
The Visceral Adiposity Index in Non-Alcoholic Fatty Liver Disease and Liver Fibrosis—Systematic Review and Meta-Analysis

 , , , and
, , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Risk of Bias Assessment in Individual Studies
2.4. Summary Measures and Synthesis of Results
2.5. Publication Bias, Sensitivity Analyses, and Meta-Regression
3. Results
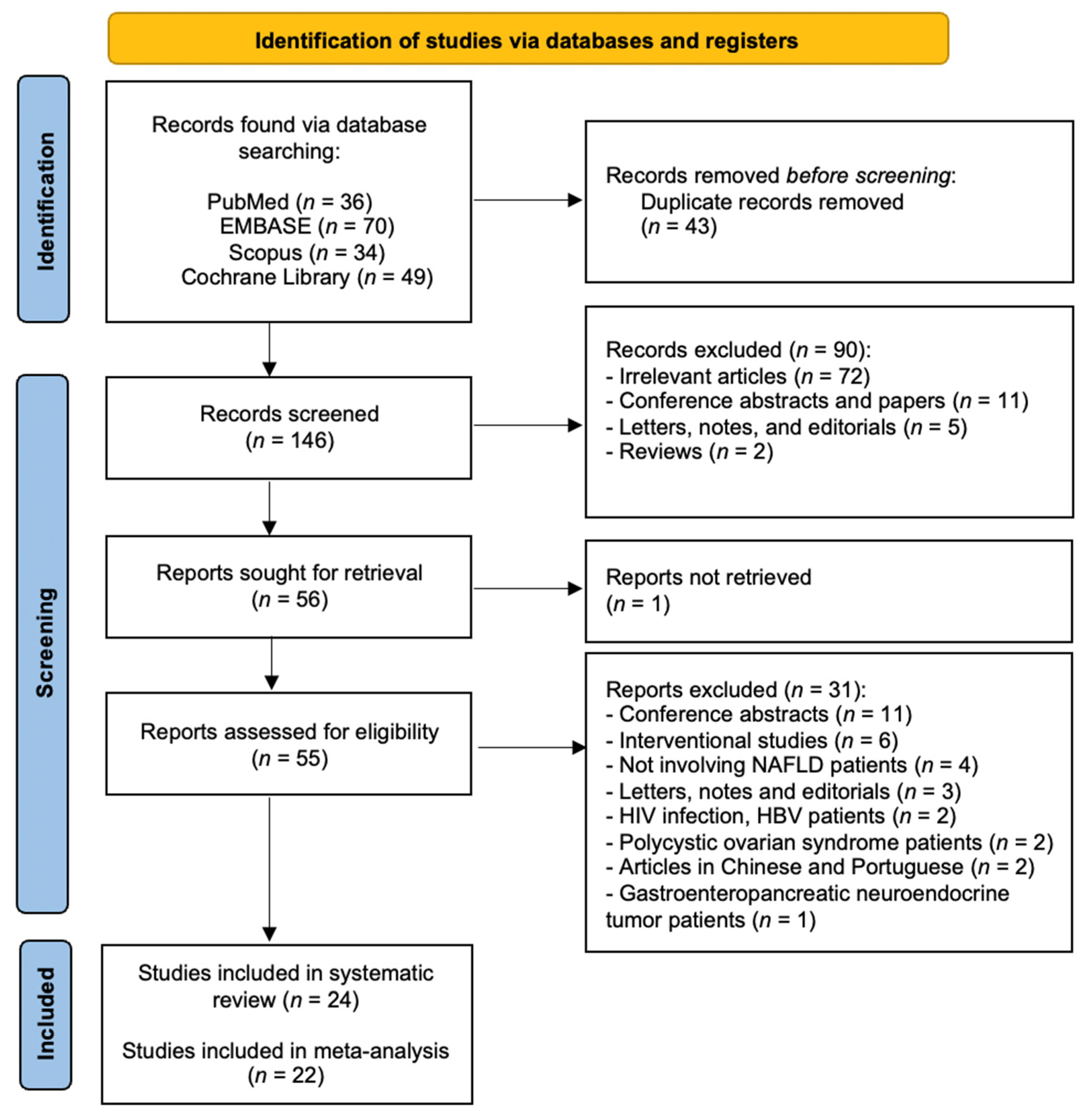
3.1. General Results
3.2. Study Characteristics
3.3. Definition of NAFLD
3.4. The VAI and NAFLD
3.5. The VAI and NASH
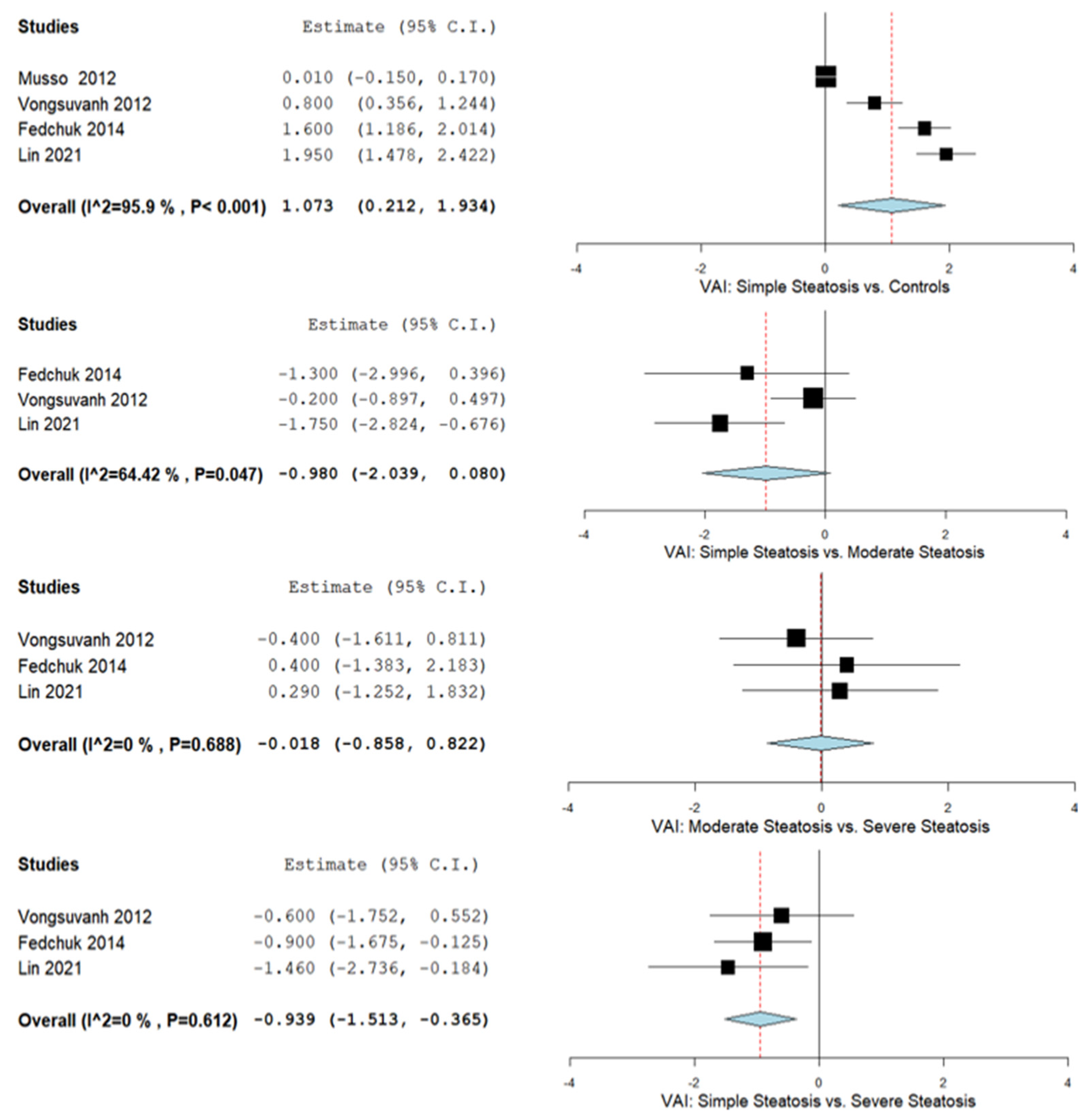
3.6. The VAI and Hepatic Steatosis Severity
3.7. The VAI and Liver Fibrosis
3.8. The VAI and Diabetic/Prediabetic NAFLD Patients
3.9. The VAI and Males and Females
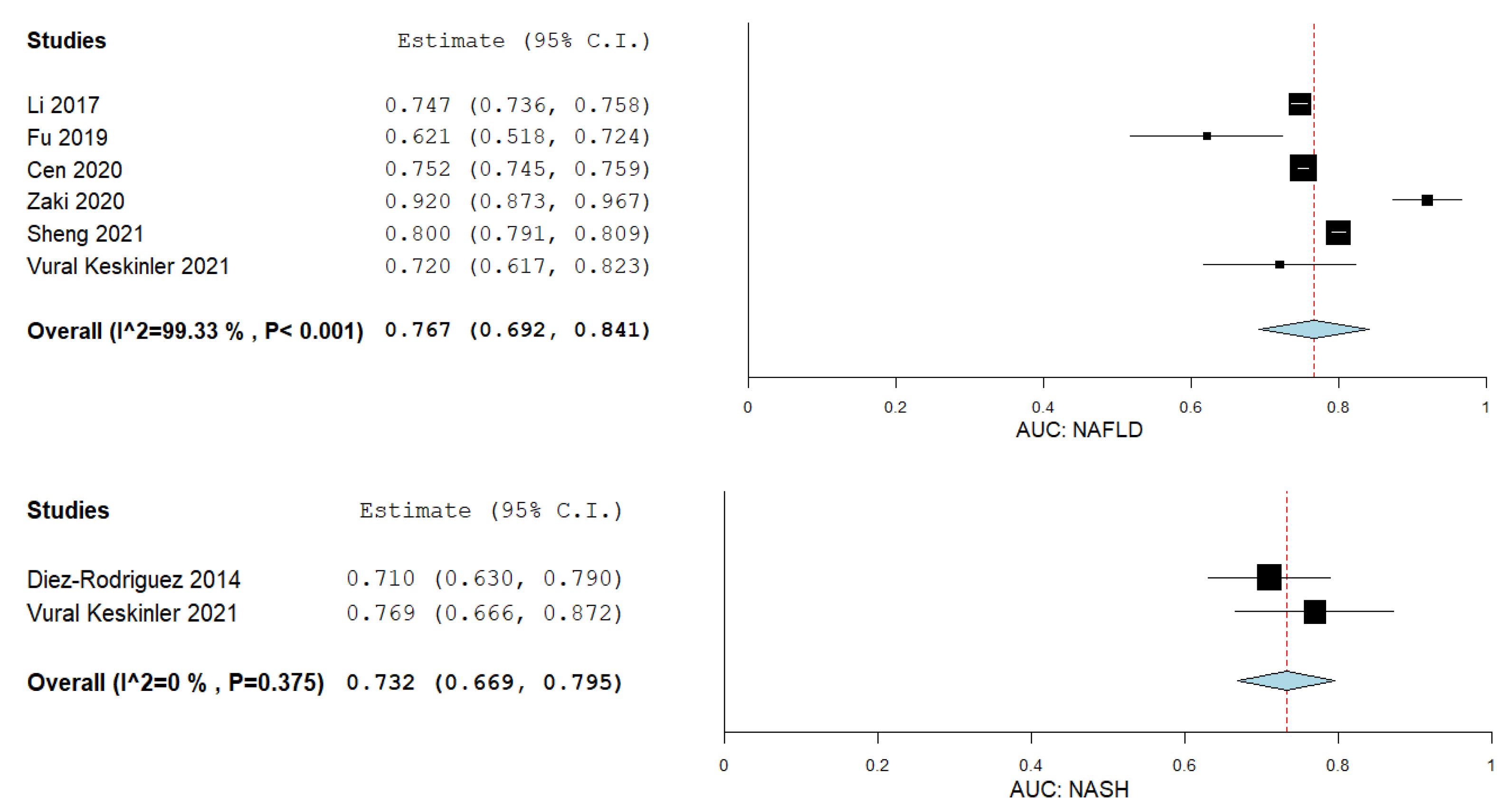
3.10. VAI in Predicting NAFLD and NASH
3.11. Publication Bias, Sensitivity Analyses, and Meta-Regression
3.12. Bias Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sporea, I.; Popescu, A.; Dumitrascu, D.; Brisc, C.; Nedelcu, L.; Trifan, A.; Gheorghe, L.; Fierbinteanu Braticevici, C. Nonalcoholic Fatty Liver Disease: Status Quo. J. Gastrointestin. Liver Dis. 2018, 27, 439–448. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Söderberg, C.; Stål, P.; Askling, J.; Glaumann, H.; Lindberg, G.; Marmur, J.; Hultcrantz, R. Decreased survival of subjects with elevated liver function tests during a 28-year follow-up. Hepatology 2010, 51, 595–602. [Google Scholar] [CrossRef] [Green Version]
- Ekstedt, M.; Franzén, L.E.; Mathiesen, U.L.; Thorelius, L.; Holmqvist, M.; Bodemar, G.; Kechagias, S. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006, 44, 865–873. [Google Scholar] [CrossRef]
- Angulo, P. Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2002, 346, 1221–1231. [Google Scholar] [CrossRef] [Green Version]
- Musso, G.; Gambino, R.; Cassader, M.; Pagano, G. Meta-analysis: Natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of noninvasive tests for liver disease severity. Ann. Med. 2011, 43, 617–649. [Google Scholar] [CrossRef]
- Musso, G.; Gambino, R.; Tabibian, J.H.; Ekstedt, M.; Kechagias, S.; Hamaguchi, M.; Hultcrantz, R.; Hagström, H.; Yoon, S.K.; Charatcharoenwitthaya, P.; et al. Association of Non-alcoholic Fatty Liver Disease with Chronic Kidney Disease: A Systematic Review and Meta-analysis. PLoS Med. 2014, 11, e1001680. [Google Scholar] [CrossRef] [Green Version]
- FAN, J.-G.; ZHU, J.; LI, X.-J.; CHEN, L.; LU, Y.-S.; LI, L.; DAI, F.; LI, F.; CHEN, S.-Y. Fatty liver and the metabolic syndrome among Shanghai adults. J. Gastroenterol. Hepatol. 2005, 20, 1825–1832. [Google Scholar] [CrossRef]
- Yang, K.C.; Hung, H.-F.; Lu, C.-W.; Chang, H.-H.; Lee, L.-T.; Huang, K.-C. Association of Non-alcoholic Fatty Liver Disease with Metabolic Syndrome Independently of Central Obesity and Insulin Resistance. Sci. Rep. 2016, 6, 27034. [Google Scholar] [CrossRef] [Green Version]
