
Foveal Avascular Zone and Choroidal Thickness Are Decreased in Subjects with Hard Drusen and without High Genetic Risk of Developing Alzheimer’s Disease

 ,
,  ,
, 
 ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
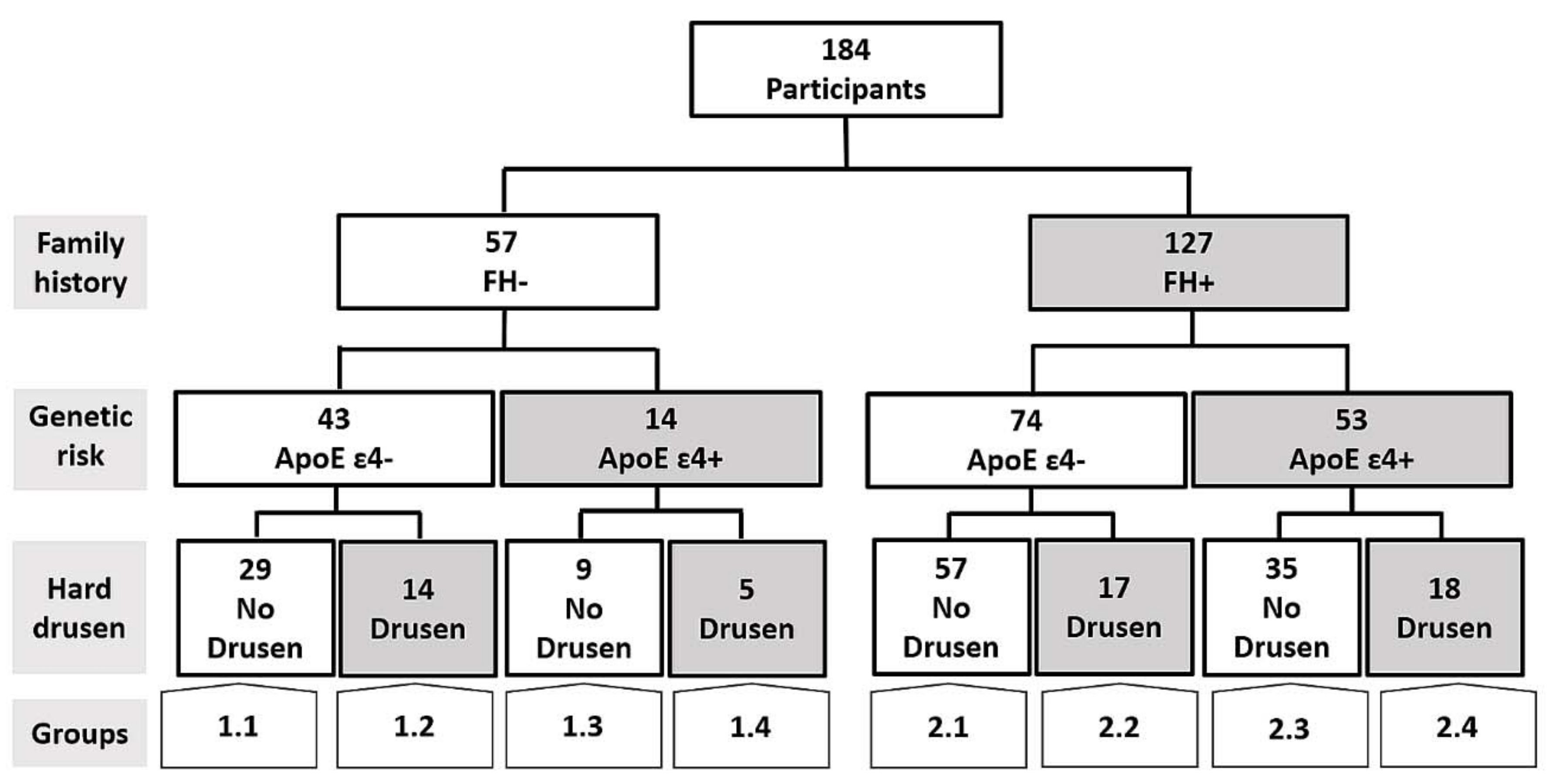
2.1. Study Design
- -
- Group 1 is a control group, which consisted of middle-aged subjects without a first-degree family history of AD (FH−).
- -
- Group 2 comprises subjects with a family history of AD (FH+). Subjects were middle-aged with at least one parent with sporadic AD. To verify the AD diagnoses of parents, a review of their medical records was conducted by a multidisciplinary diagnostic consensus panel. Only diagnoses that were made under internationally accepted criteria were included. Because autopsies were not performed in most AD patients, postmortem reports were welcome but were not used as the basis of inclusion. Relatives with known autosomal dominant mutations (i.e., preseniline-1 or 2) were not included.
- 1.1.
- FH−; ApoE ɛ4−; No Drusen (FH−, ɛ4−, HD−).
- 1.2.
- FH−; ApoE ɛ4−; Drusen (FH−, ɛ4−, HD+).
- 1.3.
- FH−; ApoE ɛ4+; No Drusen (FH−, ɛ4+, HD−).
- 1.4.
- FH−; ApoE ɛ4+; Drusen (FH−, ɛ4+, HD+).
- 2.1.
- FH+; ApoE ɛ4−; No Drusen (FH+, ɛ4−, HD−).
- 2.2.
- FH+; ApoE ɛ4−; Drusen (FH+, ɛ4−, HD+).
- 2.3.
- FH+; ApoE ɛ4+; No Drusen (FH+, ɛ4+, HD−).
- 2.4.
- FH+; ApoE ɛ4+; Drusen (FH+, ɛ4+, HD+).
