Abstract
Global COVID-19 vaccination programs for children and adolescents have been developed with international clinical trial data confirming COVID-19 mRNA vaccine safety and efficacy for the pediatric population. The impact of COVID-19 vaccination in the kidneys is thought to be explained by a complex immune-mediated relationship between the two, although the pathophysiological mechanisms of how COVID-19 vaccination potentially induces kidney pathology are not presently well known. Whilst intrinsic kidney pathologies following COVID-19 vaccination have been reported in adults, such cases are only being recently reported with greater frequency in children and adolescents. Conforming to the PRISMA checklist, we conducted a systematic review of the current literature to provide an overview on the range of intrinsic kidney pathologies that have been reported following COVID-19 vaccination in children and adolescents. All English language research articles published on or before 30 June 2022 reporting new-onset or relapsed intrinsic kidney pathology in children or adolescents (≤18 years) following COVID-19 vaccination were selected for qualitative analysis. Out of 18 cases from the 13 published articles selected, there were 10 cases of IgA nephropathy (1 case of rapidly progressive glomerulonephritis requiring acute hemodialysis), 5 cases of minimal change disease (MCD), 1 case of concurrent MCD/tubulointerstitial nephritis (TIN) and 2 cases of TIN. There is no indication currently to avoid vaccination, unless specific circumstances exist, as the benefits of COVID-19 vaccination far outweigh its risks. Concluding the findings from our systematic review based on preliminary evidence, potential adverse effects to the kidney from COVID-19 vaccination affects a small number of children and adolescents among the many who have been vaccinated. There remains good reason at present to support vaccination of children and adolescents with a greater morbidity status, such as those living with preexisting chronic kidney disease. Close observation of all children and adolescents receiving COVID-19 vaccination is recommended, particularly in those with preceding intrinsic kidney pathology to identify risks of relapsed disease.
1. Introduction
The Coronavirus disease 2019 (COVID-19) pandemic has enormous effects globally, with the disease capable of leading to greater risk of morbidity and mortality within communities [1,2]. There were 6.45 million deaths which occurred worldwide amongst individuals identified with acute COVID-19 infection by the end of July 2022 according to World Health Organization registry data, whether these were directly or indirectly caused by COVID-19 infection [1]. At present, there remain no definitive treatments or prevention strategy to reduce COVID-19 manifestations and mortality. Mass vaccination programs have emerged as the prime strategy from governments to reduce COVID-19 prevalence, following the innovations of various vaccinations targeting COVID-19 [3]. The introduction of vaccination programs complement public health infection mitigation measures that are already advocated since early days of the pandemic [3]. Whilst COVID-19 vaccination programs for replication-defective viral-vectored and messenger RNA (mRNA) vaccines have been ongoing for adults over the past 2 years, administering COVID-19 mRNA vaccinations (Pfizer-BioNTech BNT162b2, Moderna mRNA-1273 from June 2022) for children and adolescents was only recently approved and recommended to be administered through specific regimes only, as clinical trial data on COVID-19 mRNA vaccine safety and efficacy for children and adolescents emerged with greater clarity [4,5,6,7]. All of the clinical trials evaluating safety of the Pfizer-BioNTech BNT162b2 and Moderna mRNA-1273 vaccines have not identified any cases of severe adverse effects in any of the study patients [4,5,6]. The mechanism of mRNA vaccines involve lipid nanoparticle nucleoside-modified mRNA encoding the severe acute respiratory syndrome–related coronavirus-2 (SARS-CoV-2) spike protein, mediating host attachment and SARS-CoV-2 viral entry [8,9].
The effects of COVID-19 vaccination on the kidneys have been widely discussed. It is presumed that a complex immune-mediated relationship exists between the development of various kidney histopathologies and COVID-19 vaccination, although the responsible pathophysiological mechanisms are not well-established as of yet [10,11]. Data relating to the epidemiology, pathophysiology, risk factors and prognosis of individuals with new-onset and relapsed intrinsic kidney pathology following COVID-19 vaccination is reported with greater frequency in adults compared to children and adolescents [12,13,14,15]. Gradually, case reports have been published describing new-onset or relapsed cases of podocytopathy, glomerular disease and other intrinsic kidney pathologies in children and adolescents following COVID-19 vaccination, given that greater numbers of children and adolescents have been receiving COVID-19 vaccinations worldwide. Most of the reported cases are histologically diagnosed following kidney biopsy, whereas some are empirical diagnoses determined through medical history relating to kidney disease and correlation with time of COVID-19 vaccination, non-invasive investigations, and treatment response. Determining the mechanisms of how intrinsic kidney pathology manifests in children and adolescents following COVID-19 vaccination could be more challenging compared to adults, due to the ethical limitations of pursuing invasive kidney biopsy for young children, and the lack of a reliable non-invasive diagnostic test at present [16].
There have been no systematic reviews published to summarize the findings of intrinsic kidney pathology following COVID-19 vaccination in children and adolescents as of July 2022. We conducted a systematic clinical review of the current literature to delineate the range of intrinsic kidney pathologies that have manifested following COVID-19 vaccination in children and adolescents.
