Highlights
What are the main findings?
- Psychomotor intervention promotes development in preschool children with autism spectrum disorder by enhancing psychomotor and socio-emotional competence.
- A formal consensus process involving 39 Portuguese experts was conducted to generate expert consensus on psychomotor intervention guidelines for preschool children with ASD.
What is the implication of the main finding?
- The experts agreed on 88 statements, grouped under 16 sections, reflecting generic psychomotor intervention guidelines.
- The consensus guidelines may support transparent and standard psychomotor interventions, but further studies are needed to determine their efficacy.
Abstract
Psychomotor intervention has been used to promote development by the enhancement of psychomotor and socio-emotional competence. However, studies with high-quality evidence, describing psychomotor-intervention processes and outcomes are scarce. Therefore, we aimed to generate expert consensus regarding psychomotor-intervention guidelines to support psychomotor therapists through the design and implementation of interventions for preschool (3–6 years old) children with autism spectrum disorder (ASD). A formal consensus process was carried out, using modified nominal group (phase I) and Delphi survey (phase II) techniques. We recruited 39 Portuguese experts in psychomotor intervention with preschool children with ASD in phase I. Experts participated in at least one of the five online meetings, discussing themes (e.g., objectives, methods, strategies) concerning psychomotor intervention with preschool children with ASD. A deductive thematic analysis from phase I resulted in 111 statements composing round 1 of the Delphi survey. Thirty-five experts completed round 1, and 23 round 2. The experts reached a consensus (agreement > 75%) on 88 statements, grouped under 16 sections, (e.g., intervention source, general setting, intended facilitation-style), reflecting generic psychomotor-intervention guidelines. Consensus guidelines may be used to support transparent and standard psychomotor interventions, although further studies should be undertaken to determine their efficacy.
1. Introduction
Psychomotor intervention, also known as psychomotor therapy or psychomotricity, is a specific intervention modality focused on body movement-centered approaches for mental health, facilitated by a psychomotor therapist [1,2]. Psychomotor intervention is focused on an integrated perspective of the human being and the importance of body and movement on the development of an individual’s competency within a psychosocial context, where body and mind dimensions interact with each other [2]. Psychomotor intervention provided across healthcare, social, and educational settings has been recognized in several European, Central and South American countries. Depending on the purpose of the intervention, preventive or therapeutic approaches are used with children with typical development and with specific health needs. Psychomotor interventions focused on preventive approaches have shown positive results in the development of preschool children [3,4,5,6,7] as well as therapeutic approaches which have demonstrated benefits for children aged 3–6 years with special healthcare needs, namely, with autism spectrum disorder (ASD) [8,9,10].
Considering that motor delays are present among the earliest markers of ASD, with a prevalence reported in more than 80% of children diagnosed [11,12], and that motor skills during play with peers and caregivers are critical to developing social interactions and engagement [13,14], psychomotor interventions can be regarded as beneficial for children with ASD. However, with a broader scope, psychomotor as well as other movement-based practices, i.e., interventions that that use physical exertion, specific motor skills/ techniques, or mindful movement to target a variety of skills and behaviors [15] (p.4024) have insufficient evidence, although positive effects were identified [15,16,17]. Review studies on the effects of psychomotor intervention with children reinforce the scarcity of high-quality evidence [10,18] specifically with children with ASD, since most studies are case-control studies or case reports, with insufficient (or even contradictory) results and with no clear or detailed description of the implementation of practices provided [10,18]. As with other health professions [19,20,21], decisions about psychomotor intervention practices should be evidence-based, so that the best practices are implemented. Since there is limited evidence guiding professionals on how to provide such high-quality interventions, it is necessary to identify these specific features.
So far, only general guidelines on non-pharmacologic evidence-based interventions have been published to support professionals working with children with autism and their families [22,23,24,25]. International recommendations include individualized programming for each child; ongoing program evaluation; interventions emphasizing attention, imitation, communication, play, social interaction, regulation, and self-advocacy; a highly supportive environment; predictability and structure in the sessions; functional analysis of possible behavior problems; and family involvement. In Portugal, individualized intervention according to the child profile and contexts with both therapeutic and educational components are recommended [26], although no specific guidelines for psychomotor intervention has been provided.
When scientific evidence is either insufficient or conflicting, consensus protocols, where experts come to an agreement on recommendations, provide an alternative approach to develop guidance, in order to enhance implementation and fidelity among professionals. The Consolidated Standards of Reporting Trials for social and psychological interventions (CONSORT-SPI 2018) is an example of an instrument that guides behavioral and social researchers to report studies transparently [27].