2.2. Subjects
2.3. ApoE Genotyping
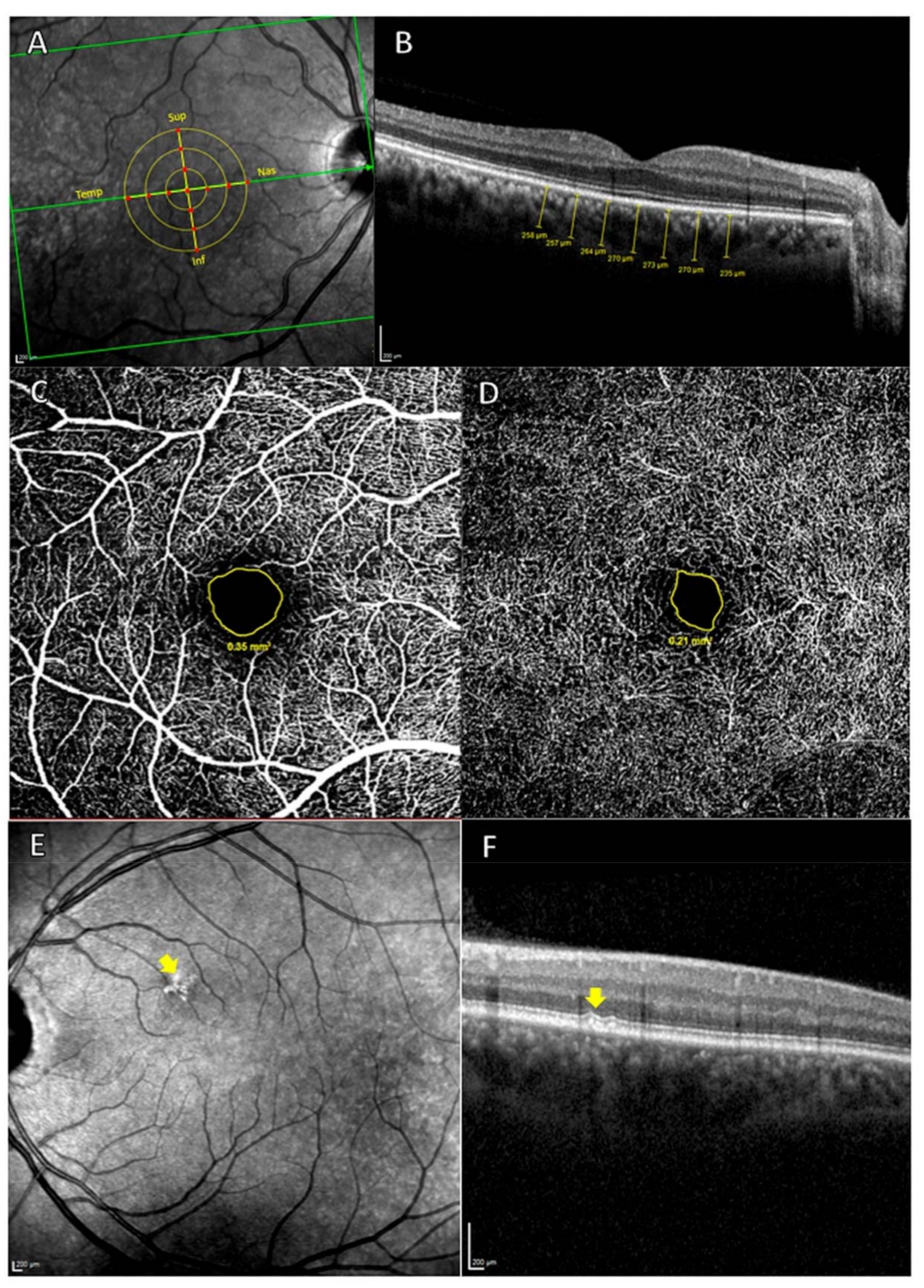
2.4. Spectral-Domain Optical Coherence Tomography (OCT) Imaging: Choroidal Thickness and FAZ Measurement
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Choroidal Thickness
3.3. Foveal Avascular Zone (FAZ)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savva, G.M.; Wharton, S.B.; Ince, P.G.; Forster, G.; Matthews, F.E.; Brayne, C. Age, Neuropathology, and Dementia. N. Engl. J. Med. 2009, 360, 2302–2309. [Google Scholar] [CrossRef] [PubMed]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef]
- Perl, D.P. Neuropathology of Alzheimer’s Disease. Mt. Sinai J. Med. A J. Transl. Pers. Med. 2010, 77, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Glenner, G.G.; Wong, C.W. Alzheimer’s disease: Initial report of the purification and characterization of a novel cerebrovascular amyloid protein. Biochem. Biophys. Res. Commun. 1984, 120, 885–890. [Google Scholar] [CrossRef]
- Thal, D.R.; Griffin, W.S.T.; de Vos, R.A.I.; Ghebremedhin, E. Cerebral amyloid angiopathy and its relationship to Alzheimer’s disease. Acta Neuropathol. 2008, 115, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Roher, A.E.; Lowenson, J.D.; Clarke, S.; Woods, A.S.; Cotter, R.J.; Gowing, E.; Ball, M.J. β-amyloid-(1-42) is a major component of cerebrovascular amyloid deposits: Implications for the pathology of Alzheimer disease. Proc. Natl. Acad. Sci. USA 1993, 90, 10836–10840. [Google Scholar] [CrossRef] [PubMed]
- Namba, Y.; Tomonaga, M.; Kawasaki, H.; Otomo, E.; Ikeda, K. Apolipoprotein E immunoreactivity in cerebral amyloid deposits and neurofibrillary tangles in Alzheimer’s disease and kuru plaque amyloid in Creutzfeldt-Jakob disease. Brain Res. 1991, 541, 163–166. [Google Scholar] [CrossRef]
- Tekirian, T.L.; Saido, T.C.; Markesbery, W.R.; Russell, M.J.; Wekstein, D.R.; Patel, E.; Geddes, J.W. N-terminal heterogeneity of parenchymal and cerebrovascular aβ deposits. J. Neuropathol. Exp. Neurol. 1998, 57, 76–94. [Google Scholar] [CrossRef] [PubMed]
- Louveau, A.; Plog, B.A.; Antila, S.; Alitalo, K.; Nedergaard, M.; Kipnis, J. Understanding the functions and relationships of the glymphatic system and meningeal lymphatics. J. Clin. Investig. 2017, 127, 3210–3219. [Google Scholar] [CrossRef]
- Kimbrough, I.F.; Robel, S.; Roberson, E.D.; Sontheimer, H. Vascular amyloidosis impairs the gliovascular unit in a mouse model of Alzheimer’s disease. Brain 2015, 138, 3716–3733. [Google Scholar] [CrossRef]
- Koronyo, Y.; Salumbides, B.C.; Sheyn, J.; Pelissier, L.; Li, S.; Ljubimov, V.; Moyseyev, M.; Daley, D.; Fuchs, D.T.; Pham, M.; et al. Therapeutic effects of glatiramer acetate and grafted CD115+ monocytes in a mouse model of Alzheimer’s disease. Brain 2015, 138, 2399–2422. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Koronyo, Y.; Rentsendorj, A.; Regis, G.C.; Sheyn, J.; Fuchs, D.T.; Kramerov, A.A.; Ljubimov, A.V.; Dumitrascu, O.M.; Rodriguez, A.R.; et al. Identification of early pericyte loss and vascular amyloidosis in Alzheimer’s disease retina. Acta Neuropathol. 2020, 139, 813–836. [Google Scholar] [CrossRef] [PubMed]
- Arvanitakis, Z.; Leurgans, S.E.; Wang, Z.; Wilson, R.S.; Bennett, D.A.; Schneider, J.A. Cerebral amyloid angiopathy pathology and cognitive domains in older persons. Ann. Neurol. 2011, 69, 320–327. [Google Scholar] [CrossRef]
- Boyle, P.A.; Yu, L.; Nag, S.; Leurgans, S.; Wilson, R.S.; Bennett, D.A.; Schneider, J.A. Cerebral amyloid angiopathy and cognitive outcomes in community-based older persons. Neurology 2015, 85, 1930–1936. [Google Scholar] [CrossRef]
- Bulut, M.; Kurtuluş, F.; Gözkaya, O.; Erol, M.K.; Cengiz, A.; Akldan, M.; Yaman, A. Evaluation of optical coherence tomography angiographic findings in Alzheimer’s type dementia. Br. J. Ophthalmol. 2018, 102, 233–237. [Google Scholar] [CrossRef]
