
Adverse Associations of Long-Term Exposure to PM2.5 and Its Components with Platelet Traits among Subway Shift-Workers without Air Purifier Use


Abstract
1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Assessment of Shift Work and Air Purifier Use
2.3. Estimated Concentrations of PM2.5 and Its Components
2.4. Platelet Parameters Measurements
2.5. Covariates’ Assessment
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Individual Associations of PM2.5 and Its Components with Platelet Parameters
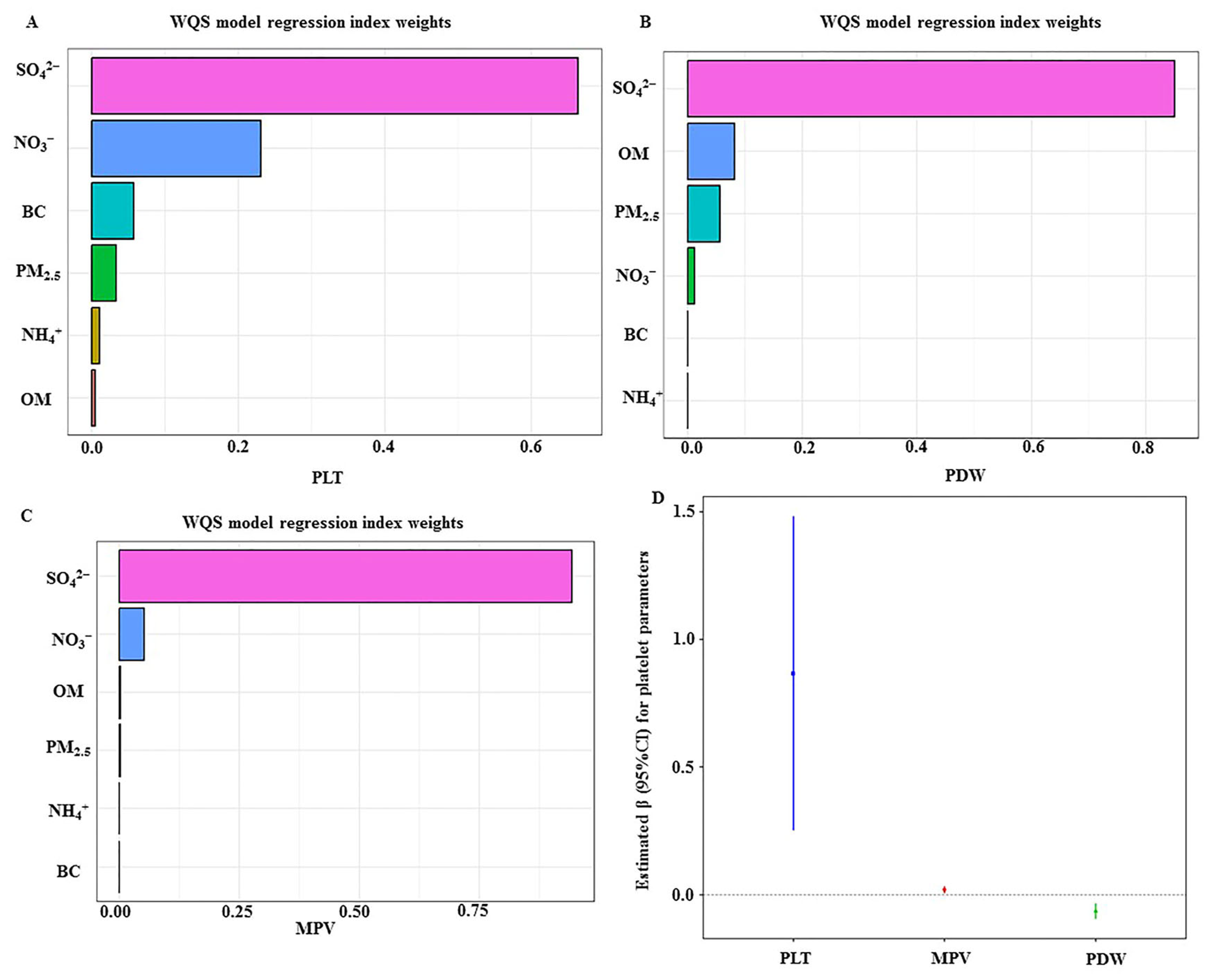
3.3. The Mixture of PM2.5 and Its Components with Platelet Parameters
3.4. The Individual and Mixture of PM2.5 and Its Components with Platelet Parameters by Air Purifier and Shift Work
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Diabetes and Air Pollution Collaborators. Estimates, trends, and drivers of the global burden of type 2 diabetes attributable to PM(2.5) air pollution, 1990–2019: An analysis of data from the Global Burden of Disease Study 2019. Lancet Planet Health 2022, 6, e586–e600. [Google Scholar] [CrossRef] [PubMed]
- Sang, S.; Chu, C.; Zhang, T.; Chen, H.; Yang, X. The global burden of disease attributable to ambient fine particulate matter in 204 countries and territories, 1990–2019: A systematic analysis of the Global Burden of Disease Study 2019. Ecotoxicol. Environ. Saf. 2022, 238, 113588. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Guo, B.; Jiang, Y.; Wang, X.; Chen, L.; Wang, X.; Chen, T.; Yang, L.; Silang, Y.; Hong, F.; et al. Long-term Exposure to Ambient PM2.5 and Its Components Associated With Diabetes: Evidence From a Large Population-Based Cohort From China. Diabetes Care 2023, 46, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Pan, R.; Wang, J.; Chang, W.W.; Song, J.; Yi, W.; Zhao, F.; Zhang, Y.; Fang, J.; Du, P.; Cheng, J.; et al. Association of PM2.5 Components with Acceleration of Aging: Moderating Role of Sex Hormones. Environ. Sci. Technol. 2023, 57, 3772–3782. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P.L.S.; Andersson, N.; Stockfelt, L.; Andersson, E.M.; Nilsson Sommar, J.; Eneroth, K.; Gidhagen, L.; Johansson, C.; Lager, A.; Leander, K.; et al. Long-Term Exposure to Particulate Air Pollution, Black Carbon, and Their Source Components in Relation to Ischemic Heart Disease and Stroke. Environ. Health Perspect. 2019, 127, 107012. [Google Scholar] [CrossRef] [PubMed]
- Poursafa, P.; Kelishadi, R. Air pollution, platelet activation and atherosclerosis. Inflamm. Allergy Drug Targets 2010, 9, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Lippmann, M. Toxicological and epidemiological studies of cardiovascular effects of ambient air fine particulate matter (PM2.5) and its chemical components: Coherence and public health implications. Crit. Rev. Toxicol. 2014, 44, 299–347. [Google Scholar] [CrossRef]
- Wang, S.; Kaur, M.; Li, T.; Pan, F. Effect of Different Pollution Parameters and Chemical Components of PM2.5 on Health of Residents of Xinxiang City, China. Int. J. Environ. Res. Public. Health. 2021, 18, 6821. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Duan, Y.; Liu, X.; Li, R.; Tu, R.; Pan, M.; Dong, X.; Mao, Z.; Huo, W.; Chen, G.; et al. Associations of long-term exposure to air pollutants, physical activity and platelet traits of cardiovascular risk in a rural Chinese population. Sci. Total Environ. 2020, 738, 140182. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Hou, J.; Zhou, Y.; Hu, C.; Sun, H.; Chen, W.; Yuan, J. Dose-response relationships between polycyclic aromatic hydrocarbons exposure and platelet indices. Environ. Pollut. 2019, 245, 183–198. [Google Scholar] [CrossRef]
