
Asymmetric Dimethylarginine as a Potential Mediator in the Association between Periodontitis and Cardiovascular Disease: A Systematic Review of Current Evidence

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
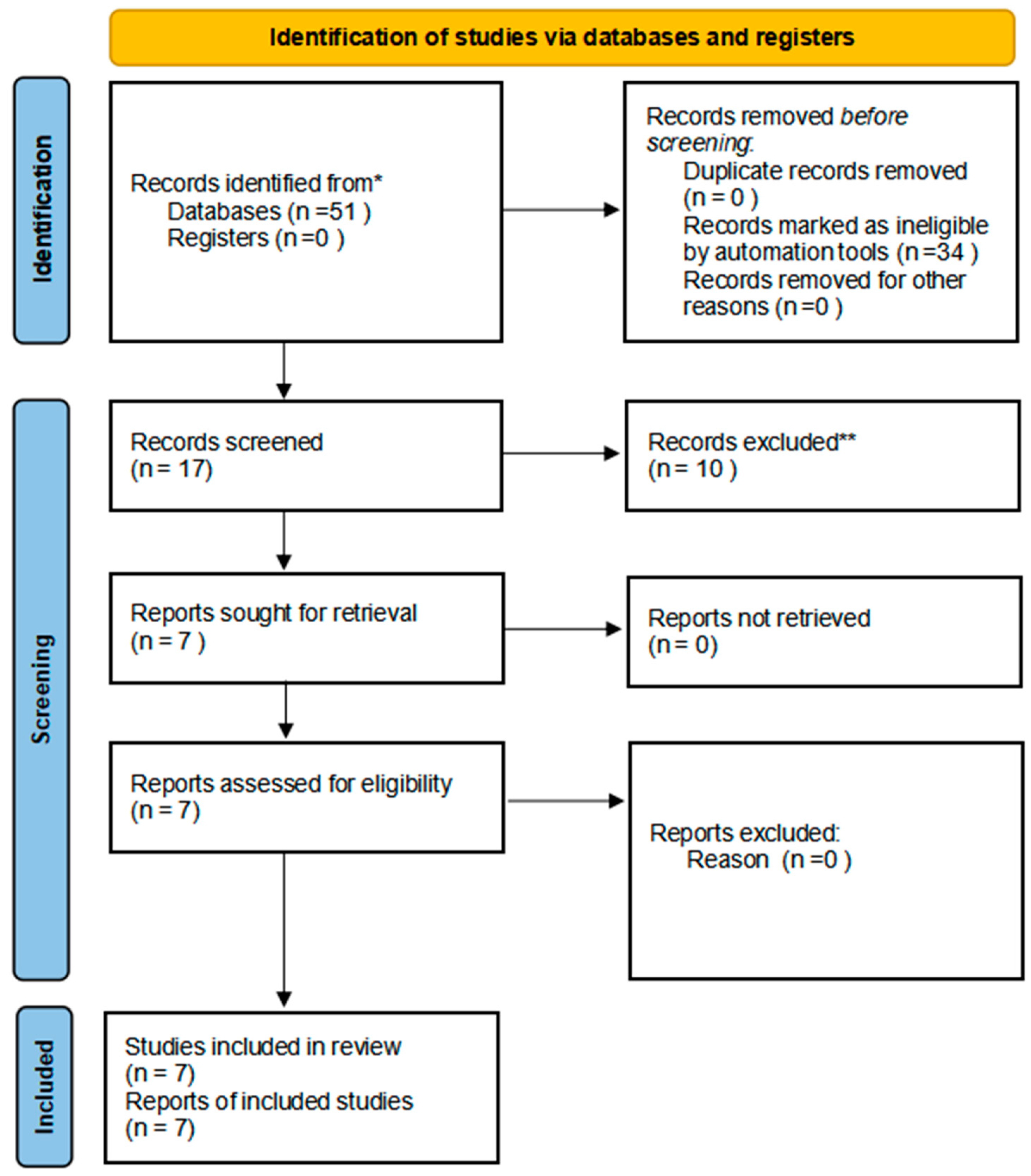
2.1. Search Strategy and Selection Criteria
- Original research articles published in English;
- Studies investigating the relationship between ADMA, periodontitis, and/or cardiovascular disease;
- Studies reporting ADMA levels in patients with periodontitis and/or cardiovascular disease;
- Studies assessing the impact of periodontal treatment on ADMA levels or endothelial function.
