
Benzalkonium Chloride Poisoning in Pediatric Patients: Report of Case with a Severe Clinical Course and Literature Review


Abstract
:
1. Introduction
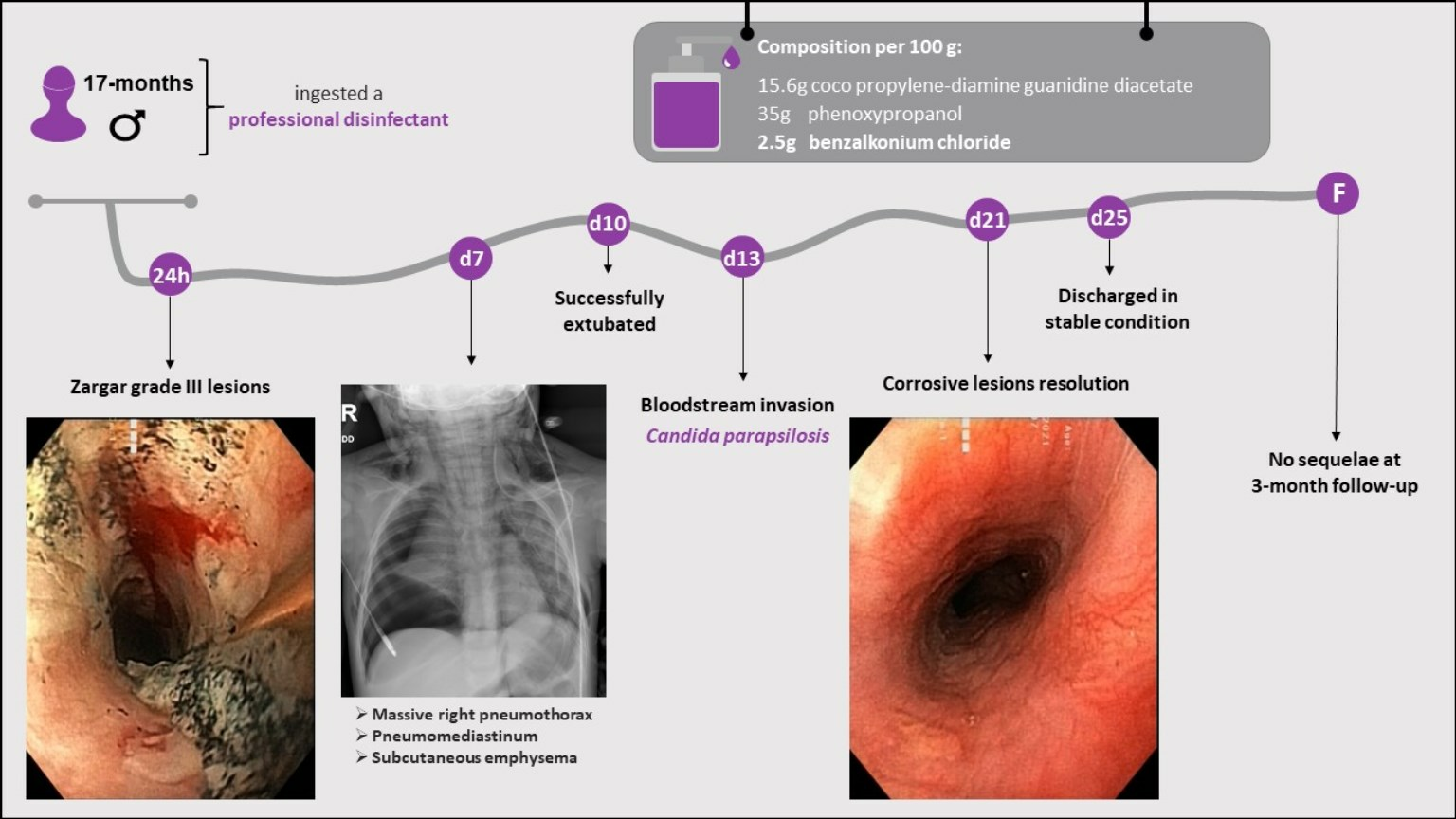
2. Case Description
3. Discussion
3.1. General Considerations
3.2. Gastrointestinal Tract Involvement
3.3. Respiratory Tract Involvement
3.4. Other Complications
3.5. Previously Reported Cases of BAC Ingestion
3.6. Pharmacological Properties
3.7. Proposed Management of BAC Poisoning
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenman, K.D.; Reilly, M.J.; Wang, L. Calls to a State Poison Center Concerning Cleaners and Disinfectants from the Onset of the COVID-19 Pandemic through April 2020. Public Health Rep. 2021, 136, 27–31. [Google Scholar] [CrossRef]
- Hrubec, T.C.; Seguin, R.P.; Xu, L.; Cortopassi, G.A.; Datta, S.; Hanlon, A.L.; Lozano, A.J.; McDonald, V.A.; Healy, C.A.; Anderson, T.C.; et al. Altered Toxicological Endpoints in Humans from Common Quaternary Ammonium Compound Disinfectant Exposure. Toxicol. Rep. 2021, 8, 646–656. [Google Scholar] [CrossRef]
- Li, D.; Sangion, A.; Li, L. Evaluating Consumer Exposure to Disinfecting Chemicals against Coronavirus Disease 2019 (COVID-19) and Associated Health Risks. Environ. Int. 2020, 145, 106108. [Google Scholar] [CrossRef]
- Osimitz, T.G.; Droege, W. Quaternary Ammonium Compounds: Perspectives on Benefits, Hazards, and Risk. Toxicol. Res. Appl. 2021, 5, 239784732110490. [Google Scholar] [CrossRef]
- Mai, Y.; Wang, Z.; Zhou, Y.; Wang, G.; Chen, J.; Lin, Y.; Ji, P.; Zhang, W.; Jing, Q.; Chen, L.; et al. From Disinfectants to Antibiotics: Enhanced Biosafety of Quaternary Ammonium Compounds by Chemical Modification. J. Hazard. Mater. 2023, 460, 132454. [Google Scholar] [CrossRef]
- Sapozhnikov, S.V.; Sabirova, A.E.; Shtyrlin, N.V.; Druk, A.Y.; Agafonova, M.N.; Chirkova, M.N.; Kazakova, R.R.; Grishaev, D.Y.; Nikishova, T.V.; Krylova, E.S.; et al. Design, Synthesis, Antibacterial Activity and Toxicity of Novel Quaternary Ammonium Compounds Based on Pyridoxine and Fatty Acids. Eur. J. Med. Chem. 2021, 211, 113100. [Google Scholar] [CrossRef] [PubMed]
- Crescioli, G.; Lanzi, C.; Gambassi, F.; Ieri, A.; Ercolini, A.; Borgioli, G.; Bettiol, A.; Vannacci, A.; Mannaioni, G.; Lombardi, N. Exposures and suspected intoxications during SARS-CoV-2 pandemic: Preliminary results from an Italian poison control centre. Intern. Emerg. Med. 2022, 17, 535–540. [Google Scholar] [CrossRef] [PubMed]