- Vanni, E.; Bugianesi, E.; Kotronen, A.; De Minicis, S.; Yki-Järvinen, H.; Svegliati-Baroni, G. From the metabolic syndrome to NAFLD or vice versa? Dig. Liver Dis. 2010, 42, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.H.; Park, C.E.; Gi, M.Y.; Cha, J.A.; Moon, A.E.; Kang, J.K.; Seong, J.M.; Lee, J.H.; Yoon, H. The association of the visceral adiposity index with insulin resistance and beta-cell function in Korean adults with and without type 2 diabetes mellitus. Endocr. J. 2020, 67, 613–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, M.C.; Pizzolanti, G.; Torregrossa, V.; Misiano, G.; Milano, S.; Giordano, C. Visceral Adiposity Index (VAI) Is Predictive of an Altered Adipokine Profile in Patients with Type 2 Diabetes. PLoS ONE 2014, 9, e91969. [Google Scholar] [CrossRef] [Green Version]
- Visceral Fat and Adiponectin: Associations with Insulin Resistance Are Tissue-Specific in Women. Metab. Syndr. Relat. Disord. 2009, 7, 61–67. [CrossRef]
- Ando, Y.; Jou, J.H. Nonalcoholic Fatty Liver Disease and Recent Guideline Updates. Clin. Liver Dis. 2021, 17, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Actis, G.C.; Olivero, A.; Lagget, M.; Pellicano, R.; Smedile, A.; Rizzetto, M. The Practice of Percutaneous Liver Biopsy in a Gastrohepatology Day Hospital: A Retrospective Study on 835 Biopsies. Dig. Dis. Sci. 2007, 52, 2576–2579. [Google Scholar] [CrossRef]
- Monelli, F.; Venturelli, F.; Bonilauri, L.; Manicardi, E.; Manicardi, V.; Rossi, P.G.; Massari, M.; Ligabue, G.; Riva, N.; Schianchi, S.; et al. Systematic review of existing guidelines for NAFLD assessment. Hepatoma Res. 2021, 7, 25. [Google Scholar] [CrossRef]
- Shen, J.; Chan, H.L.-Y.; Wong, G.L.-H.; Chan, A.W.-H.; Choi, P.C.-L.; Chan, H.-Y.; Chim, A.M.-L.; Yeung, D.K.-W.; Yu, J.; Chu, W.C.-W.; et al. Assessment of non-alcoholic fatty liver disease using serum total cell death and apoptosis markers. Aliment. Pharmacol. Ther. 2012, 36, 1057–1066. [Google Scholar] [CrossRef] [Green Version]
- Chan, W.-K.; Sthaneshwar, P.; Nik Mustapha, N.R.; Mahadeva, S. Limited Utility of Plasma M30 in Discriminating Non-Alcoholic Steatohepatitis from Steatosis—A Comparison with Routine Biochemical Markers. PLoS ONE 2014, 9, e105903. [Google Scholar] [CrossRef] [PubMed]
- Leoni, S.; Tovoli, F.; Napoli, L.; Serio, I.; Ferri, S.; Bolondi, L. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World J. Gastroenterol. 2018, 24, 3361–3373. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A.; for the AlkaMeSy Study Group. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920. [Google Scholar] [CrossRef] [Green Version]
- Kouli, G.M.; Panagiotakos, D.B.; Kyrou, I.; Georgousopoulou, E.N.; Chrysohoou, C.; Tsigos, C.; Tousoulis, D.; Pitsavos, C. Visceral adiposity index and 10-year cardiovascular disease incidence: The ATTICA study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Bijari, M.; Jangjoo, S.; Emami, N.; Raji, S.; Mottaghi, M.; Moallem, R.; Jangjoo, A.; Saberi, A. The Accuracy of Visceral Adiposity Index for the Screening of Metabolic Syndrome: A Systematic Review and Meta-Analysis. Int. J. Endocrinol. 2021, 2021, 6684627. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ismaiel, A.; Jaaouani, A.; Leucuta, D.-C.; Popa, S.