2. Materials and Methods
2.1. Eligibility Criteria
All research articles reporting new-onset or relapsed intrinsic kidney pathology in children or adolescents (≤18 years) following COVID-19 vaccination were included. Articles for inclusion described intrinsic kidney pathology in both native and transplanted kidneys. We only selected full-text articles published in the English language for review. Only studies published on or before 30 June 2022 were included.
2.2. Search Strategy and Study Selection
A systematic literature search was conducted by two independent authors (H.H.L.W. and R.C.) in the following databases: “PubMed”, “Web of Science”, “EMBASE” and “Medline-ProQuest”. The search terms incorporated the following: “COVID-19 Vaccination” AND “Kidney Histopathology” AND “Children”; “SARS-CoV-2 Vaccination” AND “Kidney Histopathology” AND “Children”; “COVID-19 Vaccination” AND “Renal Histopathology” AND “Children”; “SARS-CoV-2 Vaccination” AND “Renal Histopathology” AND “Children”; “COVID-19 Vaccination” AND “Kidney Manifestations” AND “Children”; “COVID-19 Vaccination” AND “Renal Manifestations” AND “Children”; “SARS-CoV-2 Vaccination” AND “Kidney Manifestations” AND “Children”; “SARS-CoV-2 Vaccination” AND “Renal Manifestations” AND “Children”; “COVID-19 Vaccination” AND “Nephrotic Syndrome” AND “Children”; “SARS-CoV-2 Vaccination” AND “Nephrotic Syndrome” AND “Children”; “COVID-19 Vaccination” AND “Glomerulonephritis” AND “Children”; “SARS-CoV-2 Vaccination” AND “Glomerulonephritis” AND “Children”; “COVID-19 Vaccination” AND “Nephropathy” AND “Children”; “SARS-CoV-2 Vaccination” AND “Nephropathy” AND “Children”; “COVID-19 Vaccination” AND “Kidney Histopathology” AND “Adolescents”; “SARS-CoV-2 Vaccination” AND “Kidney Histopathology” AND “Adolescents”; “COVID-19 Vaccination” AND “Renal Histopathology” AND “Adolescents”; “SARS-CoV-2 Vaccination” AND “Renal Histopathology” AND “Adolescents”; “COVID-19 Vaccination” AND “Kidney Manifestations” AND “Adolescents”; “COVID-19 Vaccination” AND “Renal Manifestations” AND “Adolescents”; “SARS-CoV-2 Vaccination” AND “Kidney Manifestations” AND “Adolescents”; “SARS-CoV2 Vaccination” AND “Renal Manifestations” AND “Adolescents”; “COVID-19 Vaccination” AND “Nephrotic Syndrome” AND “Adolescents”; “SARS-CoV-2 Vaccination” AND “Nephrotic Syndrome” AND “Adolescents”; “COVID-19 Vaccination” AND “Nephropathy” AND “Adolescents”; “SARS-CoV-2 Vaccination” AND “Nephropathy” AND “Adolescents”; “COVID-19 Vaccination” AND “Glomerulonephritis” AND “Adolescents”; “SARS-CoV-2 Vaccination” AND “Glomerulonephritis” AND “Adolescents”. The articles were screened by H.H.L.W. and R.C. for relevance and duplicate publications were removed. Duplicate screening and the eligibility check was performed by both H.H.L.W. and R.C. The study selection process was carried out using the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines (Figure 1).
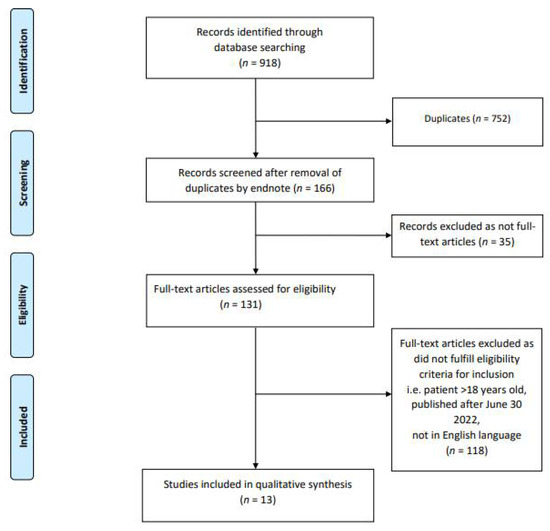
Figure 1.
PRISMA Flow Diagram.
2.3. Data Extraction
If available, data including patient demographics (age, sex and ethnicity), co-morbidities, time to presentation from the day of previous vaccination, clinical presentation, brand of vaccine administered, number of vaccine doses given, kidney parameters pre-vaccination and throughout the time period of acute presentation until most recently reported follow-up (serum creatinine, serum albumin, presence and degree of proteinuria and hematuria), information on whether kidney biopsy was performed, treatment received following diagnosis and clinical outcome following treatment, were extracted from the included articles. These data are described in the results section of this article, and also presented in tabular form.
2.4. Study Registration
A pre-defined review protocol was registered at the PROSPERO international prospective registry of systematic reviews, under registration number CRD42022331838.
3. Results
Our systematic literature search selected 13 articles describing a total of 18 cases of new-onset or relapsed intrinsic kidney pathologies following COVID-19 vaccination in children and adolescents. None of the included cases have had COVID-19 infection diagnosed prior to vaccination. Of these 18 cases, the predominant pathology was IgA nephropathy (10 cases) (Table 1) followed by nephrotic syndrome (6 cases) and tubulointerstitial nephritis (TIN) (2 cases) (Table 2).

