1. Introduction
Immunoglobulin A vasculitis (IgAV), formerly known as Henoch-Schönlein purpura, is a quite typical vasculitis of small vessels, largely occurring in childhood, characterized by deposits of immune complexes containing predominantly IgA. Its hallmark is a non-thrombocytopenic purpuric rash on the buttocks and lower limbs, but the disease is also characterized by a risk of gastrointestinal, joint and renal involvement. The overall long-term prognosis of IgAV specifically depends on renal involvement, though it is largely benign [
1]. Some patients can suffer from severe extra-skin manifestations, but the reasons for a worse disease evolution in a minority of children with IgAV remain undeciphered. The etiology of IgAV is not yet fully understood: it is thought that an aberrant immune response triggered by infectious or environmental agents in genetically predisposed children is the main intrinsic pathogenetic mechanism of the disease, leading to the formation of galactose-deficient IgA
1 and related immune complexes that precipitate in the skin, gut, joints, or kidneys [
2,
3]. Gastrointestinal involvement is relatively common in IgAV, but can vary in severity, from mild nausea to gastrointestinal bleeding and intussusception that may require surgical intervention: in a recent study about 50% of IgAV cases had gastrointestinal involvement, and 48.9% of them were classified as severe [
4]. In general terms, IgAV has an overall positive prognosis with complete recovery, highly dependent on the deposition of IgA at the renal level alone [
5].
In our study we have evaluated the clinical and laboratory parameters of a single-center cohort of children with IgAV in relation to their disease evolution and, in particular, we have tried to retrospectively determine if any clinical or laboratory clues might eventually predict the occurrence of gastrointestinal manifestations in such a cohort of patients.
2. Patients and Methods
2.1. Population
We retrospectively evaluated the medical records of 201 unselected children with IgAV, who were first admitted to the outpatient care unit of pediatric rheumatology at our university hospital in the decade 2013–2023; 6 patients who were lost at minimal follow-up or with insufficient laboratory data were excluded from our analysis. All remaining 195 children underwent regular clinical examinations and urinalysis to detect possible late renal involvement or disease recurrence. All patients were Caucasians, and none of them were taking anti-seizure medications or vitamin D dietary supplementation.
2.2. Data Collection
We evaluated generic and numeric variables including sex, age at disease onset, presence of a typical rash not only in the lower limbs but also on the upper part of trunk, persistence of the rash for more than 1 month, presence of fever (body temperature above 38 °C) at disease onset combined with laboratory tests such as C-reactive protein (CRP), white blood cell count, serum IgA, C3 and 25-hydroxyvitamin D [25(OH)-vitamin D] as possible predictive factors for the occurrence of gastrointestinal, joint, or renal involvement. Serum 25(OH)-vitamin D levels were measured by automated chemiluminescence immunoassay technology. Gastrointestinal involvement was defined by the presence of abdominal clinical symptoms and bleeding signs (positive occult fecal test or even melena). The presence of arthritis and/or arthralgia, as well as genital involvement, was determined clinically. The findings of renal involvement included gross hematuria or microscopic hematuria, defined by more than 3 red blood cells per high-power field in the sediment of 10 mL of freshly centrifuged urine, and proteinuria was detected via dipstick test by presence of more than 30 mg/dL of proteins 3 times in one week or more than 150 mg of proteins in the urine collected after 24 h, and a urinary protein/creatinine ratio > 0.2. Patients undergoing treatment with corticosteroids or with non-steroidal anti-inflammatory drugs were registered, as well as those who required surgery for any gastrointestinal complications or those who required skin and/or kidney biopsy to better characterize their clinical picture. The results of a pharyngeal swab to detect Streptococcus pyogenes (S. pyogenes) infection were also recorded.
2.3. Inclusion Criteria
IgAV was diagnosed according to the EULAR/PRINTO/PRES criteria, which consist of the combination of a palpable purpuric rash (predominantly on the lower limbs) as a mandatory criterion with any one of the following: (a) diffused abdominal pain, (b) arthritis/arthralgia, (c) signs of kidney damage (hematuria/proteinuria), or (d) IgA deposition on a biopsy from any involved site [
6]. To be eligible for our study patients had to have new-onset disease. The local Ethics Committee authorized a series of study protocols related to nutritional and environmental issues in patients with complex diseases, such as hereditary disorders or autoinflammatory and rheumatologic diseases (approval code: 2105; approval date: 5 February 2019). This study was carried out in accordance with the principles of the Declaration of Helsinki. All patients’ parents were informed about aims of this study at disease onset, and all of them signed a written consent for both the evaluation of their children’s anonymized data and unrestricted access to their medical records.
2.4. Exclusion Criteria
Patients were excluded if they (a) had a specific diagnosis of other vasculitides mimicking IgAV during an eventual hospitalization or at subsequent assessments; (b) had a previous history of hematuria or proteinuria; (c) were affected by any hematological disorders; (d) had a specific immunodeficiency; (e) had any exposure to severe acute respiratory syndrome coronavirus 2 infection.