The World Health Organization (2014) has recognized the need to use formal consensus methods in the development of clinical practice guidelines, and often uses the NGT and Delphi technique to identify stakeholders’ priorities for integration into healthcare recommendations [28,29,30,31]. The nominal group technique (NGT) and the Delphi technique are used as a consensus approach for integrating knowledge [32]. In this study, we aim to develop consensus guidelines regarding specific characteristics of psychomotor interventions for preschool children with ASD.
2. Methods
2.1. Selection and Recruitment of Participants
In the present study, academic and professional experts in psychomotor intervention with preschool children with ASD. were recruited. The ‘snowball’ technique was used to select the group of experts. In total, 70 Portuguese experts were invited by email, and provided them with information about the aim, conditions, and procedures of the study. First, the invited experts filled out an online form to gather their details regarding academic/professional experience, personal data and availability to meet and to complete online surveys.
The inclusion criteria were:
- (a)
- Have at least a bachelor’s degree in Psychomotor Therapy.
AND
- (b)
- Be a psychomotor therapist with more than three years of experience in psychomotor intervention in different contexts in Portugal, working either individually or in groups (using therapeutic or educational approaches).
OR
- (c)
- Be a researcher or university professor with scientific/professional expertise in preschool children with ASD, in psychomotor intervention.
The experts’ demographic characterization is presented in the following Table 1.

Table 1.
Experts demographics.
2.2. Procedures
The study was approved by the Faculty of Human Kinetics Ethics Council (reference number 48/2021 on 29 November 2021). Experts did not receive any payment for participation. Written informed consent to take part in this study was obtained from all participants.
The most common approaches to consensus development in healthcare and clinical fields are: the nominal group technique; the Delphi technique; and the consensus-development conference [33]. The nominal and Delphi technique chosen involve a group of ‘experts’ generating ideas and determining priorities [32]. Both are equally effective, and more effective than conventional interacting groups [30]. This study design comprised a combination of modified nominal group and Delphi techniques (see Figure 1) [32].
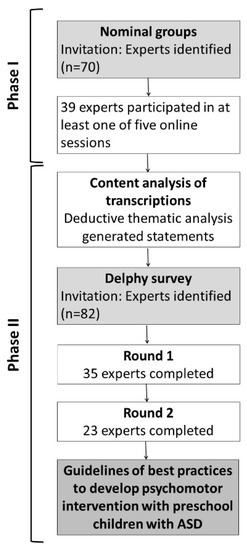
Figure 1.
Phases of the consensus approach and experts involved.
2.2.1. Phase I: Nominal Group Technique (NGT)
The NGT, a formal structured consensus-development method to integrate experts’ points of view in order to gain consensus, followed recommendations proposed by McMillan and colleagues [32,34]. First, researchers informed the participants of the aim and importance of group-expert meetings, and then online meetings on the Zoom platform took place in groups (n = 5) of 5 to 7 participants, over a 3-month period from April to June 2021. Two facilitators were responsible for the experts’ meetings: a primary facilitator leading the meetings, and an independent researcher responsible for writing down the experts’ ideas. Upon consent, meetings were recorded, transcribed and coded.
Regarding the meetings, initially a brief study-overview was presented. In each meeting, a research question was presented and discussed for 60–90 min. The questions were selected upon an initial scoping review of psychomotor intervention practices with preschool children with ASD [10], which included: (1) objectives and primary results, (2) theories and models, (3) methods, (4) environmental arrangements, and (5) strategies (see all questions in Appendix A, Table A1). Each meeting followed the four stages of NGT [32,34]: silent generation, round robin, clarification, and ranking.
In that last stage, instead of allowing participants to vote on their preferred ideas as in the traditional NGT technique, participants were invited to propose categories and then rate them, from the generated list. The rating on a scale from 1 (not at all) to 5 (extremely essential or important) concerned how essential or important the ideas were in each category. This rating process was completed individually on an online form, without any group discussion. The ratings results were given to the experts by email after each meeting.
2.2.2. Delphi Technique
After the content-analysis of transcriptions and rated categories in the NGT, three researchers (A.F., S.S. and P.L.), drafted consensus statements for the Delphi survey. The guidelines’ survey statements followed the NICE writing principles [35], and were organized into sections and themes (see Table 2), adapting a checklist designed to improve the reporting of group-based interventions [36]. This checklist included the main elements of an intervention program, according to the CONSORT-SPI 2018 [27].
Table 2.
Themes (sections) obtained in the NGT.