- Williams, M.A.; McGowan, A.J.; Cardwell, C.R.; Cheung, C.Y.; Craig, D.; Passmore, P.; Silvestri, G.; Maxwell, A.P.; McKay, G.J. Retinal microvascular network attenuation in Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2015, 1, 229–235. [Google Scholar] [CrossRef]
- Frost, S.; Kanagasingam, Y.; Sohrabi, H.; Vignarajan, J.; Bourgeat, P.; Salvado, O.; Villemagne, V.; Rowe, C.C.; Lance MacAulay, S.; Szoeke, C.; et al. Retinal vascular biomarkers for early detection and monitoring of Alzheimer’s disease. Transl. Psychiatry 2013, 3, e233. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, J.M.; Rojas, B.; Gallego, B.I.; García-Martín, E.S.; Triviño, A.; Ramírez, A.I.; Salazar, J.J.; de Hoz, R. Glia and blood retinal barrier: Effects of ocular hypertension. In Cardiovascular Disease II; iConcept Press Ltd.: Hong Kong, China, 2014; pp. 123–162. [Google Scholar]
- Donix, M.; Small, G.W.; Bookheimer, S.Y. Family history and APOE-4 genetic risk in Alzheimer’s disease. Neuropsychol. Rev. 2012, 22, 298–309. [Google Scholar] [CrossRef]
- Bendlin, B.B.; Carlsson, C.M.; Gleason, C.E.; Johnson, S.C.; Sodhi, A.; Gallagher, C.L.; Puglielli, L.; Engelman, C.D.; Ries, M.L.; Xu, G.; et al. Midlife predictors of Alzheimer’s disease. Maturitas 2010, 65, 131–137. [Google Scholar] [CrossRef]
- Jayadev, S.; Steinbart, E.J.; Chi, Y.Y.; Kukull, W.A.; Schellenberg, G.D.; Bird, T.D. Conjugal Alzheimer disease: Risk in children when both parents have Alzheimer disease. Arch. Neurol. 2008, 65, 373–378. [Google Scholar] [CrossRef]
- Ribalta, J.; Vallvé, J.C.; Girona, J.; Masana, L. Apolipoprotein and apolipoprotein receptor genes, blood lipids and disease. Curr. Opin. Clin. Nutr. Metab. Care 2003, 6, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.H.; Ozaki, S.; Nealon, M.; Neitz, J.; Mullins, R.F.; Hageman, G.S.; Johnson, L.V. Local cellular sources of apolipoprotein E in the human retina and retinal pigmented epithelium: Implications for the process of drusen formation. Am. J. Ophthalmol. 2001, 131, 767–781. [Google Scholar] [CrossRef]
- Toops, K.A.; Tan, L.X.; Lakkaraju, A. Apolipoprotein E isoforms and AMD. Adv. Exp. Med. Biol. 2016, 854, 3–9. [Google Scholar] [PubMed]
- McKay, G.J.; Patterson, C.C.; Chakravarthy, U.; Dasari, S.; Klaver, C.C.; Vingerling, J.R.; Ho, L.; de Jong, P.T.V.M.; Fletcher, A.E.; Young, I.S.; et al. Evidence of association of APOE with age-related macular degeneration—A pooled analysis of 15 studies. Hum. Mutat. 2011, 32, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- März, W.; Scharnagl, H.; Hoffmann, M.M.; Boehm, B.O.; Winkelmann, B.R. The apolipoprotein E polymorphism is associated with circulating C-reactive protein (the Ludwigshafen risk and cardiovascular health study). Eur. Heart J. 2004, 25, 2109–2119. [Google Scholar] [CrossRef]
- Baird, P.N.; Richardson, A.J.; Robman, L.D.; Dimitrov, P.N.; Tikellis, G.; McCarty, C.A.; Guymer, R.H. Apolipoprotein (APOE) gene is associated with progression of age-related macular degeneration (AMD). Hum. Mutat. 2006, 27, 337–342. [Google Scholar] [CrossRef]
- De Jong, P.T.V.M. Age-Related Macular Degeneration. N. Engl. J. Med. 2006, 355, 1474–1485. [Google Scholar] [CrossRef] [PubMed]
- Boon, C.J.F.; van de Ven, J.P.H.; Hoyng, C.B.; den Hollander, A.I.; Klevering, B.J. Cuticular drusen: Stars in the sky. Prog. Retin. Eye Res. 2013, 37, 90–113. [Google Scholar] [CrossRef] [PubMed]
- Kaarniranta, K.; Salminen, A.; Haapasalo, A.; Soininen, H.; Hiltunen, M. Age-related macular degeneration (AMD): Alzheimer’s disease in the eye? J. Alzheimer’s Dis. 2011, 24, 615–631. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, J.M.; Ramírez, A.I.; Salazar, J.J.; de Hoz, R.; Triviño, A. Changes of astrocytes in retinal ageing and age-related macular degeneration. Exp. Eye Res. 2001, 73, 601–615. [Google Scholar] [CrossRef]