- Cui, J.; Zhang, T.; Zhang, C.; Xue, Z.; Chen, D.; Kong, X.; Zhao, C.; Guo, Y.; Li, Z.; Liu, X.; et al. Long-term exposure to low concentrations of polycyclic aromatic hydrocarbons and alterations in platelet indices: A longitudinal study in China. PLoS ONE 2022, 17, e0276944. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S. Particulate matter air pollution and atherosclerosis. Curr. Atheroscler. Rep. 2010, 12, 291–300. [Google Scholar] [CrossRef]
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The mechanisms of air pollution and particulate matter in cardiovascular diseases. Heart Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Furuyama, A.; Hirano, S.; Koike, E.; Kobayashi, T. Induction of oxidative stress and inhibition of plasminogen activator inhibitor-1 production in endothelial cells following exposure to organic extracts of diesel exhaust particles and urban fine particles. Arch. Toxicol. 2006, 80, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Konca, C.; Tekin, M.; Colak, P.; Uckardes, F.; Turgut, M. An overview of platelet indices for evaluating platelet function in children with scorpion envenomation. EXCLI J. 2014, 13, 801–808. [Google Scholar] [PubMed]
- Yin, W.; Hou, J.; Xu, T.; Cheng, J.; Wang, X.; Jiao, S.; Wang, L.; Huang, C.; Zhang, Y.; Yuan, J. Association of individual-level concentrations and human respiratory tract deposited doses of fine particulate matter with alternation in blood pressure. Environ. Pollut. 2017, 230, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Viehmann, A.; Hertel, S.; Fuks, K.; Eisele, L.; Moebus, S.; Möhlenkamp, S.; Nonnemacher, M.; Jakobs, H.; Erbel, R.; Jöckel, K.H.; et al. Long-term residential exposure to urban air pollution, and repeated measures of systemic blood markers of inflammation and coagulation. Occup. Environ. Med. 2015, 72, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Chan, T.-C.; Guo, C.; Chang, L.-y.; Lin, C.; Chuang, Y.C.; Jiang, W.K.; Ho, K.F.; Tam, T.; Woo, K.S. Long-term exposure to ambient particulate matter (PM2.5) is associated with platelet counts in adults. Environ. Pollut. 2018, 240, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Huo, X.; Cheng, Z.; Wang, Q.; Zhang, Y.; Xu, X. Alterations in platelet indices link polycyclic aromatic hydrocarbons toxicity to low-grade inflammation in preschool children. Environ. Int. 2019, 131, 105043. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Al-Kindi, S.G.; Brook, R.D. Air pollution and cardiovascular disease: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2018, 72, 2054–2070. [Google Scholar] [CrossRef]
- Hadei, M.; Naddafi, K. Cardiovascular effects of airborne particulate matter: A review of rodent model studies. Chemosphere 2019, 242, 125204. [Google Scholar] [CrossRef]
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Rosa, D.; Terzoni, S.; Dellafiore, F.; Destrebecq, A. Systematic review of shift work and nurses’ health. Occup. Med. 2019, 69, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Puttonen, S.; Viitasalo, K.; Härmä, M. Effect of shiftwork on systemic markers of inflammation. Chronobiol. Int. 2011, 28, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Morikawa, Y.; Kitaoka, K.; Nakamura, K.; Sakurai, M.; Nishijo, M.; Hamazaki, Y.; Maruzeni, S.; Nakagawa, H. Effects of fatigue on immune function in nurses performing shift work. J. Occup. Health 2011, 53, 312–319. [Google Scholar] [CrossRef]