2.5. Statistical Analysis
STATA 6.0TM software (University Station, TX, USA) was used for statistical analysis. We chose to describe continuous data in terms of mean values and standard deviations if they were normally distributed, otherwise we expressed them in terms of their medians and interquartile ranges. Dichotomous variables were expressed as totals and percentages. We conducted two distinct analyses. In the first, we divided the cohort into two groups based on the presence or absence of gastrointestinal involvement. In the second analysis, we classified the population into two groups based on their serum vitamin D level. Both gastrointestinal involvement and vitamin D levels were evaluated in the acute phase of the disease during the first visit to our outpatients care unit of pediatric rheumatology. Comparisons between groups were made using Student’s t test if the data were normally distributed; alternatively, they were made using the Mann–Whitney U test. Comparisons between groups described with dichotomous data were made with the chi-square test or, if at least one of the groups was smaller than 6, with Fischer’s exact test. To exclude confounding factors in the correlation between groups we performed a multivariate logistic regression analysis adjusted for sex and age, including all variables with a p < 0.2 in the univariate analysis. A p < 0.05 was considered statistically significant. We chose to avoid correcting the study for multiple testing due to its retrospective nature, which requires further perspective confirmation. We preferred notreducing the type I error for null-association to avoid increasing the risk of type II error for any notnullassociations.
5. Discussion
The predictive factors for gastrointestinal complications in children with IgAV have not been clearly studied, although the histopathological spectrum of endoscopic findings might help us to characterize disease severity [
7]. Unlike other vasculitides occurring in childhood, such as Kawasaki disease, for which there are several recommendations in the medical literature and for which different predicting tools for disease evolution have been determined [
8,
9], no standardized regimen exists to manage IgAV in childhood, as large randomized controlled trials have not been conducted yet. Furthermore, there is an unmet need for reliable, validated and widely-accepted disease activity measures in children with IgAV. Renal involvement is the most important factor influencing IgAV prognosis, and there is controversy as to whether IgAV and IgAV-related nephropathy may be considered two faces of the same disease [
10]. The genetic regulation of endothelial function, such as polymorphisms in genes encoding components of the renin-angiotensin system, endothelial nitric oxide synthases and intercellular adhesion molecules, could contribute to the protean expression of IgAV [
11]. In addition, mutations in the
MEFV gene associated with familial Mediterranean fever could further contribute to a predisposition to IgAV [
12]. There are, at present, no measures predicting disease prognosis; however, serum interleukin-18 has been found to be significantly elevated at diagnosis in IgAV patients compared to healthy controls, and to progressively decrease as the disease turns to a positive outcome [
13]. Sestan et al. have recently found that as the severity and duration of skin manifestations increase, so does the risk of developing IgAV-related nephritis and the likelihood that aggressive treatments might be required [
14].
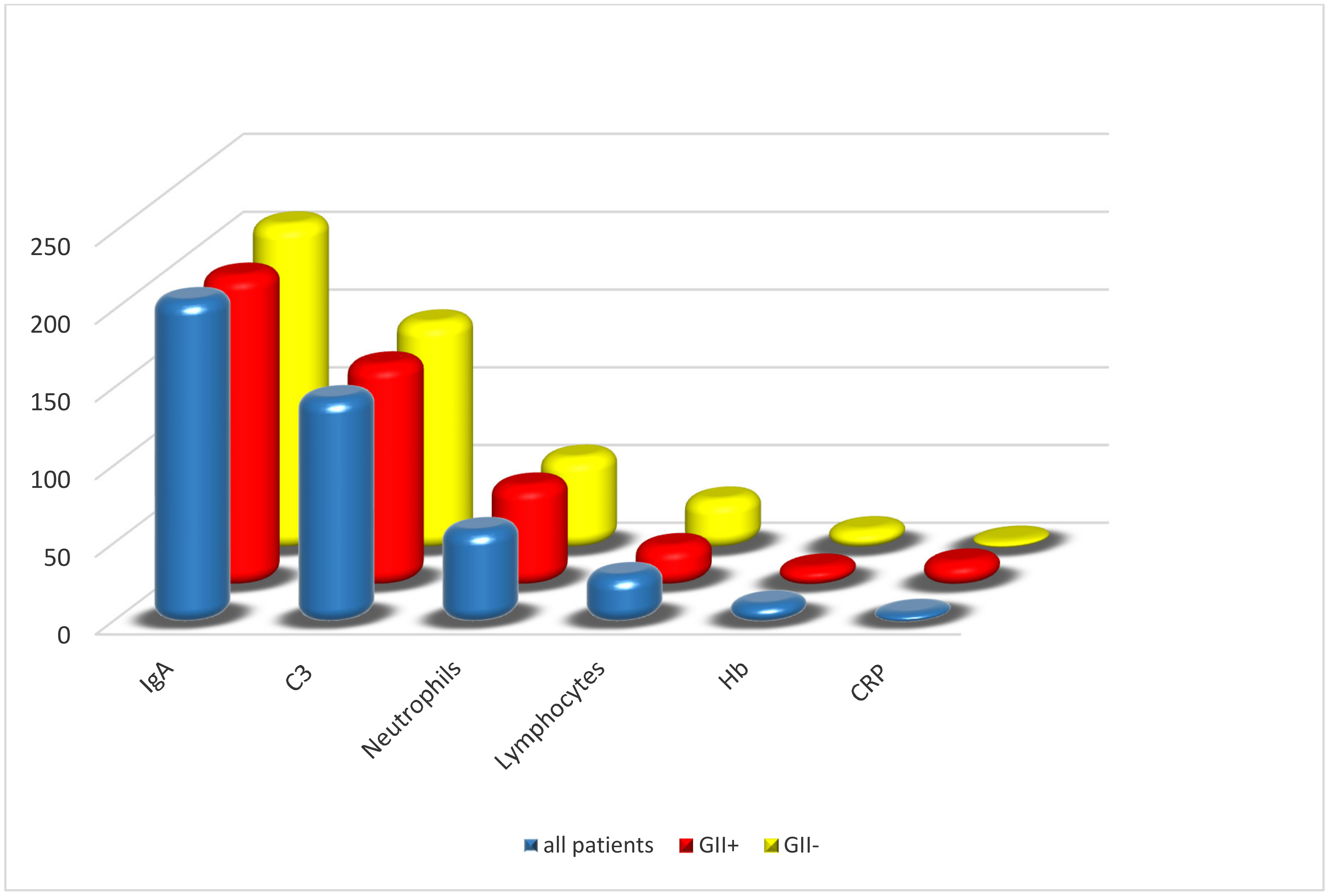
