
A Systematic Review and Meta-Analysis Comparing Surgical and Nonsurgical Treatments for Excessive Gingival Display


Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Information Sources
2.3. Eligibility Criteria (Table S2)
- Participants: adult patients 18 years of age or older with a chief complaint of EGD on smiling, with periodontal and systemic health.
- Intervention: surgical and nonsurgical treatments for EGD.
- Comparison: pre-treatment condition.
- Outcome measures: gingival display at maximum smile pre-treatment and at follow-up visits for a minimum of 6 months.
- Study design: randomized controlled trials, non-randomized studies without a control group, prospective, retrospective, comparative cohort, and case–control studies.
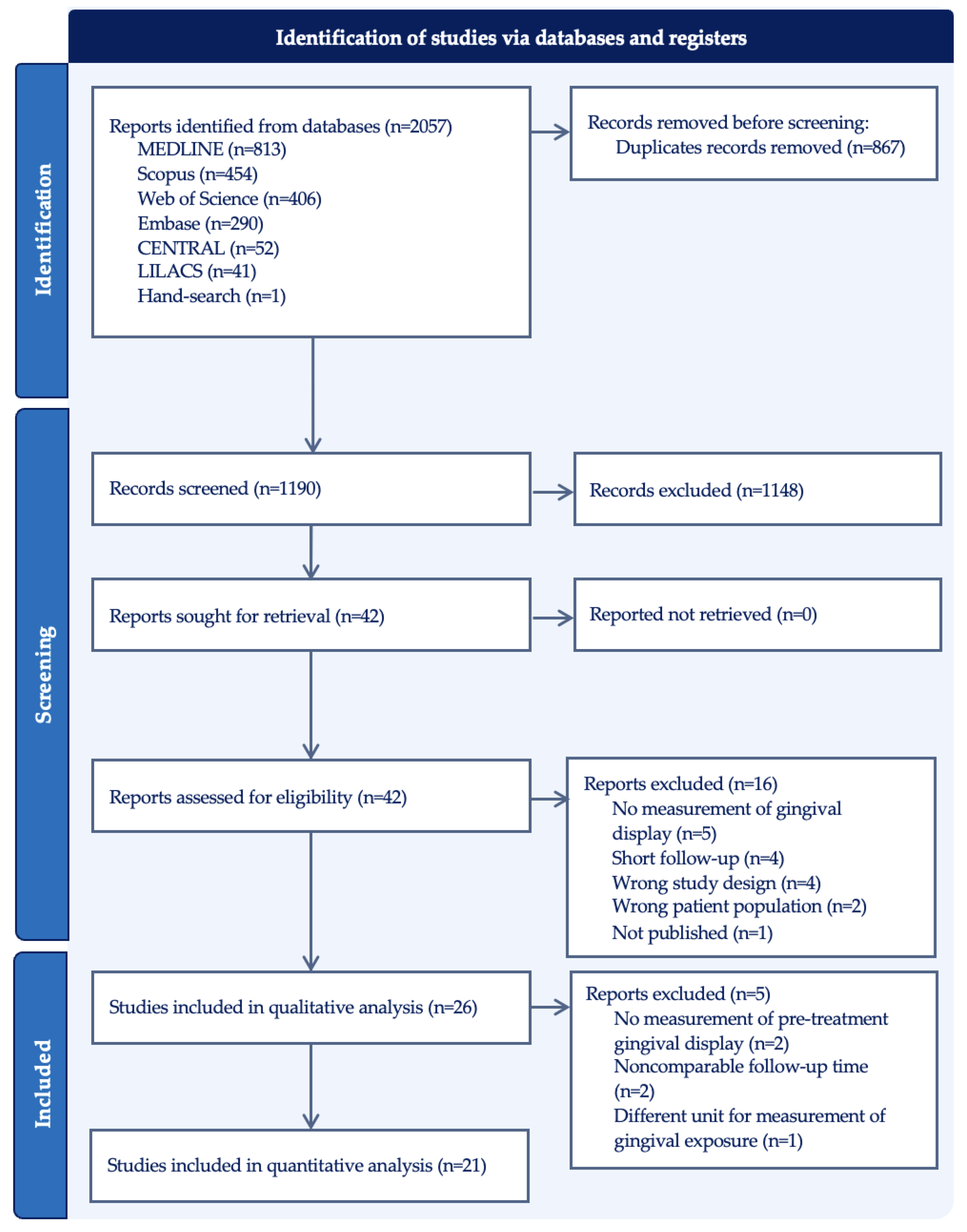
2.4. Study Selection
2.5. Data Extraction
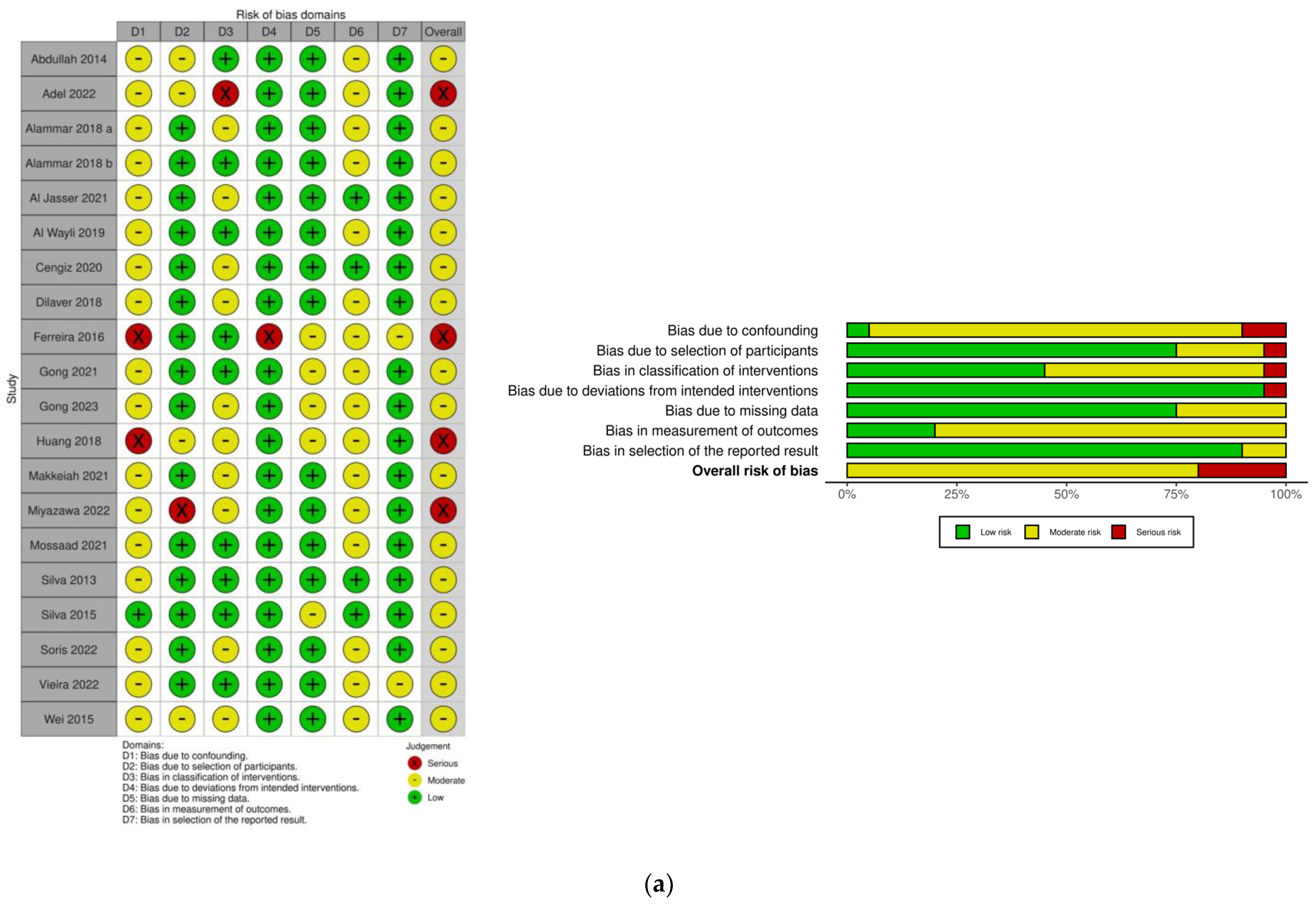
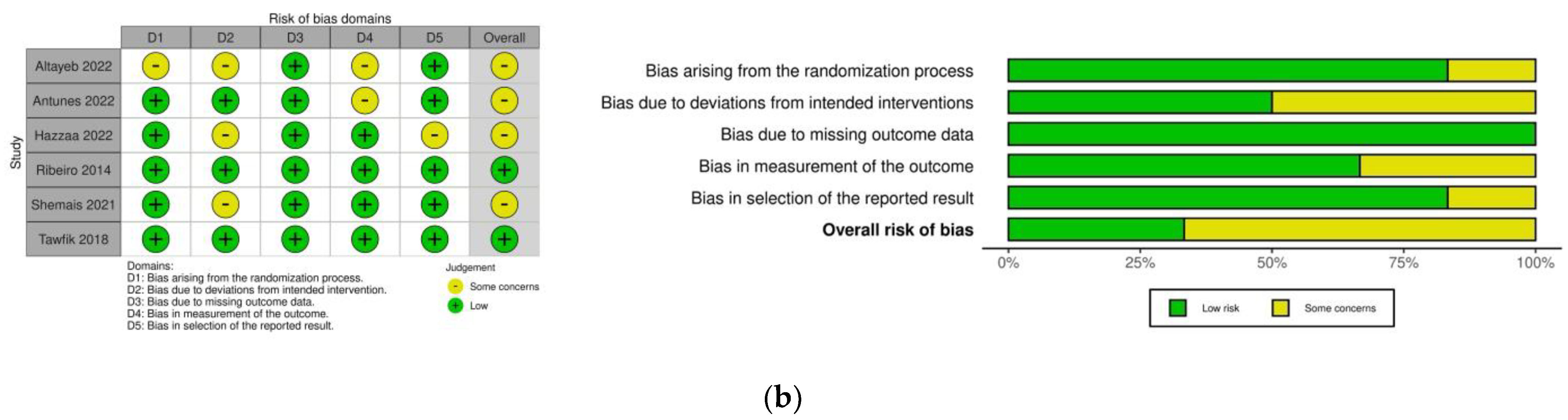
2.6. Risk of Bias Assessment
2.7. Data Analysis
3. Results
3.1. Study Characteristics
3.2. Risk of Bias
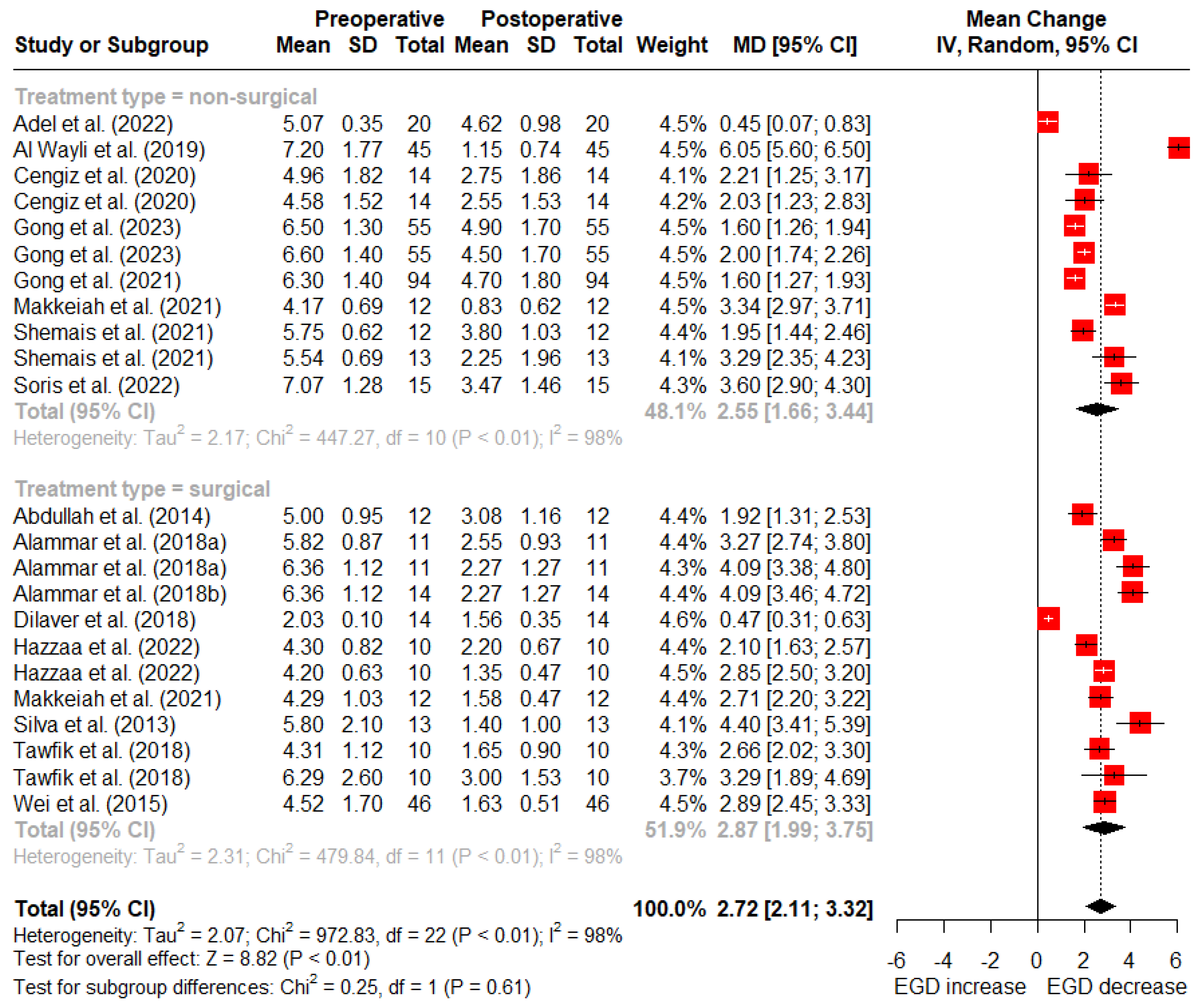
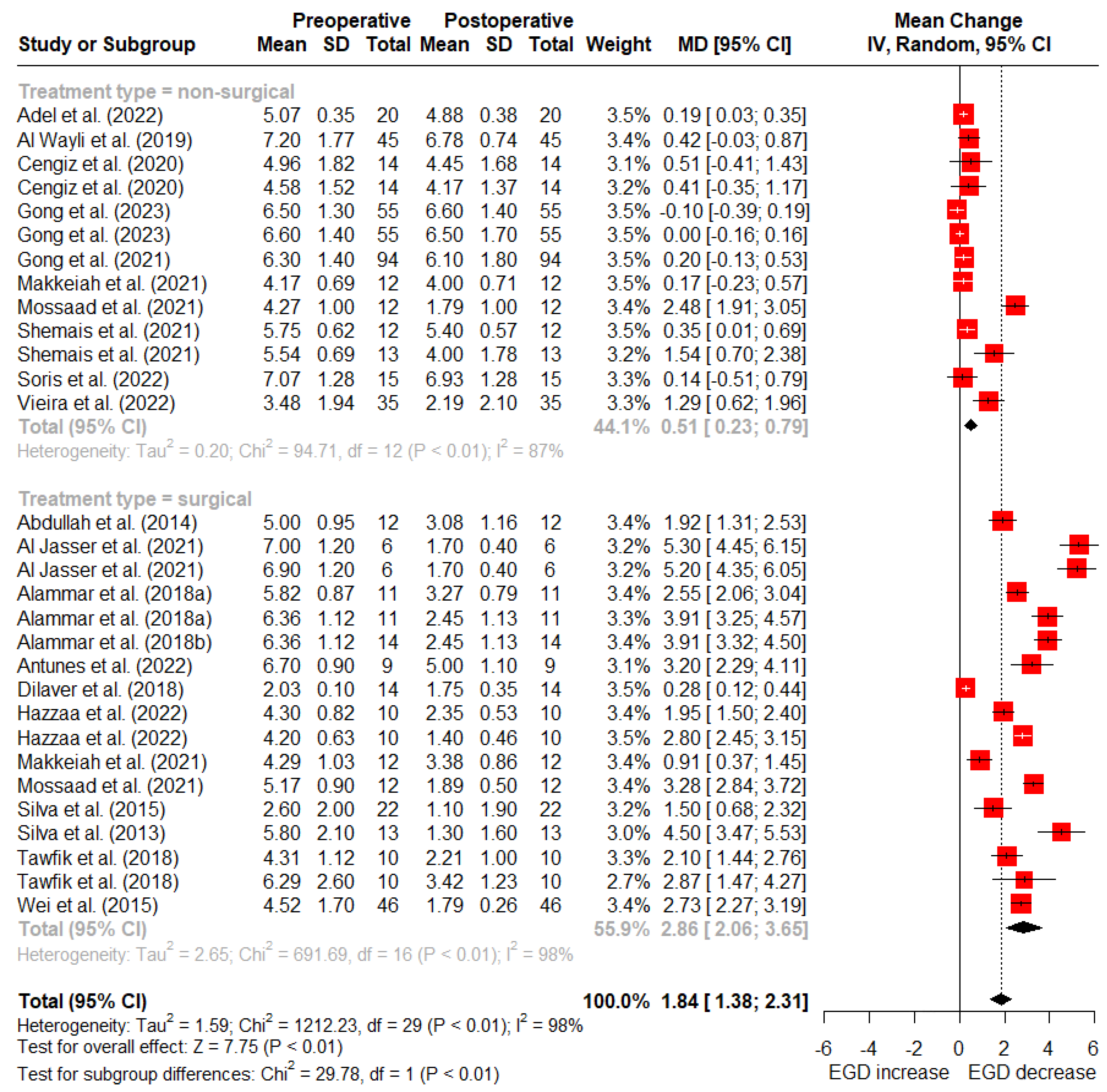
3.3. Primary Outcome
3.4. Subgroup Analysis
4. Discussion
4.1. Lip-Repositioning Surgery
4.2. Gingivectomy and Crown Lengthening
4.3. V-Y Plasty
4.4. Guided Bone Regenration
4.5. Septum Cartilage Reinforcement
4.6. Micro-Autologous Fat Transplantation
4.7. Botulinum Toxin
4.7.1. Injection Site
4.7.2. Dosage and Initial Severity of EGD
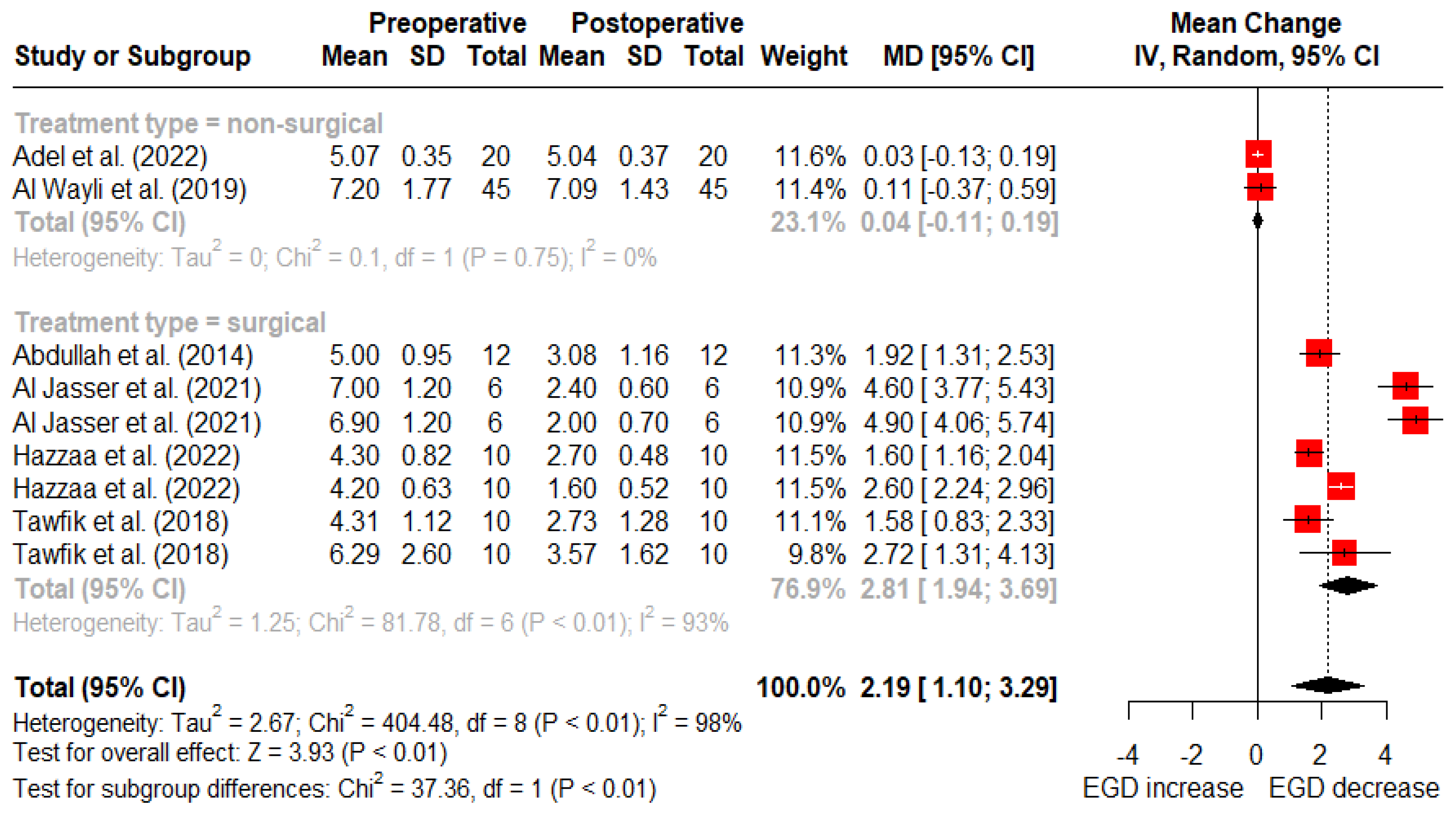
4.7.3. Stability
4.8. Orthodontic Treatment
4.9. Limtations of the Current Study
4.10. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pavone, A.F.; Ghassemian, M.; Verardi, S. Gummy Smile and Short Tooth Syndrome–Part 1: Etiopathogenesis, Classification, and Diagnostic Guidelines. Compend. Contin. Educ. Dent. 2016, 37, 102–107. [Google Scholar] [PubMed]
- Van der Geld, P.; Oosterveld, P.; Van Heck, G.; Kuijpers-Jagtman, A.M. Smile Attractiveness. Self-Perception and Influence on Personality. Angle Orthod. 2007, 77, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Peck, S.; Peck, L. Selected Aspects of the Art and Science of Facial Esthetics. In Seminars in Orthodontics; Elsevier: Amsterdam, The Netherlands, 1995; Volume 1, pp. 105–126. [Google Scholar]