-L.; Dumitrascu, D.L. The Visceral Adiposity Index in Non-Alcoholic Fatty Liver Disease and Liver Fibrosis—Systematic Review and Meta Analysis. Inplasy protocol 2021, 12, 56. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; The QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Obuchowski, N.A.; Lieber, M.L.; Wians, F.H., Jr. ROC Curves in Clinical Chemistry: Uses, Misuses, and Possible Solutions. Clin. Chem. 2004, 50, 1118–1125. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. Dmetar: Companion R Package for The Guide ‘Doing Meta-Analysis in R’. 2019. Available online: https://dmetar.protectlab.org/ (accessed on 1 November 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dynnyk, N.; Svintsitsky, A.; Solovyova, G.; Bogomaz, V.; Baka, O.; Gurbych, O.; Golovchanska, Y. Physical activity reduce hepatic apoptosis in patients with non-alcoholic fatty liver disease and visceral obesity. J. Hepatol. 2016, 64, S491. [Google Scholar] [CrossRef]
- Elsaid, M.; Li, Y.; John, T.; Catalano, C.; Rustgi, V.K. Racial and gender disparities in the relationship between non-alcoholic fatty liver disease and visceral adipose dysfunction. Hepatology 2019, 70, 738A–739A. [Google Scholar]
- Ercin, C.N.; Dogru, T.; Genc, H.; Celebi, G.; Aslan, F.; Gurel, H.; Kara, M.; Sertoglu, E.; Tapan, S.; Bagci, S.; et al. Insulin resistance but not visceral adiposity index is associated with liver fibrosis in nondiabetic subjects with nonalcoholic fatty liver disease. Hepatol. Int. 2015, 9, S369. [Google Scholar] [CrossRef] [PubMed]
- Ercin, C.N.; Dogru, T.; Tapan, S.; Genc, H.; Aslan, F.; Çelebi, G.; Kara, M.; Sertoglu, E.; Karslioglu, Y.; Kurt, I.; et al. Visceral adiposity index in nonalcoholic fatty liver disease: Association with hepatic and systemic inflammation. Biochim. Clin. 2013, 37, S677. [Google Scholar]
- Keating, S.; Parker, H.; Hickman, I.; Wallen, M.; George, J.; Johnson, N. Can equation-based indices be used to detect longitudinal change in 1h-MRS quantified intra-hepatic lipid in clinical practice? Inflamm. Intest. Dis. 2017, 2, 5. [Google Scholar] [CrossRef]
- Kondo, T.; Kitano, S.; Miyakawa, N.; Watanabe, T.; Goto, R.; Sakaguchi, M.; Igata, M.; Kawashima, J.; Motoshima, H.; Matsumura, T.; et al. Activation of heat shock response ameliorates nonalcoholic fatty liver disease biomarkers. Diabetes 2020, 69. [Google Scholar] [CrossRef]
- Kouvari, M.; Panagiotakos, D.; Chrysohoou, C.; Georgousopoulou, E.; Tousoulis, D.; Pitsavos, C. Visceral adiposity index, non-alcoholic fatty liver disease and 10-year cardiovascular disease incidence: A gender-based analysis from the attica prospective (2002–2012) study. J. Am. Coll. Cardiol. 2020, 75, 1905. [Google Scholar] [CrossRef]
- Nascimbeni, F.; Fedchuk, L.; Pais, R.; Charlotte, F.; Housset, C.; Loria, P.; Ratziu, V. Performance and limitations of five steatosis biomarkers in patients with Non-alcoholic Fatty Liver Disease. Hepatology 2014, 60, 622A. [Google Scholar] [CrossRef] [Green Version]