- du Plessis, C.E.; Mohamed, F.; Stephen, C.R.; Reuter, H.; Voigt, G.; van Hoving, D.J.; Marks, C.J. A retrospective review of calls to the Poisons Information Helpline of the Western Cape during the first 6 months of the COVID-19 pandemic in South Africa. S. Afr. J. Infect. Dis. 2022, 37, 391. [Google Scholar] [CrossRef] [PubMed]
- Le Roux, G.; Sinno-Tellier, S.; Puskarczyk, E.; Labadie, M.; von Fabeck, K.; Pélissier, F.; Nisse, P.; Paret, N.; French PCC Research Group; Descatha, A.; et al. Poisoning during the COVID-19 outbreak and lockdown: Retrospective analysis of exposures reported to French poison control centres. Clin. Toxicol. 2021, 59, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Ghai, A.; Sabour, E.; Salonga, R.; Ho, R.; Apollonio, D.E. Exposures to Bleach, Peroxide, Disinfectants, Antimalarials, and Ivermectin Reported to the California Poison Control System Before and During the COVID-19 Pandemic, 2015–2021. Public Health Rep. 2024, 139, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Yasseen Iii, A.; Weiss, D.; Remer, S.; Dobbin, N.; MacNeill, M.; Bogeljic, B.; Leong, D.; Wan, V.; Mosher, L.; Bélair, G.; et al. Increases in exposure calls related to selected cleaners and disinfectants at the onset of the COVID-19 pandemic: Data from Canadian poison centres. Health Promot. Chronic Dis. Prev. Can. 2021, 41, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kwon, D.; Lee, S.; Son, S.W.; Kwon, J.T.; Kim, P.J.; Lee, Y.H.; Jung, Y.S. Concentration-and Time-Dependent Effects of Benzalkonium Chloride in Human Lung Epithelial Cells: Necrosis, Apoptosis, or Epithelial Mesenchymal Transition. Toxics 2020, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.M.P.; Tagkopoulos, I. Benzalkonium Chlorides: Uses, Regulatory Status, and Microbial Resistance. Appl. Environ. Microbiol. 2019, 85, e00377-19. [Google Scholar] [CrossRef]
- Seguin, R.P.; Herron, J.M.; Lopez, V.A.; Dempsey, J.L.; Xu, L. Metabolism of Benzalkonium Chlorides by Human Hepatic Cytochromes P450. Chem. Res. Toxicol. 2019, 32, 2466–2478. [Google Scholar] [CrossRef]