- Willmar, K. On Le Fort I Osteotomy; A Follow-up Study of 106 Operated Patients with Maxillo-Facial Deformity. Scand. J. Plast. Reconstr. Surg. 1974, 12 (Suppl. S12), 1–68. [Google Scholar] [CrossRef] [PubMed]
- Dilaver, E.; Uckan, S. Effect of V-Y Plasty on Lip Lengthening and Treatment of Gummy Smile. Int. J. Oral Maxillofac. Surg. 2018, 47, 184–187. [Google Scholar] [CrossRef]
- Rubin, L.R. The Anatomy of a Smile: Its Importance in the Treatment of Facial Paralysis. Plast. Reconstr. Surg. 1974, 53, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Bhola, M.; Fairbairn, P.J.; Kolhatkar, S.; Chu, S.J.; Morris, T.; de Campos, M. LipStaT: The Lip Stabilization Technique- Indications and Guidelines for Case Selection and Classification of Excessive Gingival Display. Int. J. Periodontics Restor. Dent. 2015, 35, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Evian, C.I.; Cutler, S.A.; Rosenberg, E.S.; Shah, R.K. Altered Passive Eruption: The Undiagnosed Entity. J. Am. Dent. Assoc. 1993, 124, 107–110. [Google Scholar] [CrossRef]
- Kokich, V. Esthetics and Anterior Tooth Position: An Orthodontic Perspective Part II: Vertical Position. J. Esthet. Restor. Dent. 1993, 5, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Ishida, L.H.; Ishida, L.C.; Ishida, J.; Grynglas, J.; Alonso, N.; Ferreira, M.C. Efficiency of Gummy Smile Correction Using the Myotomy of the Elevator of the Upper Lip Muscle. Plast. Reconstr. Surg. 2009, 124, 10–11. [Google Scholar]
- Abdullah, W.A.; Khalil, H.S.; Alhindi, M.M.; Marzook, H. Modifying Gummy Smile: A Minimally Invasive Approach. J. Contemp. Dent. Pract. 2014, 15, 821–826. [Google Scholar] [CrossRef]
- Miskinyar, S.A.C. A New Method for Correcting a Gummy Smile. Plast. Reconstr. Surg. 1983, 72, 397–400. [Google Scholar] [CrossRef]
- Ellenbogen, R.; Swara, N. The Improvement of the Gummy Smile Using the Implant Spacer Technique. Ann. Plast. Surg. 1984, 12, 16–24. [Google Scholar] [CrossRef]
- McEntire, C. Three-Dimensional Soft Tissue Changes upon Smiling, Virginia Commonwealth University. 2013. Available online: https://scholarscompass.vcu.edu/etd/3009/ (accessed on 10 April 2023).
- Wei, J.; Herrler, T.; Xu, H.; Li, Q.; Dai, C. Treatment of Gummy Smile: Nasal Septum Dysplasia as Etiologic Factor and Therapeutic Target. J. Plast. Reconstr. Aesthet. Surg. 2015, 68, 1338–1343. [Google Scholar] [CrossRef]
