
Associations between Ethylene Oxide Exposure and Liver Function in the US Adult Population

 ,
,
Abstract
1. Introduction
2. Materials and Methods
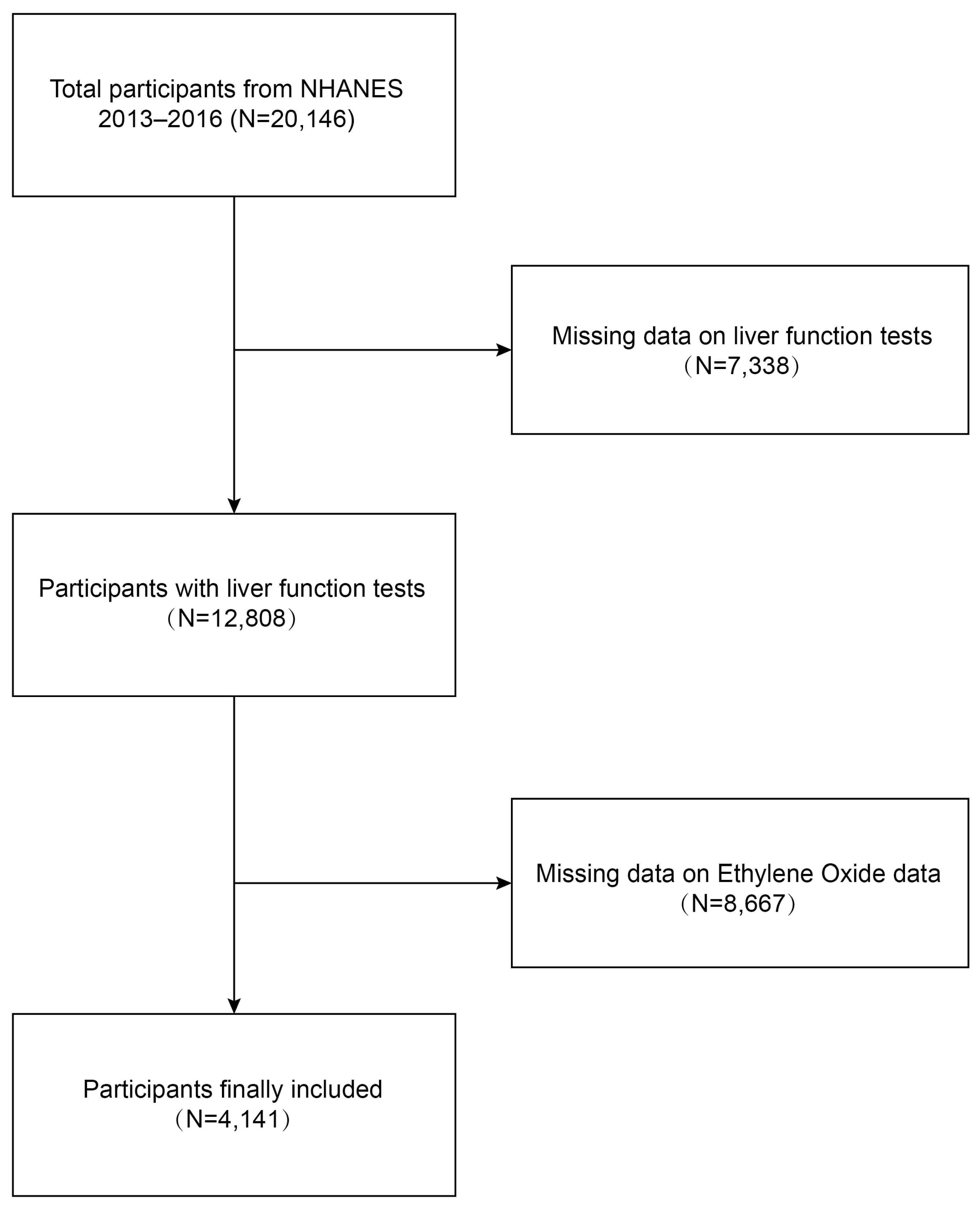
2.1. Study Population
2.2. Assessment of Hemoglobin Ethylene Oxide Levels
2.3. Measurement of Liver Function
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
3.2. Multiple Linear Regression Associations of Ethylene Oxide with LFTs in Adults
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trefts, E.; Gannon, M.; Wasserman, D.H. The liver. Curr. Biol. 2017, 27, R1147–R1151. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Zhao, L.; Li, L. Current understanding of adipose-derived mesenchymal stem cell-based therapies in liver diseases. Stem Cell Res. Ther. 2019, 10, 199. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Guo, R.; Fung, M.L.; Liong, E.C.; Tipoe, G.L. Therapeutic approaches to non-alcoholic fatty liver disease: Past achievements and future challenges. Hepatobiliary Pancreat. Dis. Int. 2013, 12, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Wang, F.; Wong, N.K.; He, J.; Zhang, R.; Sun, R.; Xu, Y.; Liu, Y.; Li, W.; Koike, K.; et al. Global liver disease burdens and research trends: Analysis from a Chinese perspective. J. Hepatol. 2019, 71, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Cramb, R.; Davison, S.M.; Dillon, J.F.; Foulerton, M.; Godfrey, E.M.; Hall, R.; Harrower, U.; Hudson, M.; Langford, A.; et al. Guidelines on the management of abnormal liver blood tests. Gut 2018, 67, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Abeysekera, K.W.M.; Macpherson, I.; Glyn-Owen, K.; McPherson, S.; Parker, R.; Harris, R.; Yeoman, A.; Rowe, I.A.; Dillon, J.F. Community pathways for the early detection and risk stratification of chronic liver disease: A narrative systematic review. Lancet Gastroenterol. Hepatol. 2022, 7, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Yang, M.; Cheng, M.; Fan, L.; Wang, X.; Xu, T.; Wang, B.; Chen, W. Associations between urinary phthalate metabolite concentrations and markers of liver injury in the US adult population. Environ. Int. 2021, 155, 106608. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Song, D.; Shin, S.; Hong, N.; Rhee, Y. Elevated serum γ-glutamyl transferase is associated with low muscle function in adults independent of muscle mass. Nutrition 2022, 103–104, 111813. [Google Scholar] [CrossRef] [PubMed]
