1. Introduction
Celiac disease (CD) is a systemic immune disorder triggered by an aberrant response to gluten proteins that causes progressive atrophy of the intestinal villi of genetically susceptible individuals, resulting in impaired intestinal absorption and malnutrition, although in many cases the disease is asymptomatic [
1]. The prevalence of CD in European and American populations of European descent is 1% [
2].
The only effective therapy for CD is to follow a rigorous and lifelong gluten-free diet, which regenerates intestinal villi and restores adequate nutrient absorption, although only 1/3 of adults have normal villous architecture (a healthy, healed intestine) after two years, and 2/3 after five years on a gluten-free diet [
3]. However, diagnosis during childhood and less severe histologic damage at diagnosis have been associated with mucosal recovery [
4]. The gluten-free diet comprises food products that originally do not contain gluten, i.e., legumes, eggs, fruits and vegetables, meat and fish derivatives, and the avoidance of wheat, barley, rye, oats, and all products derived from these cereals (starch, flour, breads, pasta, etc.), as well as any product in which gluten containing ingredients are used by the food industry [
5].
Some studies indicate nutritional imbalances in different celiac populations following a gluten-free diet in terms of macro and micronutrient intakes because of a bad choice of foods and gluten-free products (GFP) [
6]. Nutritional studies undertaken in children and youngsters, some of which have compared with a control group without the disease, have shown that CD patients consume more lipids (especially saturated), protein and simple carbohydrates, but less fiber and micronutrients such as iron, calcium, zinc, magnesium and vitamin D, folates and other B-vitamins than recommended [
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24], even if adherence to the gluten-free diet is long-term (more than one year). Childhood and adolescence carry unique issues pertaining to the diagnosis and management of celiac disease, because of the high nutritional requirements for growth during these periods. Moreover, dietary habits acquired in childhood and adolescence prevail in adulthood.
Different authors have proposed that nutritional deficiencies in CD patients may be due to GFP, which are made with highly refined flours and extra amounts of fat and sugar to obtain a texture resembling the typical and unique viscoelastic properties of wheat [
25,
26]. Gluten-free manufactured products are generally high in fat to improve their presentation and palatability [
13], and recent articles conclude that GFP often have a greater carbohydrate and lipid content, but less protein than their gluten containing equivalents [
27,
28,
29,
30]. Macronutrient analysis of GFP commercially available in Spain has evidenced that 25.4% of the products could be labelled as a source of fiber, and many presented very high contents of energy (33.5%), fats (28.5%), saturated fatty acids (30.0%), sugars (21.6%), and salt (28.3%) [
31]. Folates and other B-vitamins were also present in significantly lower amounts than in their gluten-containing counterparts [
32,
33,
34,
35]. According to Allen and Orfila [
36], only 5% of gluten-free breads were fortified with all four mandatory fortification nutrients (calcium, iron, nicotinic acid or nicotinamide, and thiamine) in the United Kingdom, and only 28% of gluten-free breads were fortified with calcium and iron. Fortified GFP represent only 10% of gluten-free staple foods in Europe, because different starches are used as main ingredient and that makes it difficult to implement a common fortification strategy [
37].
Furthermore, the use of raw materials such as unenriched rice or maize refined flours, gums, or enzymes in GFP formulation could lead to a different composition as compared to their gluten-containing homologues [
38]. GFP commercially available in Spain are primarily composed of rice and/or corn flour, and only a 28% of products are supplemented with a low quantity of quinoa, soy and other legumes, or other flours (oatmeal, sorghum, amaranth, teff, guar, chia, chestnut, flax, potato) [
31]. Since the micronutrient content of gluten-free pseudocereals and legumes is higher than that of the gluten-free cereals [
16], some authors have proposed the promotion of their use in GFP formulation [
25,
26,
35]. Breakfast cereals were the group with the most frequent inclusion of alternative cereals in GFP in the Spanish market [
31]. Therefore, manufacturers seem to be timidly introducing the use of nutritious pseudocereal and legume flours in the formulation of GFP. In this sense, Melini and Melini [
25] have also shown that an interesting trend towards some improvements in GFP composition has emerged. In this sense, although the composition in terms of fiber and sugars is highly variable among different product varieties, reports of the two last years showed more adequate levels of fiber and sugar than in the past. In fact, Larretxi et al. [
39] have reported an equivalent fiber and resistant starch content, which was even higher in breads, compared with their homologues. The increased fiber content and improved technological processes have positively affected the glycemic responses from these goods [
32].