The Delphi survey, with two rounds, was conducted over a 4-month period from February to May 2022. The anonymization of responses was guaranteed. Before each round, experts received an email with a link to access the survey. Each statement was accompanied by a 9-point hedonic scale asking for the indication of the agreement level (with 1 indicating ‘completely disagree’ and 9 ‘completely agree’). In addition, respondents were encouraged to give open-ended comments for each statement. Since the NGT was used in the first step, the Delphi technique skipped the first traditional rounds. Instead, each round was analyzed on completion, with the results contributing to the content of the subsequent round. Only experts who completed the first survey round were invited to participate in the next round [31]. Only statements with a median score greater than 7 were accepted. A second round of the survey was provided, since less than 75% of given statements scored below 7 [31,37]. The Delphi survey process terminated when consistency responses between rounds achieved 85%, i.e., more than 85% of the same statements showed consensus in two rounds, reflecting a substantial majority on topics about psychomotor intervention practices with preschool children with ASD.
2.3. Data Management and Analysis
2.3.1. Phase I
In the NGT, both qualitative and quantitative (numerical rankings) data was obtained.
Excel spread sheets from Google forms were used to gather experts rankings. Descriptive data was used for the results. Each NGT focus group was recorded via the Zoom platform, and written field notes were taken. The traditional approach of reading the transcribed audio recordings and listening to the recordings for verification of the text, was used.
2.3.2. Phase II
The statements of the Delphi survey emerged from the content analysis of phase I. Based on the output of the NGT meetings, a thematic text analysis for identifying, analyzing and reporting patterns (themes) across transcriptions of the meetings was conducted, using MAXQDA software. The thematic analysis was chosen since it follows a theoretical (deductive) approach based on the literature review [38]. This method is not associated with a pre-existing theoretical framework [38]. Data familiarization, generation of initial codes, searching the data for themes, reviewing themes, and reaching agreement for defining themes, was conducted. The initial themes (codes) were generated by one researcher (A.F.). Two researchers (S.S. and P.L.) independently reviewed the themes where an agreement was not reached. Concerning the theme “change techniques”, the play types followed a typology defined in Tool for Observing Play Outdoors [39]. The themes in the transcriptions that were rated higher and emerged more frequently across meetings were the basis used to generate the statements. In the Delphi technique, the frequency of responses for each statement (item) was calculated. If the statement had a rating of 7–9 among at least 75% of experts, this meant that consensus had been reached. The statements that did not complete this criterion were excluded. The included statements were forwarded to the subsequent round for re-rating. From round one to round two, four researchers (A.F., C.S., S.S. and P.L.) analyzed the data and reformulated or included statements, considering the experts’ comments.
3. Results
The experts’ mean age (M = 37) ranged from 26 to 68, most being female (98%). The majority of respondents were practitioners working in the field for at least five years, predominantly in a clinic and/or home context.
3.1. Phase I
The first NGT meeting involved 39 Portuguese experts, where 35 were psychomotor therapists and 4 researchers in psychomotor intervention (Table 1). Approximately 80% of them participated in all meetings.
The NGT was used to inform guideline development through the generation and prioritization of topics, with experts being asked questions such as, “What theories or models support psychomotor intervention with children with ASD (3–6 years)?”; “What are the strategies you use most (in individual and/or group intervention)?” (see Appendix A). Following the rating of each item, experts were asked to select their “top five”, in terms of relevance. From the first meeting, and after the independent analysis of the responses concerning the objectives and primary results of the psychomotor intervention, a list of 19 categories were identified. The most relevant/priority categories proposed were: social interaction, (non-verbal) communication, playfulness, self-regulation, and psychomotor skills. From the second meeting, a list of 29 categories concerning theories and models that support psychomotor intervention were obtained. The conceptualizations proposed which were considered as the most relevant/priority were: DIR Floortime model, Applied Behaviour Analysis approach, Early Start Denver Model and TEACCH method. From the third meeting, 19 categories concerning the type of activities in psychomotor intervention sessions were considered as the most relevant/priority: free play, perceptive/sensory activities, and bodily-movement activities. From the fourth meeting, 26 categories were related to the session structural aspects, where the most relevant/priority were: materials and space organization, parents’ participation; stakeholders’ communication; session length and session moments. In the final meeting, 31 categories of strategies used in psychomotor intervention were: attention to the interests of the child, child–therapist relationship, complexity of activities proposed, and feedback and reinforcement.
After deductive thematic analysis of the NGT meetings (i.e., notes, categories of ideas rated, and audio-recordings transcriptions), 74 subthemes were obtained. These subthemes were classified under 19 themes (Table 2), in order to organize the statements by sections for phase II. Each statement intended to summarize the most repeated ideas in the coded transcriptions, which were then considered as the most relevant for each NGT meeting. These statements were the basis for writing the statements for the Delphi survey.