- Huang, S.; Huang, Y.; Lin, Y.; Lee, S.; Chou, C.; Lin, T.; Takahashi, H.; Kuo, Y.; Lai, C.; Lin, S.; et al. Micro-Autologous Fat Transplantation for Treating a Gummy Smile. Aesthet. Surg. J. 2018, 38, 925–937. [Google Scholar] [CrossRef]
- Diaspro, A.; Cavallini, M.; Piersini, P.; Sito, G. Gummy Smile Treatment: Proposal for a Novel Corrective Technique and a Review of the Literature. Aesthet. Surg. J. 2018, 38, 1330–1338. [Google Scholar] [CrossRef]
- Hsien-Li Peng, P.; Peng, J.-H. Treating the Gummy Smile with Hyaluronic Acid Filler Injection. Dermatol. Surg. 2019, 45, 478–480. [Google Scholar] [CrossRef]
- Polo, M. Gummy Smile Treatment: A 40-Year Journey. AJO-DO Clin. Companion 2022, 2, 125–135. [Google Scholar] [CrossRef]
- Rasteau, S.; Savoldelli, C.; Winter, C.; Lerhe, B.; Castillo, L.; Kestemont, P. Botulinum Toxin Type A for the Treatment of Excessive Gingival Display—A Systematic Review. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e717–e723. [Google Scholar] [CrossRef]
- Lam, F.; Chan, M.Y.S. The Role of Botulinum Toxin A in the Management of Different Types of Excessive Gingival Display: A Systematic Review. Br. Dent. J. 2022, 233, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Nasr, M.W.; Jabbour, S.F.; Sidaoui, J.A.; Haber, R.N.; Kechichian, E.G. Botulinum Toxin for the Treatment of Excessive Gingival Display: A Systematic Review. Aesthet. Surg. J. 2016, 36, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Zengiski, A.C.S.; Basso, I.B.; Cavalcante-Leão, B.L.; Stechman-Neto, J.; Santos, R.S.; Guariza-Filho, O.; Zeigelboim, B.S.; Taveira, K.V.M.; de Araujo, C.M. Effect and Longevity of Botulinum Toxin in the Treatment of Gummy Smile: A Meta-Analysis and Meta-Regression. Clin. Oral Investig. 2022, 26, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Razmaitė, A.; Trakinienė, G. The Effect of Botox for the Correction of the Gummy Smile: A Systematic Review. Stomatologija 2021, 23, 63–68. [Google Scholar]
- Chagas, T.F.; de Almeida, N.V.; Lisboa, C.O.; Ferreira, D.M.T.P.; Mattos, C.T.; Mucha, J.N. Duration of Effectiveness of Botulinum Toxin Type A in Excessive Gingival Display: A Systematic Review and Meta-Analysis. Braz. Oral Res. 2018, 32, e30. [Google Scholar] [CrossRef]
- Duruel, O.; Ataman-Duruel, E.T.; Tözüm, T.F.; Berker, E. Ideal Dose and Injection Site for Gummy Smile Treatment with Botulinum Toxin-A: A Systematic Review and Introduction of a Case Study. Int. J. Periodontics Restor. Dent. 2019, 39, e167–e173. [Google Scholar] [CrossRef]