- Mishima-Kimura, S.; Yonemitsu, K.; Ohtsu, Y.; Sasao, A.; Tsutsumi, H.; Furukawa, S.; Nishitani, Y. Liquid Chromatography-Tandem Mass Spectrometry Detection of Benzalkonium Chloride (BZK) in a Forensic Autopsy Case with Survival for 18 Days Post BZK Ingestion. Leg. Med. 2018, 32, 48–51. [Google Scholar] [CrossRef]
- Tambuzzi, S.; Gentile, G.; Andreola, S.; Migliorini, A.S.; Zoja, R. Visceral Microscopic Pattern From Suicidal Ingestion of Professional Lysoform® with Delayed Death. Acad. Forensic Pathol. 2022, 12, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Karaman, I.; Koç, O.; Karaman, A.; Erdogan, D.; Çavusoglu, Y.H.; Afsarlar, Ç.E.; Yilmaz, E.; Ertürk, A.; Balci, Ö.; Özgüner, I.F. Evaluation of 968 Children with Corrosive Substance Ingestion. Indian J. Crit. Care Med. 2015, 19, 714–718. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Park, K. Acute Toxicity of Benzalkonium Chloride in Balb/c Mice Following Intratracheal Instillation and Oral Administration. Environ. Anal. Health Toxicol. 2019, 34, e2019009. [Google Scholar] [CrossRef]
- Wentworth, A.B.; Yiannias, J.A.; Davis, M.D.P.; Killian, J.M. Benzalkonium Chloride: A Known Irritant and Novel Allergen. Dermatitis 2016, 27, 14–20. [Google Scholar] [CrossRef]
- Peyneau, M.; de Chaisemartin, L.; Gigant, N.; Chollet-Martin, S.; Kerdine-Römer, S. Quaternary Ammonium Compounds in Hypersensitivity Reactions. Front. Toxicol. 2022, 4, 973680. [Google Scholar] [CrossRef]
- Migueres, N.; Debaille, C.; Walusiak-Skorupa, J.; Lipińska-Ojrzanowska, A.; Munoz, X.; van Kampen, V.; Suojalehto, H.; Suuronen, K.; Seed, M.; Lee, S.; et al. Occupational Asthma Caused by Quaternary Ammonium Compounds: A Multicenter Cohort Study. J. Allergy Clin. Immunol. Pract. 2021, 9, 3387–3395. [Google Scholar] [CrossRef]
- Lechien, J.R.; Costa De Araujo, P.; De Marrez, L.G.; Halloy, J.-L.; Khalife, M.; Saussez, S. Contact Allergy to Benzalkonium Chloride in Patients Using a Steroid Nasal Spray: A Report of 3 Cases. 2018. Available online: https://www.entjournal.com/print/article/contact-allergy-benzalkonium-chloride-patients-using-steroid-nasal-spray-report-3-cases (accessed on 27 December 2023).
- Gigasept® Instru AF Product Information Sheet. Available online: https://www.schuelke.com/media/products/docs/en/PRI_gigasept_instru_AF_664_EN_062023_06.pdf (accessed on 27 December 2023).
