
Association of F. alocis and D. pneumosintes with Periodontitis Disease Severity and Red Complex Bacteria
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
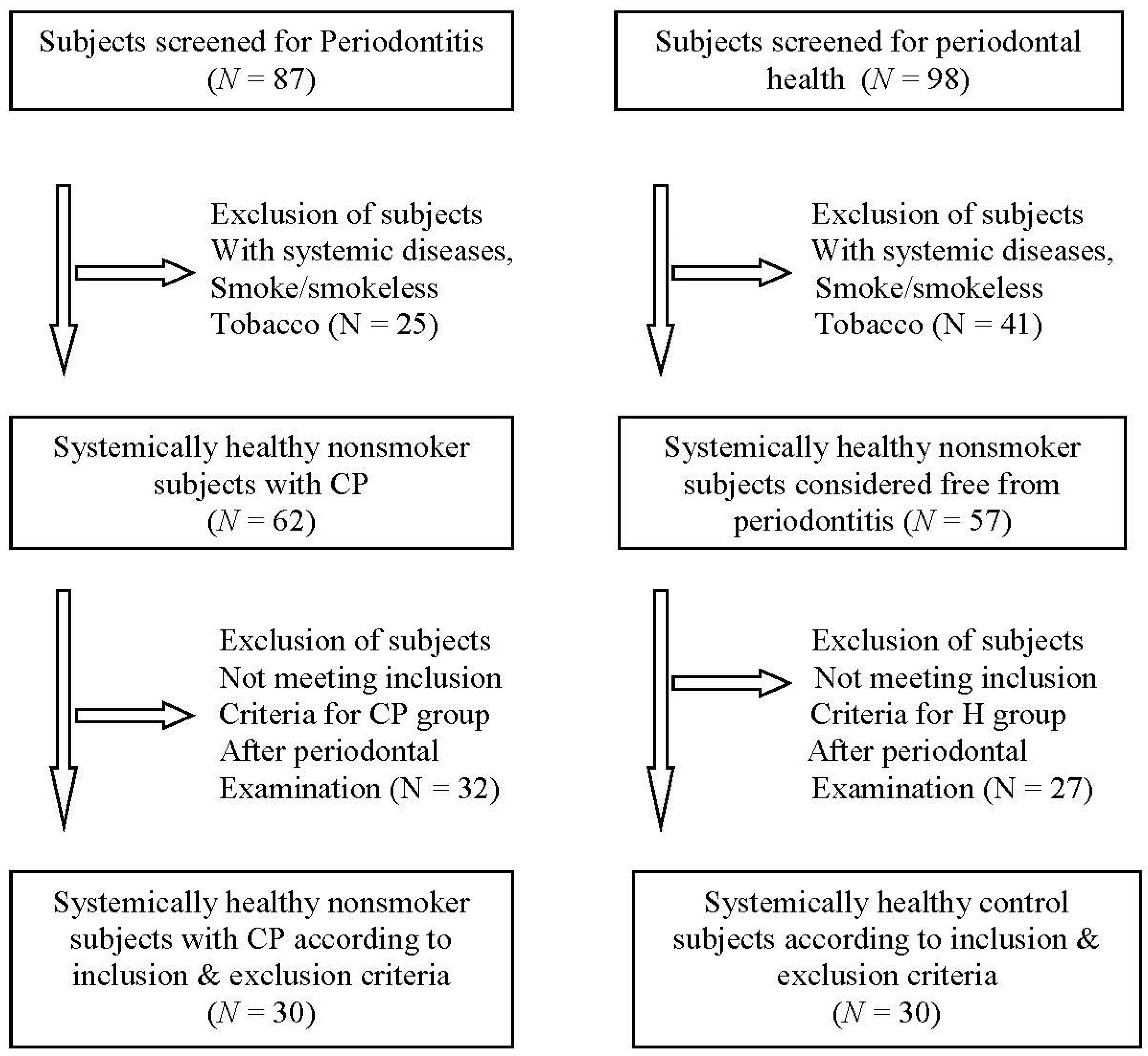
2.1. Clinical Examination and Subgingival Plaque Sample Collection
2.2. DNA Extraction and Polymerase Chain Reaction
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DNA | Deoxyribonucleic acid |
| H group | Healthy group |
| P group | Periodontitis group |
| CAL | Clinical attachment loss |
| PD | Probing depth |
| BOP | Bleeding on probing |
| PI | Plaque index |
| GI | Gingival index |
| BI | Bleeding index |
| PCR | Polymerase chain reaction |
| TE | Tris-EDTA buffer |
| 16SrRNA | 16S ribosomal ribonucleic acid |
| IL-1β | Interleukin-1β |
| IL-6 | Interleukin-6 |
| TNF-α | Tumour necrosis factor alpha |
References
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S162–S170. [Google Scholar] [CrossRef] [PubMed]
- Abusleme, L.; Hoare, A.; Hong, B.-Y.; Diaz, P.I. Microbial Signatures of Health, Gingivitis, and Periodontitis. Periodontol. 2000 2021, 86, 57–78. [Google Scholar] [CrossRef]
- Naginyte, M.; Do, T.; Meade, J.; Devine, D.A.; Marsh, P.D. Enrichment of Periodontal Pathogens from the Biofilms of Healthy Adults. Sci. Rep. 2019, 9, 5491. [Google Scholar] [CrossRef]
- Bašić, K.; Peroš, K.; Bošnjak, Z.; Šutej, I. Subgingival Microbiota Profile in Association with Cigarette Smoking in Young Adults: A Cross-Sectional Study. Dent. J. 2021, 9, 150. [Google Scholar] [CrossRef]
- Bernardi, S.; Qorri, E.; Botticelli, G.; Scarano, A.; Marzo, G.; Gatto, R.; Greco Lucchina, A.; Mortellaro, C.; Lupi, E.; Rastelli, C.; et al. Use of Electrical Field for Biofilm Implant Removal. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 114–121. [Google Scholar] [CrossRef]
- Franco, R.; Rosa, A.; Lupi, E.; Capogreco, M. The Influence of Dental Implant Roughness on Biofilm Formation: A Comprehensive Strategy. Dent. Hypotheses 2023, 14, 90. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L. Microbial Complexes in Subgingival Plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Antezack, A.; Etchecopar-Etchart, D.; La Scola, B.; Monnet-Corti, V. New Putative Periodontopathogens and Periodontal Health-Associated Species: A Systematic Review and Meta-Analysis. J. Periodontal Res. 2023, 58, 893–906. [Google Scholar] [CrossRef]
- Veras, E.L.; Castro Dos Santos, N.; Souza, J.G.S.; Figueiredo, L.C.; Retamal-Valdes, B.; Barão, V.A.R.; Shibli, J.; Bertolini, M.; Faveri, M.; Teles, F.; et al. Newly Identified Pathogens in Periodontitis: Evidence from an Association and an Elimination Study. J. Oral Microbiol. 2023, 15, 2213111. [Google Scholar] [CrossRef] [PubMed]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the Normal Bacterial Flora of the Oral Cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef]