- Review articles, case reports, editorials, and conference abstracts;
- Animal or in vitro studies;
- Studies not reporting ADMA levels or endothelial function outcomes.
2.2. Study Selection and Data Extraction
2.3. Quality Assessment
- Clarity and specificity of the research question
- Representativeness of the study sample
- Reliability and validity of the methods used to measure exposures and outcomes
- Appropriateness of statistical analyses
- Consideration and handling of potential confounding variables
2.4. Data Synthesis and Analysis
3. Results
Quality Assessment Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef] [PubMed]
- Tsioufis, C.; Thomopoulos, C.; Soldatos, N.; Syrseloudis, D.; Kasiakogias, A.; Silvestros, S.; Stefanadi, E.; Mostratou, E.; Stefanadis, C. The conjoint detrimental effect of chronic periodontal disease and systemic inflammation on asymmetric dimethyl-arginine in untreated hypertensive subjects. Atherosclerosis 2010, 208, 258–263. [Google Scholar] [CrossRef]
- De Nardin, E. The role of inflammatory and immunological mediators in periodontitis and cardiovascular disease. Ann. Periodontol. 2001, 6, 30–40. [Google Scholar] [CrossRef]
- Suzuki, J.; Aoyama, N.; Ogawa, M.; Hirata, Y.; Izumi, Y.; Nagai, R.; Isobe, M. Periodontitis and cardiovascular diseases. Expert Opin. Ther. Targets 2010, 14, 1023–1027. [Google Scholar] [CrossRef]
- Higashi, Y.; Goto, C.; Hidaka, T.; Soga, J.; Nakamura, S.; Fujii, Y.; Hata, T.; Idei, N.; Fujimura, N.; Chayama, K.; et al. Oral infection-inflammatory pathway, periodontitis, is a risk factor for endothelial dysfunction in patients with coronary artery disease. Atherosclerosis 2009, 206, 604–610. [Google Scholar] [CrossRef]
- Seinost, G.; Wimmer, G.; Skerget, M.; Thaller, E.; Brodmann, M.; Gasser, R.; Bratschko, R.O.; Pilger, E. Periodontal treatment improves endothelial dysfunction in patients with severe periodontitis. Am. Heart J. 2005, 149, 1050–1054. [Google Scholar] [CrossRef]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Suvan, J.; Hingorani, A.D.; Vallance, P.; Deanfield, J. Treatment of periodontitis and endothelial function. N. Engl. J. Med. 2007, 356, 911–920, Erratum in N. Engl. J. Med. 2018, 378, 2450. [Google Scholar] [CrossRef]
- Chauhan, N.; Mittal, S.; Tewari, S.; Sen, J.; Laller, K. Association of Apical Periodontitis with Cardiovascular Disease via Noninvasive Assessment of Endothelial Function and Subclinical Atherosclerosis. J. Endod. 2019, 45, 681–690. [Google Scholar] [CrossRef]
- Sibal, L.; Agarwal, S.C.; Home, P.D.; Boger, R.H. The Role of Asymmetric Dimethylarginine (ADMA) in Endothelial Dysfunction and Cardiovascular Disease. Curr. Cardiol. Rev. 2010, 6, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Landim, M.B.; Casella Filho, A.; Chagas, A.C. Asymmetric dimethylarginine (ADMA) and endothelial dysfunction: Implications for atherogenesis. Clinics 2009, 64, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.N.; Chan, J.C. Asymmetric dimethylarginine (ADMA): A potential link between endothelial dysfunction and cardiovascular diseases in insulin resistance syndrome? Diabetologia 2002, 45, 1609–1616. [Google Scholar] [PubMed]
- Maas, R.; Quitzau, K.; Schwedhelm, E.; Spieker, L.; Rafflenbeul, W.; Steenpass, A.; Lüscher, T.F.; Böger, R.H. Asymmetrical dimethylarginine (ADMA) and coronary endothelial function in patients with coronary artery disease and mild hypercholesterolemia. Atherosclerosis 2007, 191, 211–219. [Google Scholar] [CrossRef]
- Cooke, J.P. Does ADMA cause endothelial dysfunction? Arterioscler. Thromb. Vasc. Biol. 2000, 20, 2032–2037. [Google Scholar] [CrossRef] [PubMed]