- Obarski, P.; Włodarczyk, J. Diagnosis and Management of Gastrointestinal Chemical Burns and Post-Burn Oesophageal Stenosis. Kardiochir. Torakochirurgia Pol. 2021, 18, 252–259. [Google Scholar] [CrossRef]
- Chen, Y.J.; Seak, C.J.; Kang, S.C.; Chen, T.H.; Chen, C.C.; Ng, C.J.; Lee, C.W.; Su, M.Y.; Huang, H.C.; Chen, P.C.; et al. A New Perspective of the Risk of Caustic Substance Ingestion: The Outcomes of 468 Patients in One North Taiwan Medical Center within 20 Years. Clin. Toxicol. 2021, 59, 409–417. [Google Scholar] [CrossRef]
- Rossi, A. Acute Caustic Ingestion: State of Art and New Trends. J. Gastroenterol. Hepatol. Res. 2015, 4, 1501–1506. [Google Scholar] [CrossRef]
- Meena, B.L.; Narayan, K.S.; Goyal, G.; Sultania, S.; Nijhawan, S. Corrosive Injuries of the Upper Gastrointestinal Tract. J. Dig. Endosc. 2017, 8, 165–169. [Google Scholar] [CrossRef]
- Chirica, M.; Bonavina, L.; Kelly, M.D.; Sarfati, E.; Cattan, P. Caustic Ingestion. Lancet 2017, 389, 2041–2052. [Google Scholar] [CrossRef] [PubMed]
- Caganova, B.; Foltanova, T.; Plackova, S.; Placha, K.; Bibza, J.; Puchon, E.; Ondriasova, E.; Batora, I. Caustic Effects of Chemicals: Risk Factors for Complications and Mortality in Acute Poisoning. Monatsh. Chem. 2017, 148, 497–503. [Google Scholar] [CrossRef]
- Sharif, A.F.; Gameel, D.E.G.E.; Abdo, S.A.E.-F.; Elgebally, E.I.; Fayed, M.M. Evaluation of Pediatric Early Warning System and Drooling Reluctance Oropharynx Others Leukocytosis Scores as Prognostic Tools for Pediatric Caustic Ingestion: A Two-Center, Cross-Sectional Study. Environ. Sci. Pollut. Res. 2022, 29, 5378–5395. [Google Scholar] [CrossRef]
- Hall, A.H.; Jacquemin, D.; Henny, D.; Mathieu, L.; Josset, P.; Meyer, B. Corrosive Substances Ingestion: A Review. Crit. Rev. Toxicol. 2019, 49, 637–669. [Google Scholar] [CrossRef] [PubMed]
- Oliva, S.; Romano, C.; De Angelis, P.; Isoldi, S.; Mantegazza, C.; Felici, E.; Dabizzi, E.; Fava, G.; Renzo, S.; Strisciuglio, C.; et al. Foreign Body and Caustic Ingestions in Children: A Clinical Practice Guideline: Foreign Bodies and Caustic Ingestions in Children. Dig. Liver Dis. 2020, 52, 1266–1281. [Google Scholar] [CrossRef] [PubMed]
- Usta, M.; Erkan, T.; Cokugras, F.C.; Urganci, N.; Onal, Z.; Gulcan, M.; Kutlu, T. High Doses of Methylprednisolone in the Management of Caustic Esophageal Burns. Pediatrics 2014, 133, e1518–e1524. [Google Scholar] [CrossRef] [PubMed]
- Tringali, A.; Thomson, M.; Dumonceau, J.M.; Tavares, M.; Tabbers, M.M.; Furlano, R.; Spaander, M.; Hassan, C.; Tzvinikos, C.; Ijsselstijn, H.; et al. Pediatric Gastrointestinal Endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) Guideline Executive Summary. Endoscopy 2017, 49, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Ali Zargar, S.; Kochhar, R.; Mehta, S.; Kumar Mehta, S. The Role of Fiberoptic Endoscopy in the Management of Corrosive Ingestion and Modified Endoscopic Classification of Burns. Gastrointest. Endosc. 1991, 37, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Mantho, P.; Engbang, J.P.; Ndzana Awono, C.D.; Essola, B.; Kamguep, T.; Noah Noah, D.; Ngowe Ngowe, M. Caustic Esophageal Strictures in Children: Diagnosis, Treatment and Evolution in the City of Douala. J. Surg. Res. 2022, 5, 486–493. [Google Scholar] [CrossRef]