- Robles-Diaz, M.; Garcia-Cortes, M.; Medina-Caliz, I.; Gonzalez-Jimenez, A.; Gonzalez-Grande, R.; Navarro, J.M.; Castiella, A.; Zapata, E.M.; Romero-Gomez, M.; Blanco, S.; et al. The value of serum aspartate aminotransferase and gamma-glutamyl transpetidase as biomarkers in hepatotoxicity. Liver Int. 2015, 35, 2474–2482. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Kim, J.; Kim, B.; Park, E.Y. Association between environmental exposure to cadmium and risk of suspected non-alcoholic fatty liver disease. Chemosphere 2021, 266, 128947. [Google Scholar] [CrossRef]
- Sen, P.; Qadri, S.; Luukkonen, P.K.; Ragnarsdottir, O.; McGlinchey, A.; Jäntti, S.; Juuti, A.; Arola, J.; Schlezinger, J.J.; Webster, T.F.; et al. Exposure to environmental contaminants is associated with altered hepatic lipid metabolism in non-alcoholic fatty liver disease. J. Hepatol. 2022, 76, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Yi, W.; Ji, Y.; Gao, H.; Pan, R.; Wei, Q.; Cheng, J.; Song, J.; He, Y.; Tang, C.; Liu, X.; et al. Does the gut microbiome partially mediate the impact of air pollutants exposure on liver function? Evidence based on schizophrenia patients. Environ. Pollut. 2021, 291, 118135. [Google Scholar] [CrossRef] [PubMed]
- Kirman, C.R.; Li, A.A.; Sheehan, P.J.; Bus, J.S.; Lewis, R.C.; Hays, S.M. Ethylene oxide review: Characterization of total exposure via endogenous and exogenous pathways and their implications to risk assessment and risk management. J. Toxicol. Environ. Health B Crit. Rev. 2021, 24, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Lynch, H.N.; Kozal, J.S.; Russell, A.J.; Thompson, W.J.; Divis, H.R.; Freid, R.D.; Calabrese, E.J.; Mundt, K.A. Systematic review of the scientific evidence on ethylene oxide as a human carcinogen. Chem. Biol. Interact. 2022, 364, 110031. [Google Scholar] [CrossRef]
- Vincent, M.J.; Kozal, J.S.; Thompson, W.J.; Maier, A.; Dotson, G.S.; Best, E.A.; Mundt, K.A. Ethylene Oxide: Cancer Evidence Integration and Dose-Response Implications. Dose Response 2019, 17, 1559325819888317. [Google Scholar] [CrossRef] [PubMed]
- Xie, R.; Liu, L.; Liu, C.; Xie, S.; Huang, X.; Zhang, Y. Associations of ethylene oxide exposure and “Life’s Essential 8”. Environ. Sci. Pollut. Res. Int. 2023, 30, 121150–121160. [Google Scholar] [CrossRef] [PubMed]
- Filser, J.G.; Kessler, W.; Artati, A.; Erbach, E.; Faller, T.; Kreuzer, P.E.; Li, Q.; Lichtmannegger, J.; Numtip, W.; Klein, D.; et al. Ethylene oxide in blood of ethylene-exposed B6C3F1 mice, Fischer 344 rats, and humans. Toxicol. Sci. 2013, 136, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Kamalov, M.I.; Lavrov, I.A.; Yergeshov, A.A.; Siraeva, Z.Y.; Baltin, M.E.; Rizvanov, A.A.; Kuznetcova, S.V.; Petrova, N.V.; Savina, I.N.; Abdullin, T.I. Non-invasive topical drug delivery to spinal cord with carboxyl-modified trifunctional copolymer of ethylene oxide and propylene oxide. Colloids Surf. B Biointerfaces 2016, 140, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Grosse, Y.; Baan, R.; Straif, K.; Secretan, B.; El Ghissassi, F.; Bouvard, V.; Altieri, A.; Cogliano, V. Carcinogenicity of 1,3-butadiene, ethylene oxide, vinyl chloride, vinyl fluoride, and vinyl bromide. Lancet Oncol. 2007, 8, 679–680. [Google Scholar] [CrossRef]