Table 1.
Demographics and outcomes of children and adolescents with new-onset and relapsed IgA nephropathy following COVID-19 vaccination.
Table 2.
Demographics and outcomes of children and adolescents with new-onset and relapsed nephrotic syndrome and tubulointerstitial nephritis following COVID-19 vaccination.
3.1. IgA Nephropathy
The mean age of the 10 cases reported with IgA nephropathy was 15 years with a 1:1 male: female ratio. The median time between the day of vaccination and clinical presentation was 1 day. Seven of the ten cases were considered of new-onset with the other three being relapses of histologically diagnosed IgA nephropathy. Amongst the seven new-onset IgA nephropathy cases, four patients have been followed up in clinic for asymptomatic hematuria previously, with no formal histological diagnosis of IgA nephropathy or other intrinsic kidney pathologies. Most of the reported cases occurred following the Pfizer BNT162b2 vaccine (8 cases) and the vaccine brand was unknown in two cases. The majority of patients presented following the second dose of COVID-19 vaccination (7 cases). All of the reported cases presented with gross macroscopic hematuria with varying degrees of proteinuria, of which there is one case of rapidly progressive glomerulonephritis requiring acute hemodialysis because of oliguria. The predominant histopathological changes included crescentic changes in light microscopy and diffuse mesangial deposits of IgA and C3 in immunofluorescence. All patients who had crescentic glomerulonephritis received intravenous pulsed methylprednisolone followed by oral prednisolone and the rest received supportive therapy. Resolution and recovery of kidney function was noted in all cases following treatment [17,18,19,20,21,22,23].
3.2. Nephrotic Syndrome and Tubulointerstitial Nephritis
Nephrotic syndrome was the second commonest clinical presentation to be reported (6 cases) with four being new-onset and two cases being relapses. The mean age of the reported cases was 16 years with the majority of patients being males (4 cases) and having followed Pfizer BNT162b2 vaccine (4 cases). The median time between the day of vaccination and clinical presentation was 7 days. For patients who had kidney biopsies, histopathological changes were predominantly typical of minimal change disease (MCD). One patient presented with an overlap of MCD and TIN. All reported cases had good response to steroid treatment [24,25,26,27,28].
There were two patients presenting with TIN following Pfizer BNT162b2 vaccination. Whist one received steroid treatment, the other case recovered with supportive treatment [29].
4. Discussion
IgA nephropathy appeared as the most frequently reported intrinsic kidney pathology following COVID-19 vaccination. IgA nephropathy is the most common glomerular disease in children and adolescents, with incidences of up to 30% in countries such as Japan and Korea although the global incidence remains variable [30,31]. Approximately 30% of children and adolescents with IgA nephropathy will develop kidney failure within 20 years from diagnosis [32]. The current body of evidence suggests that IgA nephropathy is an immune complex-mediated disease whose pathophysiology involves three immunological processes-excessive production of galactose deficient IgA1 by gut lymphocytes, followed by development of IgG autoantibodies against galactose-deficient IgA1, and mesangial deposition of immune complexes in the kidney superadded by the dysregulation of soluble CD89 (CD89 is an Fc receptor for IgA) and transglutaminase 2 [33,34]. These immunological processes may be induced by an individual’s genetic predisposition (i.e., gene variants encoding galactosylation) and various environmental factors (i.e., infections, dietary imbalances) [33,35]. Vaccine-induced IgA nephropathy was reported in the context of influenza vaccinations, which is annually provided in health systems across most developed countries [36]. It was observed that intramuscular inactivated influenza vaccines elicited hyperresponsiveness in patients with existing IgA nephropathy, leading to excess production of IgA1 monomers [37].
New-onset and relapsed cases of IgA nephropathy have been increasingly reported in adults following COVID-19 vaccination. A greater level of anti-glycan antibody production may partly explain the association between COVID-19 vaccination and IgA nephropathy, given that anti-glycan antibodies cross-react with poorly galactosylated IgA1 and that mucosal immune responses are not stimulated following COVID-19 vaccination [12,38,39]. For mRNA vaccines, another explanation for the association between COVID-19 vaccination and IgA nephropathy relates to increased antibody production [12], as this type of vaccine induces a more potent T-helper cell and B-cell response in the germinal center. It is also acknowledged that many healthy individuals develop spiked IgA production following mRNA-based vaccinations, although the mechanism for this remains unclear [40].
Another scenario which might explain the apparent association between COVID-19 vaccination and IgA nephropathy is the uncovering of subclinical IgA nephropathy following COVID-19 vaccination with the onset of gross hematuria. In Japan, where the majority of IgA nephropathy cases were reported in children and adolescents following COVID-19 vaccination, it was noted that most of these patients (previously with asymptomatic hematuria) were only formally diagnosed as IgA nephropathy because of post-vaccination gross hematuria [19]. Otherwise, they would have continued follow-up in pediatric nephrology clinics once or twice per year for review of asymptomatic hematuria without active intervention as per guidance from the Japan Society of School Health and the Japanese Society for Pediatric Nephrology guidelines [19,41]. The updated Japanese Society for Pediatric Nephrology guidelines have detailed firm guidance for follow-up of asymptomatic hematuria, with kidney biopsy in scenarios where there is persistent proteinuria or hematuria, and recurrent gross hematuria [41]. These measures allow for timely diagnosis of intrinsic kidney pathologies in children and adolescents, whether this is in the context of COVID-19 vaccinations or not.