The insufficient labelling description and narrow availability of nutritionally balanced products and brands for the population affected with CD may limit to a greater or lesser extent the ability to follow a balanced diet. The question is whether the consumption of these products by the celiac population is sufficient to cause the nutritional imbalances, or whether it is due more to poor food choices from other food groups. Bearing this in mind, our aim in this study is to assess the contribution of GFP to the diet (energy and nutrient content) of a group of children and adolescents, both genders, with CD in Spain.
Only by analyzing the consumption of GFP and the amount of critical nutrients they provide in relation to the total diet will it be possible in the future to carry out correct and effective nutritional education for this population group, offering an appropriate choice of foods, both fresh and processed. In this sense, it is important that children and young people with CD become aware of the importance of reading the labelling in terms of ingredients and nutritional composition. The data in this study may also be useful for the food industry in reformulation or fortification strategies on GFP.
3. Results
A total of 70 Spanish children and adolescents with celiac disease (CD) participated in the study (35 boys and 35 girls, 56 aged 4–12 years old, and 14 aged 13–18 years old). They all declared themselves to have been on a gluten-free diet for more than one year, and 96.8% stated good adherence. In the immune tests, all values fell under threshold values (<6.9 U/mL) for untreated CD or accidental exposure to gluten. A great part of the sample (92.9%) consumed processed gluten-free products (GFP) three to four times a day, and only one volunteer declared not taking gluten-free substitutes. Most participants consumed processed GFP (98.5%), but only 30% of them consumed homemade GFP once a day or less. Volunteers declared taking between four to five meals a day, usually at home except for school days (zero to one meal a week outside the home), and seldom taking fast food (twice a month as the median). We have previously published data on dietary intake, food consumption patterns, and biochemical and anthropometric data from this same population group [
18].
Table 1 shows daily intake of gluten-free cereal-based substitutes, both processed (commercially available) and homemade. Children and adolescents with CD in Spain consume over 165 g a day of GFP, which are mostly bread and fine bakery ware, followed by pasta. Fine bakery ware includes biscuits and pastry in similar proportions, except for adolescents, who take a smaller amount of biscuits. Intake of gluten-free breakfast cereals and cereal bars is much lower, and consumption of gluten-free pizza, prepared food products and snacks varies significantly between volunteers. Only 34 out of the 70 volunteers declared that they had been taking gluten-free savory commercial products, i.e., pizza, nuggets, nachos with cheese, tortitas, gnocchi, pie, or croquette. There are no big differences between groups based on sex and age, except for a higher consumption of biscuits among children aged four to 12, and a higher consumption of savory cereal dishes in boys and adolescents over 12. Consumption of homemade GFP is testimonial as compared to commercial products.
Table 2 shows the percentage contribution of GFP to total energy and nutrient intakes, in Spanish children and adolescents, using the nutrient information presented on the labels. GFPs contributed with a high percentage (>25%) to energy, carbohydrates, fiber, and salt daily intakes and, to a lesser extent (<20%), to fat (including saturated fat), sugars and protein. When considering age and sex (
Table 3), GFP contribution to total intakes is higher in boys than girls for all nutrients analyzed, although only statistically significant in the case of saturated fat. There seems to be no effect of age; and GFP percentage contribution to energy, macronutrient, fiber, and salt intakes is similar between children aged four to 12 and adolescents over 13.