- Teta, M.J.; Sielken, R.L., Jr.; Valdez-Flores, C. Ethylene oxide cancer risk assessment based on epidemiological data: Application of revised regulatory guidelines. Risk Anal. 1999, 19, 1135–1155. [Google Scholar] [CrossRef]
- Wu, S.; Yang, Y.M.; Zhu, J.; Wang, L.L.; Xu, W.; Lyu, S.Q.; Wang, J.; Shao, X.H.; Zhang, H. Impact of hemoglobin adducts of ethylene oxide on the prevalence and prognosis of chronic kidney disease in US adults: An analysis from NHANES 2013–2016. Environ. Sci. Pollut. Res. Int. 2024, 31, 2802–2812. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Shi, P.; Chen, Z.; Zhang, W.; Lin, S.; Zheng, T.; Li, M.; Fan, L. The association between ethylene oxide exposure and asthma risk: A population-based study. Environ. Sci. Pollut. Res. Int. 2023, 30, 24154–24167. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Zhao, Y.; Jin, J.; Cheng, M.; Bai, Y.; Xu, J. The association of hemoglobin ethylene oxide levels with albuminuria in US adults: Analysis of NHANES 2013–2016. Environ. Sci. Pollut. Res. Int. 2024, 31, 4130–4139. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Cao, W.; Wang, Y.; Liu, X. Association between blood ethylene oxide levels and the prevalence of hypertension. Environ. Sci. Pollut. Res. Int. 2022, 29, 76937–76943. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.; Liu, M.; Zhang, Y.; Xie, R. Association of family income to poverty ratio and vibration-controlled transient elastography quantified degree of hepatic steatosis in U.S. adolescents. Front. Endocrinol. 2023, 14, 1160625. [Google Scholar] [CrossRef] [PubMed]
- Jinot, J.; Fritz, J.M.; Vulimiri, S.V.; Keshava, N. Carcinogenicity of ethylene oxide: Key findings and scientific issues. Toxicol. Mech. Methods 2018, 28, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Marsh, G.M.; Keeton, K.A.; Riordan, A.S.; Best, E.A.; Benson, S.M. Ethylene oxide and risk of lympho-hematopoietic cancer and breast cancer: A systematic literature review and meta-analysis. Int. Arch. Occup. Environ. Health 2019, 92, 919–939. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.R.; Fisher, J.A.; Medgyesi, D.N.; Buller, I.D.; Liao, L.M.; Gierach, G.; Ward, M.H.; Silverman, D.T. Ethylene oxide emissions and incident breast cancer and non-Hodgkin lymphoma in a US cohort. J. Natl. Cancer Inst. 2023, 115, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Thier, R.; Bolt, H.M. Carcinogenicity and genotoxicity of ethylene oxide: New aspects and recent advances. Crit. Rev. Toxicol. 2000, 30, 595–608. [Google Scholar] [CrossRef]