- Pérez-Chaparro, P.J.; Gonçalves, C.; Figueiredo, L.C.; Faveri, M.; Lobão, E.; Tamashiro, N.; Duarte, P.; Feres, M. Newly Identified Pathogens Associated with Periodontitis: A Systematic Review. J. Dent. Res. 2014, 93, 846–858. [Google Scholar] [CrossRef]
- Hiranmayi, K.V.; Sirisha, K.; Ramoji Rao, M.V.; Sudhakar, P. Novel Pathogens in Periodontal Microbiology. J. Pharm. Bioallied Sci. 2017, 9, 155–163. [Google Scholar] [CrossRef]
- Kim, H.Y.; Song, M.-K.; Gho, Y.S.; Kim, H.-H.; Choi, B.-K. Extracellular Vesicles Derived from the Periodontal Pathogen Filifactor Alocis Induce Systemic Bone Loss through Toll-like Receptor 2. J. Extracell. Vesicles 2021, 10, e12157. [Google Scholar] [CrossRef]
- Yoo, H.-J.; Lee, S.-H. Virulence of Filifactor Alocis Lipoteichoic Acid on Human Gingival Fibroblast. Arch. Oral Biol. 2022, 135, 105370. [Google Scholar] [CrossRef]
- Aruni, A.W.; Zhang, K.; Dou, Y.; Fletcher, H. Proteome Analysis of Coinfection of Epithelial Cells with Filifactor Alocis and Porphyromonas Gingivalis Shows Modulation of Pathogen and Host Regulatory Pathways. Infect. Immun. 2014, 82, 3261–3274. [Google Scholar] [CrossRef]
- Aruni, A.W.; Roy, F.; Fletcher, H.M. Filifactor Alocis Has Virulence Attributes That Can Enhance Its Persistence under Oxidative Stress Conditions and Mediate Invasion of Epithelial Cells by Porphyromonas Gingivalis. Infect. Immun. 2011, 79, 3872–3886. [Google Scholar] [CrossRef]
- Moffatt, C.E.; Whitmore, S.E.; Griffen, A.L.; Leys, E.J.; Lamont, R.J. Filifactor Alocis Interactions with Gingival Epithelial Cells. Mol. Oral Microbiol. 2011, 26, 365–373. [Google Scholar] [CrossRef]
- Dahlén, G.; Claesson, R.; Aberg, C.H.; Haubek, D.; Johansson, A.; Kwamin, F. Subgingival Bacteria in Ghanaian Adolescents with or without Progression of Attachment Loss. J. Oral Microbiol. 2014, 6, 23977. [Google Scholar] [CrossRef]
- Schlafer, S.; Riep, B.; Griffen, A.L.; Petrich, A.; Hübner, J.; Berning, M.; Friedmann, A.; Göbel, U.B.; Moter, A. Filifactor Alocis--Involvement in Periodontal Biofilms. BMC Microbiol. 2010, 10, 66. [Google Scholar] [CrossRef]
- Ozuna, H.; Snider, I.; Belibasakis, G.N.; Oscarsson, J.; Johansson, A.; Uriarte, S.M. Aggregatibacter Actinomycetemcomitans and Filifactor Alocis: Two Exotoxin-Producing Oral Pathogens. Front. Oral Health 2022, 3, 981343. [Google Scholar] [CrossRef]
- Olitsky, P.K.; Gates, F.L. Experimental Studies of the Nasopharyngeal Secretions From Influenza Patients: I. Transmission Experiments With Nasopharyngeal Washings. J. Exp. Med. 1921, 33, 125–145. [Google Scholar] [CrossRef]