- Nakao, T.; Yasumoto, A.; Tokuoka, S.; Kita, Y.; Kawahara, T.; Daimon, M.; Yatomi, Y. The impact of night-shift work on platelet function in healthy medical staff. J. Occup. Health 2018, 60, 324–332. [Google Scholar] [CrossRef]
- Liu, K.; Cao, H.; Li, B.; Guo, C.; Zhao, W.; Han, X.; Zhang, H.; Wang, Z.; Tang, N.; Niu, K.; et al. Long-term exposure to ambient nitrogen dioxide and ozone modifies systematic low-grade inflammation: The CHCN-BTH study. Int. J. Hyg. Environ. Health 2022, 239, 113875. [Google Scholar] [CrossRef]
- Wittkopp, S.; Walzer, D.; Thorpe, L.; Roberts, T.; Xia, Y.; Gordon, T.; Thurston, G.; Brook, R.; Newman, J.D. Portable air cleaner use and biomarkers of inflammation: A systematic review and meta-analysis. Am. Heart J. Plus 2022, 18, 100182. [Google Scholar] [CrossRef]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kamińska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 9213074. [Google Scholar] [CrossRef]
- Daniluk, U.; Filimoniuk, A.; Kowalczuk-Krystoń, M.; Alifier, M.; Karpińska, J.; Kaczmarski, M.G.; Lebensztejn, D.M. Association of antioxidants and vitamin D level with inflammation in children with atopic dermatitis. Int. J. Dermatol. 2019, 58, 1056–1061. [Google Scholar] [CrossRef]
- Liu, S.; Geng, G.; Xiao, Q.; Zheng, Y.; Liu, X.; Cheng, J.; Zhang, Q. Tracking Daily Concentrations of PM2.5 Chemical Composition in China since 2000. Environ. Sci. Technol. 2022, 56, 16517–16527. [Google Scholar] [CrossRef] [PubMed]
- Geng, G.; Zhang, Q.; Tong, D.; Li, M.; Zheng, Y.; Wang, S.; He, K. Chemical composition of ambient PM2.5 over China and relationship to precursor emissions during 2005–2012. Atmos Chem. Phys. 2017, 17, 9187–9203. [Google Scholar] [CrossRef]
- Barua, R.S.; Rigotti, N.A.; Benowitz, N.L.; Cummings, K.M.; Jazayeri, M.A.; Morris, P.B.; Ratchford, E.V.; Sarna, L.; Stecker, E.C.; Wiggins, B.S. 2018 ACC Expert Consensus Decision Pathway on Tobacco Cessation Treatment: A Report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J. Am. Coll. Cardiol. 2018, 72, 3332–3365. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Liu, X.; Tu, R.; Dong, X.; Zhai, Z.; Mao, Z.; Huo, W.; Chen, G.; Xiang, H.; Guo, Y. Long-term exposure to ambient air pollution attenuated the association of physical activity with metabolic syndrome in rural Chinese adults: A cross-sectional study. Environ. Int. 2020, 136, 105459. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Gao, X.; Cao, Y.; Chen, Y.; Cui, Q.; Deng, F.; Yang, B.; Lin, E.Z.; Fang, J.; Li, T.; et al. Personal airborne chemical exposure and epigenetic ageing biomarkers in healthy Chinese elderly individuals: Evidence from mixture approaches. Environ. Int. 2022, 170, 107614. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Guo, T.; Guo, H.; Chen, X.; Ma, Y.; Deng, H.; Yu, H.; Chen, Q.; Li, H.; Liu, Q.; et al. Ambient particulate air pollution, blood cell parameters, and effect modification by psychosocial stress: Findings from two studies in three major Chinese cities. Environ. Res. 2022, 210, 112932. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Jia, X.; Cui, L.; Liu, J.; Chen, J.; Wang, Y.; Niu, W.; Xu, J.; Miller, M.R.; Loh, M.; et al. Exposure to fine particulate matter promotes platelet activation and thrombosis via obesity-related inflammation. J. Hazard. Mater. 2021, 413, 125341. [Google Scholar] [CrossRef]