- Jain, R.B. Associations between observed concentrations of ethylene oxide in whole blood and smoking, exposure to environmental tobacco smoke, and cancers including breast cancer: Data for US children, adolescents, and adults. Environ. Sci. Pollut. Res. Int. 2020, 27, 20912–20919. [Google Scholar] [CrossRef]
- St Helen, G.; Jacob, P., 3rd; Peng, M.; Dempsey, D.A.; Hammond, S.K.; Benowitz, N.L. Intake of toxic and carcinogenic volatile organic compounds from secondhand smoke in motor vehicles. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2774–2782. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Hu, H.; Ni, J.; Zhang, H.; Zhang, H.; Yang, G.; Wang, Y.; Zhang, Y.; Peng, B. The relationship between ethylene oxide levels in hemoglobin and the prevalence of kidney stones in US adults: An exposure-response analysis from NHANES 2013–2016. Environ. Sci. Pollut. Res. Int. 2023, 30, 26357–26366. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, X.; Lin, F.; Zheng, J.; Chen, K.; Wang, X.; Lin, X.; Chen, X.; Ye, Q.; Wang, Y.; et al. Association between ethylene oxide levels and depressive symptoms: A cross-sectional study based on NHANES 2013–2018 database. J. Affect. Disord. 2024, 348, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Hu, G.; He, B.; Cao, Z.; He, J.; Luo, H.; Li, Y.; Yu, Q. Effect of brominated flame retardants exposure on liver function and the risk of non-alcoholic fatty liver disease in the US population. Ecotoxicol. Environ. Saf. 2024, 273, 116142. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.; Kwon, S.C. The Association of Perfluoroalkyl Substance Exposure and a Serum Liver Function Marker in Korean Adults. Toxics 2023, 11, 965. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wan, Z.; Cui, G.; Pan, A.; Liu, G. Association of exposure to ethylene oxide with risk of diabetes mellitus: Results from NHANES 2013–2016. Environ. Sci. Pollut. Res. Int. 2021, 28, 68551–68559. [Google Scholar] [CrossRef] [PubMed]
- Szwiec, E.; Friedman, L.; Buchanan, S. Levels of Ethylene Oxide Biomarker in an Exposed Residential Community. Int. J. Environ. Res. Public Health 2020, 17, 8646. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, D.L.; Crump, D.; Garcia-Reyero, N.; Hecker, M.; Hutchinson, T.H.; LaLone, C.A.; Landesmann, B.; Lettieri, T.; Munn, S.; Nepelska, M.; et al. Adverse outcome pathway (AOP) development I: Strategies and principles. Toxicol. Sci. 2014, 142, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Boobis, A.R.; Doe, J.E.; Heinrich-Hirsch, B.; Meek, M.E.; Munn, S.; Ruchirawat, M.; Schlatter, J.; Seed, J.; Vickers, C. IPCS framework for analyzing the relevance of a noncancer mode of action for humans. Crit. Rev. Toxicol. 2008, 38, 87–96. [Google Scholar] [CrossRef]