3.2. Phase II
Figure 2 presents the flow of experts and statements through the two rounds of the Delphi survey. 35 Portuguese experts (34 psychomotor therapists and one researcher) completed round 1, and 23 completed round 2 (65%). All experts had a minimum of 5 years’ experience in psychomotor intervention or research. Descriptive statistics of the 111 statements is presented by percentage of agreement obtained (percentage of experts’ rating between 7 to 9; see Supplementary Data, Table S1 round 1). The percentage of agreement ranged from 31.4% (statement 56) to 100% (statements 7, 17, 20 21, 26, 66, 84, 100, 107). For 26 statements, consensus was not reached. Regarding the sequencing of sessions and activities during the sessions, the statements showed that no consensus was reached, and thus these sections were excluded from round 2. Experts provided 79 free-text commentaries or suggestions regarding mainly the clarity and relevance of the statements. Based on a thematic analysis of this qualitative data, three new statements were generated, twelve were reformulated and five (the text of the statement was maintained) were moved to another section (see Supplementary Data, Table S1).
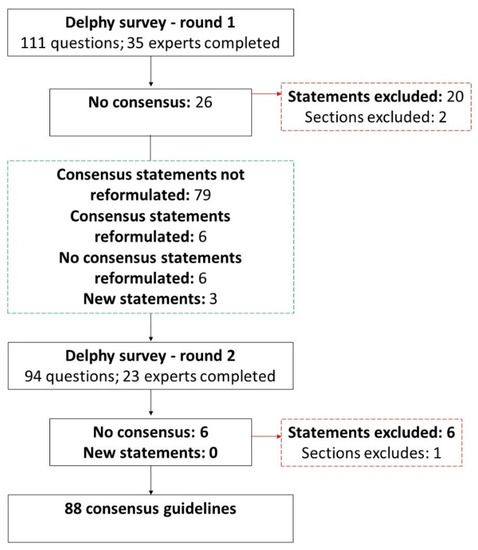
Figure 2.
Delphi survey process.
In round 2, the 94-item anonymized survey was completed by 23 experts. The percentage of agreement ranged from 65.2% (statement 10) to 100% (statements 4, 5, 11, 14, 15, 16, 18, 21, 50, 51, 52, 53, 66, 67, 86, 87). A tendency of increase in agreement across experts was observed. Six statements were excluded from section E, “Frequency of sessions”. Experts provided 53 commentaries related to the need to consider each child’s individuality. Thematic analysis generated no new items, and termination criteria for the Delphi survey were fulfilled. Experts reached consensus for the inclusion of 88 statements, grouped under 16 sections, reflecting guidelines for developing psychomotor intervention with preschool children with ASD.
Table 3 presents the 42 consensus guidelines that reached 95% or more of agreement among experts in the last round. The complete list of 88 guidelines is available as Supplementary Material (see Supplementary Data, Table S1). The sections with guidelines that met a stable consensus in both rounds with 95% or more of agreement were: intervention source, venue characteristics, change mechanisms, change techniques, strategies during the sessions, therapists delivering the sessions, and intended facilitation style (Table 3).
Table 3.
Key consensus recommendations for psychomotor intervention with preschool children with ASD.
4. Discussion
This study addressed the need of consensual guidelines within psychomotor intervention with preschool children with ASD. As such, this study used aa NGT and a Delphi survey to achieve expert consensus, aiming to better describe psychomotor intervention practices and generate more clear and effective interventions among psychomotor professionals in the future.
In phase I, 39 Portuguese experts, including psychomotor therapists working predominantly in clinical contexts of intervention (46% response rate) and researchers in psychomotor intervention (10% response rate), participated in a modified NGT process. In phase II, 23 of those experts completed two rounds of a Delphi survey (65% response rate), quantitively rating and qualitatively refining survey statements. No major changes were made between rounds, and consensus on the most important/highest priority items was reached.
With a border scope, the consensus guidelines obtained in this study are in line with the generic international guidelines for intervention with children with ASD [22,23], such as guideline 4. (individualized intervention), 26. (focus on individual strengths), 46. (objectives of intervention), 51. (supportive environment) 74. (stakeholders involvement). Most guidelines identified in this study are specific and detailed regarding the characteristics of psychomotor intervention, namely the guidelines describing change techniques and how they should be facilitated, and materials and intended facilitation, and therefore these are not mentioned in the international documents. Regarding the change techniques, the type of play used in psychomotor intervention is the major focus of movement play, structured opportunities, fine-manipulation play, expressive play, symbolic play, conventional games, constructive exploration, and sensory-exploration play. The 88 consensus guidelines were grouped under 16 sections. The most highly rated items in terms of relevance refer to the fact that psychomotor interventions can occur individually or in groups, should guarantee the child’s safety and autonomy, follow the child’s motivations, and create opportunities to develop competencies, so that sessions create a playful climate. Regarding psychomotor therapists’ competencies, several consensus statements focused on the quality of relationship as well routines and instructions during the sessions, under ongoing supervision and continuous training. This allowed us to consider that these are priorities for a clear definition of psychomotor intervention. All respondents agreed that these guidelines should have sufficient flexibility to be adapted according to the child and group characteristics. Furthermore, these guidelines seem to reinforce the multidimensional and interdisciplinary feature of psychomotor interventions, which should consider the components related to intervention design, intervention content (including theories that support intervention), participants, and facilitators, which interact with each other and impact final outcomes. As reflected in the consensus guidelines, psychomotor therapists use behavioral and educational approaches which are recommended for ASD [26]. This study adds to the scientific literature a tool to guide and support the psychomotor therapists’ practices, planning interventions according to the features recommended by adopting the methods, techniques, and strategies necessary to take into account in interventions with preschool children with ASD.