- Zhu, X.; Zhao, P.; Lu, Y.; Huo, L.; Bai, M.; Yu, F.; Tie, Y. Potential injurious effects of the fine particulate PM2.5 on the progression of atherosclerosis in apoE-deficient mice by activating platelets and leukocytes. Arch. Med. Sci. 2019, 15, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Santo Salvatore, S.; Gea, O.C.; Antonella, Z.; Andrea, B.; Maria, F.; Margherita, F. Effect of particulate matter-bound metals exposure on prothrombotic biomarkers: A systematic review. Environ. Res. 2019, 177, 108573. [Google Scholar]
- Fu, S.; Liu, L.; Zhang, X.; Liu, Z.-P.; Wang, R.-T. Platelet indices in laryngeal cancer. Cancer Biomark. 2018, 21, 675–680. [Google Scholar] [CrossRef]
- Dubey, S.; Rohra, H.; Taneja, A. Assessing effectiveness of air purifiers (HEPA) for controlling indoor particulate pollution. Heliyon 2021, 7, e07976. [Google Scholar] [CrossRef]
- Liu, Y.; Zhou, B.; Wang, J.; Zhao, B. Health benefits and cost of using air purifiers to reduce exposure to ambient fine particulate pollution in China. J. Hazard. Mater. 2021, 414, 125540. [Google Scholar] [CrossRef] [PubMed]
- Hansel, N.N.; Putcha, N.; Woo, H.; Peng, R.; Diette, G.B.; Fawzy, A.; Wise, R.A.; Romero, K.; Davis, M.F.; Rule, A.M.; et al. Randomized Clinical Trial of Air Cleaners to Improve Indoor Air Quality and Chronic Obstructive Pulmonary Disease Health: Results of the CLEAN AIR Study. Am. J. Respir. Crit. Care Med. 2022, 205, 421–430. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, Y.; Huang, X.; Rong, Y.; He, M.; Wang, Y.; Yuan, J.; Wu, T.; Chen, W. The effects of shift work on sleeping quality, hypertension and diabetes in retired workers. PLoS ONE 2013, 8, e71107. [Google Scholar] [CrossRef] [PubMed]
- Repsold, L.; Joubert, A.M. Platelet Function, Role in Thrombosis, Inflammation, and Consequences in Chronic Myeloproliferative Disorders. Cells 2021, 10, 3034. [Google Scholar] [CrossRef]
- Velazquez-Kronen, R.; MacDonald, L.A.; Akinyemiju, T.F.; Cushman, M.; Howard, V.J. Shiftwork, long working hours and markers of inflammation in a national US population-based sample of employed black and white men and women aged ≥45 years. Occup. Environ. Med. 2023, 80, 635–643. [Google Scholar] [CrossRef] [PubMed]
- El-Benhawy, S.A.; El-Tahan, R.A.; Nakhla, S.F. Exposure to Radiation During Work Shifts and Working at Night Act as Occupational Stressors Alter Redox and Inflammatory Markers. Arch. Med. Res. 2021, 52, 76–83. [Google Scholar] [CrossRef]
- Atwater, A.Q.; Castanon-Cervantes, O. Uncovering Novel Biomarkers of Inflammation as Potential Screening Targets of Disease Risk in Healthcare Shift Workers: A Pilot Study. Int. J. Nurs. Health Care Res. 2023, 6, 1466. [Google Scholar]
- Zhang, H.L.; Hu, J.L.; Kleeman, M.; Ying, Q. Source apportionment of sulfate and nitrate particulate matter in the Eastern United States and effectiveness of emission control programs. Sci. Total Environ. 2014, 490, 171–181. [Google Scholar] [CrossRef]
- Goobie, G.C.; Carlsten, C.; Johannson, K.A.; Khalil, N.; Marcoux, V.; Assayag, D.; Manganas, H.; Fisher, J.H.; Kolb, M.R.J.; Lindell, K.O.; et al. Association of Particulate Matter Exposure With Lung Function and Mortality Among Patients With Fibrotic Interstitial Lung Disease. JAMA Intern. Med. 2022, 182, 1248–1259. [Google Scholar] [CrossRef]