- Petta, S.; Amato, M.; Di Marco, V.; Cammà, C.; Pizzolanti, G.; Rosa Barcellona, M.; Cabibi, D.; Galluzzo, A.; Sinagra, D.; Giordano, C.; et al. Visceral adiposity index is associated with significant fibrosis in patients with nonalcoholic fatty liver disease. Hepatology 2011, 54, 1131A. [Google Scholar] [CrossRef]
- Petta, S.; Amato, M.; Licata, G.; Barcellona, M.; Cammà, C.; Cabibi, D.; Di Marco, V.; Giordano, C.; Sinagra, D.; Galluzzo, A.; et al. Visceral adiposity index, expression of adipose dysfunction, is associated with significant fibrosis in patients with non-alcoholic fatty liver disease. Dig. Liver Dis. 2011, 43, S83. [Google Scholar] [CrossRef]
- Vongsuvanh, R.; George, J.; Van Der Poorten, D. Visceral adiposity index is not a predictor of liver histology in patients with nonalcoholic fatty liver disease. J. Gastroenterol. Hepatol. 2011, 26, 45. [Google Scholar] [CrossRef]
- Filik, L. Visceral adiposity index and exercise in non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2012, 35, 489. [Google Scholar] [CrossRef]
- Li, Y.; Liu, L.; Wang, B.; Chen, D. Letter: Is visceral adiposity index a predictor of liver histology in patients with non-alcoholic fatty liver disease? Aliment. Pharmacol. Ther. 2013, 37, 583. [Google Scholar] [CrossRef] [PubMed]
- Petta, S.; Craxì, A. Visceral adiposity index and exercise in non-alcoholic fatty liver disease: Authors’ reply. Aliment. Pharmacol. Ther. 2012, 35, 490. [Google Scholar] [CrossRef]
- Barrea, L.; Annunziata, G.; Muscogiuri, G.; Di Somma, C.; Laudisio, D.; Maisto, M.; de Alteriis, G.; Tenore, G.C.; Colao, A.; Savastano, S. Trimethylamine-N-oxide (TMAO) as Novel Potential Biomarker of Early Predictors of Metabolic Syndrome. Nutrients 2018, 10, 1971. [Google Scholar] [CrossRef] [Green Version]
- Ibarra-Reynoso, L.D.R.; Pisarchyk, L.; Pérez-Luque, E.L.; Garay-Sevilla, M.E.; Malacara, J.M. Whole-body and hepatic insulin resistance in obese children. PLoS ONE 2014, 9, e113576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loureiro, L.M.; Cordeiro, A.; Mendes, R.; Luna, M.; Pereira, S.; Saboya, C.J.; Ramalho, A. Clinic, anthropometric and metabolic changes in adults with class III obesity classified as metabolically healthy and metabolically unhealthy. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2419–2431. [Google Scholar] [CrossRef] [Green Version]
- Vassilatou, E.; Lafoyianni, S.; Vassiliadi, D.A.; Ioannidis, D.; Paschou, S.A.; Mizamtsidi, M.; Panagou, M.; Vryonidou, A. Visceral adiposity index for the diagnosis of nonalcoholic fatty liver disease in premenopausal women with and without polycystic ovary syndrome. Maturitas 2018, 116, 1–7. [Google Scholar] [CrossRef]
- Reeds, D.N.; Chambers, K.T.; Patterson, B.W.; Finck, B.N. Intrahepatic triglyceride is more strongly associated with insulin-resistant glucose metabolism than visceral adiposity in HIV, and is improved with tauroursodeoxycholic acid treatment. Antivir. Ther. 2017, 22, A27. [Google Scholar]