- Mendoza-Geng, A.; Gonzales-Medina, K.; Meza-Mauricio, J.; Muniz, F.W.M.G.; Vergara-Buenaventura, A. Clinical Efficacy of Lip Repositioning Technique and Its Modifications for the Treatment of Gummy Smile: Systematic Review and Meta-Analysis. Clin. Oral Investig. 2022, 26, 4243–4261. [Google Scholar] [CrossRef] [PubMed]
- Younespour, S.; Yaghobee, S.; Aslroosta, H.; Moslemi, N.; Pourheydar, E.; Ghafary, E.S. Effectiveness of Different Modalities of Lip Repositioning Surgery for Management of Patients Complaining of Excessive Gingival Display: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2021, 2021, 9476013. [Google Scholar] [CrossRef]
- dos Santos-Pereira, S.A.; Cicareli, A.J.; Idalgo, F.A.; Nunes, A.G.; Kassis, E.N.; Castanha Henriques, J.F.; Bellini-Pereira, S.A. Effectiveness of Lip Repositioning Surgeries in the Treatment of Excessive Gingival Display: A Systematic Review and Meta-Analysis. J. Esthet. Restor. Dent. 2021, 33, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, O.K.; El-Nahass, H.E.; Shipman, P.; Looney, S.W.; Cutler, C.W.; Brunner, M. Lip Repositioning for the Treatment of Excess Gingival Display: A Systematic Review. J. Esthet. Restor. Dent. 2018, 30, 101–112. [Google Scholar] [CrossRef]
- Ardakani, M.T.; Moscowchi, A.; Valian, N.K.; Zakerzadeh, E. Lip Repositioning with or without Myotomy: A Systematic Review. J. Korean Assoc. Oral Maxillofac. Surg. 2021, 47, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Alshammery, D.; Alqhtani, N.; Alajmi, A.; Dagriri, L.; Alrukban, N.; Alshahrani, R.; Alghamdi, S. Non-Surgical Correction of Gummy Smile Using Temporary Skeletal Mini-Screw Anchorage Devices: A Systematic Review. J. Clin. Exp. Dent. 2021, 13, 717–723. [Google Scholar] [CrossRef]
- Moher, D.; Tetzlaff, J.; Tricco, A.C.; Sampson, M.; Altman, D.G. Epidemiology and Reporting Characteristics of Systematic Reviews. PLoS Med. 2007, 4, e78. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; McAleenan, A.; Reeves, B.C.; Higgins, J.P.T. Chapter 25: Assessing Risk of Bias in a Non-Randomized Study. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Chichester, UK, 2023; Available online: www.training.cochrane.org/handbook (accessed on 28 August 2023).