- Meek, M.E.; Boobis, A.; Cote, I.; Dellarco, V.; Fotakis, G.; Munn, S.; Seed, J.; Vickers, C. New developments in the evolution and application of the WHO/IPCS framework on mode of action/species concordance analysis. J. Appl. Toxicol. 2014, 34, 1–18. [Google Scholar] [CrossRef]
- Vinken, M.; Landesmann, B.; Goumenou, M.; Vinken, S.; Shah, I.; Jaeschke, H.; Willett, C.; Whelan, M.; Rogiers, V. Development of an adverse outcome pathway from drug-mediated bile salt export pump inhibition to cholestatic liver injury. Toxicol. Sci. 2013, 136, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Houle, C.D.; Ton, T.V.; Clayton, N.; Huff, J.; Hong, H.H.; Sills, R.C. Frequent p53 and H-ras mutations in benzene- and ethylene oxide-induced mammary gland carcinomas from B6C3F1 mice. Toxicol. Pathol. 2006, 34, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Inoue, N.; Fujishiro, K.; Kikuchi, M.; Chiba, S. Biochemical changes in rat erythrocytes caused by ethylene oxide exposure. Fundam. Appl. Toxicol. 1990, 15, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Crabtree, A.A.; Boehnke, N.; Bates, F.S.; Hackel, B.J. Consequences of poly(ethylene oxide) and poloxamer P188 on transcription in healthy and stressed myoblasts. Proc. Natl. Acad. Sci. USA 2023, 120, e2219885120. [Google Scholar] [CrossRef] [PubMed]
- Katoh, T.; Higashi, K.; Inoue, N.; Tanaka, I. Effects of chronic inhalation of ethylene oxide on lipid peroxidation and glutathione redox cycle in rat liver. Res. Commun. Chem. Pathol. Pharmacol. 1988, 61, 281–284. [Google Scholar] [PubMed]
- Zhu, X.; Kong, X.; Chen, M.; Shi, S.; Cheang, I.; Zhu, Q.; Lu, X.; Yue, X.; Tang, Y.; Liao, S.; et al. Blood ethylene oxide, systemic inflammation, and serum lipid profiles: Results from NHANES 2013–2016. Chemosphere 2022, 299, 134336. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Q1 | Q2 | Q3 | Q4 | p-Value |
|---|---|---|---|---|---|
| N = 1029 | N = 1035 | N = 1041 | N = 1036 | ||
| Age (years) | 18.98 | 19.75 | 20.71 | 16.32 | <0.0001 |
| <50 | 44.54 | 42.19 | 38.76 | 51.47 | |
| ≥50 | 55.46 | 57.81 | 61.24 | 48.53 | |
| Gender | <0.0001 | ||||
| Male | 42.87 | 45.57 | 56.95 | 49.52 | |
| Female | 57.13 | 54.43 | 43.05 | 50.48 | |
| Race, n (%) | <0.0001 | ||||
| Mexican American | 7.29 | 8.95 | 8.88 | 5.70 | |
| Other Hispanic | 5.01 | 4.69 | 5.09 | 4.02 | |