- Sterling, R.K.; King, W.C.; Khalili, M.; Kleiner, D.E.; Hinerman, A.S.; Sulkowski, M.; Chung, R.T.; Jain, M.K.; Lisker-Melman, M.; Wong, D.K.; et al. Performance of Serum-Based Scores for Identification of Mild Hepatic Steatosis in HBV Mono-infected and HBV–HIV Co-infected Adults. Dig. Dis. Sci. 2021, 1–13. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Modica, R.; Altieri, B.; Pugliese, G.; Minotta, R.; Faggiano, A.; Colao, A.; Savastano, S. Cardio-Metabolic Indices and Metabolic Syndrome as Predictors of Clinical Severity of Gastroenteropancreatic Neuroendocrine Tumors. Front. Endocrinol. 2021, 12, 649496. [Google Scholar] [CrossRef]
- Xu, C.; Ma, Z.; Wang, Y.; Liu, X.; Tao, L.; Zheng, D.; Guo, X.; Yang, X. Visceral adiposity index as a predictor of NAFLD: A prospective study with 4-year follow-up. Liver Int. 2018, 38, 2294–2300. [Google Scholar] [CrossRef]
- Balducci, S.; Cardelli, P.; Pugliese, L.; D’Errico, V.; Haxhi, J.; Alessi, E.; Iacobini, C.; Menini, S.; Bollanti, L.; Conti, F.G.; et al. Volume-dependent effect of supervised exercise training on fatty liver and visceral adiposity index in subjects with type 2 diabetes The Italian Diabetes Exercise Study (IDES). Diabetes Res. Clin. Pract. 2015, 109, 355–363. [Google Scholar] [CrossRef]
- Della Pepa, G.; Russo, M.; Vitale, M.; Carli, F.; Vetrani, C.; Masulli, M.; Riccardi, G.; Vaccaro, O.; Gastaldelli, A.; Rivellese, A.A.; et al. Pioglitazone even at low dosage improves NAFLD in type 2 diabetes: Clinical and pathophysiological insights from a subgroup of the TOSCA.IT randomised trial. Diabetes Res. Clin. Pract. 2021, 178, 108984. [Google Scholar] [CrossRef]
- Ebrahimi, S.; Gargari, B.P.; Aliasghari, F.; Asjodi, F.; Izadi, A. Ramadan fasting improves liver function and total cholesterol in patients with nonalcoholic fatty liver disease. Int. J. Vitam. Nutr. Res. 2020, 90, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Gelli, C.; Tarocchi, M.; Abenavoli, L.; Di Renzo, L.; Galli, A.; De Lorenzo, A. Effect of a counseling-supported treatment with the Mediterranean diet and physical activity on the severity of the non-alcoholic fatty liver disease. World J. Gastroenterol. 2017, 23, 3150–3162. [Google Scholar] [CrossRef]
- Montesi, L.; Caselli, C.; Centis, E.; Nuccitelli, C.; Moscatiello, S.; Suppini, A.; Marchesini, G. Physical activity support or weight loss counseling for nonalcoholic fatty liver disease? World J. Gastroenterol. 2014, 20, 10128–10136. [Google Scholar] [CrossRef]
- Reginato, E.; Pippi, R.; Aiello, C.; Tomaro, E.S.; Ranucci, C.; Buratta, L.; Bini, V.; Marchesini, G.; De Feo, P.; Fanelli, C. Effect of short term intensive lifestyle intervention on hepatic steatosis indexes in adults with obesity and/or type 2 diabetes. J. Clin. Med. 2019, 8, 851. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.I.G.; Guedes, S.E.M.; Cunha, B.E.S.; Tomiya, M.T.O.; da Silva, A.M.D.; de Brito, C.A. Sociodemographic and nutritional parameters of carriers of non-alcoholic fatty liver disease. Acta Gastroenterol. Latinoam. 2019, 49, 132–142. [Google Scholar]
- Qi, J.; Lin, Q.; Lin, X.; Chen, X. Relationship of visceral adiposity index with serum aminotransferase and nonalcoholic fatty liver disease in patients with sleep apnea. Zhonghua Yi Xue Za Zhi 2015, 95, 3420–3423. [Google Scholar] [PubMed]