- Böger, R.H. Asymmetric dimethylarginine (ADMA) and cardiovascular disease: Insights from prospective clinical trials. Vasc. Med. 2005, 10, S19–S25. [Google Scholar] [CrossRef]
- Cooke, J.P. ADMA: Its role in vascular disease. Vasc. Med. 2005, 10, S11–S17. [Google Scholar] [CrossRef]
- Böger, R.H. When the endothelium cannot say ‘NO’anymore: ADMA, an endogenous inhibitor of NO synthase, promotes cardiovascular disease. Eur. Heart J. 2003, 24, 1901–1902. [Google Scholar] [CrossRef]
- Sydow, K.; Hornig, B.; Arakawa, N.; Bode-Böger, S.M.; Tsikas, D.; Münzel, T.; Böger, R.H. Endothelial dysfunction in patients with peripheral arterial disease and chronic hyperhomocysteinemia: Potential role of ADMA. Vasc. Med. 2004, 9, 93–101. [Google Scholar] [CrossRef]
- Bermúdez, V.; Bermúdez, F.; Acosta, G.; Acosta, A.; Añez, J.; Andara, C.; Leal, E.; Cano, C.; Manuel, V.; Hernández, R.; et al. Molecular mechanisms of endothelial dysfunction: From nitric oxide synthesis to ADMA inhibition. Am. J. Ther. 2008, 15, 326–333. [Google Scholar] [CrossRef]
- Franceschelli, S.; Ferrone, A.; Pesce, M.; Riccioni, G.; Speranza, L. Biological functional relevance of asymmetric dimethylarginine (ADMA) in cardiovascular disease. Int. J. Mol. Sci. 2013, 14, 24412–24421. [Google Scholar] [CrossRef] [PubMed]
- Sydow, K.; Schwedhelm, E.; Arakawa, N.; Bode-Böger, S.M.; Tsikas, D.; Hornig, B.; Frölich, J.C.; Böger, R.H. ADMA and oxidative stress are responsible for endothelial dysfunction in hyperhomocyst(e)inemia: Effects of L-arginine and B vitamins. Cardiovasc. Res. 2003, 57, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Krzyzanowska, K.; Mittermayer, F.; Wolzt, M.; Schernthaner, G. ADMA, cardiovascular disease and diabetes. Diabetes Res. Clin. Pract. 2008, 82, S122–S126. [Google Scholar] [CrossRef] [PubMed]
- Sydow, K.; Münzel, T. ADMA and oxidative stress. Atheroscler. Suppl. 2003, 4, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Xu, X.; Shang, R.; Chen, Y. Asymmetric dimethylarginine (ADMA) as an important risk factor for the increased cardiovascular diseases and heart failure in chronic kidney disease. Nitric Oxide 2018, 78, 113–120. [Google Scholar] [CrossRef]
- Yilmaz, M.I.; Sonmez, A.; Saglam, M.; Qureshi, A.R.; Carrero, J.J.; Caglar, K.; Eyileten, T.; Cakir, E.; Oguz, Y.; Vural, A.; et al. ADMA levels correlate with proteinuria, secondary amyloidosis, and endothelial dysfunction. J. Am. Soc. Nephrol. 2008, 19, 388–395. [Google Scholar] [CrossRef]
- Avci, E.; Karabulut, A.; Alp, A.G.; Baba, B.; Bilgi, C. Crucial markers showing the risk of coronary artery disease in obesity: ADMA and neopterin. J. Med. Biochem. 2020, 39, 452–459. [Google Scholar] [CrossRef]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Military Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef]
- Şengül, V.; Güney, Z.; Kurgan, Ş.; Önder, C.; Serdar, M.A.; Günhan, M. Evaluation of salivary and serum methylated arginine metabolites and nitric oxide synthase in advanced periodontitis patients. Clin. Oral. Investig. 2022, 26, 5061–5070. [Google Scholar] [CrossRef]
- Al-Abdulla, N.; Bakhsh, A.; Mannocci, F.; Proctor, G.; Moyes, D.; Niazi, S.A. Successful endodontic treatment reduces serum levels of cardiovascular disease risk biomarkers-high-sensitivity C-reactive protein, asymmetric dimethylarginine, and matrix metalloprotease-2. Int. Endod. J. 2023, 56, 1499–1516. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Qorri, E.; Dipalma, G.; Mancini, A.; Corsalini, M.; Fabbro, M.D.; Scarano, A.; Tartaglia, G.M.; Inchingolo, F. The Impact of Periodontal Inflammation on Endothelial Function Assessed by Circulating Levels of Asymmetric Dimethylarginine: A Single-Blinded Randomized Clinical Trial. J. Clin. Med. 2022, 11, 4173. [Google Scholar] [CrossRef] [PubMed]