Nevertheless, detailed evaluation of the 10 IgA nephropathy cases following COVID-19 vaccination in our systematic review did not identify any significant trends between pre-vaccination tests and the timing of onset of post-vaccination symptoms relating to IgA nephropathy. There appear no clear causative associations between COVID-19 vaccination and onset of IgA nephropathy at present. The lack of published literature describing COVID-19 vaccination associated IgA nephropathy is a major limitation, and perhaps more accumulated cases leading to a greater sample size of this presentation would further clarify these associations.
Kidney pathology associated with the clinical presentation of nephrotic syndrome has been reported in children and adolescents following COVID-19 vaccination. MCD encompasses more than 80% of the cases of nephrotic syndrome presentations in children and adolescents [42,43]. The histological changes which occur with the MCD disease process involves the loss of processes at the glomerular visceral epithelial cell-foot, resulting in podocyte effacement, vacuolation and a more rapid growth of microvilli structures in the visceral epithelial cells [43,44,45]. Therefore, patients with MCD are more susceptible to excess proteinuria. The overwhelming majority of nephrotic syndrome presentations in children and adolescents are idiopathic (95% of cases), with the remaining (5% of cases) likely secondary to causes ranging from viral [e.g., Hepatitis B and C, Human Immunodeficiency Virus (HIV)] and inflammatory diseases (e.g., Multisystem inflammatory syndrome in children, Juvenile Idiopathic Arthritis) to less common conditions such as Amyloidosis and Henoch-Schonlein Purpura [46,47,48,49,50,51]. Prior to the COVID-19 pandemic, onset of MCD secondary to vaccination has been reported following the administration of influenza, hepatitis B, pneumococcal, and measles to tetanus–diphtheria–poliomyelitis vaccines [52,53,54,55]. The current theory of MCD pathogenesis is that the condition manifests from complex interactions between T-cells, B-cells, circulating factors, and podocytes [56]. Dysregulation of T-cell mediated immunity is widely speculated to be the main cause of COVID-19 vaccine-induced MCD, with enhanced type 2 T-helper cell activity causing release of cytokines such as interferon-γ and IL-2 leading to increased permeability factor formation [12,57]. This is in contrary to the antibody mediated immune response mechanism purported in COVID-19 vaccine-induced IgA nephropathy. The time for symptom onset in MCD is longer for most reported cases compared to IgA nephropathy.
The three histologically diagnosed cases of TIN in children and adolescents following COVID-19 vaccination are novel. There was a lack of clear-cut co-morbidities and risk factors which might have provided non-COVID-19 explanations for this pathology, but TIN is often an underdiagnosed and under-reported condition and causality is difficult to prove given a myriad of potential confounding factors [58]. The attention directed towards TIN is less compared to glomerular diseases and there are many unanswered questions regarding the temporal association between COVID-19 vaccination and TIN [59,60].
There was another novel case of antineutrophil cytoplasmic antibody (ANCA)-negative and anti-glomerular basement membrane (GBM)-negative crescentic glomerulonephritis manifesting in a 16-year old girl, who presented with dyspnea and headache approximately 6 weeks after receiving her second dose of the Pfizer BioNTech BNT162b2 vaccine [61]. The patient required acute dialysis for 2 weeks, and subsequently recovered with oral steroid and mycophenolate mofetil therapy. This case report by Kim and colleagues was published in July 2022, and hence not included in our systematic review. The authors postulated that vaccine-induced autoimmunity may have caused the development of subsequent glomerulonephritis after mRNA-based vaccination, similar to that of the IgA nephropathy cases.
From the 18 cases reported in our systematic review, the majority of cases were reported in Asia (12 cases) in which Japan (7 cases, with 6 of the 7 cases being IgA nephropathy) as most prominent. This could largely be attributed to the well-established national school urinalysis screening system in Japan, where successes in early detection of subclinical glomerulonephritis have been documented [41,62,63]. Furthermore, it is noticeable that all of the case reports occurred in developed countries (all in the ‘very high’ category of the inequality-adjusted human development index) [64]. mRNA vaccination programs for children and adolescents were only introduced in developed countries in recent months, with pediatric-dosed vaccines now being more available and accessible. No international registry data is currently available documenting the number of vaccine doses administered to children and adolescents throughout the time period covered by our systematic review. Individual national registries such as those from the United States (e.g., American Academy of Pediatrics) and Australia (e.g., Australian Government Department of Health and Aged Care) have recorded the prevalence of children and adolescents receiving COVID-19 vaccinations during this period [65,66]. For example, between March 11 2022 and 29 June 2022 in the United States, 36% of children aged 5 to 11 received the 1st dose whilst 28% of children received the 2nd dose of either Pfizer-BioNTech BNT162b2 or Moderna mRNA-1273 vaccine [65]. During a similar time period in Australia for children aged 5 to 15 years, 52.3% received the 1st dose whilst 39.5% of children received the 2nd dose of either Pfizer-BioNTech BNT162b2 or Moderna mRNA-1273 vaccine [66]. Due to the recency of COVID-19 vaccine roll-out for children and adolescents, our understanding of any indication of a global rise in kidney injury incidence since the period of vaccine roll-out for children and adolescents is limited at present. Going forward, we anticipate efforts to establish international registry data to monitor for this.
