

Effect of Pomegranate Extract Consumption on Satiety Parameters in Healthy Volunteers: A Preliminary Randomized Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Pomegranate Extract and Placebo Capsules
2.4. Satiety Session: Breakfast and Lunch Meals
2.5. Study Procedures
2.6. Food and Drink Diaries
2.7. Statistical Analysis
3. Results
3.1. Study Population
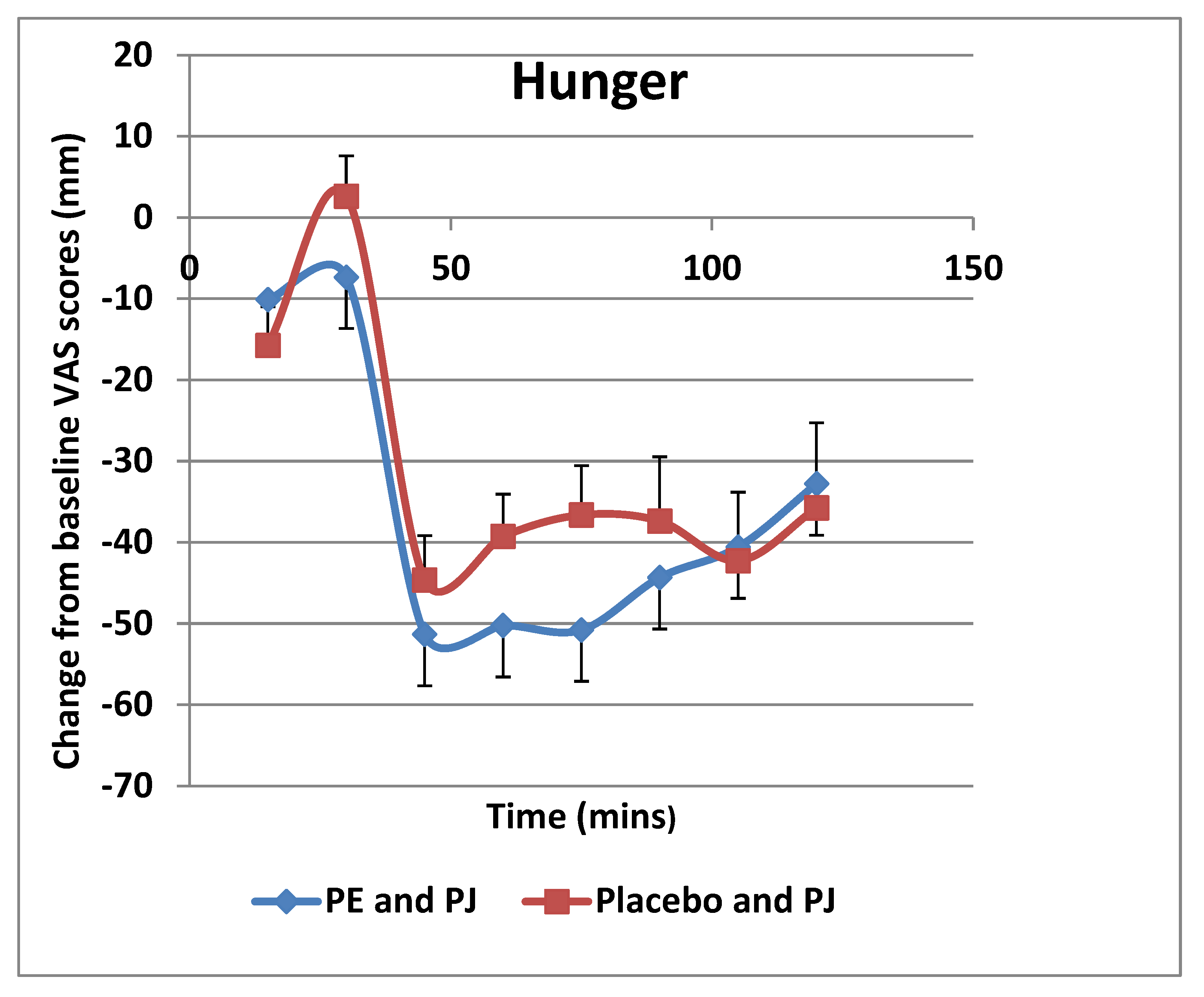
3.2. Satiety-Related Variables
3.3. Meal Quality
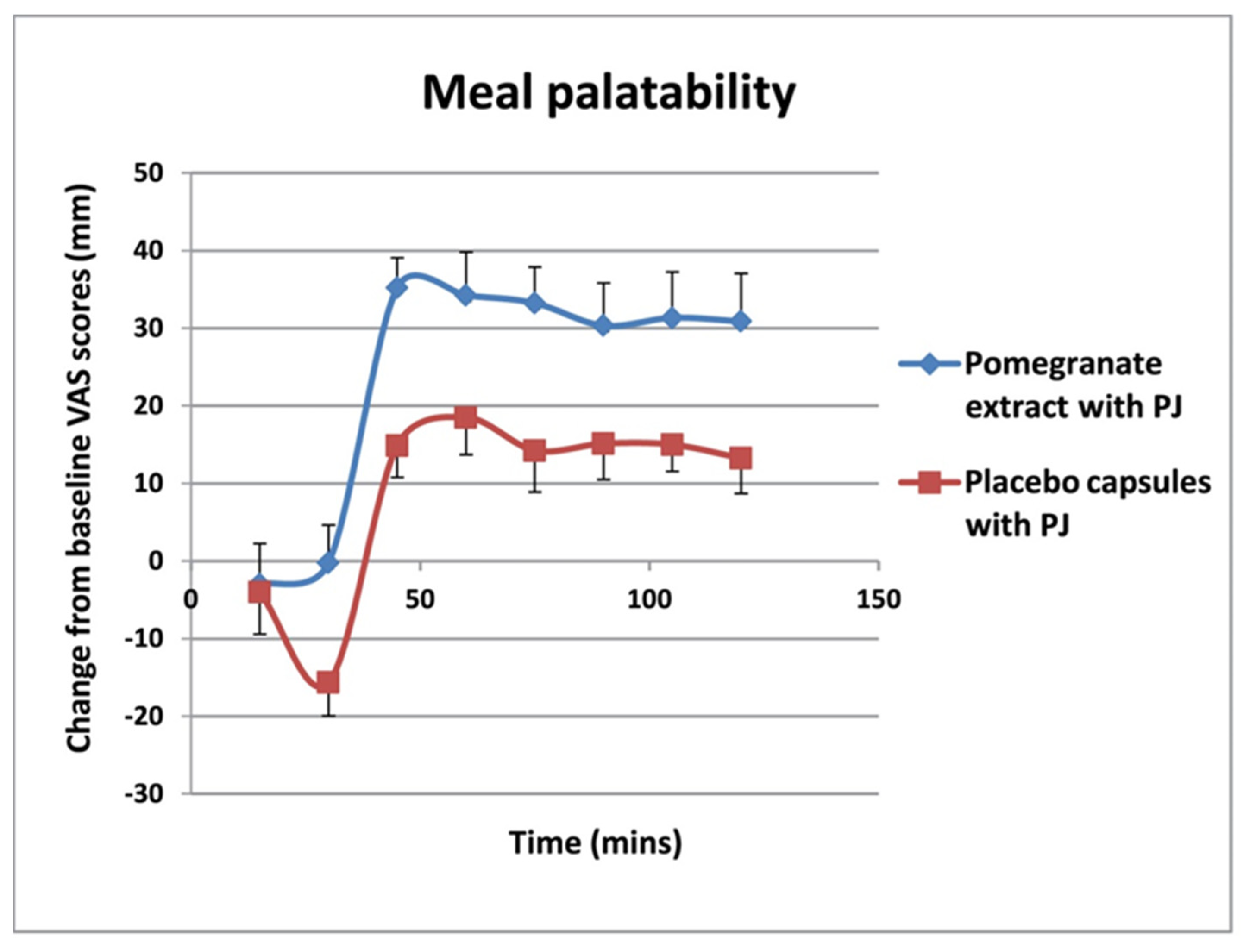
3.4. Meal Palatability
3.5. Meal Food Consumption
3.6. Food and Drink Diaries
4. Discussion
4.1. Methodology and Compliance
4.2. Satiety Mechanisms
4.3. Food Consumption
4.4. Limitations and Future Directions
4.5. Critical Issues
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gho, J.M.; Postema, P.G.; Conijn, M.; Bruinsma, N.; de Jong, J.S.; Bezzina, C.R.; Wilde, A.A.; Asselbergs, F.W. Heart failure following STEMI: A contemporary cohort study of incidence and prognostic factors. Open Heart 2017, 4, e000551. [Google Scholar] [CrossRef] [PubMed]
- WHO. Obesity and Overweight; The World Health Organization: Geneva, Switzerland, 2021; Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 26 August 2017).