- Salobrar-Garcia, E.; Méndez-Hernández, C.; de Hoz, R.; Ramírez, A.I.; López-Cuenca, I.; Fernández-Albarral, J.A.; Rojas, P.; Wang, S.; García-Feijoo, J.; Gil, P.; et al. Ocular Vascular Changes in Mild Alzheimer’s Disease Patients: Foveal Avascular Zone, Choroidal Thickness, and ONH Hemoglobin Analysis. J. Pers. Med. 2020, 10, 231. [Google Scholar] [CrossRef]
- Gharbiya, M.; Trebbastoni, A.; Parisi, F.; Manganiello, S.; Cruciani, F.; D’Antonio, F.; De Vico, U.; Imbriano, L.; Campanelli, A.; De Lena, C. Choroidal thinning as a new finding in Alzheimer’s Disease: Evidence from enhanced depth imaging spectral domain Optical Coherence Tomography. J. Alzheimer’s Dis. 2014, 40, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.Y.; Chan, V.T.T.; Mok, V.C.; Chen, C.; Wong, T.Y. Potential retinal biomarkers for dementia: What is new? Curr. Opin. Neurol. 2019, 32, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Koh, L.H.L.; Agrawal, R.; Khandelwal, N.; Sai Charan, L.; Chhablani, J. Choroidal vascular changes in age-related macular degeneration. Acta Ophthalmol. 2017, 95, e597–e601. [Google Scholar] [CrossRef] [PubMed]
- Feke, G.T.; Hyman, B.T.; Stern, R.A.; Pasquale, L.R. Retinal blood flow in mild cognitive impairment and Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2015, 1, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Teja, K.V.R.; Berendschot, T.J.M.T.; Steinbusch, H.; Webers, A.B.C.; Murthy, R.P.; Mathuranath, P.S. Cerebral and Retinal Neurovascular Changes: A Biomarker for Alzheimer’s Disease. J. Gerontol. Geriatr. Res. 2017, 6, 447. [Google Scholar]
- Jiang, H.; Liu, Y.; Wei, Y.; Shi, Y.; Wright, C.B.; Sun, X.; Rundek, T.; Baumel, B.S.; Landman, J.; Wang, J. Impaired retinal microcirculation in patients with Alzheimer’s disease. PLoS ONE 2018, 13, e0192154. [Google Scholar]
- Delaey, C.; Van de Voorde, J. Regulatory mechanisms in the retinal and choroidal circulation. Ophthalmic Res. 2000, 32, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Nickla, D.L.; Wallman, J. The multifunctional choroid. Prog. Retin. Eye Res. 2010, 29, 144–168. [Google Scholar] [CrossRef]
- Bulut, M.; Yaman, A.; Erol, M.K.; Kurtulus, F.; Toslak, D.; Dogan, B.; Turgut Coban, D.; Kaya Basar, E. Choroidal thickness in patients with mild cognitive impairment and Alzheimer’s type dementia. J. Ophthalmol. 2016, 2016, 7291257. [Google Scholar] [CrossRef]
- Triviño, A.; de Hoz, R.; Salazar, J.J.; Ramírez, A.I.; Rojas, B.; Ramírez, J.M. Distribution and organization of the nerve fiber and ganglion cells of the human choroid. Anat. Embryol. 2002, 205, 417–430. [Google Scholar] [CrossRef]
- Triviño, A.; de Hoz, R.; Rojas, B.; Salazar, J.J.; Ramirez, A.I.; Ramirez, J.M. NPY and TH innervation in human choroidal whole-mounts. Histol. Histopathol. 2005, 20, 393–402. [Google Scholar] [PubMed]
- Ramírez, J.M.; Ramírez, A.I.; Salazar, J.J.; de Hoz, R.; Rojas, B.; Triviño, A. Anatomofisiología de la úvea posterior: Coroides. In Degeneracion Macular Asociada a la Edad; Mones, J., Gómez-Ulla, F., Eds.; Probus Science: Barcelona, Spain, 2005; pp. 1–28. [Google Scholar]
- Bayhan, H.A.; Aslan Bayhan, S.; Celikbilek, A.; Tanik, N.; Gürdal, C. Evaluation of the chorioretinal thickness changes in Alzheimer’s disease using spectral-domain optical coherence tomography. Clin. Exp. Ophthalmol. 2015, 43, 145–151. [Google Scholar] [CrossRef]
- Cunha, J.P.J.P.; Proença, R.; Dias-Santos, A.; Melancia, D.; Almeida, R.; Águas, H.; Santos, B.O.; Alves, M.; Ferreira, J.; Papoila, A.L.L.; et al. Choroidal thinning: Alzheimer’s disease and aging. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2017, 8, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Trebbastoni, A.; Marcelli, M.; Mallone, F.; D’Antonio, F.; Imbriano, L.; Campanelli, A.; de Lena, C.; Gharbiya, M. Attenuation of choroidal thickness in patients with Alzheimer Disease: Evidence from an Italian Prospective Study. Alzheimer Dis. Assoc. Disord. 2016, 31, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Wylęgała, A. Principles of OCTA and Applications in Clinical Neurology. Curr. Neurol. Neurosci. Rep. 2018, 18, 96. [Google Scholar] [CrossRef]