- Ferlazzo, N.; Currò, M.; Isola, G.; Maggio, S.; Bertuccio, M.P.; Trovato-Salinaro, A.; Matarese, G.; Alibrandi, A.; Caccamo, D.; Ientile, R. Changes in the Biomarkers of Oxidative/Nitrosative Stress and Endothelial Dysfunction Are Associated with Cardiovascular Risk in Periodontitis Patients. Curr. Issues Mol. Biol. 2021, 43, 704–715. [Google Scholar] [CrossRef] [PubMed]
- Okada, A.; Murata, T.; Matin, K.; Ariyoshi, M.; Otsuka, R.; Yamashita, M.; Suzuki, M.; Wakiyama, R.; Tateno, K.; Suzuki, M.; et al. Effect of advanced periodontal self-care in patients with early-stage periodontal diseases on endothelial function: An open-label, randomized controlled trial. PLoS ONE 2021, 16, e0257247. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Alibrandi, A.; Currò, M.; Matarese, M.; Ricca, S.; Matarese, G.; Ientile, R.; Kocher, T. Evaluation of salivary and serum asymmetric dimethylarginine (ADMA) levels in patients with periodontal and cardiovascular disease as subclinical marker of cardiovascular risk. J. Periodontol. 2020, 91, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Almeida, S.; Figueredo, C.M.; Lemos, C.; Bregman, R.; Fischer, R.G. Periodontal treatment in patients with chronic kidney disease: A pilot study. J. Periodontal Res. 2017, 52, 262–267. [Google Scholar] [CrossRef]
- Pardo, A.; Signoriello, A.; Signoretto, C.; Messina, E.; Carelli, M.; Tessari, M.; De Manna, N.D.; Rossetti, C.; Albanese, M.; Lombardo, G.; et al. Detection of Periodontal Pathogens in Oral Samples and Cardiac Specimens in Patients Undergoing Aortic Valve Replacement: A Pilot Study. J. Clin. Med. 2021, 10, 3874. [Google Scholar] [CrossRef]

{kind=link}
| Component | Description |
|---|---|
| Population | Adult patients with periodontitis and/or cardiovascular diseases |
| Intervention/Exposure | Presence of periodontitis or periodontal treatment |
| Comparison | Absence of periodontitis or no periodontal treatment |
| Outcome | ADMA levels and/or endothelial function |
| Study | Study Design | Population | Methods | Key Findings |
|---|---|---|---|---|
| Şengül et al. [29] | Cross-sectional | The study included two groups: individuals diagnosed with advanced generalized periodontitis (Stage III Grade B, according to the current classification) and a control group of periodontally healthy subjects. | The researchers assessed various periodontal clinical indicators and conducted analyses of both saliva and blood samples. The analysis examined a range of compounds crucial for inflammation, endothelial function, and nitric oxide production. Among these, arginine and its methylated derivatives—asymmetric dimethylarginine (ADMA), symmetric dimethylarginine (SDMA), N-monomethyl-L-arginine (L-NMMA), and homoarginine (homoArg)—play key roles in vascular regulation. Additionally, nitric oxide synthase (NOS), the enzyme responsible for nitric oxide synthesis, and interleukin-6 (IL-6), an important inflammatory mediator, were evaluated. | The analysis revealed that patients with periodontitis exhibited significantly elevated concentrations of nitric oxide synthase (NOS), asymmetric dimethylarginine (ADMA), and arginine in their saliva compared to the control group. |