- Ferraro, C.T.L.; Gornic, C.; Barbosa, A.S.; Peixoto, R.J.M.; Colombo, A.P.V. Detection of Dialister Pneumosintes in the Subgingival Biofilm of Subjects with Periodontal Disease. Anaerobe 2007, 13, 244–248. [Google Scholar] [CrossRef]
- Doan, N.; Contreras, A.; Flynn, J.; Slots, J.; Chen, C. Molecular Identification of Dialister Pneumosintes in Subgingival Plaque of Humans. J. Clin. Microbiol. 2000, 38, 3043–3047. [Google Scholar] [CrossRef]
- Contreras, A.; Doan, N.; Chen, C.; Rusitanonta, T.; Flynn, M.J.; Slots, J. Importance of Dialister Pneumosintes in Human Periodontitis. Oral Microbiol. Immunol. 2000, 15, 269–272. [Google Scholar] [CrossRef]
- Zhao, Y.; Ye, Q.; Feng, Y.; Chen, Y.; Tan, L.; Ouyang, Z.; Zhao, J.; Hu, J.; Chen, N.; Su, X.; et al. Prevotella Genus and Its Related NOD-like Receptor Signaling Pathway in Young Males with Stage III Periodontitis. Front. Microbiol. 2022, 13, 1049525. [Google Scholar] [CrossRef]
- Drago, L.; Vassena, C.; Saibene, A.M.; Del Fabbro, M.; Felisati, G. A Case of Coinfection in a Chronic Maxillary Sinusitis of Odontogenic Origin: Identification of Dialister Pneumosintes. J. Endod. 2013, 39, 1084–1087. [Google Scholar] [CrossRef]
- Jumas-Bilak, E.; Jean-Pierre, H.; Carlier, J.-P.; Teyssier, C.; Bernard, K.; Gay, B.; Campos, J.; Morio, F.; Marchandin, H. Dialister micraerophilus sp. nov. and Dialister propionicifaciens sp. nov., Isolated from Human Clinical Samples. Int. J. Syst. Evol. Microbiol. 2005, 55, 2471–2478. [Google Scholar] [CrossRef]
- Slots, J.; Sugar, C.; Kamma, J.J. Cytomegalovirus Periodontal Presence Is Associated with Subgingival Dialister Pneumosintes and Alveolar Bone Loss. Oral Microbiol. Immunol. 2002, 17, 369–374. [Google Scholar] [CrossRef]
- Araújo, L.L.; Lourenço, T.G.B.; Colombo, A.P.V. Periodontal Disease Severity Is Associated to Pathogenic Consortia Comprising Putative and Candidate Periodontal Pathogens. J. Appl. Oral Sci. 2023, 31, e20220359. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef]
- Silness, J.; Loe, H. Periodontal Disease In Pregnancy. Ii. Correlation Between Oral Hygiene and Periodontal Condtion. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Loe, H.; Silness, J. Periodontal Disease In Pregnancy. I. Prevalence and Severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Carter, H.G.; Barnes, G.P. The Gingival Bleeding Index. J. Periodontol. 1974, 45, 801–805. [Google Scholar] [CrossRef]
- Kugaji, M.S.; Bhat, K.G.; Joshi, V.M.; Pujar, M.; Mavani, P.T. Simplified Method of Detection of Dialister Invisus and Olsenella Uli in Oral Cavity Samples by Polymerase Chain Reaction. J. Adv. Oral Res. 2017, 8, 47–52. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N. Simultaneous Detection of Dialister Pneumosintes and Filifactor Alocis in Endodontic Infections by 16S RDNA-Directed Multiplex PCR. J. Endod. 2004, 30, 851–854. [Google Scholar] [CrossRef] [PubMed]