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing Risk of Bias in a Randomized Trial. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Chichester, UK, 2023; Available online: www.Training.Cochrane.org/handbook (accessed on 28 August 2023).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. BMJ Ment Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- RStudio Team. RStudio: Integrated Development for R. RStudio, PBC. Version 2023.09.0. Available online: https://www.rstudio.com/ (accessed on 24 November 2023).
- Gong, X.; Yuan, M.; Gu, C.; Yan, B.; Li, J.; Zou, L.; An, Y.; Tang, Z.; Han, X. Effects of Dose and Injection Site on Gingival Smile Treatment with Botulinum Toxin Type A: A Prospective Study. Plast. Reconstr. Surg. 2023, 151, 56e–67e. [Google Scholar] [CrossRef] [PubMed]
- Gong, X.; Huang, H.; Gu, C.; Li, F.; Zou, L.; An, Y.; Han, X.; Tang, Z. Individual Factors of Botulinum Type A in Treatment of Gummy Smile: A Prospective Study. Aesthet. Surg. J. 2021, 41, NP842–NP850. [Google Scholar] [CrossRef] [PubMed]
- Andriola, F.d.O.; Chieza, G.S.; Cavagni, J.; Freddo, A.L.; Corsetti, A. Management of Excessive Gingival Display Using Botulinum Toxin Type A: A Descriptive Study. Toxicon 2021, 196, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.V.; Hirata, D.Y.; Reis, A.F.; Santos, V.R.; Miranda, T.S.; Faveri, M.; Duarte, P.M. Open-Flap versus Flapless Esthetic Crown Lengthening: 12-Month Clinical Outcomes of a Randomized Controlled Clinical Trial. J. Periodontol. 2014, 85, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Altayeb, W.; Arnabat-Dominguez, J.; Low, S.; Abdullah, A.; Romanos, G. Laser-Assisted Esthetic Crown Lengthening: Open-Flap Versus Flapless. Int. J. Periodontics Restor. Dent. 2022, 42, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, K.; Tamada, Y.; Tabuchi, M.; Kawaguchi, M.; Shibata, M.; Sato, T.; Okamoto, K.; Saito, N.; Goto, S. Effective Approach for Improving a Gummy Smile: Upward Movement of the Maxillary Occlusal Plane Using Midpalatal Miniscrews and a Modified Transpalatal Arch. J. Orofac. Orthop. 2022, 85, 167–180. [Google Scholar] [CrossRef]
- Ferreira, C.E.; Brandao, R.C.; Martinelli, C.B.; Pignaton, T.B. Improving Gingival Smile by Means of Guided Bone Regeneration Principles. Dent. Press. J. Orthod. 2016, 21, 116–125. [Google Scholar] [CrossRef]
- Silva, C.O.; Ribeiro-Junior, N.V.; Campos, T.V.S.; Rodrigues, J.G.; Tatakis, D.N. Excessive gingival display: Treatment by a modified lip repositioning technique. J. Clin. Periodontol. 2013, 40, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.O.; Soumaille, J.M.S.; Marson, F.C.; Progiante, P.S.; Tatakis, D.N. Aesthetic crown lengthening: Periodontal and patient-centred outcomes. J. Clin. Periodontol. 2015, 42, 1126–1134. [Google Scholar] [CrossRef]
- Alammar, A.; Heshmeh, O.; Mounajjed, R.; Goodson, M.; Hamadah, O. A comparison between modified and conventional surgical techniques for surgical lip repositioning in the management of the gummy smile. J. Esthet. Restor. Dent. 2018, 30, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Alammar, A.M.; Heshmeh, O.A. Lip Repositioning with a Myotomy of the Elevator Muscles for the Management of a Gummy Smile. Dent. Med. Probl. 2018, 55, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, O.K.; Naiem, S.N.; Tawfik, L.K.; Yussif, N.; Meghil, M.M.; Cutler, C.W.; Darhous, M.; El-Nahass, H.E. Lip repositioning with or without myotomy: A randomized clinical trial. J. Periodontol. 2018, 89, 815–823. [Google Scholar] [CrossRef]
- Al Jasser, R.N.; AlSarhan, M.A.; Alotaibi, D.H.; Bhola, M. A Modified Approach in Lip Repositioning Surgery: A Prospective Study in a Twin Population with a 3-Year Follow-Up. Int. J. Periodontics Restor. Dent. 2021, 41, e243–e253. [Google Scholar] [CrossRef] [PubMed]
- Hazzaa, H.H.; Elwakeel, N.M.; Abdulhady, E.M.; Abdel-Aziz, L.M. Evaluation of the internal dual muscle traction approach as an adjunct to the modified surgical lip repositioning method: A randomized clinical report. J. Oral Maxillofac. Surg. Med. Pathol. 2022, 34, 12–18. [Google Scholar] [CrossRef]
- Al Wayli, H. Versatility of Botulinum Toxin at the Yonsei Point for the Treatment of Gummy Smile. Int. J. Esthet. Dent. 2019, 14, 86–95. [Google Scholar] [PubMed]
- Cengiz, A.F.; Goymen, M.; Akcali, C. Efficacy of Botulinum Toxin for Treating a Gummy Smile. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 50–58. [Google Scholar] [CrossRef]
- Shemais, N.; Elarab, A.E.; ElNahass, H. The Effect of Botulinum Toxin A in Patients with Excessive Gingival Display with and without Zinc Supplementation: Randomized Clinical Trial. Clin. Oral Investig. 2021, 25, 6403–6417. [Google Scholar] [CrossRef]
- Adel, N. A Standardized Technique for Gummy Smile Treatment Using Repeated Botulinum Toxins: A 1-year Follow-up Study. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4281. [Google Scholar] [CrossRef] [PubMed]
- Soris, B.A.T.; Shenoy, K.V.; Ramadorai, A.; Kumar, C.S.C.S.; Marimuthu, L. Botulinum Toxin-A in the Treatment of Excessive Gingival Display: A Clinical Study. J. Maxillofac. Oral Surg. 2022, 21, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Vieira, C.E.A.; de Almeida, W.R.; Cotrin, P.; de Oliveira, R.C.G.; de Oliveira, R.C.G.; Valarelli, F.P.; Zamuner, J.W.; de Freitas, K.M.S. Evaluation of the botulinum toxin effects in the correction of gummy smile 32 weeks after application. ABCS Health Sci. 2022, 47, e022201. [Google Scholar] [CrossRef]
- Makkeiah, M.O.; Harfoush, M.; Makkiah, A.; Saneeva, L.; Tuturov, N.; Katbeh, I. Comparative efficacy of Botox and surgical lip repositioning in the correction of gummy smile. Stomatologiia 2021, 100, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Mossaad, A.M.; Abdelrahman, M.A.; Kotb, A.M.; Alolayan, A.B.; Elsayed, S.A.-H. Gummy Smile Management Using Diode Laser Gingivectomy Versus Botulinum Toxin Injection—A Prospective Study. Ann. Maxillofac. Surg. 2021, 11, 70–74. [Google Scholar] [PubMed]