Table 4,
Table 5,
Table 6,
Table 7,
Table 8 and
Table 9 provide an in-depth analysis of the contribution of each type of GFP to energy and nutrient intakes. The GFP with significantly higher contributions to total energy intake were bread and fine bakery ware, which accounted in similar proportions for 70% of the total energy provided by GFP (
Table 4). In the case of fat and saturated fat (
Table 5), fine bakery ware was the greatest contributor, providing a significantly higher amount—three-fold—as compared to the second greatest contributor, bread. All GFP provide carbohydrates, but fine bakery ware contributes with 59% of all sugars provided by GFP (
Table 6). Percentage contribution of GFP to total protein intake (
Table 7) is low in all cases. Bread is the most important contributor to fiber intake within the GFP, accounting for 56% of all fiber provided by GFP (
Table 8). On the other hand, salt is provided mainly by bread, which accounts for 52% of the salt provided by GFP (
Table 9). Regarding gender, savory cereal dishes contribution to total energy, saturated fat, carbohydrates, sugars, and salt was higher in boys as compared with girls. Fine bakery ware provides a lesser amount of fiber in adolescents as compared with younger children.
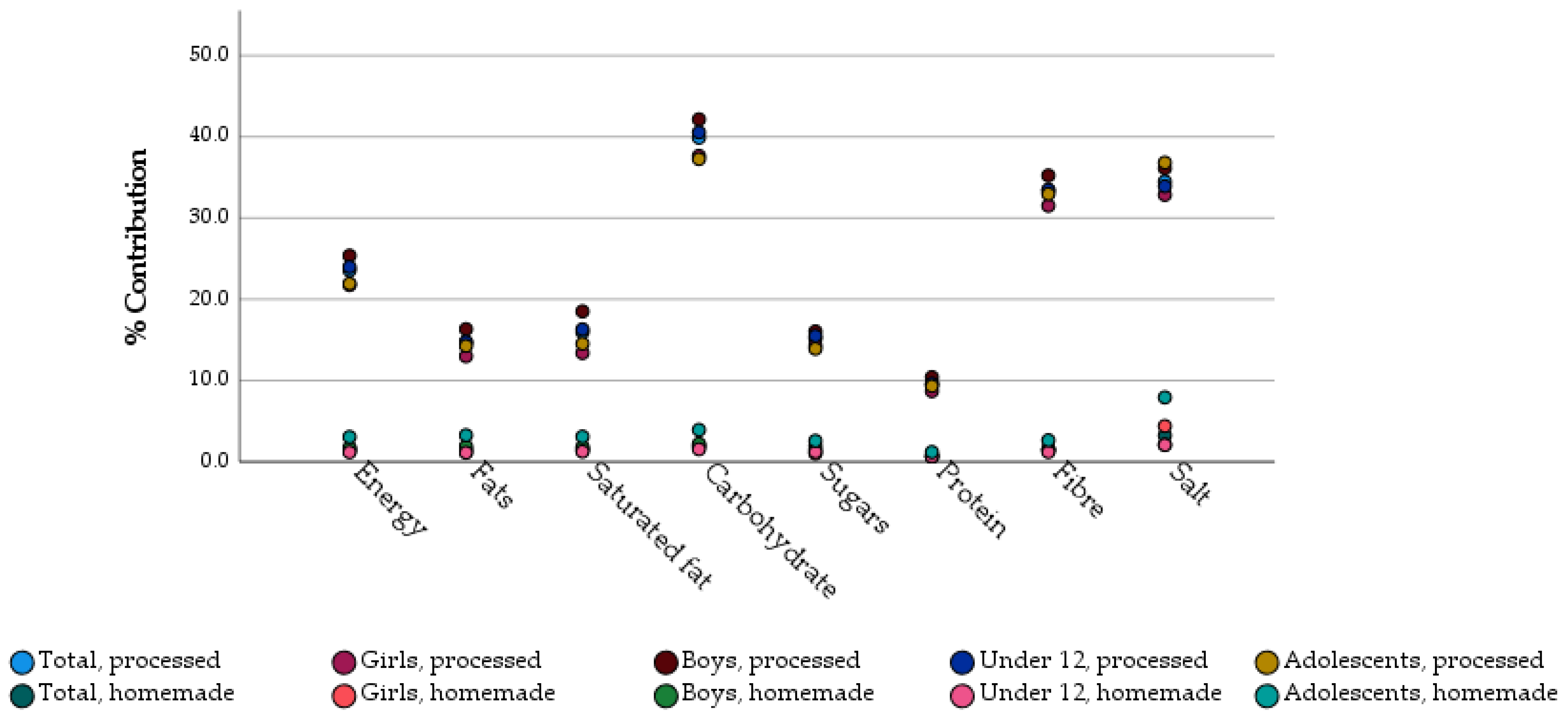
Finally, we assessed gluten-free homemade products and gluten-free commercial products separately. In this context, we observed a minimal contribution of homemade products, being most energy and nutrients coming from processed products (
Figure 1). Homemade GFP accounted for 1.5% of total energy intake, whilst processed commercial products provided 23.4% of total energy. No differences in consumption of homemade or processed commercial products were detected depending on age or gender.
4. Discussion
To our knowledge, this is the first study to assess, in a comprehensive way, the contribution of gluten-free products (GFP) to energy and macronutrient intakes in Spanish children and adolescents with celiac disease (CD), and the only one that, in addition, considers both homemade and commercial products. GFP contributed with a high percentage to energy, carbohydrate, fiber, and salt daily intakes and, to a lesser extent to fat (including saturated fat), sugars and protein. Boys tended to consume a higher amount of GFP as compared with girls, but GFP contribution to total diet was only significantly higher for boys in the case of saturated fat. However, age seemed to make no difference, with GFP contribution to daily energy and macronutrient intakes being similar in children under 12 years old and adolescents over 12. In all cases, we observed a minimal contribution of homemade products, and most energy and nutrients came from processed commercial products.