| Non-Hispanic White | 76.60 | 69.60 | 62.78 | 69.20 | |
| Non-Hispanic Black | 6.43 | 9.78 | 11.76 | 14.43 | |
| Other Race | 4.68 | 6.98 | 11.49 | 6.66 | |
| Education Level, n (%) | <0.0001 | ||||
| Less than high school | 10.62 | 13.01 | 12.31 | 22.16 | |
| High school | 19.41 | 19.07 | 31.87 | 28.20 | |
| More than high school | 69.97 | 67.92 | 55.82 | 49.64 | |
| PIR | <0.0001 | ||||
| <1.3 | 14.94 | 18.22 | 27.42 | 41.25 | |
| 1.3–3.5 | 40.32 | 38.11 | 35.15 | 36.26 | |
| ≥3.5 | 44.74 | 43.66 | 37.42 | 22.49 | |
| BMI (kg/m2) | <0.0001 | ||||
| <25 | 26.52 | 21.58 | 28.92 | 31.37 | |
| >25 | 73.48 | 78.42 | 71.08 | 68.63 | |
| Smoking, n (%) | <0.0001 | ||||
| Yes | 33.75 | 31.00 | 45.25 | 88.25 | |
| No | 66.25 | 69.00 | 54.75 | 11.75 | |
| Diabetes, n (%) | <0.0001 | ||||
| Yes | 12.36 | 18.95 | 27.76 | 15.29 | |
| No | 87.64 | 81.05 | 72.24 | 84.71 | |
| Alcohol, n (%) | <0.0001 | ||||
| Yes | 78.24 | 66.57 | 78.18 | 83.37 | |
| No | 21.76 | 33.43 | 21.82 | 16.63 | |
| Aspirin, n (%) | 0.1284 | ||||
| Yes | 68.58 | 73.78 | 74.05 | 59.80 | |
| No | 31.42 | 26.22 | 25.95 | 40.20 | |
| Acetaminophen | 0.0021 | ||||
| Yes | 0.61 | 1.22 | 0.58 | 1.71 | |
| No | 99.39 | 98.78 | 99.42 | 98.29 | |
| Statins, n (%) | 0.0121 | ||||
| Yes | 82.65 | 87.93 | 82.35 | 83.76 | |
| No | 17.35 | 12.07 | 17.65 | 16.24 | |
| Hepatitis B, n (%) | <0.0001 | ||||
| Yes | 1.25 | 1.80 | 1.64 | 3.55 | |
| No | 98.75 | 98.20 | 98.36 | 96.45 | |
| Hepatitis C, n (%) | <0.0001 | ||||
| Yes | 1.06 | 0.24 | 1.46 | 6.03 | |
| No | 98.94 | 99.76 | 98.54 | 93.97 | |
| AST (U/L) | 26.04 ± 10.41 | 25.38 ± 16.32 | 24.85 ± 10.15 | 30.09 ± 25.75 | <0.0001 |
| ALT (U/L) | 24.82 ± 15.66 | 24.48 ± 14.54 | 24.93 ± 14.56 | 28.62 ± 26.88 | <0.0001 |
| GGT (U/L) | 26.29 ± 27.69 | 25.53 ± 32.51 | 25.23 ± 21.24 | 46.95 ± 91.90 | <0.0001 |
| ALP (U/L) | 69.11 ± 38.62 | 71.46 ± 40.62 | 72.11 ± 40.67 | 72.64 ± 30.06 | 0.0242 |
| TBIL (μmol/L) | 10.81 ± 6.88 | 10.44 ± 4.99 | 10.53 ± 4.48 | 9.38 ± 4.14 | <0.0001 |
| HDL (mmol/L) | 54.77 ± 18.00 | 52.29 ± 14.52 | 51.35 ± 15.36 | 50.23 ± 15.83 | <0.0001 |
| Total cholesterol (mmol/L) | 186.89 ± 40.65 | 181.75 ± 43.00 | 179.66 ± 40.33 | 187.98 ± 42.82 | <0.0001 |
| LFTs | Model | Continuous log2-Transformed EO | Quartile 1 β (95% CI) | Quartile 2 β (95% CI) | Quartile 3 β (95% CI) | Quartile 4 β (95% CI) | p for Trend |
|---|---|---|---|---|---|---|---|
| ALP | Crude | 1.00 (0.40, 1.60) 0.0012 | 0.00 (Ref.) | 2.35 (−0.06, 4.75) 0.0556 | 3.00 (0.47, 5.53) 0.0201 | 3.53 (1.06, 6.00) 0.0051 | 0.0179 |
| Model 1 | 0.47 (−0.12, 1.06) 0.1169 | 0.00 (Ref.) | 1.98 (−0.36, 4.31) 0.0974 | 2.97 (0.48, 5.46) 0.0194 | 1.68 (−0.73, 4.10) 0.1722 | 0.4080 | |
