
Influence of Lateralization and Distalization on Joint Function after Primary Reverse Total Shoulder Arthroplasty

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Prosthetic Implant Design and Surgical Procedure
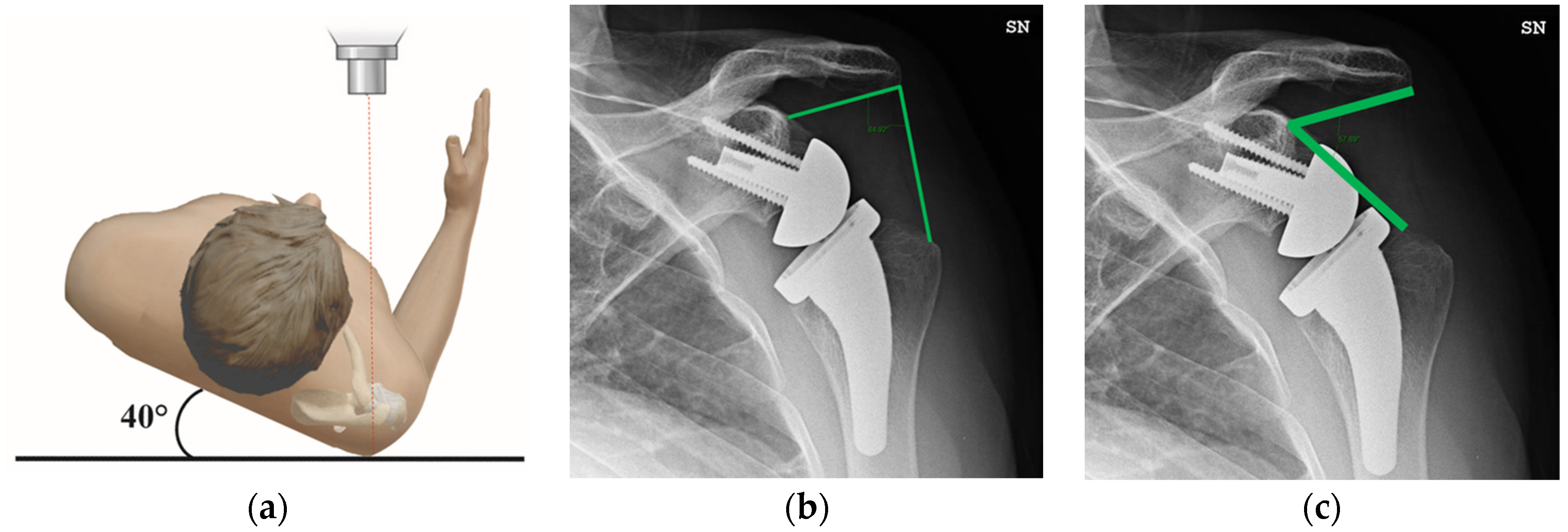
2.3. Radiographic Evaluation
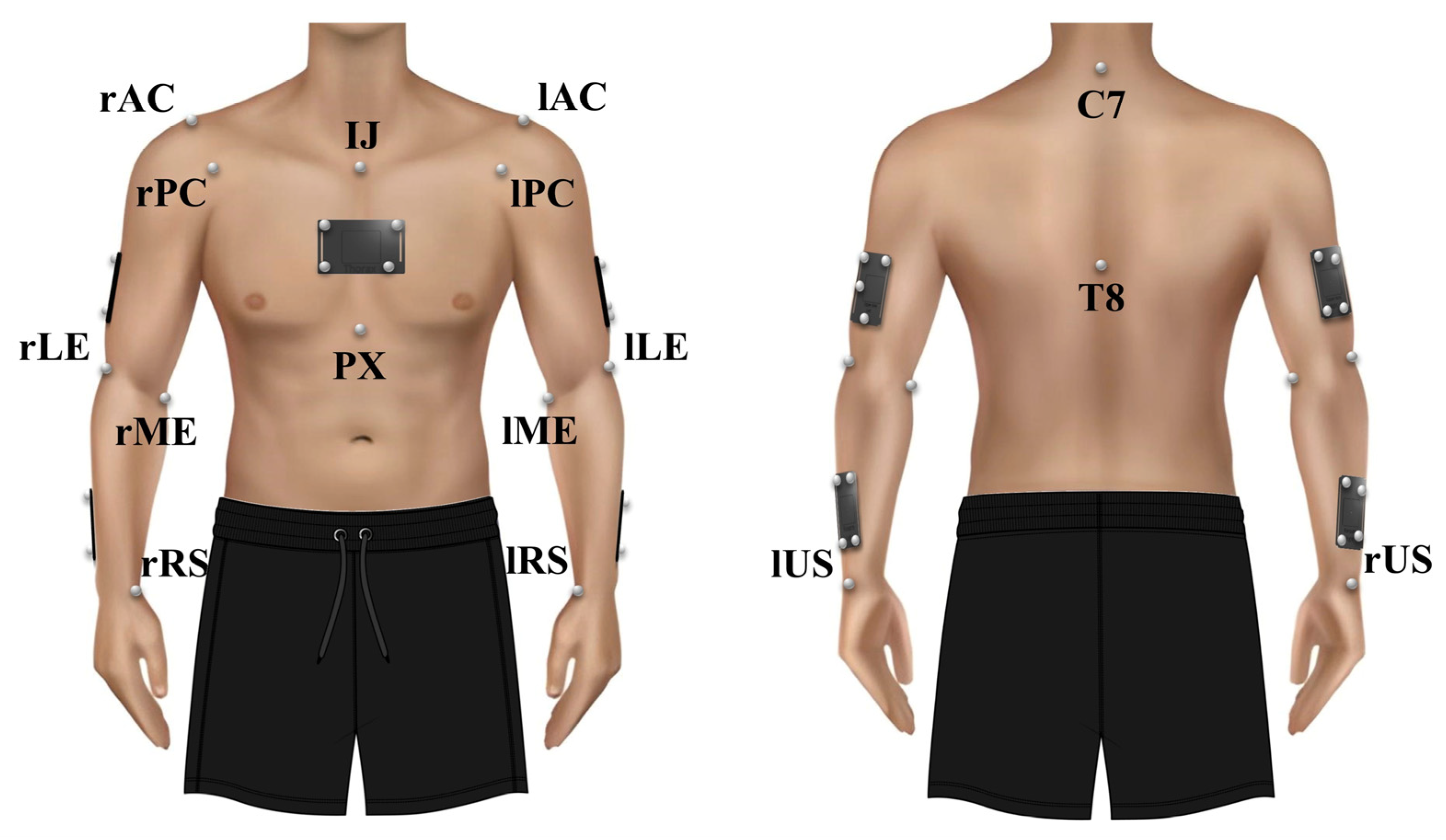
2.4. Clinical and Kinematic Data
2.5. Statistical Analysis
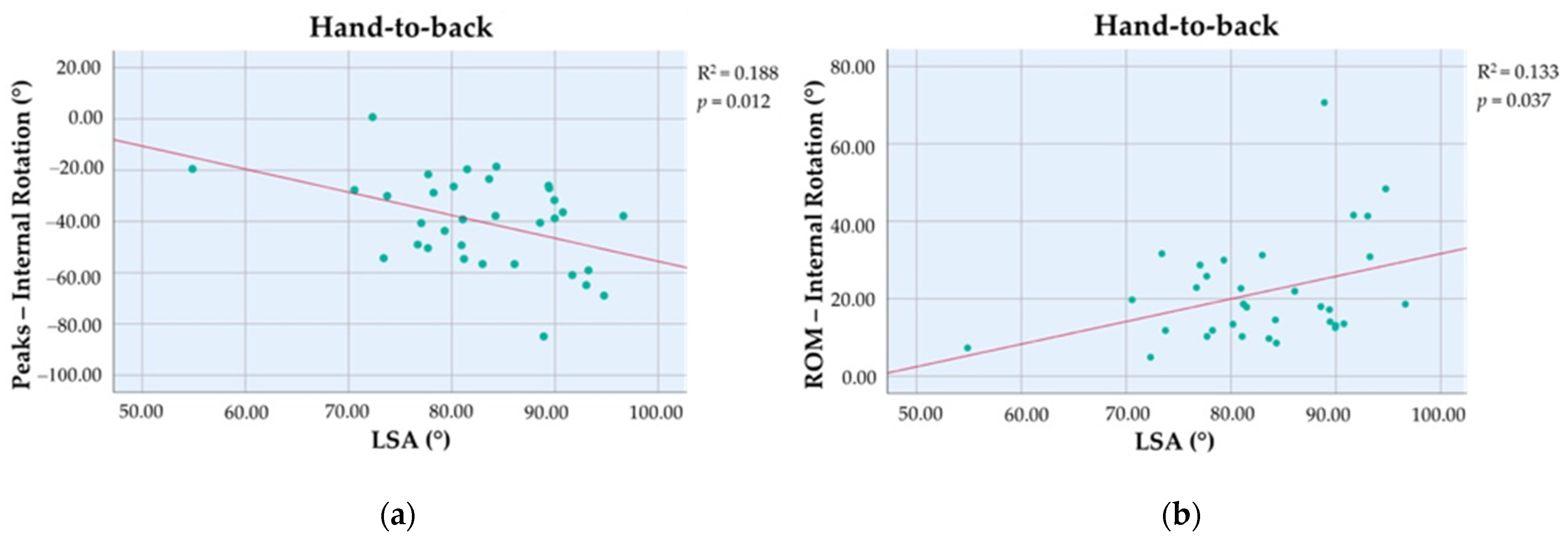
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thon, S.G.; Seidl, A.J.; Bravman, J.T.; McCarty, E.C.; Savoie, F.H.; Frank, R.M. Advances and Update on Reverse Total Shoulder Arthroplasty. Curr. Rev. Musculoskelet. Med. 2020, 13, 11–19. [Google Scholar] [CrossRef]
- Berton, A.; Longo, U.G.; Gulotta, L.V.; De Salvatore, S.; Piergentili, I.; Calabrese, G.; Roberti, F.; Warren, R.F.; Denaro, V. Humeral and Glenoid Version in Reverse Total Shoulder Arthroplasty: A Systematic Review. J. Clin. Med. 2022, 11, 7416. [Google Scholar] [CrossRef]
