
Perception of Virtual Education Learning among Dental Residents and Faculty during the COVID-19 Pandemic: A Cross-Sectional Study
 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Questionnaire Design
2.3. Data Analysis
3. Results
3.1. Demographics
3.2. Perceptions of Virtual Learning
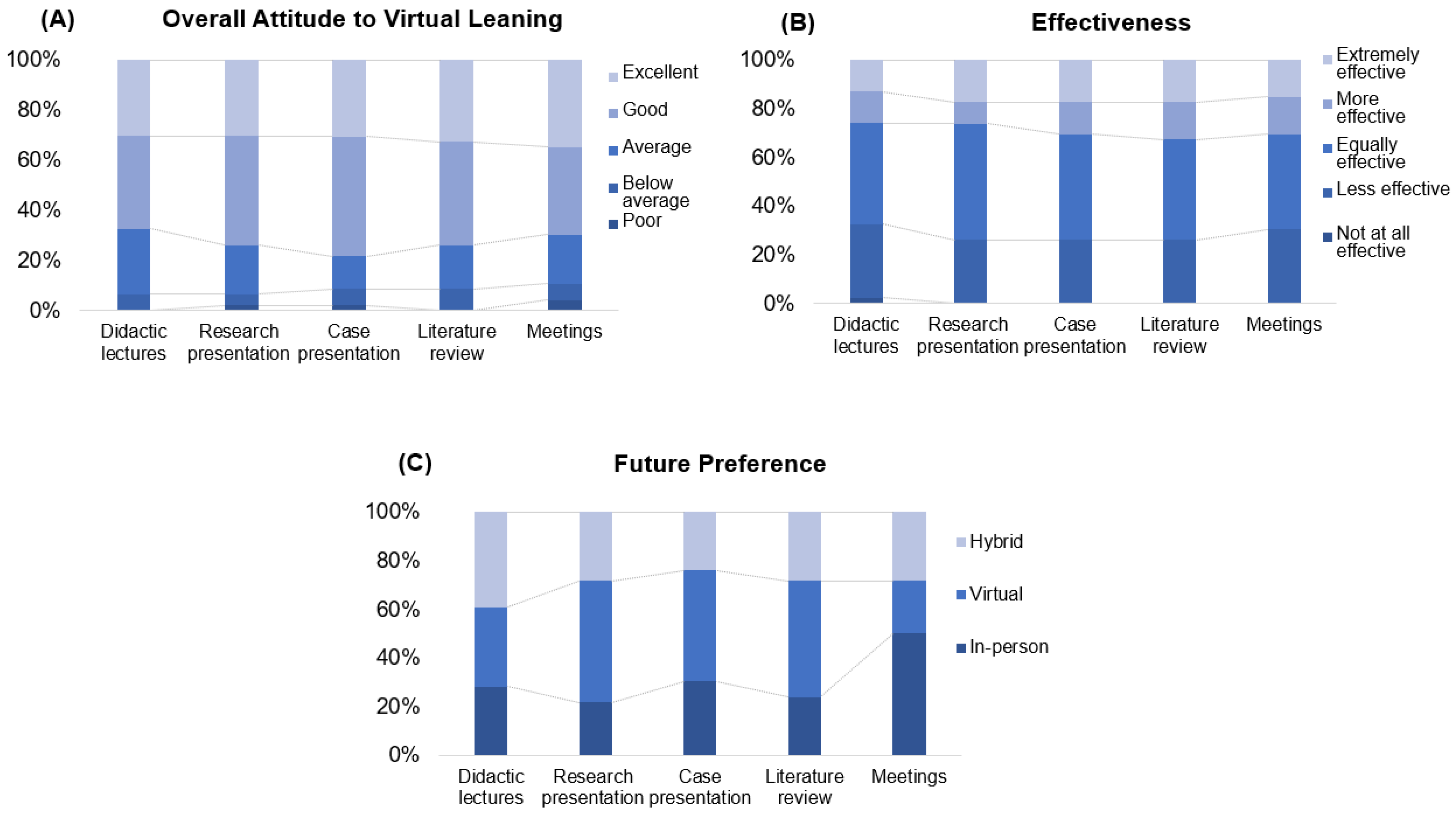
3.2.1. Residents’ Overall Feelings about Virtual Learning Modalities
3.2.2. Effectiveness of Residents’ Virtual Learning Experience in Comparison to That of the In-Person Learning Experience
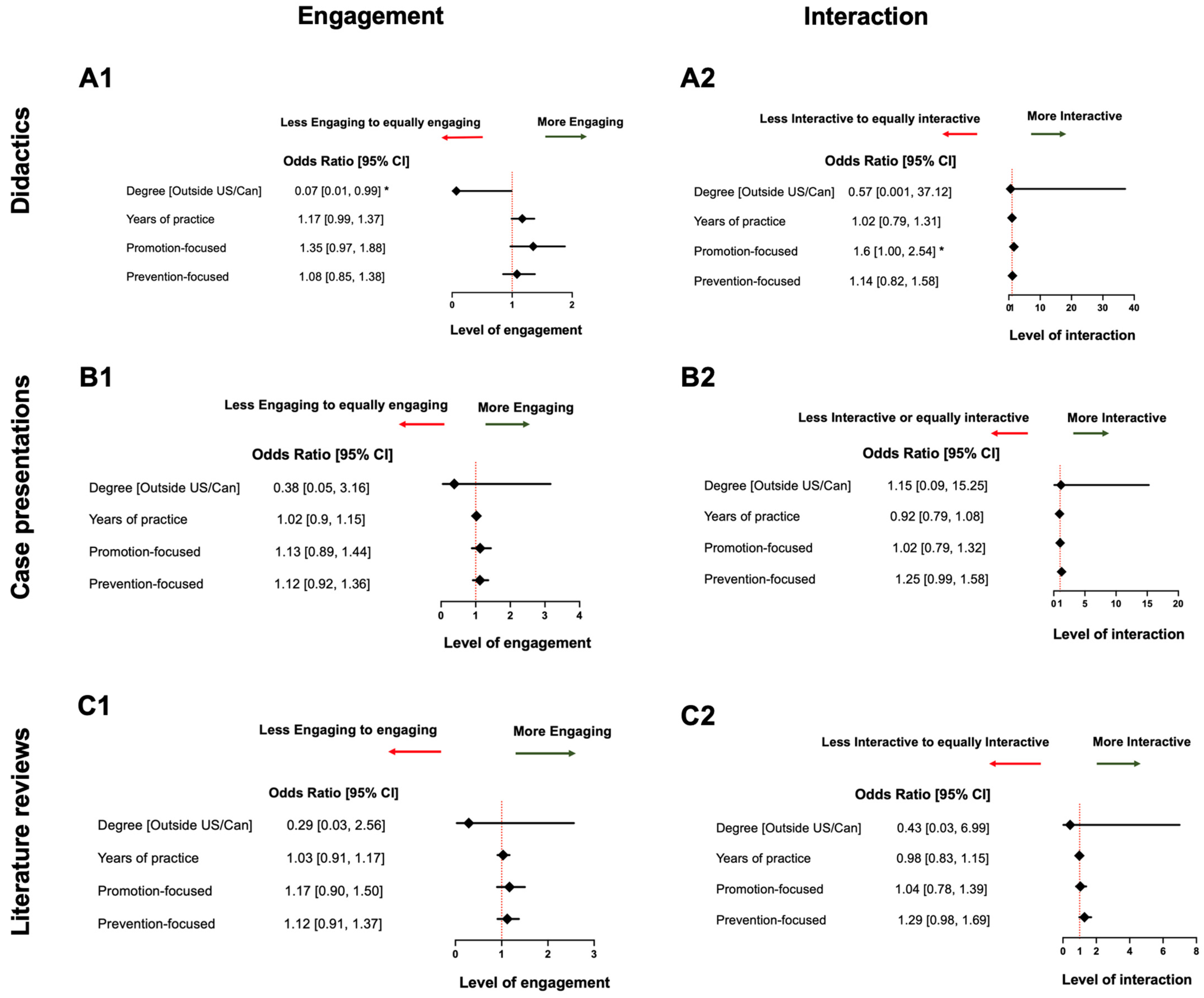
3.2.3. Engagement of Residents during Virtual Learning in Comparison with That during In-Person Learning
3.2.4. Interactions between Residents and Instructors in Virtual Learning in Comparison to Those in In-Person Learning
3.2.5. Preferred Learning Format of Residents for Upcoming Years
3.3. Regulatory Focus Theory
3.4. Burnout Level among the Residents
4. Discussion
4.1. Factors Associated with Residents’ Perceptions of Virtual Learning
4.1.1. Residents Obtained Dental Degrees outside of the U.S./Canada
4.1.2. Years of Practice and Age
4.2. Faculty Perceptions
4.3. Regulatory Focus Types
4.4. Hybrid Learning Format
4.5. Burnout among Residents
4.6. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- 1
- Your gender
- 2
- Age
- 3
- Where did you receive your DDS/DMD?
