah, WA, USA) that was connected to a chart recorder for detection of forearm blood flow (FBF) measurements. Exclusion of peripheral venous outflow was obtained by inflating to 40 mmHg a cuff placed on the upper arm with a rapid cuff inflator (model E-10; DE Hokanson, Issaquah, WA, USA). FBF was calculated as the slope of the change in forearm volume; the mean of 3 measurements was obtained at each time point.
For the evaluation of endothelial function, we used the protocol initially described by Panza et al. [
12] and subsequently used by us [
13,
14,
17,
18]. Endothelium-dependent and endothelium-independent vasodilation was assessed by a dose–response curve during intra-arterial infusions of acetylcholine (ACh) (7.5, 15, and 30 μg/mL per minute, each for 5 min) and sodium nitroprusside (SNP) (0.8, 1.6, and 3.2 μg/mL per minute, each for 5 min), respectively. Prior to the administration, ACh (Sigma, Milan, Italy) was diluted with saline and SNP (Malesci, Florence, Italy) in 5% glucose solution, and protected from light with aluminum foil.
2.2. Statistical Analysis
Data are reported as mean ± SD or as percent frequency; we used t-test or the χ2 test, as appropriate, for comparisons between groups. Relationships between paired parameters were tested by correlation coefficient of Pearson. Multivariate models (linear or logistic regression) were constructed using, as independent covariates, several traditional CV risk factors—age, gender, body mass index, glucose, LDL and HDL cholesterol, triglyceride, BP, smoking, and e-GFR—to test the independent relationship between γ-GT and the response to ACh. In an additional analysis, we tested the potential confounding effect of hs-CRP in a subgroup of 400 patients.
In the logistic regression analysis, endothelial dysfunction, as dichotomic variable, was expressed as a maximal response to ACh < 400% as previously reported [
17,
18].
In multiple linear regression models, data were expressed as standardized regression coefficient (beta) and p value. In multiple logistic regression analyses, data were expressed as odds ratio (OR), 95% confidence interval (CI), and p value.
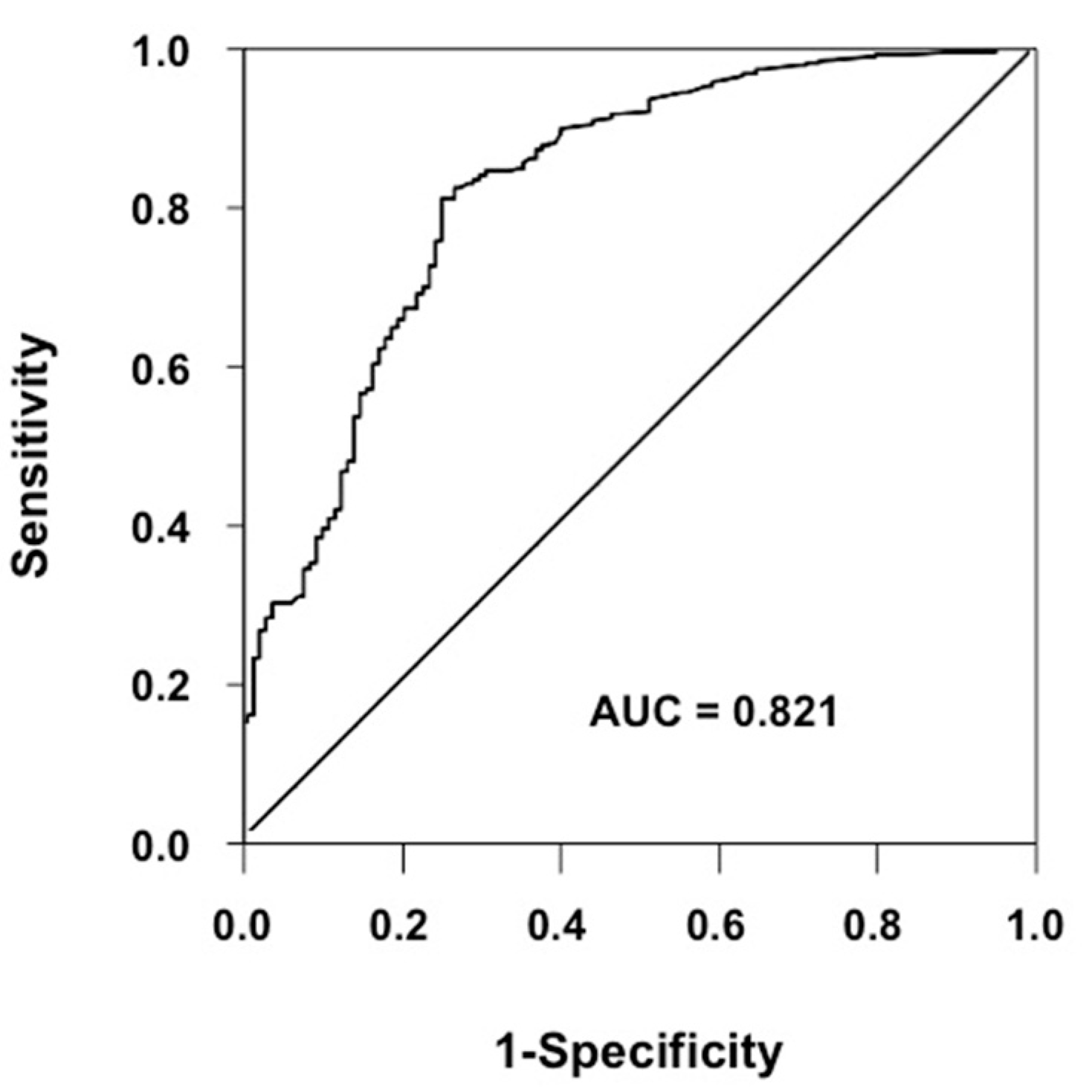
Receiver operating characteristic (ROC) analysis was used to assess the predictive value of γ-GT (area under the curve) and to identify the optimal cut-off value of the same variable for endothelial dysfunction, i.e., the value which maximizes the difference between true positive and false positive rates of endothelial dysfunction.
To assess the internal consistency of study results, a sensitivity analysis was performed by randomly dividing the whole study population into two equally sized subgroups.
All calculations were made with a standard statistical package (SPSS for Windows version 20.0; SPSS, Inc., Chicago, IL, USA).
4. Discussion