- Ashimoto, A.; Chen, C.; Bakker, I.; Slots, J. Polymerase Chain Reaction Detection of 8 Putative Periodontal Pathogens in Subgingival Plaque of Gingivitis and Advanced Periodontitis Lesions. Oral Microbiol. Immunol. 1996, 11, 266–273. [Google Scholar] [CrossRef]
- Kumar, P.S.; Griffen, A.L.; Moeschberger, M.L.; Leys, E.J. Identification of Candidate Periodontal Pathogens and Beneficial Species by Quantitative 16S Clonal Analysis. J. Clin. Microbiol. 2005, 43, 3944–3955. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S.; Leys, E.J.; Bryk, J.M.; Martinez, F.J.; Moeschberger, M.L.; Griffen, A.L. Changes in Periodontal Health Status Are Associated with Bacterial Community Shifts as Assessed by Quantitative 16S Cloning and Sequencing. J. Clin. Microbiol. 2006, 44, 3665–3673. [Google Scholar] [CrossRef]
- Dahlén, G.; Leonhardt, A. A New Checkerboard Panel for Testing Bacterial Markers in Periodontal Disease. Oral Microbiol. Immunol. 2006, 21, 6–11. [Google Scholar] [CrossRef]
- Colombo, A.P.V.; Boches, S.K.; Cotton, S.L.; Goodson, J.M.; Kent, R.; Haffajee, A.D.; Socransky, S.S.; Hasturk, H.; Van Dyke, T.E.; Dewhirst, F.; et al. Comparisons of Subgingival Microbial Profiles of Refractory Periodontitis, Severe Periodontitis, and Periodontal Health Using the Human Oral Microbe Identification Microarray. J. Periodontol. 2009, 80, 1421–1432. [Google Scholar] [CrossRef]
- Lindholm, M.; Claesson, R.; Löf, H.; Chiang, H.-M.; Oscarsson, J.; Johansson, A.; Åberg, C.H. Radiographic and Clinical Signs of Periodontitis and Associated Bacterial Species in a Swedish Adolescent Population. J. Periodontol. 2023, 94, 630–640. [Google Scholar] [CrossRef]
- Ikeda, E.; Shiba, T.; Ikeda, Y.; Suda, W.; Nakasato, A.; Takeuchi, Y.; Azuma, M.; Hattori, M.; Izumi, Y. Japanese Subgingival Microbiota in Health vs. Disease and Their Roles in Predicted Functions Associated with Periodontitis. Odontology 2020, 108, 280–291. [Google Scholar] [CrossRef]
- Ko, Y.; Lee, E.-M.; Park, J.C.; Gu, M.B.; Bak, S.; Ji, S. Salivary Microbiota in Periodontal Health and Disease and Their Changes Following Nonsurgical Periodontal Treatment. J. Periodontal Implant Sci. 2020, 50, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Kook, J.-K.; Park, S.-N.; Lim, Y.K.; Choi, G.H.; Jung, J.-S. Characteristics of the Salivary Microbiota in Periodontal Diseases and Potential Roles of Individual Bacterial Species to Predict the Severity of Periodontal Disease. Microbiol. Spectr. 2023, 11, e0432722. [Google Scholar] [CrossRef]