- Halford, J.C.; Harrold, J.A. Satiety-enhancing products for appetite control: Science and regulation of functional foods for weight management. Proc. Nutr. Soc. 2012, 71, 350–362. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, M.R.; Chambers, L. Satiety-relevant sensory qualities enhance the satiating effects of mixed carbohydrate-protein preloads. Am. J. Clin. Nutr. 2011, 94, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.G.; Bloom, S.R. Gut hormones and the regulation of energy homeostasis. Nature 2006, 444, 854–859. [Google Scholar] [CrossRef]
- Drapeau, V.; King, N.; Hetherington, M.; Doucet, E.; Blundell, J.; Tremblay, A. Appetite sensations and satiety quotient: Predictors of energy intake and weight loss. Appetite 2007, 48, 159–166. [Google Scholar] [CrossRef]
- Parra, D.; Ramelb, A.; Bandarra, N.; Kielyd, M.; Martínez, J.A.; Thorsdottirb, I. A diet rich in long chain omega-3 fatty acids modulates satiety in overweight and obese volunteers during weight loss. Appetite 2008, 51, 676–680. [Google Scholar] [CrossRef]
- Blundell, J. Making claims: Functional foods for managing appetite and weight. Nat. Rev. Endocrinol. 2010, 6, 53–56. [Google Scholar] [CrossRef]
- Stubbs, J.; Whybrow, S.; Lavin, J. Dietary and Lifestyle measures to enhance satiety and weight control. Nutr. Bull. 2010, 35, 113–125. [Google Scholar] [CrossRef]
- Clegg, M.; Shafat, A. Energy and macronutrient composition of breakfast affect gastric emptying of lunch and subsequent food intake, satiety and satiation. Appetite 2010, 54, 517–523. [Google Scholar] [CrossRef]
- de Graaf, C.; Blom, W.A.; Smeets, P.A.; Stafleu, A.; Hendriks, H.F. Biomarkers of satiation and satiety. Am. J. Clin. Nutr. 2004, 79, 946–961. [Google Scholar] [CrossRef] [Green Version]
- Dansinger, M.L.; Gleason, J.A.; Griffith, J.L.; Selker, H.P.; Schaefer, E.J. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: A randomized trial. JAMA 2005, 293, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Sadoul, B.C.; Schuring, E.A.; Symersky, T.; Mela, D.J.; Masclee, A.A.; Peters, H.P. Measuring satiety with pictures compared to visual analogue scales. An exploratory study. Appetite 2012, 58, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Ahima, R.S.; Antwi, D.A. Brain regulation of appetite and satiety. Endocrinol. Metab. Clin. N. Am. 2008, 37, 811–823. [Google Scholar] [CrossRef] [PubMed]
- Benelam, B. Satiation, satiety and their effects on eating behaviour. Nutr. Bull. 2009, 34, 126–173. [Google Scholar] [CrossRef]
- Meydani, M.; Syeda, T.H. Dietary polyphenols and obesity. Nutrients 2010, 2, 737–751. [Google Scholar] [CrossRef]
- Singh, M.; Thrimawithana, T.; Shukla, R.; Adhikari, B. Managing obesity through natural polyphenols: A review. Future Foods 2020, 1–2, 100002. [Google Scholar] [CrossRef]
- Lai, C.S.; Tsai, M.L.; Badmaev, V.; Jimenez, M.; Ho, C.T.; Pan, M.H. Xanthigen suppresses preadipocyte differentiation and adipogenesis through down-regulation of PPARγ and C/EBPs and modulation of SIRT-1, AMPK, and FoxO pathways. J. Agric. Food Chem. 2012, 60, 1094–1101. [Google Scholar] [CrossRef]
- Gil, M.I.; Tomás-Barberán, F.A.; Hess-Pierce, B.; Holcroft, D.M.; Kader, A.A. Antioxidant activity of pomegranate juice and its relationship with phenolic composition and processing. J. Agric. Food Chem. 2000, 48, 4581–4589. [Google Scholar] [CrossRef]