| Model 2 | 2.61 (1.97, 3.24) <0.0001 | 0.00 (Ref.) | 0.48 (−1.78, 2.74) 0.6760 | 3.75 (1.30, 6.20) 0.0027 | 8.48 (5.75, 11.22) <0.0001 | <0.0001 | |
| ALT | Crude | 0.72 (0.42, 1.01) <0.0001 | 0.00 (Ref.) | −0.34 (−1.51, 0.84) 0.5754 | 0.11 (−1.12, 1.35) 0.8573 | 3.80 (2.59, 5.01) <0.0001 | <0.0001 |
| Model 1 | 0.69 (0.40, 0.99) <0.0001 | 0.00 (Ref.) | −0.42 (−1.57, 0.73) 0.4747 | −0.73 (−1.96, 0.49) 0.2398 | 3.65 (2.46, 4.83) <0.0001 | <0.0001 | |
| Model 2 | 0.50 (0.09, 0.90) 0.0158 | 0.00 (Ref.) | −1.65 (−3.07, −0.24) 0.0223 | −0.25 (−1.79, 1.29) 0.7517 | 0.36 (−1.36, 2.07) 0.6846 | 0.3020 | |
| AST | Crude | 0.67 (0.40, 0.94) <0.0001 | 0.00 (Ref.) | −0.67 (−1.73, 0.40) 0.2187 | −1.20 (−2.32, −0.08) 0.0358 | 4.05 (2.95, 5.14) <0.0001 | <0.0001 |
| Model 1 | 0.71 (0.44, 0.98) <0.0001 | 0.00 (Ref.) | −0.67 (−1.72, 0.39) 0.2136 | −1.71 (−2.84, −0.59) 0.0028 | 4.16 (3.07, 5.25) <0.0001 | <0.0001 | |
| Model 2 | −0.39 (−0.89, 0.11) 0.1242 | 0.00 (Ref.) | −2.54 (−4.29, −0.78) 0.0047 | −3.17 (−5.07, −1.26) 0.0011 | −2.60 (−4.73, −0.48) 0.0165 | 0.0695 | |
| GGT | Crude | 4.53 (3.72, 5.35) <0.0001 | 0.00 (Ref.) | −0.75 (−3.98, 2.48) 0.6476 | −1.06 (−4.46, 2.35) 0.5430 | 20.66 (17.34,23.98) <0.0001 | <0.0001 |
| Model 1 | 4.62 (3.80, 5.44) <0.0001 | 0.00 (Ref.) | −1.09 (−4.31, 2.12) 0.5049 | −2.70 (−6.13, 0.72) 0.1222 | 20.81 (17.49,24.14) <0.0001 | <0.0001 | |
| Model 2 | 5.75 (4.46, 7.05) <0.0001 | 0.00 (Ref.) | −3.84 (−8.43, 0.76) 0.1018 | −1.33 (−6.32, 3.66) 0.6016 | 15.06 (9.50, 20.63) <0.0001 | <0.0001 | |
| TBIL | Crude | −0.39 (−0.48, −0.31) <0.0001 | 0.00 (Ref.) | −0.38 (−0.71, −0.04) 0.0302 | −0.29 (−0.64, 0.07) 0.1150 | −1.43 (−1.78, −1.08) <0.0001 | <0.0001 |
| Model 1 | −0.42 (−0.50, −0.34) <0.0001 | 0.00 (Ref.) | −0.42 (−0.75, −0.09) 0.0125 | −0.62 (−0.98, −0.27) 0.0005 | −1.55 (−1.89, −1.21) <0.0001 | <0.0001 | |
| Model 2 | −0.30 (−0.43, −0.16) <0.0001 | 0.00 (Ref.) | 0.18 (−0.29, 0.65) 0.4593 | 0.10 (−0.41, 0.61) 0.7009 | −1.19 (−1.76, −0.62) <0.0001 | <0.0001 |
| Subgroup | ALP [β (95% CI)] | p for Interaction | ALT [β (95% CI)] | p for Interaction | AST [β (95% CI)] | p for Interaction | GGT [β (95% CI)] | p for Interaction | TBIL [β (95% CI)] | p for Interaction |
|---|---|---|---|---|---|---|---|---|---|---|
| Gender | <0.0001 | <0.0001 | 0.2503 | <0.0001 | 0.7400 | |||||
| Male | 3.81 (2.86, 4.76) | −0.75 (−1.35, −0.14) | −0.36 (−1.12, 0.40) | −0.70 (−2.59, 1.19) | −0.22 (−0.43, −0.02) | |||||
| Female | 0.87 (0.00, 1.74) | 1.23 (0.68, 1.78) | −0.96 (−1.65, −0.27) | 8.83 (7.11, 10.56) | −0.27 (−0.45, −0.09) | |||||
| Age | 0.0002 | 0.0086 | 0.5331 | 0.0002 | 0.0036 | |||||