- López-de-Eguileta, A.; Lage, C.; López-García, S.; Pozueta, A.; García-Martínez, M.; Kazimierczak, M.; Bravo, M.; de Arcocha-Torres, M.; Banzo, I.; Jimenez-Bonilla, J.; et al. Evaluation of choroidal thickness in prodromal Alzheimer’s disease defined by amyloid PET. PLoS ONE 2020, 15, e0239484. [Google Scholar] [CrossRef]
- Foster, N.L.; Chase, T.N.; Mansi, L.; Brooks, R.; Fedio, P.; Patronas, N.J.; Di Chiro, G. Cortical abnormalities in Alzheimer’s disease. Ann. Neurol. 1984, 16, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.A.; Jahng, G.H.; Weiner, M.W.; Miller, B.L.; Chui, H.C.; Jagust, W.J.; Gorno-Tempini, M.L.; Schuff, N. Pattern of cerebral hypoperfusion in Alzheimer disease and mild cognitive impairment measured with arterial spin-labeling MR imaging: Initial experience. Radiology 2005, 234, 851–859. [Google Scholar] [CrossRef]
- Bertram, L.; Lill, C.M.; Tanzi, R.E. The genetics of alzheimer disease: Back to the future. Neuron 2010, 68, 270–281. [Google Scholar] [CrossRef]
- Edwards, G.A.; Gamez, N.; Escobedo, G.; Calderon, O.; Moreno-Gonzalez, I. Modifiable risk factors for Alzheimer’s disease. Front. Aging Neurosci. 2019, 11, 146. [Google Scholar] [CrossRef]
- Klaver, C.C.W.; Kliffen, M.; Van Duijn, C.M.; Hofman, A.; Cruts, M.; Grobbee, D.E.; Van Broeckhoven, C.; De Jong, P.T.V.M. Genetic association of apolipoprotein E with age-related macular degeneration. Am. J. Hum. Genet. 1998, 63, 200–206. [Google Scholar] [CrossRef]
- Zareparsi, S.; Reddick, A.C.; Branham, K.E.H.; Moore, K.B.; Jessup, L.; Thoms, S.; Smith-Wheelock, M.; Yashar, B.M.; Swaroop, A. Association of apolipoprotein E alleles with susceptibility to age-related macular degeneration in a large cohort from a single center. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1306–1310. [Google Scholar] [CrossRef] [PubMed]
- Souied, E.H.; Benlian, P.; Amouyel, P.; Feingold, J.; Lagarde, J.P.; Munnich, A.; Kaplan, J.; Coscas, G.; Soubrane, G. The ε4 allele of the Apolipoprotein E gene as a potential protective factor for exudative age-related macular degeneration. Am. J. Ophthalmol. 1998, 125, 353–359. [Google Scholar] [CrossRef]
- Mullins, R.F.; Johnson, M.N.; Faidley, E.A.; Skeie, J.M.; Huang, J. Choriocapillaris vascular dropout related to density of drusen in human eyes with early age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1606–1612. [Google Scholar] [CrossRef] [PubMed]
- Lutty, G.A.; McLeod, D.S.; Bhutto, I.A.; Edwards, M.M.; Seddon, J.M. Choriocapillaris dropout in early age-related macular degeneration. Exp. Eye Res. 2020, 192, 107939. [Google Scholar] [CrossRef]
- Berenberg, T.L.; Metelitsina, T.I.; Madow, B.; Dai, Y.; Ying, G.S.; Dupont, J.C.; Grunwald, L.; Brucker, A.J.; Grunwald, J.E. The association between drusen extent and foveolar choroidal blood flow in age-related macular degeneration. Retina 2012, 32, 25–31. [Google Scholar] [CrossRef]
- Chung, S.E.; Kang, S.W.; Lee, J.H.; Kim, Y.T. Choroidal thickness in polypoidal choroidal vasculopathy and exudative age-related macular degeneration. Ophthalmology 2011, 118, 840–845. [Google Scholar] [CrossRef]
- Pauleikhoff, D.; Chen, J.C.; Chisholm, I.H.; Bird, A.C. Choroidal perfusion abnormality with age-related Bruch’s membrane change. Am. J. Ophthalmol. 1990, 109, 211–217. [Google Scholar] [CrossRef]
- Böker, T.; Fang, T.; Steinmetz, R. Refractive error and choroidal perfusion characteristics in patients with choroidal neovascularization and age-related macular degeneration. Ger. J. Ophthalmol. 1993, 2, 10–13. [Google Scholar]
- Chen, J.C.; Fitzke, F.W.; Pauleikhoff, D.; Bird, A.C. Functional loss in age-related Bruch’s membrane change with choroidal perfusion defect. Investig. Ophthalmol. Vis. Sci. 1992, 33, 334–340. [Google Scholar]