- Han, B.; Xu, J.; Zhang, Y.; Li, P.; Li, K.; Zhang, N.; Han, J.; Gao, S.; Wang, X.; Geng, C.; et al. Associations of Exposure to Fine Particulate Matter Mass and Constituents with Systemic Inflammation: A Cross-Sectional Study of Urban Older Adults in China. Environ. Sci. Technol. 2022, 56, 7244–7255. [Google Scholar] [CrossRef] [PubMed]
- Yi, W.; Zhao, F.; Pan, R.; Zhang, Y.; Xu, Z.; Song, J.; Sun, Q.; Du, P.; Fang, J.; Cheng, J.; et al. Associations of Fine Particulate Matter Constituents with Metabolic Syndrome and the Mediating Role of Apolipoprotein B: A Multicenter Study in Middle-Aged and Elderly Chinese Adults. Environ. Sci. Technol. 2022, 56, 10161–10171. [Google Scholar] [CrossRef] [PubMed]
- van der Meijden, P.E.J.; Heemskerk, J.W.M. Platelet biology and functions: New concepts and clinical perspectives. Nat. Rev. Cardiol. 2019, 16, 166–179. [Google Scholar] [CrossRef]
- Robertson, S.; Miller, M.R. Ambient air pollution and thrombosis. Part Fibre Toxicol. 2018, 15, 1. [Google Scholar] [CrossRef]
- Chu, S.G.; Becker, R.C.; Berger, P.B.; Bhatt, D.L.; Eikelboom, J.W.; Konkle, B.; Mohler, E.R.; Reilly, M.P.; Berger, J.S. Mean platelet volume as a predictor of cardiovascular risk: A systematic review and meta-analysis. J. Thromb. Haemost. 2010, 8, 148–156. [Google Scholar] [CrossRef]
- Kazensky, L.; Matković, K.; Gerić, M.; Žegura, B.; Pehnec, G.; Gajski, G. Impact of indoor air pollution on DNA damage and chromosome stability: A systematic review. Arch. Toxicol. 2024; online ahead of print. [Google Scholar] [CrossRef]
- Kim, S. Overview of Cotinine Cutoff Values for Smoking Status Classification. Int. J. Environ. Res. Public. Health 2016, 13, 1236. [Google Scholar] [CrossRef]
- Huang, J.; Cai, A.; Wang, W.; He, K.; Zou, S.; Ma, Q. The Variation in Chemical Composition and Source Apportionment of PM2.5 before, during, and after COVID-19 Restrictions in Zhengzhou, China. Toxics 2024, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- Ye, T.; Guo, S.; Xie, Y.; Chen, Z.; Abramson, M.J.; Heyworth, J.; Hales, S.; Woodward, A.; Bell, M.; Guo, Y.; et al. Health and related economic benefits associated with reduction in air pollution during COVID-19 outbreak in 367 cities in China. Ecotoxicol. Environ. Saf. 2021, 222, 112481. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wu, W.; Li, Y.; Li, Y. An investigation of PM2.5 concentration changes in Mid-Eastern China before and after COVID-19 outbreak. Environ. Int. 2023, 175, 107941. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Total Population (n = 8772) | Air Purifier Use | p-Values | Shift-Work | p-Values | ||
|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | ||||
| Age (year, mean ± SD) | 27.2 ± 4.1 | 26.9 ± 4.0 | 28.8 ± 4.4 | <0.001 a | 28.4 ± 5.2 | 26.6 ± 3.4 | <0.001 a |
| Gender (n, %) | <0.001 b | <0.001 b | |||||
| Males | 7024 (80.1) | 6066 (81.2) | 958 (73.4) | 2413 (89.5) | 4602 (75.9) | ||
| Females | 1748 (19.9) | 1400 (18.8) | 348 (26.6) | 284 (10.5) | 1462 (24.1) | ||
| Education level (n, %) | 0.029 b | <0.001 b | |||||
| <17 years | 8615 (98.2) | 7342 (98.3) | 1273 (97.5) | 2549 (94.5) | 6055 (99.9) | ||
| ≥17 years | 157 (1.8) | 124 (1.7) | 33 (2.5) | 148 (5.5) | 9 (0.1) | ||
| Marital status (n, %) | <0.001 b | <0.001 b | |||||
| Married/living together | 3148 (35.9) | 2320 (31.1) | 828 (63.4) | 1145 (42.5) | 1997 (32.9) | ||