A comparison with other studies that used a similar methodology with the aim of developing intervention guidelines, shows that the combination of NGT and the Delphi technique are found in medical research [40,41,42]. Nevertheless, this combination was not found in therapeutic studies. Development of healthcare practice recommendations usually used methods based on systematic reviews and meta-analyses [43]. The specific research question and the methods are novel in psychomotor-intervention research. The combination of the two techniques was used to answer our research question, following a prescribed set of procedures [32,41]. A Delphi survey preceded by an NGT process made for a complex data analysis that was necessary to guarantee that guidelines were based on the heterogeneity of experts’ opinions. However, the use of the RAND/UCLA method (a hybrid of the Delphi and NGT) is suggested, to simplify the consensus process [41] in a future replication of this study.
Regarding the limitations of the study, the size and composition of the panel of experts may influence the quality of the data, and whether the judgments are accepted and considered feasible, especially if the number of experts is rather low [31]. Since this study included only experts from Portugal, it may be considered that the consensus guidelines identified will require further exploration, by consulting other internationally recognized experts in the psychomotor-intervention field [31,44]. The number and diversity of experts, mainly in the second phase, was lower than originally anticipated; however, the groups of experts were heterogeneous, with a wide range of years of experience and intervention contexts. The composition of the expert panel would benefit if the number of years of experience in psychomotor intervention and the number of ASD children accompanied in the last two years were higher. Thus, it is our opinion that a balanced number of therapists and researchers, between therapists working in therapeutic and educational contexts and the inclusion of experts from different countries, will improve the contextual and geographic representation in future studies. Nonetheless, the expert sample-size of this study may also be regarded as a strength, since more than double the proposed size limit of 12 was achieved.
Another limitation of this study was the fact that categories of ideas rated in the NGT process were generated at the end of each meeting while the participants were providing their suggestions. This process could be improved with a classification of categories created with more time, namely after the ideas gathered from experts allowing a deeper reflexion of the summarized and described ideas. Moreover, since the statements during the Delphi survey process were drawn from a content-analysis procedure, the subjectivity of the authors’ experience and knowledge (A.F., S.S. and P.L.) could have influenced the final consensus guidelines.
In phase I, group feedback was provided after each meeting. In phase II no feedback (individual or group) was provided to participants between rounds, contrary to what is considered to be a feature which is regarded as a strength of consensus methods [43]. In both phases, experts commented on key-terms definitions (e.g., non-directive vs. directive approach, structured vs. unstructured activities, play vs. game, guidelines…). A clear a priori statement of the definition of concepts ensured that assessment statements by experts started from a common understanding of key concepts and definitions, to avoid subjective perspectives and biases [44]. However, this is the first study, as far as we know, that attempted to systematically achieve consensus within the psychomotor-intervention field, where a transparency of processes was guaranteed, and all the study was done in accordance with internationally recognized guidelines (CONSORT-PSI 2018). These guidelines fill the gap in evidence based on a consensus of the experience of experts in this area, supporting the future development of psychomotor-intervention efficacy studies. It is recommended that a consensus-based approach drawn from systematic reviews on the topic under study, is conducted.
The authors understand first that further work will be required to test the usefulness and applicability of the proposed guidelines by psychomotor therapists currently undertaking intervention with children with ASD in Portugal and in other countries. Secondly, a replication of this study, including psychomotor-intervention experts working in educational contexts from different countries, a multidisciplinary clinician group, and service-user representatives, is recommended. Thirdly, further developments of this research may include the study of these guidelines for children with typical development, considering the role of peers that support inclusion within natural contexts. Finally, more research is recommended regarding the impact of psychomotor interventions for preschool children with ASD. Because scientific evidence regarding psychomotor intervention for children with ASD is scarce [7,10], this study will contribute to guiding the planning and reporting of psychomotor interventions that is necessary to guarantee the quality of intervention.