- Danesi, F.; Ferguson, L.R. Could Pomegranate Juice Help in the Control of Inflammatory Diseases? Nutrients 2017, 9, 958. [Google Scholar] [CrossRef]
- Kaplan, M.; Hayek, T.; Raz, A.; Coleman, R.; Dornfeld, L.; Vaya, J.; Aviram, M. Pomegranate juice supplementation to atherosclerotic mice reduces macrophage lipid peroxidation, cellular cholesterol accumulation and development of atherosclerosis. J. Nutr. 2001, 131, 2082–2089. [Google Scholar] [CrossRef] [Green Version]
- Aviram, M.; Volkova, N.; Coleman, R.; Dreher, M.; Reddy, M.K.; Ferreira, D.; Rosenblat, M. Pomegranate phenolics from the peels, arils, and flowers are antiatherogenic: Studies in vivo in atherosclerotic apolipoprotein E-deficient (E0) mice and in vitro in cultured macrophages and lipoproteins. J. Agric. Food Chem. 2008, 56, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Dujaili, A.I.; Good, G.; Tsang, C. Consumption of Pomegranate Juice Attenuates Exercise - Induced Oxidative Stress, Blood Pressure and Urinary Cortisol/Cortisone Ratio in Human Adults. EC Nutr. 2016, 4.6, 982–995. [Google Scholar]
- McFarlin, B.K.; Strohacker, K.A.; Kueht, M.L. Pomegranate seed oil consumption during a period of high-fat feeding reduces weight gain and reduces type 2 diabetes risk in CD-1 mice. Br. J. Nutr. 2009, 102, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Al-Muammar, M.N.; Khan, F. Obesity: The preventive role of the pomegranate (Punica granatum). Nutrition 2012, 28, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Tsang, C.; Smail, N.F.; Almoosawi, S.; Davidson, I.; Al-Dujaili, E.A. Intake of polyphenol-rich pomegranate pure juice influences urinary glucocorticoids, blood pressure and homeostasis model assessment of insulin resistance in human volunteers. J. Nutr. Sci. 2012, 1, e9. [Google Scholar] [CrossRef]
- Al-Dujaili, E.A.S. Functional Foods need more Mechanistic Studies. EC Nutr. 2016, 4.1, 770–771. [Google Scholar]
- Stockton, A.; Al-Dujaili, E.; McDougall, G.; Davidson, I.; Drummond, S.; Wyness, L. Effect of Pomegranate Extract Consumption on Cardiovascular Disease Risk Factors, Stress Hormones, and Quality of Life in Human Volunteers: An Exploratory Randomised, Double-Blind, Placebo-Controlled Trial. EC Nutr. 2015, 2, 396–411. [Google Scholar]
- Cerdá, B.; Cerón, J.J.; Tomás-Barberán, F.A.; Espín, J.C. Repeated oral administration of high doses of the pomegranate ellagitannin punicalagin to rats for 37 days is not toxic. J. Agric. Food Chem. 2003, 51, 3493–3501. [Google Scholar] [CrossRef]
- Lei, F.; Zhang, X.N.; Wang, W.; Xing, D.M.; Xie, W.D.; Su, H.; Du, L.J. Evidence of anti-obesity effects of the pomegranate leaf extract in high-fat diet induced obese mice. Int. J. Obes. 2007, 31, 1023–1029. [Google Scholar] [CrossRef]
- González-Ortiz, M.; Martínez-Abundis, E.; Espinel-Bermúdez, M.C.; Pérez-Rubio, K.G. Effect of pomegranate juice on insulin secretion and sensitivity in patients with obesity. Ann. Nutr. Metab. 2011, 58, 220–223. [Google Scholar] [CrossRef]
- Smeets, A.J.; Lejeune, M.P.; Westerterp-Plantenga, M.S. Effects of oral fat perception by modified sham feeding on energy expenditure, hormones and appetite profile in the postprandial state. Br. J. Nutr. 2009, 101, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Research Randomizer. Available online: https://www.randomizer.org/ (accessed on 10 January 2016).