Overall, the relative lack of reported cases at present makes it difficult to synthesize a summary of overall findings and be confident about the links, if any, between the number of COVID-19 vaccination doses and risks of developing intrinsic kidney pathology. There are no case–control or cohort studies available in the topic area to conduct a meta-analysis. Hence, the article is presented as a descriptive systematic review with only case reports being identified from our search process. Furthermore, our analysis was inevitably limited in concluding significant associations between baseline morbidity profile, investigation results (e.g., serum creatinine), the nature of one’s acute clinical presentation and their eventual outcomes amongst the included cases. Exact duration of hospitalization was only documented for 2 cases amongst those included for detailed evaluation, and the completeness and detail in which serum and urinary investigation results were reported by authors of the included cases have been inconsistent. The majority of these cases occurred too recently for us to determine how patients have evolutionized post-treatment from the reported episode of intrinsic kidney pathology developing following COVID-19 vaccination. Apart from the single case of IgA nephropathy with rapidly progressive glomerulonephritis in which acute hemodialysis was indicated because of oliguric symptoms, all of the other cases included in this systematic review recovered well from their presenting episode with supportive treatment and/or steroid therapy. It is also quite possible that children presenting with IgA nephritis following vaccination actually had previously undiagnosed IgA disease.
5. Conclusions
In conclusion, our systematic review summarizes currently reported intrinsic kidney pathologies which manifested in children and adolescents following COVID-19 vaccination. Based on these preliminarily reported cases, the potential immune-mediated relationship between COVID-19 vaccines and onset of various intrinsic kidney pathologies has been explored. It should be acknowledged that the number of reported cases of intrinsic kidney pathology developing following COVID-19 vaccination is very small in relation to the hundreds of millions of vaccinations that have already occurred in children and adolescents, and that the protective benefits offered by COVID-19 vaccinations far outweigh its risks. At present, there is no indication to avoid vaccination unless specific circumstances exist. On the contrary, there have been reported serious complications associated with COVID-19 infection in pediatric patients with kidney disease, which reinforces the importance of COVID-19 vaccination in this vulnerable group [67]. In the future, we recommend the continued development and expansion of COVID-19 vaccination programs worldwide and keeping a watchful eye on children and adolescents with preexisting kidney disease. From the recency of cases included in this systematic review, and the relative lack of published data addressing the association between development of new-onset or relapsed intrinsic kidney pathologies and COVID-19 vaccination in children and adolescents, further reports and primary research will be needed to provide greater clarification on possible pathophysiological associations.
Author Contributions
Conceptualization, H.H.L.W. and R.C.; Methodology, H.H.L.W. and R.C.; software, H.H.L.W. and R.C.; Validation, H.H.L.W., P.A.K. and R.C.; Formal Analysis, H.H.L.W. and R.C.; Investigation, H.H.L.W. and R.C.; Resources, H.H.L.W. and R.C.; Data Curation, H.H.L.W.; Writing—original draft preparation, H.H.L.W. and R.C.; Writing—review and editing, M.S. and P.A.K.; Visualization, H.H.L.W., P.A.K., M.S. and R.C.; Supervision, P.A.K. and R.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 18 September 2022).
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Ewer, K.J.; Barrett, J.R.; Belij-Rammerstorfer, S.; Sharpe, H.; Makinson, R.; Morter, R.; Flaxman, A.; Wright, D.; Bellamy, D.; Bittaye, M.; et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 2021, 27, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Ali, K.; Berman, G.; Zhou, H.; Deng, W.; Faughnan, V.; Coronado-Voges, M.; Ding, B.; Dooley, J.; Girard, B.; Hillebrand, W.; et al. Evaluation of mRNA-1273 SARS-CoV-2 vaccine in adolescents. N. Engl. J. Med. 2021, 385, 2241–2251. [Google Scholar] [CrossRef]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 COVID-19 vaccine in children 5 to 11 years of age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Creech, C.B.; Anderson, E.; Berthaud, V.; Yildirim, I.; Atz, A.M.; Melendez Baez, I.; Finkelstein, D.; Pickrell, P.; Kirstein, J.; Yut, C.; et al. Evaluation of mRNA-1273 COVID-19 vaccine in children 6 to 11 years of age. N. Engl. J. Med. 2022, 386, 2011–2023. [Google Scholar] [CrossRef]
- FDA. FDA Briefing Document: EUA Amendment Request for Use of the Moderna COVID-19 Vaccine in Children 6 Months through 17 Years of Age. Available online: https://www.fda.gov/media/159189/download (accessed on 18 July 2022).