- Cen, C.; Wang, W.; Yu, S.; Tang, X.; Liu, J.; Liu, Y.; Zhou, L.; Yu, J.; Zheng, S. Development and validation of a clinical and laboratory-based nomogram to predict nonalcoholic fatty liver disease. Hepatol. Int. 2020, 14, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Coccia, F.; Testa, M.; Guarisco, G.; Bonci, E.; Di Cristofano, C.; Silecchia, G.; Leonetti, F.; Gastaldelli, A.; Capoccia, D. Noninvasive assessment of hepatic steatosis and fibrosis in patients with severe obesity. Endocrine 2020, 67, 569–578. [Google Scholar] [CrossRef]
- Díez-Rodríguez, R.; Ballesteros-Pomar, M.D.; Calleja-Fernández, A.; González-De-Francisco, T.; González-Herráez, L.; Calleja-Antolín, S.; Cano-Rodríguez, I.; Olcoz-Goñi, J.L. Insulin resistance and metabolic syndrome are related to non-alcoholic fatty liver disease, but not visceral adiposity index, in severely obese patients. Rev. Esp. Enferm. Dig. 2014, 106, 522–528. [Google Scholar] [PubMed]
- Ebrahimi, R.; Shanaki, M.; Mohassel Azadi, S.; Bahiraee, A.; Radmard, A.R.; Poustchi, H.; Emamgholipour, S. Low level of adiponectin predicts the development of Nonalcoholic fatty liver disease: Is it irrespective to visceral adiposity index, visceral adipose tissue thickness and other obesity indices? Arch. Physiol. Biochem. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Eremić-Kojić, N.; Đerić, M.; Govorčin, M.L.; Balać, D.; Kresoja, M.; Kojić-Damjanov, S. Assessment of hepatic steatosis algorithms in non-alcoholic fatty liver disease. Hippokratia 2018, 22, 10–16. [Google Scholar]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
- Feng, R.N.; Du, S.S.; Wang, C.; Li, Y.C.; Liu, L.Y.; Guo, F.C.; Sun, C.H. Lean-non-alcoholic fatty liver disease increases risk for metabolic disorders in a normal weight Chinese population. World J. Gastroenterol. 2014, 20, 17932–17940. [Google Scholar] [CrossRef]
- Fu, C.P.; Ali, H.; Rachakonda, V.P.; Oczypok, E.A.; DeLany, J.P.; Kershaw, E.E. The ZJU index is a powerful surrogate marker for NAFLD in severely obese North American women. PLoS ONE 2019, 14, e0224942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izadi, A.; Gargari, B.P.; Aliasghari, F.; Ebrahimi, S. Adipokines and visceral adiposity index in relation to clinical findings of NAFLD patients. Prog. Nutr. 2018, 20, 145–152. [Google Scholar] [CrossRef]
- Karamfilova, V.; Gateva, A.; Alexiev, A.; Zheleva, N.; Velikova, T.; Ivanova-Boyanova, R.; Ivanova, R.; Cherkezov, N.; Kamenov, Z.; Mateva, L. The association between retinol-binding protein 4 and prediabetes in obese patients with nonalcoholic fatty liver disease. Arch. Physiol. Biochem. 2019, 1–6. [Google Scholar] [CrossRef]
- Keating, S.E.; Parker, H.M.; Hickman, I.J.; Gomersall, S.R.; Wallen, M.P.; Coombes, J.S.; Macdonald, G.A.; George, J.; Johnson, N.A. NAFLD in clinical practice: Can simple blood and anthropometric markers be used to detect change in liver fat measured by (1) H-MRS? Liver Int. 2017, 37, 1907–1915. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; You, W.; Ren, W. The ZJU index is a powerful index for identifying NAFLD in the general Chinese population. Acta Diabetol. 2017, 54, 905–911. [Google Scholar] [CrossRef]