| Divorced/widowed/separated/Unmarried | 5624 (64.1) | 5146 (68.9) | 478 (36.6) | 1552 (57.5) | 4067 (67.1) | ||
| Total family income (n, %) | <0.001 b | <0.001 b | |||||
| <100,000 RMB | 3740 (44.0) | 3354 (46.3) | 386 (30.6) | 1136 (43.6) | 2599 (44.1) | ||
| 100,000 RMB | 2479 (29.1) | 2119 (29.2) | 360 (28.6) | 728 (27.9) | 1749 (29.7) | ||
| >150,000 RMB | 2288 (26.9) | 1774 (24.5) | 514 (40.8) | 743 (28.5) | 1541 (26.2) | ||
| Smoking status (n, %) | 0.129 b | 0.003 b | |||||
| Never | 6559 (74.8) | 5603 (75) | 956 (73.2) | 1961 (72.7) | 4591 (75.7) | ||
| Former | 278 (3.2) | 226 (3.0) | 52 (4.0) | 104 (3.9) | 174 (2.9) | ||
| Current | 1935 (22.1) | 1637 (21.9) | 298 (22.8) | 632 (23.4) | 1299 (21.4) | ||
| Drinking status (n, %) | 0.566 b | <0.001 b | |||||
| Never | 7010 (79.9) | 5969 (79.9) | 1041 (79.7) | 2056 (76.2) | 4946 (81.6) | ||
| Former | 175 (2.0) | 144 (1.9) | 31 (2.4) | 74 (2.7) | 100 (1.6) | ||
| Current | 1587 (18.1) | 1353 (18.1) | 234 (17.9) | 567 (21.0) | 1018 (16.8) | ||
| Passive smoking (n, %) | 0.027 b | <0.001 b | |||||
| Yes | 4652 (54.1) | 3998 (54.6) | 654 (51.3) | 1540 (58.2) | 3106 (52.3) | ||
| No | 3940 (45.9) | 3319 (45.4) | 621 (48.7) | 1107 (41.8) | 2828 (47.7) | ||
| Physical activity-MET (h/week, mean ± SD) | 9.1 ± 17.7 | 10.1 ± 19.0 | 8.9 ± 17.5 | 0.004 c | 10.2 ± 17.9 | 8.5 ± 17.6 | <0.001 c |
| Body mass index (kg/m2, mean ± SD) | 23.3 ± 3.7 | 23.8 ± 3.8 | 23.2 ± 3.6 | <0.001 a | 23.7 ± 3.6 | 23.1 ± 3.7 | <0.001 a |
| Dyslipidemia (n, %) | <0.001 b | <0.001 b | |||||
| Yes | 2542 (29.0) | 2106 (28.2) | 436 (33.4) | 873 (32.4) | 1666 (27.5) | ||
| No | 6228 (71.0) | 5359 (71.8) | 869 (66.6) | 1824 (67.6) | 4396 (72.5) | ||
| T2D (n, %) | 0.841 b | 0.020 b | |||||
| Yes | 85 (1.0) | 73 (1.0) | 12 (0.9) | 36 (1.3) | 49 (0.8) | ||
| No | 8687 (99.0) | 7393 (99.0) | 1294 (99.1) | 2661 (98.7) | 6015 (99.2) | ||
| Hypertension (n, %) | 0.247 b | 0.139 b | |||||
| Yes | 912 (10.4) | 788 (10.6) | 124 (9.5) | 299 (11.1) | 609 (10.0) | ||
| No | 7860 (89.6) | 6678 (89.4) | 1182 (90.5) | 2398 (88.9) | 5455 (90.0) | ||
| Platelet parameters | |||||||
| PLT (109/L, median, IQR) | 212 (182, 245) | 212 (181, 244) | 213 (184, 246) | 0.214 c | 211 (180, 244) | 212 (183, 245) | 0.053 c |
| MPV (fL, median, IQR) | 9.2 (8.4, 10) | 9.2 (8.4, 10.0) | 9.3 (8.5, 10.0) | 0.454 c | 9.4 (8.5, 10.1) | 9.2 (8.4, 9.9) | <0.001 b |
| PDW (fL, median, IQR) | 15.4 (11.7, 15.9) | 15.4 (11.7, 15.9) | 15.3 (11.5, 15.9) | 0.015 c | 15.2 (11.5, 15.9) | 15.4 (11.7, 15.9) | 0.009 c |
| Variables | 3-Year Average Concentrations | Spearman Correlation Coefficients | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Minimum | Maximum | IQR | PM2.5 | SO42− | NO3− | NH4+ | OM | BC | |
| PM2.5 (μg/m3) | 56.24 | 53.61 | 46.44 | 75.65 | 9.77 | 1.00 | |||||
| SO42− (μg/m3) | 9.61 | 9.63 | 8.25 | 14.86 | 1.35 | 0.933 ** | 1.00 | ||||
| NO3− (μg/m3) | 11.77 | 11.58 | 10.41 | 18.98 | 1.76 | 0.798 ** | 0.917 ** | 1.00 | |||
| NH4+ (μg/m3) | 7.09 | 6.93 | 6.22 | 12.44 | 1.10 | 0.788 ** | 0.906 ** | 0.990 ** | 1.00 | ||
| OM (μg/m3) | 14.30 | 13.51 | 11.10 | 18.73 | 2.30 | 0.939 ** | 0.790 ** | 0.608 ** | 0.588 ** | 1.00 | |
| BC (μg/m3) | 2.77 | 2.62 | 2.08 | 3.71 | 0.50 | 0.929 ** | 0.771 ** | 0.579 ** | 0.559 ** | 0.994 ** | 1.00 |
| Variables | Model 1 (β, 95%CI) | Model 2 (β, 95%CI) | Model 3 (β, 95%CI) |
|---|---|---|---|
| PLT | |||
| PM2.5 | 13.6 (3.6, 23.6) | 17.2 (7.1, 27.2) | 16.7 (6.7, 26.8) |