| <50 | 5.56 (3.78, 7.33) | −0.86 (−1.98, 0.27) | −0.91 (−2.30, 0.49) | −0.47 (−4.11, 3.17) | 0.05 (−0.21, 0.30) | |||||
| ≥50 | 1.97 (1.26, 2.67) | 0.75 (0.30, 1.19) | −0.44 (−0.99, 0.12) | 7.04 (5.59, 8.48) | −0.38 (−0.53, −0.23) | |||||
| Education level | 0.0403 | 0.0245 | 0.5037 | 0.0007 | <0.0001 | |||||
| Less than high school | 1.95 (0.56, 3.34) | 0.03 (−0.87, 0.92) | −1.68 (−2.80, −0.56) | 4.70 (1.92, 7.48) | −0.97 (−1.26, −0.67) | |||||
| High school | 3.47 (2.01, 4.94) | −1.10 (−2.05, −0.16) | −1.18 (−2.36, −0.00) | −0.41 (−3.35, 2.52) | 0.14 (−0.18, 0.45) | |||||
| More than high school | 1.33 (0.49, 2.16) | 0.39 (−0.15, 0.93) | −0.92 (−1.59, −0.24) | 6.04 (4.37, 7.71) | −0.18 (−0.36, 0.00) | |||||
| BMI | 0.2370 | 0.2795 | 0.0016 | 0.0039 | 0.9680 | |||||
| <25 | 1.14 (−0.69, 2.97) | −0.06 (−1.21, 1.09) | 1.56 (0.13, 3.00) | 0.44 (−3.26, 4.14) | −0.29 (−0.67, 0.10) | |||||
| ≥25 | 2.31 (1.62, 2.99) | 0.61 (0.18, 1.04) | −0.88 (−1.42, −0.34) | 6.22 (4.83, 7.61) | −0.29 (−0.44, −0.15) | |||||
| Diabetes status | <0.0001 | <0.0001 | 0.0253 | 0.0597 | 0.7444 | |||||
| Yes | 0.21 (−0.85, 1.28) | 1.49 (0.81, 2.18) | −1.35 (−2.20, −0.51) | 6.85 (4.65, 9.05) | −0.37 (−0.60, −0.14) | |||||
| No | 3.53 (2.74, 4.32) | −0.37 (−0.88, 0.13) | −0.16 (−0.79, 0.47) | 4.25 (2.62, 5.88) | −0.32 (−0.49, −0.15) | |||||
| Smoking | 0.3743 | 0.2015 | 0.9654 | <0.0001 | 0.0048 | |||||
| Yes | 1.89 (1.17, 2.60) | 0.40 (−0.06, 0.86) | −0.68 (−1.25, −0.11) | 5.51 (4.09, 6.94) | −0.46 (−0.61, −0.31) | |||||
| No | 2.83 (0.86, 4.79) | −0.46 (−1.71, 0.79) | −0.72 (−2.29, 0.85) | −4.05 (−7.96, −0.15) | 0.15 (−0.25, 0.55) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Wang, J.; Lei, D.; Peng, D.; Zong, K.; Li, K.; Wu, Z.; Liu, Y.; Huang, Z. Associations between Ethylene Oxide Exposure and Liver Function in the US Adult Population. Toxics 2024, 12, 551. https://doi.org/10.3390/toxics12080551
Li S, Wang J, Lei D, Peng D, Zong K, Li K, Wu Z, Liu Y, Huang Z. Associations between Ethylene Oxide Exposure and Liver Function in the US Adult Population. Toxics. 2024; 12(8):551. https://doi.org/10.3390/toxics12080551
Chicago/Turabian StyleLi, Shanshan, Jinzhou Wang, Dengliang Lei, Dadi Peng, Kezhen Zong, Kaili Li, Zhongjun Wu, Yanyao Liu, and Zuotian Huang. 2024. "Associations between Ethylene Oxide Exposure and Liver Function in the US Adult Population" Toxics 12, no. 8: 551. https://doi.org/10.3390/toxics12080551
APA StyleLi, S., Wang, J., Lei, D., Peng, D., Zong, K., Li, K., Wu, Z., Liu, Y., & Huang, Z. (2024). Associations between Ethylene Oxide Exposure and Liver Function in the US Adult Population. Toxics, 12(8), 551. https://doi.org/10.3390/toxics12080551