- Neelakandan, A.; Potluri, R.; Yadalam, P.K.; Chakraborty, P.; Saravanan, A.V.; Arunraj, R. The Varied Proportion of Filifactor Alocis in Periodontal Health and Disease in the South Indian Subpopulation. Contemp. Clin. Dent. 2021, 12, 433–438. [Google Scholar] [CrossRef]
- Ayala Herrera, J.L.; Apreza Patrón, L.; Martínez Martínez, R.E.; Domínguez Pérez, R.A.; Abud Mendoza, C.; Hernández Castro, B. Filifactor Alocis and Dialister Pneumosintes in a Mexican Population Affected by Periodontitis and Rheumatoid Arthritis: An Exploratory Study. Microbiol. Immunol. 2019, 63, 392–395. [Google Scholar] [CrossRef]
- Nishiyama, S.A.B.; Nakano, V.; Velásquez-Melendez, G.; Avila-Campos, M.J. Occurrence of Herpes Simplex Virus 1 and Three Periodontal Bacteria in Patients with Chronic Periodontitis and Necrotic Pulp. Can. J. Microbiol. 2008, 54, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Aruni, A.W.; Mishra, A.; Dou, Y.; Chioma, O.; Hamilton, B.N.; Fletcher, H.M. Filifactor Alocis—A New Emerging Periodontal Pathogen. Microbes Infect. 2015, 17, 517–530. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, H.F.M.; Oswal, P.U.; Kugaji, M.S.; Katti, S.S.; Bhat, K.G.; Joshi, V.M. Co-Occurrence of Filifactor Alocis with Red Complex Bacteria in Type 2 Diabetes Mellitus Subjects with and without Chronic Periodontitis: A Pilot Study. Int. J. Transl. Med. 2023, 3, 97–107. [Google Scholar] [CrossRef]
- Chen, H.; Liu, Y.; Zhang, M.; Wang, G.; Qi, Z.; Bridgewater, L.; Zhao, L.; Tang, Z.; Pang, X. A Filifactor Alocis-Centered Co-Occurrence Group Associates with Periodontitis across Different Oral Habitats. Sci. Rep. 2015, 5, 9053. [Google Scholar] [CrossRef]
- Wyss, C. Dependence of Proliferation of Bacteroides Forsythus on Exogenous N-Acetylmuramic Acid. Infect. Immun. 1989, 57, 1757. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Socransky, S.S. Microbial Etiological Agents of Destructive Periodontal Diseases. Periodontol. 2000 1994, 5, 78–111. [Google Scholar] [CrossRef]
- Ghayoumi, N.; Chen, C.; Slots, J. Dialister Pneumosintes, a New Putative Periodontal Pathogen. J. Periodontal Res. 2002, 37, 75–78. [Google Scholar] [CrossRef]
- Oliveira, R.R.D.S.; Fermiano, D.; Feres, M.; Figueiredo, L.C.; Teles, F.R.F.; Soares, G.M.S.; Faveri, M. Levels of Candidate Periodontal Pathogens in Subgingival Biofilm. J. Dent. Res. 2016, 95, 711–718. [Google Scholar] [CrossRef]
- Razooqi, Z.; Höglund Åberg, C.; Kwamin, F.; Claesson, R.; Haubek, D.; Oscarsson, J.; Johansson, A. Aggregatibacter Actinomycetemcomitans and Filifactor Alocis as Associated with Periodontal Attachment Loss in a Cohort of Ghanaian Adolescents. Microorganisms 2022, 10, 2511. [Google Scholar] [CrossRef]