| SO42− | 14.2 (4.6, 23.8) | 17.2 (7.5, 26.8) | 16.5 (6.9, 26.2) |
| NO3− | 8.8 (−1.9, 19.5) | 10.9 (0.1, 21.7) | 10.6 (−0.2, 21.4) |
| NH4+ | 7.2 (−3.0, 17.4) | 9.2 (−1.1, 19.4) | 8.8 (−1.4, 19.1) |
| OM | 11.2 (2.3, 20.1) | 14.5 (5.5, 23.5) | 14.2 (5.2, 23.2) |
| BC | 10.9 (2.4, 19.4) | 14.1 (5.5, 22.7) | 13.7 (5.1, 22.3) |
| MPV | |||
| PM2.5 | 0.4 (0.1, 0.6) | 0.3 (0.1, 0.5) | 0.3 (0.1, 0.5) |
| SO42− | 0.5 (0.3, 0.7) | 0.4 (0.2, 0.6) | 0.4 (0.2, 0.6) |
| NO3− | 0.3 (0.1, 0.6) | 0.3 (0.0, 0.5) | 0.3 (0.0, 0.5) |
| NH4+ | 0.3 (0.1, 0.5) | 0.2 (0.0, 0.5) | 0.2 (0.0, 0.5) |
| OM | 0.3 (0.1, 0.5) | 0.2 (0.0, 0.4) | 0.2 (0.0, 0.4) |
| BC | 0.3 (0.1, 0.5) | 0.2 (0.0, 0.4) | 0.2 (0.0, 0.4) |
| PDW | |||
| PM2.5 | −1.2 (−1.7, −0.7) | −1.2 (−1.7, −0.7) | −1.2 (−1.7, −0.7) |
| SO42− | −1.3 (−1.8, −0.9) | −1.3 (−1.8, −0.9) | −1.3 (−1.8, −0.9) |
| NO3− | −1.0 (−1.5, −0.5) | −1.0 (−1.5, −0.4) | −1.0 (−1.5, −0.4) |
| NH4+ | −0.9 (−1.3, −0.4) | −0.8 (−1.3, −0.3) | −0.8 (−1.3, −0.3) |
| OM | −0.9 (−1.4, −0.5) | −1.0 (−1.4, −0.5) | −1.0 (−1.4, −0.5) |
| BC | −0.9 (−1.3, −0.5) | −0.9 (−1.4, −0.5) | −0.9 (−1.4, −0.5) |
| Variables | PLT a (β, 95%CI) | MPV a (β, 95%CI) | PDW a (β, 95%CI) |
|---|---|---|---|
| Usage of air purifiers | |||
| PM2.5 | 9.4 (−16.6, 35.3) | 0.0 (−0.6, 0.6) | −0.4 (−1.7, 0.8) |
| SO42− | 13.7 (−11.5, 38.8) | 0.1 (−0.5, 0.6) | −0.5 (−1.8, 0.7) |
| NO3− | 18.2 (−10.6, 47.1) | −0.2 (−0.8, 0.5) | −0.7 (−2.1, 0.6) |
| NH4+ | 14.4 (−13.2, 42.1) | −0.1 (−0.7, 0.5) | −0.7 (−2.0, 0.7) |
| OM | 5.3 (−18.0, 28.6) | 0.0 (−0.5, 0.5) | −0.3 (−1.4, 0.8) |
| BC | 4.6 (−17.7, 27.0) | 0.0 (−0.5, 0.5) | −0.2 (−1.3, 0.8) |
| Non-usage of air purifiers | |||
| PM2.5 | 16.7 (6.6, 26.7) | 0.3 (0.1, 0.5) | −1.2 (−1.7, −0.7) |
| SO42− | 16.5 (6.9, 26.1) | 0.4 (0.2, 0.6) | −1.3 (−1.8, −0.9) |
| NO3− | 10.6 (−0.2, 21.3) | 0.3 (0.0, 0.5) | −1.0 (−1.5, −0.4) |
| NH4+ | 8.8 (−1.5, 19.1) | 0.2 (0.0, 0.5) | −0.8 (−1.3, −0.3) |
| OM | 14.1 (5.2, 23.1) | 0.2 (0.0, 0.4) | −1.0 (−1.4, −0.5) |
| BC | 13.7 (5.1, 22.3) | 0.2 (0.0, 0.4) | −0.9 (−1.4, −0.5) |
| Variables | PLT a (β, 95%CI) | MPV a (β, 95%CI) | PDW a (β, 95%CI) |
|---|---|---|---|
| Shift work (Yes) | |||
| PM2.5 | 20.9 (8.7, 33.1) | 0.39 (0.11, 0.66) | −1.37 (−1.95, −0.79) |
| SO42− | 21.4 (9.6, 33.2) | 0.50 (0.24, 0.76) | −1.52 (−2.08, −0.96) |
| NO3− | 16.4 (3.3, 29.6) | 0.30 (0.01, 0.59) | −1.14 (−1.76, −0.51) |
| NH4+ | 14.4 (1.9, 26.9) | 0.26 (−0.01, 0.54) | −0.99 (−1.58, −0.39) |
| OM | 17.1 (6.2, 28.0) | 0.27 (0.03, 0.51) | −1.05 (−1.57, −0.54) |
| BC | 16.1 (5.7, 26.5) | 0.28 (0.05, 0.51) | −1.02 (−1.52, −0.53) |
| Shift work (No) | |||
| PM2.5 | 7.3 (−10.4, 24.9) | 0.04 (−0.38, 0.47) | −0.73 (−1.61, 0.15) |
| SO42− | 6.7 (−10.1, 23.5) | 0.20 (−0.2, 0.61) | −0.76 (−1.6, 0.07) |
| NO3− | −0.7 (−19.5, 18) | 0.10 (−0.36, 0.55) | −0.45 (−1.38, 0.48) |
| NH4+ | −2 (−19.9, 15.8) | 0.08 (−0.35, 0.51) | −0.35 (−1.24, 0.54) |
| OM | 6.8 (−9.2, 22.7) | −0.04 (−0.42, 0.35) | −0.58 (−1.37, 0.21) |
| BC | 7.5 (−7.8, 22.8) | −0.03 (−0.4, 0.34) | −0.59 (−1.35, 0.17) |
| Variables | PLT (β, 95%CI) a | MPV (β, 95%CI) a | PDW (β, 95%CI) a |
|---|---|---|---|
| Total population a | 0.6925 (0.196, 1.1889) | 0.0124 (0.0014, 0.0233) | −0.0568 (−0.0802, −0.0333) |
| Usage of air purifier b | −0.376 (−1.6725, 0.9206) | 0.0022 (−0.0249, 0.0292) | −0.0204 (−0.0812, 0.0404) |
| Non-usage of air purifier b | 0.7886 (0.2471, 1.3301) | 0.0111 (−0.0005, 0.0227) | −0.0513 (−0.0762, −0.0264) |