- Demirören, K.; Kocamaz, H.; Doğan, Y. Gastrointestinal System Lesions in Children Due to the Ingestion of Alkali and Acid Corrosive Substances. Turk. J. Med. Sci. 2015, 45, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Ollandzobo, L.C.A.-I.I.; Ahoui-Apendi, C.; Mimiesse-Monamou, J.F.; Babela, J.R.M.; Deby-Gassaye; Ibara, B.I.A.; Ibara, J.-R. Ingestion of Caustics by Children in Brazzaville (CONGO). Open J. Pediatr. 2018, 8, 283–291. [Google Scholar] [CrossRef]
- Alser, O.; Hamouri, S.; Novotny, N.M. Esophageal Caustic Injuries in Pediatrics: A Sobering Global Health Issue. Asian Cardiovasc. Thorac. Ann. 2019, 27, 431–435. [Google Scholar] [CrossRef]
- Niedzielski, A.; Schwartz, S.G.; Partycka-Pietrzyk, K.; Mielnik-Niedzielska, G. Caustic Agents Ingestion in Children: A 51-Year Retrospective Cohort Study. Ear Nose Throat J. 2020, 99, 52–57. [Google Scholar] [CrossRef]
- Nardo, G.D.; Betalli, P.; Illiceto, M.T.; Giulia, G.; Martemucci, L.; Caruso, F.; Lisi, G.; Romano, G.; Villa, M.P.; Ziparo, C.; et al. Caustic Ingestion in Children: 1 Year Experience in 3 Italian Referral Centers. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 19–22. [Google Scholar] [CrossRef]
- Elkaramany, M. An Overview of Corrosive Injury of the Upper Gastrointestinal Tract: Discussion of Types, Clinical Evaluation, and Management Procedures. Adv. Dig. Med. 2018, 5, 115–120. [Google Scholar] [CrossRef]
- Kumar, A.; Chetiwal, R.; Rastogi, P.; Tanwar, S.; Gupta, S.; Patnaik, R.; Vankayalapati, M.; Gupta, S.; Arya, A. Severe Esophagitis and Chemical Pneumonitis as a Consequence of Dilute Benzalkonium Chloride Ingestion: A Case Report. Int. J. Med. Stud. 2021, 9, 231–234. [Google Scholar] [CrossRef]
- Spiller, H.A. A Case of Fatal Ingestion of a 10% Benzalkonium Chloride Solution. J. Forensic Toxicol. Pharmacol. 2014, 3, 1000113. [Google Scholar] [CrossRef]
- Wilson, J.T. Benzalkonium Chloride Poisoning in Infant Twins. Arch. Pediatr. Adolesc. Med. 1975, 129, 1208. [Google Scholar] [CrossRef] [PubMed]
- Bekdas, M.; Ozturk, S.; Kara, B.; Acar, S.; Ozturk, H. An Unpleasant Result of Imprecision: Esophageal Corrosive Injury Due to the Oral Intake of 10% Benzalkonium Chloride. Br. J. Med. Med. Res. 2016, 14, 1–4. [Google Scholar] [CrossRef]
- Civan, H.A.; Gulcu, D.; Erkan, T. Corrosive Esophagitis with Benzalkonium Chloride in a Two Days Old Neonate. Pediatr. Gastroenterol. Hepatol. Nutr. 2016, 19, 207–209. [Google Scholar] [CrossRef]
- Turan, C.; Özkan, U.; Özokutan, B.H.; Özdemir, M.; Okur, H.; Küçükaydın, M. Corrosive Injuries of the Esophagus in Newborns. Pediatr. Surg. Int. 2000, 16, 483–484. [Google Scholar] [CrossRef] [PubMed]
- Okan, F.; Coban, A.; Ince, Z.; Can, G. A Rare and Preventable Cause of Respiratory Insufficiency Ingestion of Benzalkonium Chloride. Pediatr. Emerg. Care 2007, 23, 404–406. [Google Scholar] [CrossRef]
- Amigoni, M.; Bellani, G.; Zambelli, V.; Scanziani, M.; Farina, F.; Fagnani, L.; Latini, R.; Fumagalli, R.; Pesenti, A. Unilateral Acid Aspiration Augments the Effects of Ventilator Lung Injury in the Contralateral Lung. Anesthesiology 2013, 119, 642–651. [Google Scholar] [CrossRef]
- Chirica, M.; Kelly, M.D.; Siboni, S.; Aiolfi, A.; Riva, C.G.; Asti, E.; Ferrari, D.; Leppäniemi, A.; Ten Broek, R.P.G.; Brichon, P.Y.; et al. Esophageal Emergencies: WSES Guidelines. World J. Emerg. Surg. 2019, 14, 26. [Google Scholar] [CrossRef]
- Arnold, W.A.; Blum, A.; Branyan, J.; Bruton, T.A.; Carignan, C.C.; Cortopassi, G.; Datta, S.; DeWitt, J.; Doherty, A.C.; Halden, R.U.; et al. Quaternary Ammonium Compounds: A Chemical Class of Emerging Concern. Environ. Sci. Technol. 2023, 57, 7645–7665. [Google Scholar] [CrossRef]