Our retrospective analysis of 195 children with IgAV has revealed that a higher percentage of neutrophils and lower percentage of lymphocytes at the first assessment were significantly associated with the occurrence of gastrointestinal involvement. In addition, a positive S. pyogenes pharyngeal swab, a deficiency of 25(OH)-vitamin D, a persistent purpuric rash for more than 1 month and purpuric lesions in the genital area were associated with gastrointestinal disease. However, multiple logistic regression showed that only low levels of 25(OH)-vitamin D (<30 ng/mL), persistent rash and genital lesions were independently associated with signs of gastrointestinal involvement. Further analysis (both univariate and multivariate) was performed to investigate whether vitamin D deficiency could be associated with other IgAV manifestations: our results found that only 25(OH)-vitamin D deficiency was significantly associated with the occurrence of gastrointestinal manifestations, suggesting that low levels of vitamin D may, at least one-sidedly, contribute to the development of IgAV-related gastrointestinal disease, although diet, medications and eventual comorbidities can influence vitamin D status and bias such results.
A few studies with different sample sizes had already shown that some IgAV patients might have lower serum vitamin D levels than healthy children. Zhu et al. demonstrated that leukotriene B4 was increased and 25(OH)-vitamin D decreased in children with IgAV, speculating that vitamin D deficiency might be correlated with disease severity [
15]. More recently, Wang and Ye retrospectively found that 663 patients with IgAV hospitalized in a single Chinese center during a 3-year-period had reduced vitamin D levels, as did children with IgAV-related nephritis, with both a history of previous streptococcal infection and signs of gastrointestinal involvement, in comparison to 400 healthy sex/age-matched controls, suggesting that maintaining high vitamin D levels might prevent renal damage or complications in other organs [
16]. In addition, Fu et al. found that recurrence rates and the incidence of renal damage in 100 children with IgAV regularly treated with vitamin D for four weeks were significantly lower than those seen in 100 children with IgAV who did not receive vitamin D after 6 months of follow-up [
17].
Several autoimmune diseases tend to share a predisposition to vitamin D deficiency, which might produce an alteration of the microbiome and disrupt the integrity of the intestinal epithelial barrier [
18]. It has been also suggested that vitamin D deficiency may play a role in the immune activation of patients with systemic lupus erythematosus, and have an active part in many comorbidities and even complications of this disorder [
19]. Long-term treatment with vitamin D provided an enhancement of T-reg cells and production of Th2 cytokines in patients with systemic lupus erythematosus [
20]. Moreover, vitamin D supplementation reduced anti-dsDNA positivity in systemic lupus erythematosus, and could possibly reduce the risk of disease recurrence, although further confirmation studies in a larger number of patients are needed [
21]. Low serum concentrations of 25(OH)-vitamin D have been also found in children with Kawasaki disease, possibly contributing to the development of vascular complications in these patients [
22]. Vitamin D deficiency has also been observed in children with periodic fever/aphthosis/pharyngitis/adenitis syndrome, a multifactorial non-hereditary autoinflammatory disorder of childhood, and vitamin D supplementation seemed to significantly reduce the number and overall duration of the typical inflammatory flares of this condition [
23,
24]. Recently, it has been reported that IgAV might have seasonal peaks, reflecting different exposure rates to infectious agents or different levels of sun exposure, which might explain an eventual subsequent hypovitaminosis D [
25].
Despite the general results of our study, some limitations need to be declared as well: the retrospective nature of this analysis, the lack of a control group population, a relatively limited number of IgAV patients due to the single-centered structure of our project, a lack of data related to the dietary habits of the recruited children, and a lacking determination of IgAV prognosis in the long-term.


 ,
, 






{kind=link}
{kind=link}
{kind=link}