- 4
- How long have you been practicing dentistry? Years
- 5
- Which residency program are you currently in?
- 6
- When will you graduate from your program at the EIOH?
- 1
- What device do you use the most for virtual learning?
- 2
- How do you feel overall about virtual learning education at EIOH AEGD?
| Courses | Poor | Below average | Average | Good | Excellent |
| (a) Didactic lectures | |||||
| (b) Research presentation | |||||
| (c) Case presentation | |||||
| (d) Literature review | |||||
| (e) Meetings |
- 3
- How effective has virtual learning been for you, comparing to in-person learning, for the following courses?
| Courses | Not at all effective | Less effective | Equally effective | More effective | Extremely effective |
| (a) Didactic lectures | |||||
| (b) Research presentation | |||||
| (c) Case presentation | |||||
| (d) Literature review | |||||
| (e) Meetings |
- 4
- How would you rate your engagement in virtual learning, comparing to in-person learning, for the following courses?
| Courses | Not at all engaged | Less engaged | Equally engaged | More engaged | Extremely engaged |
| (a) Didactic lectures | |||||
| (b) Research presentation | |||||
| (c) Case presentation | |||||
| (d) Literature review | |||||
| (e) Meetings |
- 5
- How would you rate your interactions with your co-residents and instructors during virtual learning, comparing to in-person learning, for the following courses?
| Courses | No interactions | Less interactions | Equal interactions | More interaction | Extremely more interactions |
| (a) Didactic lectures | |||||
| (b) Research presentation | |||||
| (c) Case presentation | |||||
| (d) Literature review | |||||
| (e) Meetings |
- 6
- In the coming year, what learning format would you prefer for the following courses?
| Courses | In-person | Virtual | Hybrid |
| (a) Didactic lectures | |||
| (b) Research presentation | |||
| (c) Case presentation | |||
| (d) Literature review | |||
| (e) Meetings |
- 7
- Do you have other comments for AEGD virtual learning?
| Please indicate next to each statement the extent to which each is true for you. Circle your response. | Definitely untrue | Not true | Probably not true | Neither true nor untrue | Probably true | True | Definitely true | |
| 1 | I prefer to work without instructions from others | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 2 | Rules and regulations are helpful and necessary for me | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 3 | For me, it is very important to carry out the obligations placed on me | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 4 | I generally solve problems creatively | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 5 | I'm not bothered about reviewing or checking things really closely | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 6 | I like to do things in a new way | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 7 | I always try to make my work as accurate and error free as possible | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 8 | I like trying out lots of different things, and am often successful in doing so | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 9 | It is important to me that my achievements are recognized and valued by other people | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| 10 | I often think about what other people expect of me | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
- A
- I enjoy work I have no symptoms of burnout.
- B
- Occasionally I am under stress and I don’t have as much energy as I once did, but I don’t feel burned out.
- C
- I am definitely burned out and have one or more symptoms of burnout, such as physical and emotional exhaustion.
- D
- The symptoms of burnout that I’m experiencing won’t go away. I think about frustration at work a lot.
- E
- I feel completely burned out and often wonder if I can go on. I am at the point where I made some changes or may need to seek some sort of help.