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef]
- Pegu, A.; O’Connell, S.E.; Schmidt, S.D.; O’Dell, S.; Talana, C.A.; Lai, L.; Albert, J.; Anderson, E.; Bennett, H.; Corbett, K.S.; et al. Durability of mRNA-1273 vaccine–induced antibodies against SARS-CoV-2 variants. Science 2021, 373, 1372–1377. [Google Scholar] [CrossRef]
- Kronbichler, A.; Anders, H.J.; Fernandez-Juárez, G.M.; Floege, J.; Goumenos, D.; Segelmark, M. Immunonephrology Working Group of the ERA-EDTA (European Renal Association—European Dialysis and Transplant Association). Recommendations for the use of COVID-19 vaccines in patients with immune-mediated kidney diseases. Nephrol. Dial. Transplant. 2021, 36, 1160–1168. [Google Scholar] [CrossRef]
- Stevens, K.I.; Frangou, E.; Shin, J.I.; Anders, H.J.; Bruchfeld, A.; Schönermarck, U.; Hauser, T.; Westman, K.; Fernandez-Juarez, G.M.; Floege, J.; et al. Perspective on COVID-19 vaccination in patients with immune-mediated kidney diseases: Consensus statements from ERA-IWG and EUVAS. Nephrol. Dial. Transplant. 2022, 37, 1400–1410. [Google Scholar] [CrossRef]
- Wu, H.H.L.; Kalra, P.A.; Chinnadurai, R. New-Onset and Relapsed Kidney Histopathology Following COVID-19 Vaccination: A Systematic Review. Vaccines 2021, 9, 1252. [Google Scholar] [CrossRef]
- Fenoglio, R.; Lalloni, S.; Marchisio, M.; Oddone, V.; De Simone, E.; Del Vecchio, G.; Sciascia, S.; Roccatello, D. New Onset Biopsy-Proven Nephropathies after COVID Vaccination. Am. J. Nephrol. 2022, 53, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Bomback, A.S.; Kudose, S.; D’Agati, V.D. De novo and relapsing glomerular diseases after COVID-19 vaccination: What do we know so far? Am. J. Kidney Dis. 2021, 78, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Li, N.L.; Coates, P.T.; Rovin, B.H. COVID-19 vaccination followed by activation of glomerular diseases: Does association equal causation? Kidney Int. 2021, 100, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Alshami, A.; on behalf of the Pediatric Nephrology Clinical Pathway Development Team; Roshan, A.; Catapang, M.; Jöbsis, J.J.; Kwok, T.; Polderman, N.; Sibley, J.; Sibley, M.; Mammen, C.; et al. Indications for kidney biopsy in idiopathic childhood nephrotic syndrome. Pediatr. Nephrol. 2017, 32, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Hanna, C.; Hernandez, L.P.; Bu, L.; Kizilbash, S.; Najera, L.; Rheault, M.N.; Czyzyk, J.; Kouri, A.M. IgA nephropathy presenting as macroscopic hematuria in 2 pediatric patients after receiving the Pfizer COVID-19 vaccine. Kidney Int. 2021, 100, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Horino, T.; Sawamura, D.; Inotani, S.; Ishihara, M.; Komori, M.; Ichii, O. Newly diagnosed IgA nephropathy with gross haematuria following COVID-19 vaccination. QJM Int. J. Med. 2022, 115, 28–29. [Google Scholar] [CrossRef]
- Okada, M.; Kikuchi, E.; Nagasawa, M.; Oshiba, A.; Shimoda, M. An adolescent girl diagnosed with IgA nephropathy following the first dose of the COVID-19 vaccine. CEN Case Rep. 2022, 11, 376–379. [Google Scholar] [CrossRef]
- Niel, O.; Florescu, C. IgA nephropathy presenting as rapidly progressive glomerulonephritis following first dose of COVID-19 vaccine. Pediatr. Nephrol. 2022, 37, 461–462. [Google Scholar] [CrossRef]
- Morisawa, K.; Honda, M. Two patients presenting IgA nephropathy after COVID-19 vaccination during a follow-up for asymptomatic hematuria. Pediatr. Nephrol. 2022, 37, 1695–1696. [Google Scholar] [CrossRef]
- Udagawa, T.; Motoyoshi, Y. Macroscopic hematuria in two children with IgA nephropathy remission following Pfizer COVID-19 vaccination. Pediatr. Nephrol. 2022, 37, 1693–1694. [Google Scholar] [CrossRef]
- Abdel-Qader, D.H.; Alkhatatbeh, I.H.; Hayajneh, W.; Annab, H.; Al Meslamani, A.Z.; Elmusa, R.A. IgA nephropathy in a pediatric patient after receiving the first dose of Pfizer-BioNTech COVID-19 vaccine. Vaccine 2022, 40, 2528–2530. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, E.; Uchimura, T.; Hirai, Y.; Togashi, H.; Oyama, Y.; Inaba, A.; Shiga, K.; Ito, S. New-onset pediatric nephrotic syndrome following Pfizer-BioNTech SARS-CoV-2 vaccination: A case report and literature review. CEN Case Rep. 2022, 11, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Pella, E.; Sarafidis, P.A.; Alexandrou, M.E.; Stangou, M.; Nikolaidou, C.; Kosmidis, D.; Papagianni, A. De novo Minimal Change Disease in an Adolescent after Pfizer-BioNTech COVID-19 Vaccination: A Case Report. Case Rep. Nephrol. Dial. 2022, 12, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Alhosaini, M.N. A Case of Minimal Change Disease after SARS-CoV-2 Vaccination under the Age of 18. Avicenna J. Clin. Med. 2022, 12, 31–33. [Google Scholar] [CrossRef]