- Rolls, B.J.; Morris, E.L.; Roe, L.S. Portion size of food affects energy intake in normal-weight and overweight men and women. Am. J. Clin. Nutr. 2002, 76, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Burger, K.S.; Fisher, J.O.; Johnson, S.L. Mechanisms behind the portion size effect: Visibility and bite size. Obesity 2011, 19, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Veldhorst, M.A.; Nieuwenhuizen, A.G.; Hochstenbach-Waelen, A.; van Vught, A.J.; Westerterp, K.R.; Engelen, M.P.; Brummer, R.J.; Deutz, N.E.; Westerterp-Plantenga, M.S. Dose-dependent satiating effect of whey relative to casein or soy. Physiol. Behav. 2009, 96, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: What, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef]
- Astbury, N.M.; Stevenson, E.J.; Morris, P.; Taylor, M.A.; Macdonald, I.A. Dose-response effect of a whey protein preload on within-day energy intake in lean subjects. Br. J. Nutr. 2010, 104, 1858–1867. [Google Scholar] [CrossRef] [PubMed]
- Tinuviel Software. NetWISP (Version 3.0 and 4.0); Tinuviel Software: Anglesey, UK, 2006. [Google Scholar]
- Beck, E.J.; Tosh, S.M.; Batterham, M.J.; Tapsell, L.C.; Huang, X.F. Oat beta-glucan increases postprandial cholecystokinin levels, decreases insulin response and extends subjective satiety in overweight subjects. Mol. Nutr. Food Res. 2009, 53, 1343–1351. [Google Scholar] [CrossRef]
- Livingstone, B.E.; Robson, P.J.; Welch, R.W.; Burns, A.A.; Burrows, M.S.; Mccormack, C. Methodological issues in the assessment of satiety. Näringsforskning 2000, 44, 98–103. [Google Scholar] [CrossRef]
- Almoosawi, S.; McDougall, J.G.; Fyfe, L.; Al-Dujaili, E.A.S. Investigating the inhibitory activity of green coffee and cacao bean extracts on pancreatic lipase. Nutr. Bull. 2010, 35, 207–212. [Google Scholar] [CrossRef]
- Lesschaeve, I.; Noble, A.C. Polyphenols: Factors influencing their sensory properties and their effects on food and beverage preferences. Am. J. Clin. Nutr. 2005, 81, 330S–335S. [Google Scholar] [CrossRef]
- Zaremba, S.M.M.; Drummond, S.; Steinert, R.E. The need to standardize ad libitum eating protocols in dietary fibre appetite research. Eur. J. Clin. Nutr. 2017, 71, 570–572. [Google Scholar] [CrossRef]
- Josic, J.; Olsson, A.T.; Wickeberg, J.; Lindstedt, S.; Hlebowicz, J. Does green tea affect postprandial glucose, insulin and satiety in healthy subjects: A randomized controlled trial. Nutr. J. 2010, 9, 63. [Google Scholar] [CrossRef]
- Jull, A.B.; Ni Mhurchu, C.; Bennett, D.A.; Dunshea-Mooij, C.A.; Rodgers, A. Chitosan for overweight or obesity. Cochrane Database Syst. Rev. 2008, CD003892. [Google Scholar] [CrossRef]
- Gibson, R.; Eriksen, R.; Lamb, K.; McMeel, Y.; Vergnaud, A.C.; Spear, J.; Aresu, M.; Chan, Q.; Elliott, P.; Frost, G. Dietary assessment of British police force employees: A description of diet record coding procedures and cross-sectional evaluation of dietary energy intake reporting (The Airwave Health Monitoring Study). BMJ Open 2017, 7, e012927. [Google Scholar] [CrossRef]