References
- Naciri, A.; Radid, M.; Kharbach, A.; Chemsi, G. E-learning in health professions education during the COVID-19 pandemic: A systematic review. J. Educ. Eval. Health Prof. 2021, 18, 27. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Karaca, O.; Cinarcik, B.S.; Asik, A.; Saglam, C.; Yigit, Y.; Hakverdi, G.; Yetkiner, A.A.; Ersin, N. Impact of fully online flipped classroom on academic achievement in undergraduate dental education: An experimental study. Eur. J. Dent. Educ. 2024, 28, 212–226. [Google Scholar] [CrossRef] [PubMed]
- Wilcha, R.J. Effectiveness of Virtual Medical Teaching During the COVID-19 Crisis: Systematic Review. JMIR Med. Educ. 2020, 6, e20963. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Larocque, N.; Shenoy-Bhangle, A.; Brook, A.; Eisenberg, R.; Chang, Y.M.; Mehta, P. Resident Experiences with Virtual Radiology Learning During the COVID-19 Pandemic. Acad. Radiol. 2021, 28, 704–710. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dost, S.; Hossain, A.; Shehab, M.; Abdelwahed, A.; Al-Nusair, L. Perceptions of medical students towards online teaching during the COVID-19 pandemic: A national cross-sectional survey of 2721 UK medical students. BMJ Open 2020, 10, e042378. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mheissen, S.; Almuzian, M.; Wertheimer, M.B.; Khan, H. Global survey to assess preferences when attending virtual orthodontic learning sessions: Optimising uptake from virtual lectures. Prog. Orthod. 2021, 22, 47. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Higgins, E.T.; Shah, J.; Friedman, R. Emotional responses to goal attainment: Strength of regulatory focus as moderator. J. Pers. Soc. Psychol. 1997, 72, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Cui, Y.; Wang, X.; Wang, J.; Du, K.; Luo, Z. Regulatory Focus, Motivation, and Their Relationship with Creativity Among Adolescents. Front. Psychol. 2021, 12, 666071. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, R.; Liu, H.; Yao, M.; Chen, Y. Regulatory Focus and Subjective Well-Being: The Mediating Role of Coping Styles and the Moderating Role of Gender. J. Psychol. 2019, 153, 714–731. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Shanafelt, T.D.; Sinsky, C.A.; Cipriano, P.F.; Bhatt, J.; Ommaya, A.; West, C.P.; Meyers, D. Burnout among Health Care Professionals: A Call to Explore and Address This Underrecognized Threat to Safe, High-Quality care. National Academy of Medicine. 2017. Available online: https://nam.edu/burnout-among-health-care-professionals-a-call-to-explore-and-address-this-underrecognized-threat-to-safe-high-quality-care/ (accessed on 20 March 2024).
- Shah, A.; Wyatt, M.; Gourneau, B.; Shih, G.; De Ruyter, M. Emotional exhaustion among anesthesia providers at a tertiary care center assessed using the MBI burnout survey. Psychol. Health Med. 2019, 24, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, F.; Noto, A.; Foresta, G.; Santonocito, C.; Palumbo, G.J.; Arcadipane, A.; Maybauer, D.M.; Maybauer, M.O. Incidence and Factors Associated with Burnout in Anesthesiology: A Systematic Review. Biomed. Res. Int. 2017, 2017, 8648925. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chi, D.L.; Randall, C.L.; Hill, C.M. Dental trainees’ mental health and intention to leave their programs during the COVID-19 pandemic. J. Am. Dent. Assoc. 2021, 152, 526–534. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kirkpatrick, H.; Wasfie, T.; Laykova, A.; Barber, K.; Hella, J.; Vogel, M. Emotional Intelligence, Burnout, and Wellbeing among Residents as a Result of the COVID-19 Pandemic. Am. Surg. 2022, 88, 1856–1860. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cevik, H.; Ungan, M. The impacts of the COVID-19 pandemic on the mental health and residency training of family medicine residents: Findings from a nationwide cross-sectional survey in Turkey. BMC Fam. Pract. 2021, 22, 226. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fellner, B.; Holler, M.; Kirchler, E.; Schabmann, A. Regulatory Focus Scale (RFS): Development of a scale to record dispositional regulatory focus. Swiss J. Psychol. Schweiz. Z. Für Psychol. Rev. Suisse Psychol. 2007, 66, 109–116. [Google Scholar] [CrossRef]