- Jongvilaikasem, P.; Rianthavorn, P. Minimal change disease and acute interstitial nephritis following SARS-CoV-2 BNT162b2 vaccination. Pediatr. Nephrol. 2022, 37, 1419–1421. [Google Scholar] [CrossRef]
- Güngör, T.; Yazılıtaş, F.; Kargın Çakıcı, E.; Karakaya, D.; Bülbül, M. Relapse of Idiopathic Nephrotic Syndrome After SARS-CoV-2 Vaccination: Two Case Reports. J. Paediatr. Child Health 2022, 58, 939–940. [Google Scholar] [CrossRef]
- Choi, J.H.; Kang, K.S.; Han, K.H. Two adolescent cases of acute tubulointerstitial nephritis after second dose of COVID-19 mRNA vaccine. Hum. Vaccin. Immunother. 2022, 18, 2059308. [Google Scholar] [CrossRef]
- Coppo, R. Pediatric IgA Nephropathy in Europe. Kidney Dis. 2019, 5, 182–188. [Google Scholar] [CrossRef]
- Hogg, R.J. Idiopathic immunoglobulin A nephropathy in children and adolescents. Pediatr. Nephrol. 2010, 25, 823–829. [Google Scholar] [CrossRef][Green Version]
- Gutiérrez, E.; Carvaca-Fontán, F.; Luzardo, L.; Morales, E.; Alonso, M.; Praga, M. A personalized update on IgA nephropathy: A new vision and new future challenges. Nephron 2020, 144, 555–571. [Google Scholar] [CrossRef]
- Knoppova, B.; Reily, C.; Maillard, N.; Rizk, D.V.; Moldoveanu, Z.; Mestecky, J.; Raska, M.; Renfrow, M.B.; Julian, B.A.; Novak, J. The origin and activities of IgA1-containing immune complexes in IgA nephropathy. Front. Immunol. 2016, 7, 117. [Google Scholar] [CrossRef] [PubMed]
- Yeo, S.C.; Cheung, C.K.; Barratt, J. New insights into the pathogenesis of IgA nephropathy. Pediatr. Nephrol. 2018, 33, 763–777. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.N. Pathogenesis of IgA nephropathy. Nat. Rev. Nephrol 2012, 8, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.; Shah, H.H. Vaccine-associated kidney diseases: A narrative review of the literature. Saudi J. Kidney Dis. Transpl. 2019, 30, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Van den Wall Bake, A.W.; Beyer, W.E.; Evers-Schouten, J.H.; Hermans, J.; Daha, M.R.; Masurel, N.; Van Es, L.A. Humoral immune response to influenza vaccination in patients with primary immunoglobulin A nephropathy. An analysis of isotype distribution and size of the influenza-specific antibodies. J. Clin. Investig. 1989, 84, 1070–1075. [Google Scholar] [CrossRef] [PubMed]
- Abramson, M.; Yu, S.M.; Campbell, K.N.; Chung, M.; Salem, F. IgA nephropathy after SARS-CoV-2 vaccination. Kidney Med. 2021, 3, 860–863. [Google Scholar] [CrossRef]
- Zhao, X.; Chen, H.; Wang, H. Glycans of SARS-CoV-2 spike protein in virus infection and antibody production. Front. Mol. Biosci. 2021, 8, 53. [Google Scholar] [CrossRef]
- Wisnewski, A.V.; Luna, J.C.; Redlich, C.A. Human IgG and IgA responses to COVID-19 mRNA vaccines. PLoS ONE 2021, 16, e0249499. [Google Scholar] [CrossRef]
- The Japanese Society for Pediatric Nephrology. The 2020 Japanese Society for Pediatric Nephrology guidelines for pediatric IgA nephropathy. Shindan to Chiryo-sya; The Japanese Society for Pediatric Nephrology: Tokyo, Japan, 2020. [Google Scholar]
- Noone, D.G.; Iijima, K.; Parekh, R. Idiopathic nephrotic syndrome in children. Lancet 2018, 392, 61–74. [Google Scholar] [CrossRef]
- Meyrier, A.; Niaudet, P. Acute kidney injury complicating nephrotic syndrome of minimal change disease. Kidney Int. 2018, 94, 861–869. [Google Scholar] [CrossRef]
- Vivarelli, M.; Massella, L.; Ruggiero, B.; Emma, F. Minimal change disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Bertelli, R.; Bonanni, A.; Caridi, G.; Canepa, A.; Ghiggeri, G.M. Molecular and cellular mechanisms for proteinuria in minimal change disease. Front. Med. 2018, 5, 170. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, P.L.; Ferreira-Centeno, A.; Farkas-Szallasi, T.; Abraham, A.A.; Garrett, C.T. Viral DNA in microdissected renal biopsy tissue from HIV infected patients with nephrotic syndrome. Kidney Int. 1993, 43, 1347–1352. [Google Scholar] [CrossRef]
- Gupta, A.; Quigg, R.J. Glomerular diseases associated with hepatitis B and C. Adv. Chronic. Kidney Dis. 2015, 22, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Rowley, A.H. Understanding SARS-CoV-2-related multisystem inflammatory syndrome in children. Nat. Rev. Immunol. 2020, 20, 453–454. [Google Scholar] [CrossRef] [PubMed]