- Park, E.J.; Jin, S.W.; Kang, M.S.; Yang, M.J.; Kim, S.H.; Han, H.Y.; Kang, J.W. Pulmonary inflammation and cellular responses following exposure to benzalkonium chloride: Potential impact of disrupted pulmonary surfactant homeostasis. Toxicol. Appl. Pharmacol. 2022, 440, 115930. [Google Scholar] [CrossRef]
- DeLeo, P.C.; Tu, V.; Fuls, J. Systemic absorption of benzalkonium chloride after maximal use of a consumer antiseptic wash product. Regul. Toxicol. Pharmacol. 2021, 124, 104978. [Google Scholar] [CrossRef] [PubMed]
- Barber, O.W.; Hartmann, E.M. Benzalkonium chloride: A systematic review of its environmental entry through wastewater treatment, potential impact, and mitigation strategies. Crit. Rev. Environ. Sci. Technol. 2022, 52, 2691–2719. [Google Scholar] [CrossRef]
- Sekijima, H.; Oshima, T.; Ueji, Y.; Kuno, N.; Kondo, Y.; Nomura, S.; Asakura, T.; Sakai-Sugino, K.; Kawano, M.; Komada, H.; et al. Toxicologic pathological mechanism of acute lung injury induced by oral administration of benzalkonium chloride in mice. Toxicol. Res. 2023, 39, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, S.; Yutao, L.; Goh, S.G.; Ng, C.; Luhua, Y.; Tran, N.H.; Gin, K.Y. Quaternary ammonium compounds of emerging concern: Classification, occurrence, fate, toxicity and antimicrobial resistance. J. Hazard. Mater. 2023, 445, 130393. [Google Scholar] [CrossRef]
- Johnson, N.F. Pulmonary Toxicity of Benzalkonium Chloride. J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 1–17. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active ingredients: | 15.6% Cocospropylene diamine–guanidine diacetate |
| 35% Phenoxypropanols | |
| 2.5% Benzalkonium chloride | |
| pH: | 9.1–9.5 |
| Density: | 0.99 g/cm3 |
| Viscosity: | 30 mPa*s |
| Okan [49] | Civan [47] | Wilson [45] | Wilson [45] | Bekdas [46] | Kumar [43] | Tambuzzi [16] | Spiller [44] | |
|---|---|---|---|---|---|---|---|---|
| Age | 2 days | 2 days | 2 months | 2 months | 2 months | 42 years | 61 years | 78 years |
| Sex | F | F | M | F | M | M | F | M |
| Intentional | No | No | No | No | No | No | Yes | Yes |
| Concentration (%) | 10 | 10 | 11 | 11 | 10 | <10 | 10 | 10 |
| Esophageal corrosive injury | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Lung injury | Yes | No | Yes | No | Yes | Yes | Yes | Yes |
| Received corticoids | Yes | No | No | No | Yes | Yes | Yes | Unknown |
| Received antibiotics | Yes | Yes | Yes | No | Yes | Yes | No | Unknown |
| Outcome | Favorable | Favorable | Favorable | Favorable | Favorable | Favorable | Deceased | Deceased |
| Sequels | No | Unknown | No | No | No | No | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nițescu, V.; Lescaie, A.; Boghițoiu, D.; Ulmeanu, C. Benzalkonium Chloride Poisoning in Pediatric Patients: Report of Case with a Severe Clinical Course and Literature Review. Toxics 2024, 12, 139. https://doi.org/10.3390/toxics12020139
Nițescu V, Lescaie A, Boghițoiu D, Ulmeanu C. Benzalkonium Chloride Poisoning in Pediatric Patients: Report of Case with a Severe Clinical Course and Literature Review. Toxics. 2024; 12(2):139. https://doi.org/10.3390/toxics12020139
Chicago/Turabian StyleNițescu, Viorela, Andreea Lescaie, Dora Boghițoiu, and Coriolan Ulmeanu. 2024. "Benzalkonium Chloride Poisoning in Pediatric Patients: Report of Case with a Severe Clinical Course and Literature Review" Toxics 12, no. 2: 139. https://doi.org/10.3390/toxics12020139