- Holz, F.G.; Wolfensberger, T.J.; Piguet, B.; Gross-Jendroska, M.; Wells, J.A.; Minassian, D.C.; Chisholm, I.H.; Bird, A.C. Bilateral Macular Drusen in Age-related Macular Degeneration: Prognosis and Risk Factors. Ophthalmology 1994, 101, 1522–1528. [Google Scholar] [CrossRef]
- Prünte, C.; Niesel, P. Quantification of choroidal blood-flow parameters using indocyanine green video-fluorescence angiography and statistical picture analysis. Graefe’s Arch. Clin. Exp. Ophthalmol. 1988, 226, 55–58. [Google Scholar] [CrossRef]
- Friedman, E.; Ivry, M.; Ebert, E.; Glynn, R.; Gragoudas, E.; Seddon, J. Increased Scleral Rigidity and Age-related Macular Degeneration. Ophthalmology 1989, 96, 104–108. [Google Scholar] [CrossRef]
- Schultz, N.; Byman, E.; Wennström, M. Levels of Retinal Amyloid-β Correlate with Levels of Retinal IAPP and Hippocampal Amyloid-β in Neuropathologically Evaluated Individuals. J. Alzheimer’s Dis. 2020, 73, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Smyth, L.C.D.; Rustenhoven, J.; Scotter, E.L.; Schweder, P.; Faull, R.L.M.; Park, T.I.H.; Dragunow, M. Markers for human brain pericytes and smooth muscle cells. J. Chem. Neuroanat. 2018, 92, 48–60. [Google Scholar] [CrossRef]
- Snodderly, D.M.; Weinhaus, R.S.; Choi, J.C. Neural-vascular relationships in central retina of macaque monkeys (Macaca fascicularis). J. Neurosci. 1992, 12, 1169–1193. [Google Scholar] [CrossRef] [PubMed]
- Conrath, J.; Giorgi, R.; Raccah, D.; Ridings, B. Foveal avascular zone in diabetic retinopathy: Quantitative vs. qualitative assessment. Eye 2005, 19, 322–326. [Google Scholar] [CrossRef]
- Van De Kreeke, J.A.; Nguyen, H.T.; Konijnenberg, E.; Tomassen, J.; Den Braber, A.; Ten Kate, M.; Yaqub, M.; Van Berckel, B.; Lammertsma, A.A.; Boomsma, D.I.; et al. Optical coherence tomography angiography in preclinical Alzheimer’s disease. Br. J. Ophthalmol. 2019, 104, 157–161. [Google Scholar] [CrossRef]
- O’bryhim, B.; Apte, R.; Kung, N.; Coble, D.; Van Starven, G.P. Association of preclinical Alzheimer disease with optical coherence tomographic angiography findings. JAMA Ophthalmol. 2018, 136, 1242–1248. [Google Scholar] [CrossRef] [PubMed]
- Chua, J.; Hu, Q.; Ke, M.; Tan, B.; Hong, J.; Yao, X.; Hilal, S.; Venketasubramanian, N.; Garhöfer, G.; Cheung, C.; et al. Retinal Microvascular Alterations in Alzheimer’s Disease and Mild Cognitive Impairment. Alzheimers. Res. Ther. 2020, 12, 161. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Zhou, N.; Knoll, B.M.; Samra, S.; Ward, M.R.; Weintraub, S.; Fawzi, A.A. Parafoveal vessel loss and correlation between peripapillary vessel density and cognitive performance in amnestic mild cognitive impairment and early Alzheimer’s Disease on optical coherence tomography angiography. PLoS ONE 2019, 14, e0214685. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.Y.; Choi, E.Y.; Kim, M.; Lee, H.K.; Byeon, S.H. Changes in retinal microvasculature and retinal layer thickness in association with apolipoprotein E genotype in Alzheimer’s disease. Sci. Rep. 2021, 11, 1847. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhao, Q.; Tao, R.; Lu, H.; Xiao, Z.; Zheng, L.; Ding, D.; Ding, S.; Ma, Y.; Lu, Z.; et al. Decreased Retinal Vascular Density in Alzheimer’s Disease (AD) and Mild Cognitive Impairment (MCI): An Optical Coherence Tomography Angiography (OCTA) Study. Front. Aging Neurosci. 2021, 12, 295. [Google Scholar] [CrossRef] [PubMed]
- Grewal, D.S.; Polascik, B.W.; Hoffmeyer, G.C.; Fekrat, S. Assessment of differences in retinal microvasculature using OCT angiography in Alzheimer’s disease: A twin discordance report. Ophthalmic Surg. Lasers Imaging Retin. 2018, 49, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Zabel, P.; Kaluzny, J.J.; Wilkosc-Debczynska, M.; Gebska-Toloczko, M.; Suwala, K.; Zabel, K.; Zaron, A.; Kucharski, R.; Araszkiewicz, A. Comparison of Retinal Microvasculature in Patients with Alzheimer’s Disease and Primary Open-Angle Glaucoma by Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2019, 60, 3447. [Google Scholar] [CrossRef]