- Sanders, M.; Fiscella, K.; Hill, E.; Ogedegbe, O.; Cassells, A.; Tobin, J.N.; Williams, S.; Veazie, P. Motivation to move fast, motivation to wait and see: The association of prevention and promotion focus with clinicians’ implementation of the JNC-7 hypertension treatment guidelines. J. Clin. Hypertens. 2021, 23, 1752–1757. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Han, Y.; Chang, Y.; Kearney, E. “It’s Doable”: International Graduate Students’ Perceptions of Online Learning in the U.S. During the Pandemic. J. Stud. Int. Educ. 2022, 26, 165–182. [Google Scholar] [CrossRef] [PubMed]
- Hattar, S.; AlHadidi, A.; Sawair, F.A.; Alraheam, I.A.; El-Ma’aita, A.; Wahab, F.K. Impact of COVID-19 pandemic on dental education: Online experience and practice expectations among dental students at the University of Jordan. BMC Med. Educ. 2021, 21, 151. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jafar, K.; Ananthpur, K.; Venkatachalam, L. Digital divide and access to online education: New evidence from Tamil Nadu, India. J. Soc. Econ. Dev. 2023, 25, 313–333. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Al Achkar, M.; Dahal, A.; Frogner, B.K.; Skillman, S.M.; Patterson, D.G. Integrating Immigrant Health Professionals into the U.S. Healthcare Workforce: Barriers and Solutions. J. Immigr. Minor Health 2023, 25, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Tejedor, S.; Cervi, L.; Pérez-Escoda, A.; Jumbo, F.T. Digital Literacy and Higher Education during COVID-19 Lockdown: Spain, Italy, and Ecuador. Publications 2020, 8, 48. [Google Scholar] [CrossRef]
- Raby, C.L.; Madden, J.R. Moving academic conferences online: Understanding patterns of delegate engagement. Ecol. Evol. 2021, 11, 3607–3615. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kopec, K.T.; Stolbach, A. Transitioning to Virtual: ACMT’s 2020 Annual Scientific Meeting. J. Med. Toxicol. 2020, 16, 353–355. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cui, W.L.; Ye, M.L. An Introduction of Regulatory Focus Theory and Its Recently Related Researches. Psychology 2017, 8, 837–847. [Google Scholar] [CrossRef]
- Watling, C.; Driessen, E.; van der Vleuten, C.P.; Vanstone, M.; Lingard, L. Understanding responses to feedback: The potential and limitations of regulatory focus theory. Med. Educ. 2012, 46, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Steele, K.; Singh, L. Combining the Best of Online and Face-to-Face Learning: Hybrid and Blended Learning Approach for COVID-19, Post Vaccine, & Post-Pandemic World. J. Educ. Technol. Syst. 2021, 50, 140–171. [Google Scholar] [CrossRef]
- Vallee, A.; Blacher, J.; Cariou, A.; Sorbets, E. Blended Learning Compared to Traditional Learning in Medical Education: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e16504. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gong, L.; Song, Y.; Xu, Y.; Wang, M.; Ma, H.; Liu, W.; Zhu, L.; Li, J.; Luan, M.; Chu, W.; et al. The use of a technology-assisted and teacher-supervised online discussion platform to promote academic progress in blended embryology courses. BMC Med. Educ. 2022, 22, 817. [Google Scholar] [CrossRef]
- Aladwan, F.; Fakhouri, H.; Alawamrah, A.; Rababah, O. Students Attitudes toward Blended Learning among students of the University of Jordan. Mod. Appl. Sci. 2018, 12, 217. [Google Scholar] [CrossRef]
- McMurray, J.E.; Linzer, M.; Konrad, T.R.; Douglas, J.; Shugerman, R.; Nelson, K. The work lives of women physicians results from the physician work life study. The SGIM Career Satisfaction Study Group. J. Gen. Intern. Med. 2000, 15, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Templeton, K.C.; Bernstein, J.; Sukhera, L.M.; Nora, C.; Newman, H.; Burstin, C.; Guille, L.; Lynn, M.L.; Schwarze, S.S.; Busis, N. Gender-Based Differences in Burnout: Issues Faced by Women Physicians. National Academy of Medicine. 2019. Available online: https://nam.edu/gender-based-differences-in-burnout-issues-faced-by-women-physicians/ (accessed on 20 March 2024).
- Murphy, B. Why Do Women Resident Physicians Report More Burnout Listen up American Medical Association. 2023. Available online: https://www.ama-assn.org/medical-residents/medical-resident-wellness/why-do-women-resident-physicians-report-more-burnout#:~:text=One%20contributor%20to%20burnout%20among,to%20prove%20that%20you%20belong (accessed on 20 March 2024).