- Antunes, K.B.; Dias, A.; Kahn, S.; Schneider, L.F.J.; Cavalcante, L.M. Use of Botulinum Toxin Before Surgical Lip Repositioning: A Randomized Clinical Trial. Int. J. Periodontics Restor. Dent. 2022, 42, e175–e183. [Google Scholar] [CrossRef] [PubMed]
- Horn, R.O.R.; Elias, C.N.; Joly, J.C. A Lip Repositioning Technique Using Polyester Threads for Gummy Smile Treatment. Int. J. Dent. 2022, 2022, 3972150. [Google Scholar] [CrossRef] [PubMed]
- Garber, D.A.; Salama, M.A. The Aesthetic Smile: Diagnosis and Treatment. Periodontology 2000 1996, 11, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Akram, H.M.; Ali, O.H.; Omran, N.K.; Ali, A.O. Diode Laser versus Scalpel Gingivectomy. Biomed. Pharmacol. J. 2017, 10, 1799–1804. [Google Scholar] [CrossRef]
- Muradin, M.; Rosenberg, A.; van der Bilt, A.; Stoelinga, P.; Koole, R. The Effect of Alar Cinch Sutures and V-Y Closure on Soft Tissue Dynamics after Le Fort I Intrusion Osteotomies. J. Cranio-Maxillo-Facial Surg. 2009, 37, 334–340. [Google Scholar] [CrossRef]
- Rubin, L.R.; Mishriki, Y.; Lee, G. Anatomy of the Nasolabial Fold: The Keystone of the Smiling Mechanism. Plast. Reconstr. Surg. 1989, 83, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.-S.; Hur, M.-S.; Hu, K.-S.; Song, W.-C.; Koh, K.-S.; Baik, H.-S.; Kim, S.-T.; Kim, H.-J.; Lee, K.-J. Surface Anatomy of the Lip Elevator Muscles for the Treatment of Gummy Smile Using Botulinum Toxin. Angle Orthod. 2009, 79, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Koshy, J.C.; Sharabi, S.E.; Feldman, E.M.; Hollier, L.H.; Patrinely, J.R.; Soparkar, C.N.S. Effect of Dietary Zinc and Phytase Supplementation on Botulinum Toxin Treatments. J. Drugs Dermatol. 2012, 11, 507–512. [Google Scholar] [PubMed]
- Papageorgiou, S.N.; Xavier, G.M.; Cobourne, M.T. Basic Study Design Influences the Results of Orthodontic Clinical Investigations. J. Clin. Epidemiol. 2015, 68, 1512–1522. [Google Scholar] [CrossRef]
- Peck, S.; Peck, L.; Kataja, M. The Gingival Smile Line. Angle Orthod. 1992, 62, 91–100; discussion 101–102. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/ Year | Country | Study Design | Population Age N (F:M) | Etiology | Intervention Number (n) | Comparison Number (n) | Landmark for Measurement | Pre-Treatment Gingival Exposure | Post-Treatment Gingival Exposure | Follow-Up | Measured Stability at Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Silva 2013 [46] | Brazil | prospective | 28.7 ± 11.0 (19–49) N = 13 (11:2) | hyperactive upper lip (>8 mm mobility) | modified LRS without excision of maxillary midline labial frenum | baseline | from the inferior border of the upper lip vermillion to the GM of the right central incisor | 5.80 ± 2.1 | 3 months 1.40 ± 1.00 | 3, 6 months | 6 months 1.30 ± 1.60 |
| Abdullah 2014 [11] | Saudi Arabia | N/A | 23.75 ± 2.89 (20–29) N = 12 (10:2) | not specified (acceptable vertical dimension and tooth–gingiva relationship) | LRS with frenectomy and myotomy of LLS muscles using circumdental sutures | baseline | N/A | 5.0 ± 0.95 | 1 month 2.66 ± 0.77 | 1, 3, 6, 12 months | 3, 6, 12 months 3.08 ± 1.16 |
| Ribeiro 2014 [42] | Brazil | split-mouth randomized controlled trial | 27.5± 5.8 (21–40) N = 28 (20:8) | APE in at least three maxillary teeth (excluded: orthodontic treatment) | conventional open-flap (OF) ECL (n = 28) | flapless (FL) ECL (n = 28) | relative GM on buccal surface measured using a surgical stent | N/A | reduction from baseline OF: 1.3 ± 0.5 FL: 1.1 ± 0.5 | 3, 6, 12 months | reduction at 3 months: OF: 1.2 ± 0.5 FL: 1.0 ± 0.5 reduction at 6 and 12 months: OF and FL: 1.0 ± 0.5 |
| Silva 2015 [47] | Brazil | prospective | 23.5 ± 2.7 (19–32) N = 32 (26:6) | APE—width/length ratio ≥0.85 and gingival margin incisal to tooth cervical convexity (excluded: orthodontic treatment, heavy restorations) | ECL with osteoplasty and osteotomy | baseline | distance between central incisor GM during active smile and the inferior border of the upper lip vermilion | 2.6 ± 2.0 | N/A | 6 months | 1.1 ± 1.9 |
| Wei 2015 [15] | China | prospective | 28.7 ± 7.7 (18–49) N = 46 (gender N/A) | nasal septum dysplasia with increased columella upward maximum movability (CUMM) | septum cartilage reinforcement and additional extension as needed (auricular cartilage n = 18, costicartilage n= 13, ePTFE implant n = 15, augmentation rhinoplasty n = 31) | 150 volunteers | N/A | 4.52 ± 1.7 | 1 month 1.18 ± 0.59 | 1, 3, 6 months | 3 months 1.63 ± 0.51 6 months 1.79 ± 0.26 |
| Ferreira 2016 [45] | Brazil | prospective | 26 (20–49) N = 12 (F) | VME | GBR with xenogenic bone substitute (Bio-OssTM) and resorbable membrane (Bio-GideTM); n = 8 required ECL | baseline | measured surface area of gingival exposure | 275.44 mm2 (≥5 mm during full posed smile) | N/A | 1, 6, 12 months | 12 months no ECL: reduction of 112.01 mm2 with ECL: reduction of 167.01 mm2 |
| Alammar 2018 a [48] | Syria | prospective | 18–38 N = 22 (19:3) | short upper lip, hyperactive lip elevator muscles (>8 mm mobility) | conventional LRS (partial-thickness flap excluding myotomy elevator muscles) (n = 11) | modified LRS (full-thickness flap with myotomy of elevator muscles) (n = 11) | inferior border of upper lip vermillion to the gingival margin of the anterior maxillary teeth | conventional: 5.82 ± 0.87 modified: 6.36 ± 1.12 | 1 month conventional: 2.18 ± 0.75 modified: 0.91 ± 1.22 | 1, 3, 6 months | 3 months conventional: 2.55 ± 0.93 modified: 2.27 ± 1.27 6 months conventional: 3.27 ± 0.79 modified: 2.45 ± 1.13 |
| Alammar 2018 b [49] | Syria | prospective | 18–38 N = 14 (gender N/A) | short upper lip, hyperactive lip elevator muscles (>8 mm mobility) (excluded: VME, gingival display >6 mm) | LRS (full-thickness flap, V-shaped in the upper lip frenum to preserve the labial midline) with myotomy of the elevator muscles. | Baseline | inferior border of the upper lip vermillion to the gingival margin of the anterior maxillary teeth during full active smile | 6.36 ± 1.12 | 1 month 0.91 ± 1.22 | 1, 3, 6 months | 3 months 2.27 ± 1.27 6 months 2.45 ± 1.13 |