- Kari, J. Steroid-sensitive nephrotic syndrome and juvenile idiopathic arthritis. Pediatr. Nephrol. 2002, 11, 975–976. [Google Scholar] [CrossRef]
- Bilginer, Y.; Akpolat, T.; Ozen, S. Renal amyloidosis in children. Pediatr. Nephrol. 2011, 26, 1215–1227. [Google Scholar] [CrossRef]
- Tan, J.; Tang, Y.; Xu, Y.; Yan, S.; Xu, Y.; Tan, L.; Zhong, Z.; Tarun, P.; Qin, W. The clinicopathological characteristics of Henoch-Schönlein purpura nephritis with presentation of nephrotic syndrome. Kidney Blood Press Res. 2019, 44, 754–764. [Google Scholar] [CrossRef]
- Gutiérrez, S.; Dotto, B.; Petiti, J.P.; Paul, A.L.; Dionisio de Cabalier, M.E.; Torres, A.I.; Mukdsi, J.H. Minimal change disease following influenza vaccination and acute renal failure: Just a coincidence? Nefrología 2012, 32, 414–415. [Google Scholar]
- Weijers, J.; Alvarez, C.; Hermans, M.M. Post-vaccinal minimal change disease. Kidney Int. 2021, 100, 459–461. [Google Scholar] [CrossRef]
- Kikuchi, Y.; Imakiire, T.; Hyodo, T.; Higashi, K.; Henmi, N.; Suzuki, S.; Miura, S. Minimal change nephrotic syndrome, lymphadenopathy and hyperimmunoglobulinemia after immunization with a pneumococcal vaccine. Clin. Nephrol. 2002, 58, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Clajus, C.; Spiegel, J.; Bröcker, V.; Chatzikyrkou, C.; Kielstein, J.T. Minimal change nephrotic syndrome in an 82 year old patient following a tetanus-diphteria-poliomyelitis-vaccination. BMC Nephrol. 2009, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Horinouchi, T.; Nozu, K.; Iijima, K. An updated view of the pathogenesis of steroid-sensitive nephrotic syndrome. Pediatr. Nephrol. 2022, 37, 1957–1965. [Google Scholar] [CrossRef]
- Kaklamanos, A.; Belogiannis, K.; Skendros, P.; Gorgoulis, V.G.; Vlachoyiannopoulos, P.G.; Tzioufas, A.G. COVID-19 Immunobiology: Lessons Learned, New Questions Arise. Front. Immunol. 2021, 12, 719023. [Google Scholar] [CrossRef]
- León-Román, J.; Agraz, I.; Vergara, A.; Ramos, N.; Toapanta, N.; García-Carro, C.; Gabaldón, A.; Bury, R.; Bermejo, S.; Bestard, O. COVID-19 infection and renal injury: Where is the place for acute interstitial nephritis disease? Clin. Kidney J. 2022, 15, 1698–1704. [Google Scholar] [CrossRef]
- Wu, H.H.L.; Li, J.W.C.; Bow, A.; Woywodt, A.; Ponnusamy, A. Acute interstitial nephritis following SARS-CoV-2 vaccination. Clin. Kidney J. 2022, 15, 576–581. [Google Scholar] [CrossRef]
- Storrar, J.; Kudose, S.; Woywodt, A. Have we missed AINything? Acute interstitial nephritis in SARS-CoV-2 infection and vaccination. Clin. Kidney J. 2022, 15, 1643–1652. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Jung, J.; Cho, H.; Lee, J.; Go, H.; Lee, J.H. A child with crescentic glomerulonephritis following SARS-CoV-2 mRNA (Pfizer-BioNTech) vaccination. Pediatr. Nephrol. 2022, 1–4. [Google Scholar] [CrossRef]
- Sakai, T.; Kitagawa, T. Screening system for asymptomatic renal disease in children in Japan. Pediatr. Int. 1990, 32, 677–681. [Google Scholar] [CrossRef]
- Imai, E.; Yamagata, K.; Iseki, K.; Iso, H.; Horio, M.; Mkino, H.; Hishida, A.; Matsuo, S.; Fine, D.M.; Garg, N. Kidney disease screening program in Japan: History, outcome, and perspectives. Clin. J. Am. Soc. Nephrol. 2007, 2, 1360–1366. [Google Scholar] [CrossRef]
- Hicks, D.A. The inequality-adjusted human development index: A constructive proposal. World Dev. 1997, 25, 1283–1298. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Children and COVID-19 Vaccinations Trends AAP Analysis of Data Posted by the Centers for Disease Control and Prevention as of 29 June 2022. Available online: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-vaccination-trends/ (accessed on 18 September 2022).
- Australian Government Department of Health and Aged Care. COVID-19 Vaccination Numbers and Statistics. Available online: https://www.health.gov.au/initiatives-and-programs/covid-19-vaccines/numbers-statistics (accessed on 18 September 2022).
- Ionescu, M.D.; Balgradean, M.; Cirstoveanu, C.G.; Balgradean, I.; Popa, L.I.; Pavelescu, C.; Capitanescu, A.; Berghea, E.; Filip, C. Myopericarditis Associated with COVID-19 in a Pediatric Patient with Kidney Failure Receiving Hemodialysis. Pathogens 2021, 10, 486. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).