5. Conclusions
The current study engaged experts to develop and reach consensus guidelines addressing the transparency in psychomotor intervention and related research. This study is an important first step within the psychomotor-intervention field since the findings provide a summary of specific features of psychomotor interventions with preschool children with ASD. Results gave insights into how practices are, and should be, conducted by psychomotor therapists. The consensus-based approach resulted in 88 guidelines, where 42 reached more than 95% of agreement. The aim of these guidelines is to contribute to evidence studies by tailoring the coverage and challenges to define psychomotor intervention as a comprehensive intervention. We recommend the use of these guidelines (and their sections) to standardize the planning and reporting of psychomotor-intervention programs that can be more easily replicated, disseminated, and researched. Given the potential impact of psychomotor interventions in the development of preschool children with ASD, it is imperative to conduct high-quality research in the future. The issues identified in the present study can inform the research and practical agenda in the psychomotor therapy field. We suggest a broader representation of experts, to ensure these guidelines retain relevance to all stakeholders involved in the growing national and international field of psychomotor intervention. Furthermore, this study could serve as a model for generating consensual guidelines within psychomotor therapy in other target groups.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/children9111778/s1, Table S1: Statements rated in round 1 and 2.
Author Contributions
P.L., S.S. and A.F. were responsible for the conceptualization; A.F. made a substantial contribution to the conception and design, as well as to the writing (original draft preparation). P.L., S.S. and C.S. made substantial contributions to the design of the study and the revision of the manuscript for intellectual content, as the supervisors of the project. A.R. and T.B. assisted with the formal analysis. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Fundação para a Ciência e a para Tecnologia (FCT, Portugal), PhD grant number SFRH/BD/143886/2019.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Faculdade de Motricidade Humana (reference number 48/2021 from 29 November 2021).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank all researchers and psychomotor therapists including Mariana Moreira, Cristina Carvalho, Inês Neto, Nídia Amorim, Sofia Ferreira, Ana Fonseca Félix, Graça Faria, Evelina Brígido, Vera Pradiante, Barbara Santos, Ana Cristina Pereira, Ana Rita Pereira, Catarina Ferreira, Raquel Branco, Sara Teixeira, Joana Silva, Joana Veríssimo, Rita Mendes, Joana Carvalho, Joana Lopes, Claudia Machado Gil, and others who contributed to the development of these guidelines, by providing their valuable opinions.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Questions of NGT meetings.
Table A1.
Questions of NGT meetings.
| Questions Intended to Get Participants to Think about; One Initial Question per Topic | |
|---|---|
| Meeting 1 Trial question Topic: Question: | From your experience what are the primary needs of children with ASD (3–6 years old) that psychomotor intervention may improve? Objectives and primary results What are the aims of psychomotor intervention for children with ASD (3–6 years old)? |
| Meeting 2 Topic: Question: | Theories and models What theories or models support psychomotor intervention with children with ASD (3–6 years)? |
| Meeting 3 Topic: Question: | Methods What types of activities (individual and/or group) are carried out in psychomotor intervention with children with ASD (3–6 years)? (Experts are invited to give two examples of activities in the clarification stage) |
| Meeting 4 Topic: Question: | Environmental arrangements How are the sessions structured (individual and/or group)? Please select three of these aspects on which you would like to give your ideas:
|
| Meeting 5 Topic: Question: | Strategies What are the strategies you use most (in individual and/or group intervention)? Select three of these types of strategies about which you want to give your ideas:
|
References
- Probst, M.; Knapen, J.; Poot, G.; Vancampfort, D. Psychomotor Therapy and Psychiatry: What’s in a Name? Open Complement. Med. J. 2010, 2, 105–113. [Google Scholar] [CrossRef]
- European Forum of Psychomotricity. Statutes of the European Forum of Psychomotricity. 2015. Available online: https://psychomot.org/ (accessed on 20 September 2022).