Our results are slightly different to those shown by Zucotti et al. [
13] in their cross-sectional study on children with CD as compared to controls, in which commercially available GFP accounted for 36.3% of daily total energy intake and 18% of total protein-derived energy in Italian children. In this same research [
13], almost half (49.5%) of the total carbohydrate intake and the majority (77.0%) of the 53.2% carbohydrate-derived daily energy was derived from GFP, results which are higher than those found in our study (almost 40% of total carbohydrates and 40% of carbohydrate-derived energy are provided by GFP). In the case of fat, our results are similar to those shown in Italian children, where GFP contributed a median of 12.9 g per day of fat intake. On the other hand, Larretxi et al. [
39] have revealed that the main contributors to the fiber intake of Spanish adult and pediatric participants following a gluten-free diet are GFP (~50%), especially breads, but fiber intake was still slightly below recommendations. In our study, GFP contribution to daily fiber intakes is lower (~36%).
According to a cross-sectional study using a representative sample of Spanish population [
42], grains (i.e., grains and flours, bread, breakfast cereals, cereal bars, pasta, and bakery and pastry) are the main contributors to energy, carbohydrate, and fiber intakes, providing up to 30%, 49% and 47% of total daily intake in children (aged 9–12 years), and up to 31%, 51% and 49% of total daily intake in adolescents (aged 13–17 years). This same study [
42] showed that the main contributors to protein intake are meat and meat products, followed by grains and grain-based products, and milk and dairy products, contributing, all together, to about 72% of the protein intake in children and adolescents. Finally, grains were also the fourth contributor to lipid intake (12%) in children and adolescents, providing a significant amount of saturated fat from bakery wares and pastry in children (11%) and 15% of total sugar intake [
42]. In the present study, GFP provided 25% of total energy, an amount which is close to that described for all grains in general population in Spain with the same age. Moreover, GFP contribution to energy daily intake is in the range of a healthy breakfast, which according to dietary recommendations in Spain should contribute around 20–25% to the total daily energy intake [
43]. Therefore, GFP contribution to total energy intake in children and adolescents with CD may be considered significant and, consequently, relevant to the nutritional adequacy of the diet.