| Dilaver 2018 [5] | Turkey | prospective | 23.2 (18–30) N = 14 (12:2) | short upper lip (<20 mm in F, <23 mm in M), VME cases that refused surgery (excluded: gingival hyperplasia, APE, short clinical crown, prior V–Y plasty) | V-Y plasty with supra-periosteal dissection of submucosa and underlying muscles | baseline | middle uppermost point of the gingival margin of each crown and the corresponding locations on the upper lip measured for central incisors | 2.03 ± 0.1 | 1 month 0.80 ± 0.12 | 1, 3, 6 months | 3 months 1.56 ± 0.35 6 months 1.75 ± 0.35 |
| Tawfik 2018 [50] | Egypt | single-blinded, randomized clinical trial | ≥18 N = 20 (18:2) | not specified (all with normal clinical crown dimensions) | LRS with myotomy (lower incision like Rosenblatt and Simon and upper incision like Rubenstein and Kostianovsky modification) (n = 10) | conventional LRS without myotomy (n = 10) | N/A | with myotomy: 6.29 ± 2.6 without myotomy: 4.31 ± 1.12 | 3 months with myotomy: 3.00 ± 1.53 without myotomy: 1.65 ± 0.9 | 3, 6, 12 months | 6 months with myotomy: 3.42 ± 1.23 without myotomy: 2.21 ± 1.0 12 months with myotomy: 3.57 ± 1.62 without myotomy: 2.73 ± 1.28 |
| Al Jasser 2021 [51] | Saudi Arabia | prospective | ≥18 years N = 12 (twins) (F) | Excluded: VME, skeletal deformity, previous Botox or fillers, short upper lip, APE | LRS by LipStaT technique—no suture in the thick connective tissue (n = 6) | LRS with deep periosteal suture in the thick connective tissue (n = 6) | molar to molar at 3 buccal locations, from gingival margin to base of the upper lip during full dynamic smile | without periosteal suture: 7.0 ± 1.2 with periosteal suture: 6.9 ± 1.2 | 6 months without periosteal suture: 1.7 ± 0.4 with periosteal suture: 1.7 ± 0.4 | 1, 2, 3, 4 weeks, 1, 6 months, 1, 2, 3 years | 1 and 2 years without periosteal suture: 2.4 ± 0.6 with periosteal suture: 2 ± 0.7 3 years without periosteal suture: 5.0 ± 1.8 with periosteal suture: 3.5 ± 1.4 |
| Altayeb 2022 [43] | Qatar-USA | randomized clinical study | 22–45 N = 36 (22:14) | APE (gingival overlap of over 19% of the anatomical crown height) | Er,Cr:YSGG (2780 nm) laser–assistedopen-flap (OF) ECL with variable-thickness flap (n = 18) | Er,Cr:YSGG (2780 nm) laser–assisted flapless (FL) ECL (n = 18) | GM level of central incisors (from incisal edge to gingival zenith) | N/A | reduction from baseline OF: 2.37 ± 0.54 FL: 2.28 ± 0.39 | 1, 3, 9 months | Reduction at 1 month OF: 2.34 ± 0.48 FL: 2 ± 0.48 3 months OF: 2.16 ± 0.48 FL: 1.9 ± 0.33 9 months OF: 2.09 ± 0.49 FL: 2.01 ± 0.41 |
| Hazzaa 2022 [52] | Egypt | randomized clinical trial | iMTA: 30.7 ± 5.0 LRS alone: 29.9 ± 3.1 N = 20 (14:6) | excluded: VME >8 mm | modified LRS with internal dual muscular traction approach (iMTA) and evelo-periosteal suturing (n = 10) | modified LRS (excluding maxillary labial frenum) (n = 10) | gingival margin until the upper border of the lip | iMTA: 4.2 ± 0.63 LRS alone: 4.3 ± 0.82 | 3 months iMTA: 1.35 ± 0.47 LRS alone: 2.2 ± 0.67 | 3, 6, 12 months | 6 months iMTA: 1.4 ± 0.46 LRS alone: 2.35 ± 0.53 12 months iMTA: 1.6 ± 0.52 LRS alone: 2.7 ± 0.48 |
| Huang 2018 [16] | Taiwan | N/A | 23–40 N = 7 (6:1) | N/A | fat micro-transplantation into the nasolabial groove, ergotrid, and upper lip using MAFT-GUN (mean volume: 16.1 mL) | baseline | gum line at the midline of the incisors (right and left) and canines (right and left) to the lowest portion of the upper lip | 4.4 ± 2.5 | measured at follow-up | 6–24 months | −0.5 ± 1.2 |
| Al Wayli 2019 [53] | Saudi Arabia | prospective | 30.5 ± 9.43 (18–45) N = 45 (F) | hyperfunctional upper lip elevator muscles; other diagnosed etiologies were corrected before the study (excluded VME) | BTX, Dysport dilution: 100 units/2.0 mL injection site: Yonsei points bilaterally dose: 3 units/side | baseline | distance between the lowest margin of the upper lipperpendicular to the midportion of the maxillary central incisor’s gingival margin | 7.20 ± 1.77 | 12 weeks 1.15 ± 0.74 | 2, 12, 24, 36 weeks | 24 weeks 6.78 ± 0.74 36 weeks 7.09 ± 1.43 |
| Cengiz 2020 [54] | Turkey | prospective cohort | 22.11 ± 4.55 (19.8–38.1) N = 28 (21:7) | not specified (excluded: >8 mm EGD) | BTX, Allergan dilution: 100 units/2.0 mL injection site: LLSAN on the most superior point of the nasolabial fold dose: 2.5 units/side | BTX, Allergan dilution: 100 units/2.0 mL injection site: OO, 5 mm inferior to the central and most inferior point of the nostrils dose: 1.25 units/side | distance between the gingival margin on the midline of the maxillary right central incisor and the inferior border of the upper lip | LLSAN: 4.96 ± 1.82 OO: 4.58 ± 1.52 | 3 days LLSAN: 2.48 ± 1.85 OO: 2.80 ± 1.75 | 3, 15 days, 1, 4, 5, 6 months | 15 days LLSAN: 1.92 ± 1.70 OO: 2.16 ± 1.65 1 month LLSAN: 1.83 ± 1.74 OO: 2.2 ± 1.57 4 months LLSAN: 2.75 ± 1.86 OO: 2.55 ± 1.53 6 months LLSAN: 4.45 ± 1.68 OO: 4.17 ± 1.37 |
| Gong 2021 [40] | China | prospective | 27 (25–32) N = 94 (77:17) | excluded: previous disease or treatment affecting the position of the gingiva or upper lip | BTX, Allergan dilution: 100 units/2.0 mL injection site: LLSAN at the muscle bulge at the uppermost part of the nasolabial fold dose: 2 units/side | baseline | distance between the inferior margin point of the right central incisor and the lower margin of the upper lip | 6.3 ± 1.4 (anterior) | 4 weeks 3.9 ± 2.0 | 4, 12, 32 weeks | 12 weeks 4.7 ± 1.8 32 weeks 6.1 ± 1.8 |
| Shemais 2021 [55] | Egypt | randomized controlled clinical trial | 25 ± 4 (20–30) N = 25 (23:2) | hypermobile and short lip, VME of maximum 4 mm, normal clinical crown dimensions | 50 mg oral zinc supplement for 4 days prior to injection with BTX-A, Allergan dilution: N/A injection site: Yonsei points (1 cm lateral to the ala and 3 cm above the lip line) dose: 3 units/side (n = 13) | BTX-A, Allergan without zinc supplement (n = 12) | recorded using a UNC15 periodontal probe at the midpoint of the right central incisor and premolars at maximum smile | Zinc and BTX: 5.54 ± 0.69 BTX only: 5.75 ± 0.62 | 2 weeks Zinc and BTX: 0.65 ± 1.26 BTX only: 1.41 ± 0.86 | 2, 6, 12, 18, 24 weeks | 12 week Zinc and BTX: 2.25 ±1.06 BTX only: 3.8 ± 1.03 24 weeks Zinc and BTX: 4 ± 1.78 BTX only: 5.4 ± 0.57 |