| Ferlazzo et al. [30] | Cross-sectional | The study encompassed four distinct groups: individuals diagnosed with periodontitis (PT), subjects with confirmed coronary heart disease (CHD), patients presenting with both conditions simultaneously (PT+CHD), and a cohort of healthy participants serving as controls. | A comprehensive analysis of blood samples, focusing on several key components: plasma concentrations of coenzyme Q10 (CoQ10), nitrotyrosine (NT), and asymmetric dimethylarginine (ADMA). Additionally, the researchers examined the expression levels of genes associated with inflammation in peripheral blood mononuclear cells (PBMCs) by quantifying their messenger RNA (mRNA). | PT+CHD patients had significantly lower CoQ10, higher NT, and higher ADMA levels compared to controls; inflammatory gene expression upregulated in PT, CHD, and PT+CHD groups. |
| Isola et al. [31] | Cross-sectional | Individuals diagnosed with chronic periodontitis (CP), subjects with confirmed coronary heart disease (CHD), patients presenting with both conditions concurrently (CP+CHD), and a cohort of healthy participants serving as controls. | The study protocol involved a comprehensive assessment of clinical and periodontal characteristics. Additionally, biological samples, including both serum and saliva, were collected from all participants. These samples were subsequently analyzed to quantify the levels of asymmetric dimethylarginine (ADMA) and high-sensitivity C-reactive protein (hs-CRP). | The analysis revealed that subjects with coronary heart disease, both with and without concurrent chronic periodontitis, exhibited significantly elevated concentrations of ADMA in both salivary and serum samples. The concentrations detected in these groups significantly exceeded those found in both the healthy control subjects and individuals diagnosed solely with chronic periodontitis. |
| Al-Abdulla et al. [32] | Prospective cohort (2-year follow-up) | Patients who had received one of two types of endodontic interventions: either a non-surgical revision of previous root canal therapy or a surgical procedure addressing periapical lesions. | A comprehensive assessment included multiple parameters: the condition of periapical tissues, measured systemic blood pressure, and analyzed blood samples for glycated hemoglobin (HbA1c) and lipid profiles. Additionally, the researchers quantified the serum levels of specific inflammatory markers, including high-sensitivity C-reactive protein (hs-CRP), asymmetric dimethylarginine (ADMA), and matrix metalloproteinase-2 (MMP-2). | Serum levels of hs-CRP, ADMA, MMP-2, HbA1C, and lipid levels were significantly reduced at 2 years compared to pre-operative levels. The analysis of blood samples taken two years post-intervention revealed a significant decrease in several key biomarkers compared to their pre-operative values. Specifically, the researchers observed marked reductions in serum concentrations of high-sensitivity C-reactive protein (hs-CRP), asymmetric dimethylarginine (ADMA), and matrix metalloproteinase-2 (MMP-2). Additionally, glycated hemoglobin (HbA1c) levels and various lipid parameters showed substantial improvements over the two-year period. |
| Rapone et al. [33] | Randomized controlled trial (6-month follow-up) | Individuals diagnosed with advanced periodontal disease who had no history of cardiovascular disease (CVD) or presence of traditional CVD risk factors. | The study protocol included comprehensive evaluations at three time points: before treatment, and at three- and six-months post-intervention. These assessments encompassed a thorough medical examination, detailed periodontal clinical measurements, laboratory quantification of asymmetric dimethylarginine (ADMA) levels, and ultrasonographic evaluation of flow-mediated dilation (FMD). | Following intensive periodontal therapy, the researchers found no statistically significant alterations in ADMA concentrations. However, the group receiving the intervention demonstrated an improvement in flow-mediated dilation, suggesting enhanced endothelial function. |