Our data, taken together, show a high consumption of products marketed and labelled as gluten-free, the vast majority of which are processed. Although some authors have described an incipient reformulation of these products [
31], especially concerning fiber and types of fat, and no differences in fiber content between GFP and their gluten-containing counterparts has been described [
39], high GFP consumption could raise several problems, both nutritionally and otherwise, since the low nutritional quality of these products has been highlighted in various studies [
25,
26].
From the nutritional point of view, grains and cereal-based products are staple foods in Mediterranean type diets. Because of a different composition of GFP as compared to regular counterparts, gluten-free diets may be low in fiber and rich in fat, saturated fat, and salt [
25,
44]. In the case of fiber, GFP in our study provided less fiber (30%) than regular grains in Spanish children and adolescents [
42]. Gluten-free bread was the main contributor. Nonetheless, GFP plus other naturally gluten-free grains i.e., rice and corn, and other food sources contributed to a total dietary fiber intake which, as a median value, was adequate in children (18 g/day), but low in adolescents (17 g/day), according to dietary reference values from the European Food Safety Authority (EFSA) i.e., 14–16 g/day for children between four and 10 years old, and 19–21 g/day for adolescents between 11 and 17 years old [
45]. This may be due also to a higher intake of fruits in boys with CD as compared to controls, as we have described before in this same study group [
18].
As compared to regular grains, GFP contribution to total and saturated fat intakes in our study was higher than that of all grains in healthy children and adolescents consuming a regular diet in Spain (16% vs. 13% for total fat and 17% vs. 13% for saturated fat), as published in the ANIBES study [
42]. The GFPs that most contributed fat and saturated fat were fine bakery ware. Moreover, GFP contribution was particularly high in males and for saturated fat (17%), posing a worrying situation for children and adolescents following a gluten-free diet. Other authors have already stated that following a gluten-free diet increases the risk of cardiometabolic related pathologies such as obesity [
46,
47] or cardiovascular disease [
48]. On this basis, it seems reasonable to propose a fat and saturated fat reduction in GFP formulation, especially in the case of fine bakery ware.
GFP were also important contributors to total sugar intake, especially in the diets of children on a gluten-free diet under 12 years old and boys, where they contributed to almost 18% of total sugar intake. This is a 30% higher amount as compared to Spanish children, whose diets include grains that provide 13% of total sugar intake, as described in the study by Ruiz et al. [
42]. Children under 12 years old on a gluten-free diet in our study were consuming 17% of total energy from sugars [
18], although only 2.6% of total calories were coming from sugars in GFP. A young population group with CD in Spain (aged 10 to 23) also reported higher consumption of added sugar and total fat than healthy individuals [
14]. According to recommendations [
49], the intake of added and free sugars should be as low as possible in the context of a nutritionally adequate diet. Thus, children, especially boys, could also benefit from sugar content reduction in their diets. Nonetheless, GFP do not seem to contribute decisively to total sugar intakes in our study.
GFP provide only 10% of protein daily intake, which is only half the contribution of all grains to protein intakes in healthy children and adolescents [
42]. GFP are known to contain a lower amount of protein as compared to gluten-containing counterparts [
27,
28,
29,
30], due to gluten extraction or to the use of refined flours and starches in their formulation. Nonetheless, protein intake in Spanish children and adolescents with celiac disease is not below that of healthy controls [
18], and protein intakes in Spain are excessive and nutritionally unnecessary in healthy individuals [
42].