- Ferré, G.; Dueñas, J.M.; Camps, C. Differences between the dynamic and normative psychomotricity in child development. Rev. Int. Med. Ciencias Act. Físi. Deporte 2021, 2, 47–62. [Google Scholar] [CrossRef]
- Moreira, M.S.; Almeida, G.N.; Marinho, S.M. Efectos de un programa de Psicomotricidad Educativa en niños en edad preescolar. Sportis 2016, 2, 326–342. [Google Scholar] [CrossRef]
- Vetter, M.; Sandmeier, A. Psychomotricity: Effects of psychomotor interventions from the perspective of teachers. Eur. Psychomot. J. 2020, 12, 30–42. [Google Scholar]
- Fotiadou, E.G.; Neofotistou, K.H.; Giagazoglou, P.F.; Tsimaras, V.K. The effect of a psychomotor education program on the static balance of children with intellectual disability. J. Strength Cond. Res. 2017, 31, 1702–1708. [Google Scholar] [CrossRef] [PubMed]
- Moschos, G.; Pollatou, E. The effect of a psychomotor intervention program in children 3–10 years of age: A systematic review. Body Mov. Danc. Psychother. 2022, 294–309. [Google Scholar] [CrossRef]
- Caliendo, M.; Di Sessa, A.; D’Alterio, E.; Frolli, A.; Verde, D.; Iacono, D.; Romano, P.; Vetri, L.; Carotenuto, M. Efficacy of Neuro-Psychomotor Approach in Children Affected by Autism Spectrum Disorders: A Multicenter Study in Italian Pediatric Population. Brain Sci. 2021, 11, 1210. [Google Scholar] [CrossRef] [PubMed]
- Emck, C. Double trouble? Movement behaviour and psychiatric conditions in children: An opportunity for treatment and development. Arts Psychother. 2014, 41, 214–222. [Google Scholar] [CrossRef]
- Frazão, A.; Santos, S.; Lebre, P. Psychomotor Intervention Practices for Children with Autism Spectrum Disorder: A Scoping Review. Rev. J. Autism Dev. Disord. 2021. [Google Scholar] [CrossRef]
- Bhat, A.N. Is Motor Impairment in Autism Spectrum Disorder Distinct from Developmental Coordination Disorder A Report from the SPARK Study. Phys. Ther. 2020, 100, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Paquet, A.; Olliac, B.; Golse, B.; Vaivre-Douret, L. Nature of motor impairments in autism spectrum disorder: A comparison with developmental coordination disorder. J. Clin. Exp. Neuropsychol. 2019, 41, 1–14. [Google Scholar] [CrossRef]
- Bhat, A.N. Motor Impairment Increases in Children with Autism Spectrum Disorder as a Function of Social Communication, Cognitive and Functional Impairment, Repetitive Behavior Severity, and Comorbid Diagnoses: A SPARK Study Report. Autism Res. 2021, 14, 202–219. [Google Scholar] [CrossRef]
- Leonard, H.C.; Hill, E.L. Review: The impact of motor development on typical and atypical social cognition and language: A systematic review. Child Adolesc. Ment. Health. 2014, 19, 163–170. [Google Scholar] [CrossRef]
- Hume, K.; Steinbrenner, J.R.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Szendrey, S.; McIntyre, N.S.; Yücesoy-Özkan, S.; Savage, M.N. Evidence-based practices for children, youth, and young adults with Autism: Third Generation Review. J. Autism Dev. Disord. 2021, 51, 4013–4032. [Google Scholar] [CrossRef] [PubMed]
- Steinbrenner, J.R.; Hume, K.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Szendrey, S.; McIntyre, N.S.; Yücesoy-Özkan, S.; Savage, M.N. Evidence-Based Practices for Children, Youth, and Young Adults with Autism Spectrum Disorder; The University of North Carolina at Chapel Hill: Chapel Hill, NC, USA; Frank Porter Graham Child Development Institute: Chapel Hill, NC, USA; National Clearinghouse on Autism Evidence and Practice Review Team: Chapel Hill, NC, USA, 2020. [Google Scholar]
- Zampella, C.J.; Wang, L.A.L.; Haley, M.; Hutchinson, A.G.; de Marchena, A. Motor Skill Differences in Autism Spectrum Disorder: A Clinically Focused Review. Curr. Psychiatry Rep. 2021, 23, 10. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, K.V.V.; Lima, S.A. Intervenção psicomotora no desenvolvimento infantil: Uma revisão integrativa. Rev. Bras. Promoção Saúde 2019, 32, 1–10. [Google Scholar] [CrossRef]
- Blease, C.R.; Lilienfeld, S.O.; Kelley, J.M. Evidence-Based Practice and Psychological Treatments: The Imperatives of Informed Consent. Front Psychol. 2016, 7, 1–5. [Google Scholar] [CrossRef]
- Cook, S.C.; Schwartz, A.C.; Kaslow, N.J. Evidence-Based Psychotherapy: Advantages and Challenges. Neurotherapeutics 2017, 14, 537–545. [Google Scholar] [CrossRef]
- Fuentes, J.; Hervás, A.; Howlin, P. ESCAP practice guidance for autism: A summary of evidence-based recommendations for diagnosis and treatment. Eur. Child Adolesc. Psychiatry 2021, 30, 6961–6984. [Google Scholar] [CrossRef]
- Weissman, L. Autism Spectrum Disorder in Children and Adolescents: Overview of Management. In UpToDate; Augustyn, M., Patterson, M., Eds.; UpToDate: Waltham, MA, USA, 2021. [Google Scholar]
- Weissman, L. Autism Spectrum Disorder in Children and Adolescents: Behavioral and Educational Interventions. In UpToDate; Augustyn, M., Patterson, M., Eds.; UpToDate: Waltham, MA, USA, 2021. [Google Scholar]
- National Institute for Health and Care Excellence. Autism Spectrum Disorder in under 19s: Support and Management. 2021. Available online: https://www.nice.org.uk/guidance/cg170 (accessed on 11 January 2022).