- Gonçalves, C.; Soares, G.M.S.; Faveri, M.; Pérez-Chaparro, P.J.; Lobão, E.; Figueiredo, L.C.; Baccelli, G.T.; Feres, M. Association of Three Putative Periodontal Pathogens with Chronic Periodontitis in Brazilian Subjects. J. Appl. Oral Sci. 2016, 24, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Feres, M.; Retamal-Valdes, B.; Gonçalves, C.; Cristina Figueiredo, L.; Teles, F. Did Omics Change Periodontal Therapy? Periodontol. 2000 2021, 85, 182–209. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Target | Primer Sequence (5′-3′) a | Amplification Length (bp) |
|---|---|---|
| Filifactor alocis | CAGGTGGTTTAACAAGTTAGTGG CTAAGTTGTCCTTAGCTGTCTCG | 594 [36] |
| Dialister pneumosintes | TTCTAAGCATCGCATGGTGC GATTTCGCTTCTCTTTGTTG | 1105 [36] |
| Porphyromonas gingivalis | AGGCAGCTTGCCATACTGCG ACTGTTAGCAACTACCGATGT | 404 [37] |
| Treponema denticola | TAATACCGAATGTGCTCATTTACAT TCAAAGAAGCATTCCCTCTTCTTCTTA | 316 [37] |
| Tannerella forsythia | GCGTATGTAACCTGCCCGCA TGCTTCAGTGTCAGTTATACCT | 641 [37] |
| Parameter | H Group | P Group | p-Value |
|---|---|---|---|
| Gender (Male/Female) | 12/18 | 13/17 | 0.7934 * |
| Age (years) | 44.03 ± 10.11 | 42.07 ± 10.60 | 0.465 # |
| GI | 0.100 ± 0.043 | 2.09 ± 0.188 | <0.0001 γ |
| PI | 0.094 ± 0.040 | 2.23 ± 0.193 | <0.0001 γ |
| BI | 3.098 ± 2.191 | 93.30 ± 6.517 | <0.0001 γ |
| PD | 1.465 ± 0.333 | 5.361 ± 0.252 | <0.0001 γ |
| CAL | 0.000 ± 0.000 | 5.014 ± 0.566 | <0.0001 γ |
| Organisms | Negative/ Positive | H Group | P Group | Total | Fisher’s Exact Test p-Value |
|---|---|---|---|---|---|
| F. alocis | Negative | 24 (80%) | 14 (46.7) | 38 (63.3%) | 0.015 * |
| Positive | 6 (20%) | 16 (53.3%) | 22 (36.7%) | ||
| D. pneumosintes | Negative | 24 (80%) | 10 (33.33%) | 34 (56.67) | 0.0006 * |
| Positive | 6 (20%) | 20 (66.67%) | 26 (43.33) | ||
| P. gingivalis | Negative | 24 (80%) | 17 (56.67) | 41 (68.33) | 0.09 |
| Positive | 6 (20%) | 13 (43.33) | 19 (31.67) | ||
| T. denticola | Negative | 24 (80%) | 14 (46.7) | 38 (63.3%) | 0.015 * |
| Positive | 6 (20%) | 16 (53.3%) | 22 (36.7%) | ||
| T. forsythia | Negative | 22 (73.33) | 21 (70.00) | 43 (71.67) | 1.0 |
| Positive | 8 (26.67) | 9 (30.00) | 17 (28.33) |
| Group | Red Complex Bacteria | F. alocis | Total | Fisher’s Exact Test p-Value | ||
|---|---|---|---|---|---|---|
| Negative | Positive | |||||
| H group (N = 30) | P. gingivalis | Negative | 19 (79.2%) | 5 (20.8%) | 24 (100.0%) | 1.0 |
| Positive | 5 (83.3%) | 1 (16.7%) | 6 (100.0%) | |||
| T. denticola | Negative | 20 (83.3%) | 4 (16.7%) | 24 (100.0% | 0.5705 | |
| Positive | 4 (66.7%) | 2 (33.3%) | 6 (100.0%) | |||
| T. forsythia | Negative | 16 (72.7%) | 6 (27.3%) | 22 (100.0%) | 0.1550 | |
| Positive | 8 (100.0%) | 0 (0%) | 8 (100.0%) | |||