- Li, M.; Shu, W.; Zunong, J.; Amaerjiang, N.; Xiao, H.; Li, D.; Vermund, S.H.; Hu, Y. Predictors of non-alcoholic fatty liver disease in children. Pediatr. Res. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.T.; Lee, M.Y.; Wang, C.W.; Wu, D.W.; Chen, S.C. Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population. Int. J. Environ. Res. Public Health 2021, 18, 857. [Google Scholar] [CrossRef]
- Musso, G.; Cassader, M.; De Michieli, F.; Rosina, F.; Orlandi, F.; Gambino, R. Nonalcoholic steatohepatitis versus steatosis: Adipose tissue insulin resistance and dysfunctional response to fat ingestion predict liver injury and altered glucose and lipoprotein metabolism. Hepatology 2012, 56, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Okamura, T.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. The visceral adiposity index is a predictor of incident nonalcoholic fatty liver disease: A population-based longitudinal study. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 375–383. [Google Scholar] [CrossRef]
- Sheng, G.; Lu, S.; Xie, Q.; Peng, N.; Kuang, M.; Zou, Y. The usefulness of obesity and lipid-related indices to predict the presence of Non-alcoholic fatty liver disease. Lipids Health Dis. 2021, 20, 134. [Google Scholar] [CrossRef]
- Villanueva-Ortega, E.; Garcés-Hernández, M.J.; Herrera-Rosas, A.; López-Alvarenga, J.C.; Laresgoiti-Servitje, E.; Escobedo, G.; Queipo, G.; Cuevas-Covarrubias, S.; Garibay-Nieto, G.N. Gender-specific differences in clinical and metabolic variables associated with NAFLD in a Mexican pediatric population. Ann. Hepatol. 2019, 18, 693–700. [Google Scholar] [CrossRef]
- Vural Keskinler, M.; Mutlu, H.H.; Sirin, A.; Erkalma Senates, B.; Colak, Y.; Tuncer, I.; Oguz, A. Visceral Adiposity Index As a Practical Tool in Patients with Biopsy-Proven Nonalcoholic Fatty Liver Disease/Nonalcoholic Steatohepatitis. Metab. Syndr. Relat. Disord. 2021, 19, 26–31. [Google Scholar] [CrossRef]
- Zaki, M.; Amin, D.; Mohamed, R. Body composition, phenotype and central obesity indices in Egyptian women with non-alcoholic fatty liver disease. J. Complement Integr. Med. 2020, 18, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus, P. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Kim, D.; Chung, G.E.; Kwak, M.S.; Seo, H.B.; Kang, J.H.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Lee, H.S.; Kim, C.Y. Body Fat Distribution and Risk of Incident and Regressed Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2016, 14, 132–138.e4. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.; Alkharfy, K.; Wani, K.; Amer, O.E.; Ul Haq, S.; Rahman, S.; Alnaami, A.M.; Livadas, S.; et al. Does visceral adiposity index signify early metabolic risk in children and adolescents?: Association with insulin resistance, adipokines, and subclinical inflammation. Pediatr. Res. 2014, 75, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Maffeis, C.; Manfredi, R.; Trombetta, M.; Sordelli, S.; Storti, M.; Benuzzi, T.; Bonadonna, R.C. Insulin sensitivity is correlated with subcutaneous but not visceral body fat in overweight and obese prepubertal children. J. Clin. Endocrinol. Metab. 