- Verweij, H.; van der Heijden, F.; van Hooff, M.L.M.; Prins, J.T.; Lagro-Janssen, A.L.M.; van Ravesteijn, H.; Speckens, A.E.M. The contribution of work characteristics, home characteristics and gender to burnout in medical residents. Adv. Health Sci. Educ. Theory Pract. 2017, 22, 803–818. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Norvell, J.; Unruh, G.; Norvell, T.; Templeton, K.J. Addressing Burnout Among Women Residents: Results from Focus Group Discussions. Kans J. Med. 2023, 16, 83–87. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
| Residents (n = 46) | Faculty (n = 10) | |
|---|---|---|
| Gender (female) | 41.40% (27) | 30% (3) |
| Age group (year) | ||
| 20–30 | 21.7% (10) | 0 |
| 31–40 | 43.50% (20) | 10% (1) |
| 41–50 | 34.80% (16) | 40% (4) |
| 51–60 | 0 | 0 |
| >60 | 0 | 50% (5) |
| Dental school | ||
| U.S./Canada | 17.40% (8) | 40% (4) |
| Outside U.S./Canada | 82.60% (38) | 60% (6) |
| Program enrolled | ||
| 1-yr AEGD | 15.20% (7) | |
| 2-yr AEGD | 39.10% (18) | |
| 3-yr AEGD + MS | 37.00% (17) | |
| 4-yr AEGD + MS | 8.70% (4) | |
| Program graduation (year) | ||
| 2021 | 47.80% (22) | |
| 2022 | 26.10% (12) | |
| 2023 | 19.60% (9) | |
| 2024 | 6.50% (3) | |
| Device used | ||
| Desktop | 97.80% (45) | 30% (3) |
| Laptop | 2.20% (1) | 60% (6) |
| Tablet | 0 | 0 |
| Smartphone | 0 | 10% (1) |
| Odds Ratio [95% Confidence Interval] | p-Value | |
|---|---|---|
| Overall feelings about virtual learning | ||
| Case presentation | ||
| Years of Practice | 0.80 [0.65,0.97] | 0.027 * |
| Literature review | ||
| Years of Practice | 0.85 [0.72, 0.99] | 0.047 * |
| Effectiveness of virtual learning | ||
| Didactic lectures | ||
| Dental degree Received Outside U.S./Canada (Yes vs. No) | 0.07 [0.007, 0.65] | 0.020 * |
| Case presentation | ||
| Age group (31–40 yrs vs. 20–30 yrs) | 0.08 [0.01, 0.68] | 0.021 * |
| Literature review | ||
| Age group (31–40 yrs vs. 20–30 yrs) | 0.14 [0.02, 0.93] | 0.041 * |
| Future preferred learning format | ||
| Literature review | ||
| Dental Degree Received Outside U.S./Canada (Yes vs. No) | 12.04 [1.04, 139.5] | 0.047 * |
| Overall Burnout level | ||
| Gender (Female vs. Male) | 3.8 [1.03, 13.7] | 0.044 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, S.; Kar, K.S.; Vasani, S.; Al Jallad, N.; Sanders, M.R.; Cacciato, R.; Wu, T.T.; Xiao, J.; Malmstrom, H. Perception of Virtual Education Learning among Dental Residents and Faculty during the COVID-19 Pandemic: A Cross-Sectional Study. Dent. J. 2024, 12, 231. https://doi.org/10.3390/dj12080231
Cui S, Kar KS, Vasani S, Al Jallad N, Sanders MR, Cacciato R, Wu TT, Xiao J, Malmstrom H. Perception of Virtual Education Learning among Dental Residents and Faculty during the COVID-19 Pandemic: A Cross-Sectional Study. Dentistry Journal. 2024; 12(8):231. https://doi.org/10.3390/dj12080231
Chicago/Turabian StyleCui, Shasha, Kumari Saswati Kar, Shruti Vasani, Nisreen Al Jallad, Mechelle R. Sanders, Rita Cacciato, Tong Tong Wu, Jin Xiao, and Hans Malmstrom. 2024. "Perception of Virtual Education Learning among Dental Residents and Faculty during the COVID-19 Pandemic: A Cross-Sectional Study" Dentistry Journal 12, no. 8: 231. https://doi.org/10.3390/dj12080231
APA StyleCui, S., Kar, K. S., Vasani, S., Al Jallad, N., Sanders, M. R., Cacciato, R., Wu, T. T., Xiao, J., & Malmstrom, H. (2024). Perception of Virtual Education Learning among Dental Residents and Faculty during the COVID-19 Pandemic: A Cross-Sectional Study. Dentistry Journal, 12(8), 231. https://doi.org/10.3390/dj12080231