| Okada et al. [34] | Randomized controlled trial (3-month follow-up) | Individuals diagnosed with incipient periodontal disease, representing the early stages of the condition. | Assessments of flow-mediated dilation (FMD) and serum asymmetric dimethylarginine (ADMA) concentrations. These measurements were conducted at the initiation of the study and again after a three-month interval. | Despite observed improvements in clinical periodontal parameters, the analysis revealed no statistically significant changes in either flow-mediated dilation or serum ADMA levels in any of the study groups at the three-month follow-up evaluation. |
| Almeida et al. [35] | Pilot cohort | Individuals diagnosed with advanced chronic periodontitis who were also in the pre-dialysis stage of chronic kidney disease. | The study protocol included a comprehensive assessment of multiple parameters at three distinct time points: before treatment, and at 90 and 180 days following periodontal intervention. The evaluated measures encompassed periodontal clinical indicators, estimated glomerular filtration rate (eGFR), various metabolic markers, and serum asymmetric dimethylarginine (ADMA) concentrations. | Six months following periodontal therapy, the analysis revealed significant positive changes across several parameters. The researchers observed marked improvements in periodontal clinical indicators, a notable increase in estimated glomerular filtration rate, and a substantial reduction in serum ADMA levels. |
| Study | Study Design | Quality Rating | Risk of Bias |
|---|---|---|---|
| Şengül et al. [29] | Cross-sectional | Good | Low |
| Ferlazzo et al. [30] | Cross-sectional | Good | Low |
| Isola et al. [31] | Cross-sectional | Good | Low |
| Al-Abdulla et al. [32] | Prospective cohort | Good | Low |
| Rapone et al. [33] | Randomized controlled trial | Good | Low |
| Okada et al. [34] | Randomized controlled trial | Fair | Moderate |
| Almeida et al. [35] | Pilot cohort | Fair | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rapone, B.; Inchingolo, F.; Tartaglia, G.M., Jr.; De Francesco, M.; Ferrara, E. Asymmetric Dimethylarginine as a Potential Mediator in the Association between Periodontitis and Cardiovascular Disease: A Systematic Review of Current Evidence. Dent. J. 2024, 12, 297. https://doi.org/10.3390/dj12090297
Rapone B, Inchingolo F, Tartaglia GM Jr., De Francesco M, Ferrara E. Asymmetric Dimethylarginine as a Potential Mediator in the Association between Periodontitis and Cardiovascular Disease: A Systematic Review of Current Evidence. Dentistry Journal. 2024; 12(9):297. https://doi.org/10.3390/dj12090297
Chicago/Turabian StyleRapone, Biagio, Francesco Inchingolo, Giulia Margherita Tartaglia, Jr., Maurizio De Francesco, and Elisabetta Ferrara. 2024. "Asymmetric Dimethylarginine as a Potential Mediator in the Association between Periodontitis and Cardiovascular Disease: A Systematic Review of Current Evidence" Dentistry Journal 12, no. 9: 297. https://doi.org/10.3390/dj12090297
APA StyleRapone, B., Inchingolo, F., Tartaglia, G. M., Jr., De Francesco, M., & Ferrara, E. (2024). Asymmetric Dimethylarginine as a Potential Mediator in the Association between Periodontitis and Cardiovascular Disease: A Systematic Review of Current Evidence. Dentistry Journal, 12(9), 297. https://doi.org/10.3390/dj12090297