2008, 93, 2122–2128. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.C.; Giordano, C. The current version of the visceral adiposity index is not suitable for application in pediatric populations: Comments on the article by Al-Daghri et al. Pediatr. Res. 2014, 76, 415. [Google Scholar] [CrossRef] [Green Version]
- Hernández, M.J.G.; Huerta, S.F. Pediatric Visceral Adiposity Index Adaptation Correlates with Homa-Ir, Matsuda, and Transaminases. Endocr. Pract. 2018, 24, 294–301. [Google Scholar] [CrossRef]
- Jayakumar, S.; Harrison, S.A.; Loomba, R. Noninvasive Markers of Fibrosis and Inflammation in Nonalcoholic Fatty Liver Disease. Curr. Hepatol. Rep. 2016, 15, 86–95. [Google Scholar] [CrossRef] [Green Version]
- Vali, Y.; Lee, J.; Boursier, J.; Spijker, R.; Verheij, J.; Brosnan, M.J.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H.; on behalf of the LITMUS Systematic Review Team. FibroTest for Evaluating Fibrosis in Non-Alcoholic Fatty Liver Disease Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2415. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Adams, L.A.; de Ledinghen, V.; Wong, G.L.; Sookoian, S. Noninvasive biomarkers in NAFLD and NASH—current progress and future promise. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 461–478. [Google Scholar] [CrossRef] [PubMed]
- Ismaiel, A.; Leucuta, D.C.; Popa, S.L.; Fagoonee, S.; Pellicano, R.; Abenavoli, L.; Dumitrascu, D.L. Noninvasive biomarkers in predicting non-alcoholic steatohepatitis and assessing liver fibrosis: Systematic review and meta-analysis. Panminerva. Med. 2020. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismaiel, A.; Jaaouani, A.; Leucuta, D.-C.; Popa, S.-L.; Dumitrascu, D.L. The Visceral Adiposity Index in Non-Alcoholic Fatty Liver Disease and Liver Fibrosis—Systematic Review and Meta-Analysis. Biomedicines 2021, 9, 1890. https://doi.org/10.3390/biomedicines9121890
Ismaiel A, Jaaouani A, Leucuta D-C, Popa S-L, Dumitrascu DL. The Visceral Adiposity Index in Non-Alcoholic Fatty Liver Disease and Liver Fibrosis—Systematic Review and Meta-Analysis. Biomedicines. 2021; 9(12):1890. https://doi.org/10.3390/biomedicines9121890
Chicago/Turabian StyleIsmaiel, Abdulrahman, Ayman Jaaouani, Daniel-Corneliu Leucuta, Stefan-Lucian Popa, and Dan L. Dumitrascu. 2021. "The Visceral Adiposity Index in Non-Alcoholic Fatty Liver Disease and Liver Fibrosis—Systematic Review and Meta-Analysis" Biomedicines 9, no. 12: 1890. https://doi.org/10.3390/biomedicines9121890
APA StyleIsmaiel, A., Jaaouani, A., Leucuta, D.-C., Popa, S.-L., & Dumitrascu, D. L. (2021). The Visceral Adiposity Index in Non-Alcoholic Fatty Liver Disease and Liver Fibrosis—Systematic Review and Meta-Analysis. Biomedicines, 9(12), 1890. https://doi.org/10.3390/biomedicines9121890