- Direção-Geral da Saúde. Norma no 002/2019-Abordagem Diagnóstica e Intervenção na Perturbação do Espetro do Autismo em Idade Pediátrica e no Adulto. 2019. Available online: https://normas.dgs.min-saude.pt/wp-content/uploads/2019/09/Abordagem-Diagnostica-e-Intervencao-na-Perturbacao-do-Espetro-do-Autismo-em-Idade-Pediatrica-e-no-Adulto_2019.pdf (accessed on 29 September 2022).
- Yiulin, W.; Fan, L.; Yuting, D.; Zhaoxiang, B.; Chi, Z.; Yaolong, C. CONSORT-SPI 2018 explanation and elaboration: Guidance for reporting social and psychological intervention trials. Chin. J. Evid. Based Med. 2020, 20, 1458–1470. [Google Scholar] [CrossRef]
- Manera, K.; Hanson, C.S.; Gutman, T.; Tong, A. Consensus Methods: Nominal Group Technique. In Handbook of Research Methods in Health Social Sciences; Liamputtong, P., Ed.; Springer: Singapore, 2019; pp. 737–750. [Google Scholar]
- World Health Organization. WHO Handbook for Guideline Development, 2nd. ed.; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Van de, A.H.; Delbecq, A.L. The Effectiveness of Nominal, Delphi, and Interacting Group Decision Making Processes. Acad. Manag. J. 1974, 17, 605–621. [Google Scholar] [CrossRef]
- Niederberger, M.; Spranger, J. Delphi Technique in Health Sciences: A Map. Front. Public Health 2020, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Skela-Savič, B.; MacRae, R.; Lillo-Crespo, M.; Rooney, K.D. The Development of a Consensus Definition for Healthcare Improvement Science (HIS) in Seven European Countries: A consensus methods approach. Zdr. Varst. 2017, 56, 82–90. [Google Scholar] [CrossRef]
- McMillan, S.S.; Kelly, F.; Sav, A.L.; Kendall, E.; King, M.A.; Whitty, J.A.; Wheeler, A.J. Using the Nominal Group Technique: How to analyse across multiple groups. Health Serv. Outcomes Res. Methodol. 2014, 14, 92–108. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Developing NICE Guidelines: The Manual. NICE. 2014. Available online: http://www.nice.org.uk/article/pmg20 (accessed on 12 February 2022).
- Borek, A.J.; Abraham, C.; Smith, J.R.; Greaves, C.J.; Tarrant, M. A checklist to improve reporting of group-based behaviour-change interventions. BMC Public Health 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the Delphi method for selecting healthcare quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Loebach, J.; Cox, A. Tool for observing play outdoors (Topo): A new typology for capturing children’s play behaviors in outdoor environments. Int. J. Environ. Res. Public Health 2020, 17, 5611. [Google Scholar] [CrossRef]
- Foth, T.; Efstathiou, N.; Vanderspank-Wright, B.; Ufholz, L.A.; Dütthorn, N.; Zimansky, M.; Humphrey-Murto, S. The use of Delphi and Nominal Group Technique in nursing education: A review. Int. J. Nurs. Stud. 2016, 60, 112–120. [Google Scholar] [CrossRef]
- Humphrey-murto, S.; Varpio, L.; Gonsalves, C.; Wood, T.J. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med. Teacher 2016, 39, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Verwoerd, M.; Wittink, H.; Maissan, F.; Smeets, R. Consensus of potential modifiable prognostic factors for persistent pain after a first episode of nonspecific idiopathic, non-traumatic neck pain: Results of nominal group and Delphi technique approach. BMC Musculoskelet. Disord. 2020, 21, 656. [Google Scholar] [CrossRef] [PubMed]
- Platz, T. Methods for the Development of Healthcare Practice Recommendations Using Systematic Reviews and Meta-Analyses. Front. Neurol. 2021, 12, 699968. [Google Scholar] [CrossRef]
- Nasa, P.; Jain, R.; Juneja, D. Delphi methodology in healthcare research: How to decide its appropriateness. World J. Methodol. 2021, 11, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Beiderbeck, D.; Frevel, N.; Von Der Gracht, H.A.; Schmidt, S.L.; Schweitzer, V.M. Preparing, conducting, and analyzing Delphi surveys: Cross-disciplinary practices, new directions, and advancements. MethodsX 2021, 8, 01401. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).