- Yoon, S.P.; Grewal, D.S.; Thompson, A.C.; Polascik, B.W.; Dunn, C.; Burke, J.R.; Fekrat, S. Retinal Microvascular and Neurodegenerative Changes in Alzheimer’s Disease and Mild Cognitive Impairment Compared with Control Participants. Ophthalmol. Retin. 2019, 3, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.R.; Thore, C.R. Review: Cerebral microvascular pathology in ageing and neurodegeneration. Neuropathol. Appl. Neurobiol. 2011, 37, 56–74. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Ophthalmological Evaluation | ||
|---|---|---|
| Screening Questions | Visual Exam | Inclusion Criteria |
| Do you use glasses? Yes/no Do you know if you have myopia, hypermetropy, or astigmatism? Yes/no Do you know your diopter measurements? Yes/no Do you have any ocular pathologies? Yes/no Do you receive any type of ocular treatment? Yes/no Have you undergone any type of ocular surgery? Yes/no | Refraction Visual acuity Biomicroscopy Intraocular pressure OCT/OCTA | ±5 Spherocylindrical refractive >0.5 dec <21 mmHg Free of ocular disease Free of congenital malformation Free of known or suspected glaucoma |
| Demographic/MMSE Data | FH− | FH+ | ||||||
|---|---|---|---|---|---|---|---|---|
| ApoE ɛ4− | ApoE ɛ4+ | ApoE ɛ4− | ApoE ɛ4+ | |||||
| No HD | HD | No HD | HD | No HD | HD | No HD | HD | |
| Group 1.1 | Group 1.2 | Group 1.3 | Group 1.4 | Group 2.1 | Group 2.2 | Group 2.3 | Group 2.4 | |
| N | 29 | 14 | 9 | 5 | 57 | 17 | 35 | 18 |
| Age | 59.0 (54.0–65.0) | 62.5 (56.0–69.0) | 63.0 (54.0–70.0) | 63.0 (58.0–76.5) | 58.0 (53.0–62,0) | 63.0 (56.5–58.5) | 57.0 (57.0–65.0) | 55.5 (51.0–63.0) |
| Sex Male/Female | 12/17 | 6/8 | 3/6 | 0/5 | 22/35 | 6/11 | 11/24 | 9/9 |
| MMSE | 29.0 (28.0–29.0) | 29.0 (29.0–29.0) | 29.0 (28.0–30.0) | 29.0 (29.0–30.0) | 29.0 (28.5–29.0) | 29.0 (28.0–29.0) | 29.0 (29.0–29.0) | 29.0 (28.0–30.0) |
| Vascular Areas Analyzed | FH− | FH+ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ApoE ɛ4− | ApoE ɛ4+ | ApoE ɛ4− | ApoE ɛ4+ | |||||||
| No HD | HD | No HD | HD | No HD | HD | No HD | HD | |||
| Group 1.1 | Group 1.2 | Group 1.3 | Group 1.4 | Group 2.1 | Group 2.2 | Group 2.3 | Group 2.4 | |||
| FAZ | Superficial | 0.47 (0.39–0.62) | 0.45 (0.42–0.68) | 0.47(0.37–0.84) | 0.47 (0.37–0.82) | 0.51 (0.39–0.62) | 0.67 (0.62–0.80) | 0.54 (0.44–0.68) | 0.59 (0.43–0.83) | |
| Deep | 0.23 (0.18–0.31) | 0.22 (0.16–0.34) | 0.24 (0.2–0.359 | 0.23 (0.12–0.34) | 0.26 (0.39–0.33) | 0.29 (0.24–0.38) | 0.28 (0.23–0.33) | 0.29 (0.21–0.41) | ||
| Choroidal Thickness | Subfoveal | 268.0 (213.5–307.5) | 249.5 (176.8–268.0) | 257.0 (234.0–318.0) | 252.5 (164.5–279.8) | 273.0 (231.0–309.5) | 255.0 (215.5–287.0) | 263.0 (212.0–302.0) | 241.0 (224.5–296.5) | |
| Temporal | 500 μm | 260.0 (210.5–325.0) | 234.0 (159.8–259.0) | 266.0 (231.5–316.0) | 256.5 (173.3–296.3) | 263.0 (220.5–302.0) | 252.0 (199.5–292.0) | 256.0 (228.0–295.0) | 252.0 (222.8–297.3) | |
| 1000 μm | 248.0 (207.5–316.0) | 219.5 (161.8–267.50) | 276.0 (202.5–300.0) | 256.5 (176.5–310.3) | 263.0 (218.5–288.5) | 248.0 (195.5–292.0) | 253.0 (219.0–287.0) | 247.5 (217.5–282.0) | ||
| 1500 μm | 232.0 (202.0–296.0) | 222.5 (157.5–255.3) | 254,0 (186.5–343.0) | 255.0 (189.8–292.5) | 255.0 (216.0–288.5) | 251.0 (202.5–282.0) | 250.0 (215.0–280.0) | 265.0 (214.5–291.0) | ||
| Nasal | 500 μm | 261.0 (204.5–313.5) | 230.5 (177.0–252.5) | 238.0 (228.0–302.5) | 256.5 (180.3–292.3) | 267.0 (220.5–295.0) | 234.0 (198.5–285.5) | 249.0 (199.0–297.0) | 244.0 (224.0–286.2) | |
| 1000 μm | 233.0 (195.5–303.5) | 206.0 (150.8–282.0) | 223.0 (204.5–291.5) | 257.0 (173.3–295.8) | 255.0 (190.5–299.0) | 225.0 (191.0–274.5) | 240.0 (182.0–281.0) | 248.5 (198.8–268.0) | ||