GFP contribution to daily salt intake reached 38% as a median value, with slightly higher contributions in boys and adolescents over 12 years old. High salt content has been described as one of the key inadequacies of GFP, besides high fat and low protein contents [
25]. In Spanish population, main dietary sources of sodium are meat and meat products and cereal and grains, accounting for 53% of sodium consumption [
50]. According to our data, gluten-free cereal products are also primary contributors to sodium/salt intakes, in the same order of magnitude as all grains, and bread plays a leading role. Moreover, sodium intakes in Spain in general population are above recommendations, and significantly higher amongst children and adolescents when compared to adults and the elderly [
50]. Therefore, salt reduction in GFP could be an effective intervention for health promotion and disease prevention. In fact, several agreements between the Spanish Health Administration and the food industry have prompted manufacturers to decrease salt addition to foods [
51] and to bread [
52], as a main contributor to sodium intakes, not only because of its salt content, but also and mainly because of the frequency of consumption. Unfortunately, special products such as commercial GFP designed for consumers with CD fall out of the scope of these initiatives.
Although the contribution of GFP to salt intakes is high, data on salt and sodium intakes should be taken cautiously since there are specific difficulties in the estimation of this nutrient. In our study, we quantified sodium coming from regular foods using data from Spanish Food Composition Tables on the DIAL® software version 3.15, and salt in GFP as presented by manufacturers in the label. Therefore, we have not quantified discretionary salt use (salt added during cooking or at the table). All data on sodium have been converted to salt (1 mg sodium = 2.4 mg salt).
In our view, there are several alternative ways to improve the nutritional quality of the gluten-free diet, apart from GFP reformulation to reduce the content of critical nutrients. For example, some authors have proposed fortification of GFP. Cyrkot et al. [
33] exposed the fact that gluten-free folate-rich foods represented <15% of all household food purchases, and 69% of children had low folate intakes. Along the same line of conclusions, Larretxi et al. [
35] proposed GFP fortification with folate and biotin to prevent the deficiencies observed in the gluten-free diet, at least in the case of pediatric CD. These findings highlight the opportunity for vitamin and mineral fortification policies for GFP and the necessity of nutrition guidelines for children with CD consuming a gluten-free diet.
Alimentary education should also become part of the therapeutic pathway to understand the importance of labels, choice of food, and combination of macro and micronutrients. Furthermore, the dietary therapeutic approach should encourage the use of naturally gluten-free products such as pseudo-cereals that have been shown to have good nutritional quality [
20], and green vegetables, fruits, legumes, and fish [
17,
22,
32].
A logical and intelligent strategy that could bring long-term benefits is the use of homemade products made with flours from other sources (other than rice and corn) complemented with proper nutrition education, including the avoidance of commercial GFP. Gluten restriction has important implications for nutrient adequacy, since staple foods (e.g., breads, pastas, and cereals) are key nutrient sources in the western diet, especially in young people. The use of nutrient-dense gluten-free flours, rather than starches, in homemade foods may improve nutrient intakes, and homemade recipes may allow for fat and sugar control. In this sense, chickpea flour registered the highest folate content followed by quinoa, amaranth, and flaxseed gluten-free flours; chickpea, flaxseed, and chia flours have higher protein contents; and tapioca, buckwheat, and brown rice flour are rich in carbohydrates and total starch [
53]. The challenge in using alternative flours in natura in food preparation is the need for high food literacy (e.g., food skills, budgeting, and nutrition knowledge) and more time for meal planning and cooking in comparison to purchasing ready-to-serve products.
Regarding the limitations of the present study, it is important to state that there is a lack of nutritional information about gluten-free products on food composition since labels do not provide information on micronutrient contents. Data on salt and sodium intakes should be taken cautiously since we have not quantified discretionary salt use (salt added during cooking or at the table). Finally, the research is a follow up study of an initial project comparing dietary habits of children with and without CD, and the sample size was adapted to the comparison research. Therefore, sample representativeness error increases to 10% for conclusions drawn over the whole population of children and adolescents with CD and to 26% when concerning adolescents. Increasing the sample size in future studies will help to confirm the results found in here.

 ,
, 


{kind=link}