To our knowledge, findings obtained in this study demonstrate, for the first time, the association between serum γ-GT within the normal range and endothelial dysfunction, evaluated by strain-gauge plethysmography, in a very large and well-characterized population of never-treated hypertensive patients. Particularly, the risk of endothelial dysfunction increases by 93% for each 10 IU/L elevation of this enzyme (
Table 4).
It is well established that the primary role of γ-GT is to contribute to the maintenance of intracellular homeostasis of glutathione (GSH), one of the major intracellular antioxidant components [
20], even if some experimental findings demonstrated that, in the presence of iron or other transition metals, it might also be involved in the generation of ROS [
9]. Thus, on the basis of this evidence, γ-GT emerged over time as an early and sensitive enzyme related to oxidative stress. In fact, its circulating levels, within normal range, resulted in the increase of F2-isoprostanes, fibrinogen, and CRP, all markers of systemic inflammation [
9]. Interestingly, this association was observed independently of the presence of metabolic alterations, typically related to γ-GT elevation [
5,
21]. Consistent with these findings, we also observed a significant relationship between γ-GT and hs-CRP, confirming previously published data suggesting that elevation of γ-GT is involved in the subclinical inflammatory response and oxidative stress [
22], both conditions associated with endothelial dysfunction [
13,
23].
Another important finding of this study is that ALT levels, within the normal range, are also significantly associated with endothelial function. Particularly, the increase of 10 IU/L of ALT almost doubles the risk of endothelial dysfunction, as reported in
Table 4. Although a significant relationship between γ-GT values within the normal range and the incidence of chronic elevation of ALT was previously reported [
24], no data are available to demonstrate a possible pathogenetic role of ALT in the activation of an oxidative stress process. Although γ-GT can be considered as an early biomarker of systemic and hepatic oxidative stress, ALT elevation might reflect possible inflammatory liver damage as a consequence of this increased oxidative stress. In accordance with this, we previously reported that hypertensive patients with both metabolic syndrome and non-alcoholic fatty liver disease (NAFLD) had a reduced endothelium-dependent vasodilation in comparison with hypertensives with metabolic syndrome without NAFLD [
25]. Serum ALT values were significantly higher in hypertensives with NAFLD than in those without (42.0 + 10.8 vs. 24.6 + 5.2 UI/L), leading to the hypothesis that NAFLD—and the associated elevation of ALT levels—could be considered as an early biomarker of endothelial dysfunction.

 ,
, 



{kind=link}