- Beasley, J.M.; Riley, W.T.; Davis, A.; Singh, J. Evaluation of a PDA-based dietary assessment and intervention program: A randomized controlled trial. J. Am. Coll. Nutr. 2008, 27, 280–286. [Google Scholar] [CrossRef]
- Opala, T.; Rzymski, P.; Pischel, I.; Wilczak, M.; Wozniak, J. Efficacy of 12 weeks supplementation of a botanical extract-based weight loss formula on body weight, body composition and blood chemistry in healthy, overweight subjects—A randomised double-blind placebo-controlled clinical trial. Eur. J. Med. Res. 2006, 11, 343–350. [Google Scholar]
- Moyad, M.A. The optimal male health diet and dietary supplement program. Urol Clin. N. Am. 2012, 39, 89–107. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutritional Composition | Pasta (500 g Cooked) | Pasta Sauce (500 g) | Total Meal Composition | Pomegranate Juice (PJ) | Placebo Juice |
|---|---|---|---|---|---|
| Energy (kcal) | 765 | 220 | 985 | 72 | 72 |
| Protein (g) | 28 | 9 | 37 | 0.6 | Trace |
| Carbohydrates (g) | 138.5 | 39.5 | 178 | 18 | 18 |
| Sugars (g) | 3.5 | 35 | 38.5 | ||
| Fat (g) | 8.5 | 3 | 11.5 | Trace | Trace |
| Saturated fat (g) | 2.5 | 0.5 | 3 | ||
| Fibre (g) | 12 | 9 | 21 | Trace | Trace |
| Sodium (g) | Trace | 2 | 2 | ||
| Polyphenols (mg GAE) | 126 | Negligible |
| Time | Procedures |
|---|---|
| 8:30 a.m. | Breakfast served and eaten. 60 g crunchy nut cornflakes; 150 mL semi-skim milk; 150 mL pomegranate juice (PJ) or placebo drink (PLD). |
| 3-h interval | Participants fast and then returned to the kitchen/food laboratory for the lunch session. |
| 11:30 a.m. (0–15 min) | Starting to complete VAS for satiety (VAS 1 baseline; zero point) 150 mL of PJ juice preload for all participants (both groups) (VAS 2 satiety and palatability variables). |
| 12:00 noon (30 min) | Lunch presented to each participant (VAS 3 satiety variables before eating anything) |
| 12:05 p.m. (35 min) | Participants consumed 1 spoon of lunch (VAS for palatability and meal quality variables). Afterwards, participants continued to eat the lunch. |
| 12:15 p.m. (45 min) | Participants completed VAS 4 for satiety and meal palatability variables. A timer prompts the participants. |
| 12:30 p.m. (60 min) | VAS 5; satiety and meal palatability (repeat VAS 4) |
| 12:45 p.m. (75 min) | VAS 6; satiety and meal palatability (repeat VAS 4) |
| 1:00 p.m. (90 min) | VAS 7; satiety and meal palatability (repeat VAS 4) |
| 1:15 p.m. (105 min) | VAS 8; satiety and meal palatability (repeat VAS 4) |
| 1:30 p.m. (120 min) | VAS 9; satiety and meal palatability (repeat VAS 4) |
| Characteristic | Pomegranate Extract Capsule Group Mean (SD) | Placebo Capsule Group Mean (SD) |
|---|---|---|
| Age (years) | 34.5 (13.7) | 32.6 (12.9) |
| Gender (M; F) | 4; 10 | 4; 10 |