| 1500 μm | 221 (175.50–278.5) | 182.5 (140.5–269.3) | 217.0 (171.0–278.0) | 271.0 (134.0–300.0) | 228.0 (183.5–274.5) | 205.0 (170.5–242.0) | 218.0 (174.0–265.0) | 252.0 (179.8–263.0) | ||
| Superior | 500 μm | 262.0 (218.0–301.0) | 222.0 (170.8–273.5) | 260.0 (228.5–311.5) | 265.5 (182.8–292.8) | 265.0 (228.0–299−0) | 262.0 (219.5–282.5) | 257.0 (209.0–309.0) | 252.5 (222.0–284.0) | |
| 1000 μm | 255.0 (218.5–297.0) | 227.0 (170.8–263.8) | 256.0 (227.5–308.5) | 272.5 (180.8–281.8) | 271.0 (228.5–302.0) | 259.0 (217.5–289.0) | 267.0 (223.0–299.0) | 252.5 (234.3–288.0) | ||
| 1500 μm | 259.0 (209.5–306.5) | 223.0 (147.0–253.3) | 250.0 (225.5–319.0) | 269.0 (174.0–298.0) | 261.0 (224.5–305.5) | 261.0 (206.0–286.0) | 262.0 (226.0–300.0) | 257.5 (233.3–290.3) | ||
| Inferior | 500 μm | 262.0 (209.5–311.5) | 222.5 (172.8–274.3) | 256.0 (222.0–308.5) | 272.0 (179.5–284.3) | 270.0 (231.5–304.0) | 252.0 (208.5–276.5) | 265.0 (216.0–310.0) | 251.5 (216,3–301,3) | |
| 1000 μm | 266.0 (217.0–306.5) | 219.0 (165.0–270.8) | 267.0 (229.5–308.5) | 267.5 (171.0–296.5) | 271.0 (227.5–295.5) | 252.0 (211.5–268.0) | 270.0 (216.0–322.0) | 243.0 (219.8–287.3) | ||
| 1500 μm | 264.0 (213.5–312.0) | 217.0 (169.0–257.25) | 262.0 (218.5–300.5) | 271.5 (183.0–276.0) | 268.0 (224.0–304.0) | 257.0 (211.0–266.5) | 250.0 (214.0–317.0) | 269.0 (216.0–309.5) | ||
| Study Groups | FH− | FH+ | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ApoE ɛ4− | ApoE ɛ4+ | ApoE ɛ4− | ApoE ɛ4+ | ||||||||
| No HD | HD | No HD | HD | No HD | HD | No HD | HD | ||||
| Group 1.1 | Group 1.2 | Group 1.3 | Group 1.4 | Group 2.1 | Group 2.2 | Group 2.3 | Group 2.4 | ||||
| FH− | ApoEɛ4− | No HD | 1.1 | Choroid: Sup 1500 (0.030), Inf 1500 (0.028) | |||||||
| HD | 1.2 | Choroid: Sup 1500 (0.039) | Choroid: Sup 1500 (0.019), Inf 1500 (0.040) | ||||||||
| ApoEɛ4+ | No HD | 1.3 | |||||||||
| HD | 1.4 | ||||||||||
| FH+ | ApoEɛ4− | No HD | 2.1 | Superficial FAZ (<0.001) | |||||||
| HD | 2.2 | Superficial FAZ (0.013) | |||||||||
| ApoEɛ4+ | No HD | 2.3 | |||||||||
| HD | 2.4 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Cuenca, I.; de Hoz, R.; Alcántara-Rey, C.; Salobrar-García, E.; Elvira-Hurtado, L.; Fernández-Albarral, J.A.; Barabash, A.; Ramírez-Toraño, F.; de Frutos-Lucas, J.; Salazar, J.J.; et al. Foveal Avascular Zone and Choroidal Thickness Are Decreased in Subjects with Hard Drusen and without High Genetic Risk of Developing Alzheimer’s Disease. Biomedicines 2021, 9, 638. https://doi.org/10.3390/biomedicines9060638
López-Cuenca I, de Hoz R, Alcántara-Rey C, Salobrar-García E, Elvira-Hurtado L, Fernández-Albarral JA, Barabash A, Ramírez-Toraño F, de Frutos-Lucas J, Salazar JJ, et al. Foveal Avascular Zone and Choroidal Thickness Are Decreased in Subjects with Hard Drusen and without High Genetic Risk of Developing Alzheimer’s Disease. Biomedicines. 2021; 9(6):638. https://doi.org/10.3390/biomedicines9060638
Chicago/Turabian StyleLópez-Cuenca, Inés, Rosa de Hoz, Celia Alcántara-Rey, Elena Salobrar-García, Lorena Elvira-Hurtado, José A. Fernández-Albarral, Ana Barabash, Federico Ramírez-Toraño, Jaisalmer de Frutos-Lucas, Juan J. Salazar, and et al. 2021. "Foveal Avascular Zone and Choroidal Thickness Are Decreased in Subjects with Hard Drusen and without High Genetic Risk of Developing Alzheimer’s Disease" Biomedicines 9, no. 6: 638. https://doi.org/10.3390/biomedicines9060638
APA StyleLópez-Cuenca, I., de Hoz, R., Alcántara-Rey, C., Salobrar-García, E., Elvira-Hurtado, L., Fernández-Albarral, J. A., Barabash, A., Ramírez-Toraño, F., de Frutos-Lucas, J., Salazar, J. J., Ramírez, A. I., & Ramírez, J. M. (2021). Foveal Avascular Zone and Choroidal Thickness Are Decreased in Subjects with Hard Drusen and without High Genetic Risk of Developing Alzheimer’s Disease. Biomedicines, 9(6), 638. https://doi.org/10.3390/biomedicines9060638