| Total populationc | 0.7961 (0.2911, 1.3011) | 0.0173 (0.006, 0.0287) | −0.0551 (−0.0842, −0.026) |
| Shift work (Yes) | 1.0441 (0.4300, 1.6582) | 0.0127 (−0.0004, 0.0258) | −0.0204 (−0.0812, 0.0404) |
| Shift work (No) | 0.1133 (−0.7545, 0.9812) | 0.0073 (−0.0137, 0.0284) | −0.0080 (−0.0516, 0.0357) |
| Shift-Work | Air Purifier Use | PLT a (β, 95%CI) | MPV a (β, 95%CI) | PDW a (β, 95%CI) |
|---|---|---|---|---|
| Yes | Yes | |||
| PM2.5 | 14.9 (−19.2, 49) | 0.04 (−0.65, 0.73) | −0.44 (−1.98, 1.10) | |
| SO42− | 18 (−14.8, 50.8) | 0.01 (−0.65, 0.68) | −0.45 (−1.93, 1.03) | |
| NO3− | 21.3 (−15.6, 58.1) | −0.30 (−1.05, 0.45) | −0.41 (−2.07, 1.26) | |
| NH4+ | 16.9 (−18.3, 52.1) | −0.27 (−0.98, 0.44) | −0.33 (−1.93, 1.26) | |
| OM | 10.4 (−20.2, 41) | 0.05 (−0.57, 0.67) | −0.36 (−1.75, 1.02) | |
| BC | 9.5 (−19.8, 38.8) | 0.10 (−0.50, 0.69) | −0.35 (−1.68, 0.97) | |
| No | Yes | |||
| PM2.5 | 1.3 (−38.2, 40.8) | −0.15 (−1.24, 0.93) | 0.31 (−1.87, 2.49) | |
| SO42− | 7.9 (−30.7, 46.4) | 0.07 (−0.99, 1.12) | −0.08 (−2.22, 2.05) | |
| NO3− | 13.4 (−32.6, 59.4) | −0.04 (−1.3, 1.22) | −0.73 (−3.27, 1.81) | |
| NH4+ | 11 (−33.6, 55.7) | 0.10 (−1.12, 1.32) | −0.69 (−3.16, 1.77) | |
| OM | −2.8 (−38.4, 32.8) | −0.21 (−1.18, 0.77) | 0.49 (−1.47, 2.46) | |
| BC | −3.0 (−37.0, 31.0) | −0.22 (−1.15, 0.71) | 0.56 (−1.31, 2.44) | |
| Yes | No | |||
| PM2.5 | 21.4 (8.2, 34.5) | 0.42 (0.13, 0.72) | −1.47 (−2.1, −0.84) | |
| SO42− | 21.5 (8.8, 34.2) | 0.56 (0.28, 0.85) | −1.65 (−2.26, −1.04) | |
| NO3− | 15.2 (1.1, 29.3) | 0.38 (0.06, 0.70) | −1.21 (−1.88, −0.53) | |
| NH4+ | 13.6 (0.1, 27.0) | 0.33 (0.03, 0.64) | −1.05 (−1.69, −0.40) | |
| OM | 17.7 (6.0, 29.4) | 0.29 (0.02, 0.55) | −1.12 (−1.68, −0.56) | |
| BC | 16.7 (5.6, 27.9) | 0.29 (0.04, 0.54) | −1.09 (−1.62, −0.55) | |
| No | No | |||
| PM2.5 | 8.3 (−11.5, 28.0) | 0.08 (−0.38, 0.55) | −0.88 (−1.84, 0.08) | |
| SO42− | 5.7 (−13.0, 24.3) | 0.24 (−0.20, 0.68) | −0.82 (−1.73, 0.09) | |
| NO3− | −4.5 (−25.1, 16.1) | 0.13 (−0.36, 0.61) | −0.28 (−1.29, 0.72) | |
| NH4+ | −5.4 (−25.0, 14.2) | 0.08 (−0.38, 0.54) | −0.19 (−1.14, 0.76) | |
| OM | 8.9 (−8.9, 26.7) | −0.01 (−0.43, 0.41) | −0.76 (−1.63, 0.11) | |
| BC | 10.0 (−7.1, 27.0) | 0.004 (−0.40, 0.41) | −0.79 (−1.62, 0.04) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Wang, P.; Shang, L.; Ye, F.; Liu, L.; He, Z. Adverse Associations of Long-Term Exposure to PM2.5 and Its Components with Platelet Traits among Subway Shift-Workers without Air Purifier Use. Toxics 2024, 12, 529. https://doi.org/10.3390/toxics12080529
Liu J, Wang P, Shang L, Ye F, Liu L, He Z. Adverse Associations of Long-Term Exposure to PM2.5 and Its Components with Platelet Traits among Subway Shift-Workers without Air Purifier Use. Toxics. 2024; 12(8):529. https://doi.org/10.3390/toxics12080529
Chicago/Turabian StyleLiu, Junling, Pei Wang, Lv Shang, Fang Ye, Li Liu, and Zhenyu He. 2024. "Adverse Associations of Long-Term Exposure to PM2.5 and Its Components with Platelet Traits among Subway Shift-Workers without Air Purifier Use" Toxics 12, no. 8: 529. https://doi.org/10.3390/toxics12080529
APA StyleLiu, J., Wang, P., Shang, L., Ye, F., Liu, L., & He, Z. (2024). Adverse Associations of Long-Term Exposure to PM2.5 and Its Components with Platelet Traits among Subway Shift-Workers without Air Purifier Use. Toxics, 12(8), 529. https://doi.org/10.3390/toxics12080529