| Height (m) | 1.66 (0.06) | 1.70 (0.09) |
| Weight (kg) | 70.0 (13.7) | 72.1 (12.0) |
| BMI (kg/m2) | 25.1 (4.5) | 24.94 (3.4) |
| Variable | Pomegranate Extract (PE) | Placebo (PL) Group (n = 14) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Group (n = 14) | |||||||||
| p | p | ||||||||
| Mean | SD | SEM | Value | Mean | SD | SEM | Value | ||
| Energy (kcal) | Baseline | 1913.20 | 415.97 | 107.40 | 1840.64 | 411.93 | 113.19 | ||
| 4th week | 2109.53 | 512.60 | 132.35 | 2119.79 | 542.34 | 143.30 | |||
| Change | −196.33 | 388.90 | 100.41 | 0.071 | −279.14 | 629.49 | 168.24 | 0.121 | |
| Energy (kJ) | Baseline | 8037.53 | 1744.32 | 450.38 | 7738.14 | 322.55 | 86.21 | ||
| 4th week | 8893.00 | 2148.51 | 554.74 | 8931.14 | 556.36 | 148.69 | |||
| Change | −855.47 | 1611.12 | 415.99 | 0.069 | 1193.00 | 2639.54 | 705.45 | 0.115 | |
| Protein (g) | Baseline | 75.52 | 16.42 | 4.24 | 78.44 | 1345.88 | 359.70 | ||
| 4th week | 75.23 | 12.69 | 3.28 | 91.34 | 2338.91 | 625.10 | |||
| Change | 0.29 | 17.48 | 4.51 | 0.950 | −12.89 | 24.31 | 6.50 | 0.069 | |
| Carbohydrate (g) | Baseline | 232.75 | 59.84 | 15.45 | 210.76 | 38.45 | 10.28 | ||
| 4th week | 297.53 | 74.52 | 19.24 | 269.29 | 54.24 | 14.50 | |||
| Change | −64.78 | 30.69 | 7.92 | 0.021 | −58.53 | 80.59 | 21.54 | 0.018 | |
| Sugars (g) | Baseline | 101.47 | 42.59 | 11.00 | 90.91 | 34.67 | 9.27 | ||
| 4th week | 129.14 | 47.02 | 12.14 | 111.00 | 67.11 | 17.94 | |||
| Change | −27.67 | 30.17 | 7.79 | 0.033 | −20.09 | 29.12 | 7.78 | 0.023 | |
| Starch (g) | Baseline | 127.12 | 44.23 | 11.42 | 112.13 | 27.58 | 7.37 | ||
| 4th week | 162.75 | 44.19 | 11.41 | 154.53 | 26.64 | 7.12 | |||
| Change | −35.63 | 31.52 | 8.14 | 0.021 | −42.40 | 60.00 | 16.04 | 0.026 | |
| Total fat (g) | Baseline | 76.73 | 30.22 | 7.80 | 80.28 | 30.08 | 8.04 | ||
| 4th week | 71.60 | 26.46 | 6.83 | 77.90 | 44.82 | 11.98 | |||
| Change | 5.13 | 32.90 | 8.50 | 0.556 | 2.38 | 33.40 | 8.93 | 0.794 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stockton, A.; Al-Dujaili, E.A.S. Effect of Pomegranate Extract Consumption on Satiety Parameters in Healthy Volunteers: A Preliminary Randomized Study. Foods 2022, 11, 2639. https://doi.org/10.3390/foods11172639
Stockton A, Al-Dujaili EAS. Effect of Pomegranate Extract Consumption on Satiety Parameters in Healthy Volunteers: A Preliminary Randomized Study. Foods. 2022; 11(17):2639. https://doi.org/10.3390/foods11172639
Chicago/Turabian StyleStockton, Angela, and Emad A. S. Al-Dujaili. 2022. "Effect of Pomegranate Extract Consumption on Satiety Parameters in Healthy Volunteers: A Preliminary Randomized Study" Foods 11, no. 17: 2639. https://doi.org/10.3390/foods11172639
APA StyleStockton, A., & Al-Dujaili, E. A. S. (2022). Effect of Pomegranate Extract Consumption on Satiety Parameters in Healthy Volunteers: A Preliminary Randomized Study. Foods, 11(17), 2639. https://doi.org/10.3390/foods11172639