| Adel 2022 [56] | Egypt | N/A | 25–45 N = 20 (F) | hypermobile upper lip (twice normal translation range of 6–8 mm) | BTX dilution: 100 unit/2 mL injection site: Yonsei point for all cases, additional 2 points at insertion of ZM muscles for mixed smile cases dose: 1 unit at Yonsei point per 1 mm of gingival show, 0.5 unit for other points; additional injection at 4 and 8 months | baseline | vertical distance from free gingival margin of central incisor to lower border of upper lip measured digitally on smiling | 5.07 ± 0.35 | 14 days 0 ± 0 | 14 days, 4, 8, 12 months | 4 months 4.62 ± 0.98 8 months 4.88 ± 0.38 12 months 5.04 ± 0.37 |
| Miyazawa 2022 [44] | Japan | retrospective | 23.2 ± 4.2 (17–33) N = 16 (F) | gummy smile ≥3.0 mm, maxillary or bimaxillary protrusion | orthodontic treatment with extraction of 4 premolars and two self-drilling miniscrews in the midpalatal suture ligated to a modified transpalatal arch | baseline | movement of prosthion was used to quantify the changes in gingival exposure at the maxillary central incisors | 4.6 ± 1.2 | 1.6 ± 1.6 | average treatment duration: 4 years 2 months (2.5–8 years) | N/A |
| Soris 2022 [57] | India | N/A | 18–40 N = 15 (10:5) | hyperactive lip elevator muscles or VME (excluded: short upper lip) | BTX, Allergan dilution: 4 unit/0.1 mL injection site: Yonsei points and upper lip philtrum dose: 4 units/side at Yonsei points and 2 units at upper lip philtrum | baseline | crest of the gingiva (centrals in anterior and premolars in posterior gummy smile) to the lower most border of the upper lip | 7.07 ± 1.28 | 7 days 5.07 ± 0.96 | 3, 7, 15 days, 1, 2, 3, 4, 5, 6 months | 15 days 3.40 ± 1.06 1 month 3.07 ± 1.33 3 months 3.47 ± 1.46 6 months 6.93 ± 1.28 |
| Vieira 2022 [58] | Brazil | prospective | 25.5 ± 5.6 N = 35 (30:5) | muscular hyperfunction (excluded: VME, >5 mm of gingival display) | BTX, Dysport dilution: 2 units/0.01 mL injection site: LLSAN muscle dose: 2 units/side | baseline | linear distance between lower margin of the upper lip to the incisal edge of the maxillary central incisor minus the size of the crown of the right maxillary central incisor | 3.48 ± 1.94 | 2 weeks −0.04 ± 1.57 | 2, 32 weeks | 32 weeks 2.19 ± 2.10 |
| Gong 2023 [39] | China | prospective | 28.9 ± 5.9 (18–60) N = 55 (51:4) | hypermobility of upper lip, short clinical crown, dentoalveolar extrusion, short upper lip (excluded: history of or active orthodontic treatment) | BTX, Allergan simplified injection dilution: 100 units/2.5 mL injection site: bilateral LLSAN dose: 2 units/side | individualized injection after 8 months dilution: 100 units/2.5 mL injection site: bilateral LLSAN and Yonsei points dose: base on severity of anterior gingival smile: mild (3–5 mm) 2 units/side moderate (5–7 mm): 3 units/side severe (≥7 mm): 5 units/side | distance between the superior margin of the right incisor and the lower margin of the upper lip | simplified: 6.5 ± 1.3 individualized: 6.6 ± 1.4 | 4 weeks simplified: 4.1 ± 1.8 individualized: 3.8 ± 1.6 | 4, 12, 32 weeks | 12 weeks simplified: 4.9 ± 1.7 individualized: 4.5 ± 1.7 32 weeks simplified: 6.6 ± 1.4 individualized: 6.5 ± 1.7 |
| Makkeiah 2021 [59] | Syria | prospective cohort | 18–41 N = 24 (F) | hyperactive upper lip | LRS (partial-thickness flap) (n = 12) | BTX A dilution: 100 units/2 mL injection sites: 3 sites bilaterally into the LLS and LLSAN muscles dose: 4–6 units/site (n = 12) | difference between the lower margin of the upper lip and the superior margin of the right and left central incisors and canines at maximum smile | LRS: 4.25 ± 0.85 BTX: 4.29 ± 0.53 | 2 weeks LRS: 1.35 ± 0.72 BTX: 0.46 ± 0.38 | 2 weeks, 2, 6 months | 2 months LRS: 2.17 ± 0.52 BTX: 1.73 ± 0.38 6 months LRS: 3.23 ± 0.74 BTX: 3.94 ± 0.55 |
| Mossaad 2021 [60] | Egypt | comparative cohort | 25–35 N = 24 (F) | excluded: VME | diode laser gingivectomy (premolar to premolar) (n = 12) | BTX, Allergan: dilution: 100 units/2.5 mL injection site: 4 units on both sides of the nasolabial fold at Yonsei points and 2 units below the nose (orbicularis oris muscle) dose: 6 units/side (n = 12) | vertical exposure of gingiva from the lower border of the upper lip to the free gingival margin of the maxillary anterior teeth | laser: 5.17 ± 0.9 BTX: 4.27 ± 1.0 | 1 week laser: 1.89 ± 0.5 BTX: 1.79 ± 1.0 | 1 week, 1, 3, 6 months | at 6 months, BTX group returned to pre-treatment evel but effect of laser remained; no measurements reported |
| Antunes 2022 [61] | Brazil | randomized clinical trial | 20–46 N = 18 (F) | hyperactive upper lip (lip displacement ≥ 9 mm) with or without other causes of EGD such as VME or APE (excluded: short lip) | BTX A, Allergan 15 days beforeLRS (partial-thickness flap) dilution: 50 units/1 mL injection site: bilateral LLSAN, LLS, Zmi muscles injection dose: 2 units/muscle, 6 units/side (n = 9) | LRS (partial-thickness flap) alone (n = 9) | cervical margin of the maxillary right central incisor to the lip at maximum smile | BTX and LRS: 6.1 ± 0.8 LRS: 6.7 ± 0.9 mm | N/A | 15 days, 3, 6 months | 6 months BTX and LRS: 1.6 ± 1.4 LRS: 5.0 ± 1.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maleki, M.; Huang, B.; Mendes, V.C.; Caminiti, M.F.; Finer, Y. A Systematic Review and Meta-Analysis Comparing Surgical and Nonsurgical Treatments for Excessive Gingival Display. Dent. J. 2024, 12, 154. https://doi.org/10.3390/dj12060154
Maleki M, Huang B, Mendes VC, Caminiti MF, Finer Y. A Systematic Review and Meta-Analysis Comparing Surgical and Nonsurgical Treatments for Excessive Gingival Display. Dentistry Journal. 2024; 12(6):154. https://doi.org/10.3390/dj12060154
Chicago/Turabian StyleMaleki, Mahdis, Bo Huang, Vanessa C. Mendes, Marco F. Caminiti, and Yoav Finer. 2024. "A Systematic Review and Meta-Analysis Comparing Surgical and Nonsurgical Treatments for Excessive Gingival Display" Dentistry Journal 12, no. 6: 154. https://doi.org/10.3390/dj12060154