| P group (N = 30) | P. gingivalis | Negative | 6 (35.3%) | 11 (64.7%) | 17 (100.0%) | 0.2685 |
| Positive | 8 (61.5%) | 5 (38.5%) | 13 (100.0%) | |||
| T. denticola | Negative | 9 (64.3%) | 5 (35.7%) | 14 (100.0%) | 0.1414 | |
| Positive | 5(31.3%) | 11 (68.8%) | 16 (100.0%) | |||
| T. forsythia | Negative | 12 (57.1%) | 9 (42.9%) | 21(100.0%) | 0.1184 | |
| Positive | 2 (22.2%) | 7 (77.8%) | 9 (100.0%) | |||
| Group | Red Complex Bacteria | D. pneumosintes | Total | Fisher’s Exact Test p-Value | ||
|---|---|---|---|---|---|---|
| Negative | Positive | |||||
| H group (N = 30) | P. gingivalis | Negative | 20 (83.33%) | 4 (16.67%) | 24 (100.0%) | 0.5705 |
| Positive | 4 (66.67%) | 2 (33.33%) | 6 (100.0%) | |||
| T. denticola | Negative | 19 (79.17%) | 5 (20.83%) | 24 (100.0% | 1.0000 | |
| Positive | 5 (83.33%) | 1 (16.67%) | 6 (100.0%) | |||
| T. forsythia | Negative | 17 (77.27%) | 5 (22.73%) | 22 (100.0%) | 1.0000 | |
| Positive | 7 (87.50%) | 1 (12.50%) | 8 (100.0%) | |||
| P group (N = 30) | P. gingivalis | Negative | 4 (23.53%) | 13 (76.47%) | 17 (100.0%) | 0.2553 |
| Positive | 6 (46.15%) | 7 (53.85%) | 13 (100.0%) | |||
| T. denticola | Negative | 6 (42.86%) | 8 (57.14%) | 14 (100.0%) | 0.4421 | |
| Positive | 4 (25.00%) | 12 (75.00%) | 16 (100.0%) | |||
| T. forsythia | Negative | 10 (47.62%) | 11 (52.38%) | 21(100.0%) | 0.0134 * | |
| Positive | 0 (0.00%) | 9 (100%) | 9 (100.0%) | |||
| Clinical Attachment Loss | F. alocis | Fisher’s Exact Test p-Value | D. pneumosintes | Fisher’s Exact Test p-Value | ||
|---|---|---|---|---|---|---|
| Negative | Positive | Negative | Positive | |||
| <3 mm | 24 (80.0%) | 6 (20.0%) | 0.024 * | 24 (80%) | 6 (20%) | 0.0007 * |
| 3–5 mm | 8 (44.4%) | 10 (55.6%) | 5 (27.77%) | 13 (72.23%) | ||
| >5 mm | 6 (50.0%) | 6 (50.0%) | 5 (41.66%) | 7 (58.34%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaikh, H.F.M.; Oswal, P.U.; Kugaji, M.S.; Katti, S.S.; Bhat, K.G.; Kandaswamy, E.; Joshi, V.M. Association of F. alocis and D. pneumosintes with Periodontitis Disease Severity and Red Complex Bacteria. Dent. J. 2024, 12, 105. https://doi.org/10.3390/dj12040105
Shaikh HFM, Oswal PU, Kugaji MS, Katti SS, Bhat KG, Kandaswamy E, Joshi VM. Association of F. alocis and D. pneumosintes with Periodontitis Disease Severity and Red Complex Bacteria. Dentistry Journal. 2024; 12(4):105. https://doi.org/10.3390/dj12040105
Chicago/Turabian StyleShaikh, Hawaabi F. M., Pratima U. Oswal, Manohar Suresh Kugaji, Sandeep S. Katti, Kishore Gajanan Bhat, Eswar Kandaswamy, and Vinayak M. Joshi. 2024. "Association of F. alocis and D. pneumosintes with Periodontitis Disease Severity and Red Complex Bacteria" Dentistry Journal 12, no. 4: 105. https://doi.org/10.3390/dj12040105