- Longo, U.G.; Gulotta, L.V.; De Salvatore, S.; Berton, A.; Piergentili, I.; Bandini, B.; Lalli, A.; Denaro, V. The Role of Humeral Neck-Shaft Angle in Reverse Total Shoulder Arthroplasty: 155° versus <155°—A Systematic Review. J. Clin. Med. 2022, 11, 3641. [Google Scholar] [CrossRef]
- Wagner, E.R.; Farley, K.X.; Higgins, I.; Wilson, J.M.; Daly, C.A.; Gottschalk, M.B. The incidence of shoulder arthroplasty: Rise and future projections compared with hip and knee arthroplasty. J. Shoulder Elb. Surg. 2020, 29, 2601–2609. [Google Scholar] [CrossRef]
- Longo, U.G.; Papalia, R.; Castagna, A.; De Salvatore, S.; Guerra, E.; Piergentili, I.; Denaro, V. Shoulder replacement: An epidemiological nationwide study from 2009 to 2019. BMC Musculoskelet. Disord. 2022, 23, 889. [Google Scholar] [CrossRef]
- Roche, C.P. Reverse Shoulder Arthroplasty Biomechanics. J. Funct. Morphol. Kinesiol. 2022, 7, 13. [Google Scholar] [CrossRef]
- Berliner, J.L.; Regalado-Magdos, A.; Ma, C.B.; Feeley, B.T. Biomechanics of reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2015, 24, 150–160. [Google Scholar] [CrossRef]
- Werthel, J.D.; Walch, G.; Vegehan, E.; Deransart, P.; Sanchez-Sotelo, J.; Valenti, P. Lateralization in reverse shoulder arthroplasty: A descriptive analysis of different implants in current practice. Int. Orthop. 2019, 43, 2349–2360. [Google Scholar] [CrossRef]
- Boileau, P.; Moineau, G.; Roussanne, Y.; O’Shea, K. Bony increased-offset reversed shoulder arthroplasty: Minimizing scapular impingement while maximizing glenoid fixation. Clin. Orthop. Relat. Res. 2011, 469, 2558–2567. [Google Scholar] [CrossRef]
- Sprowls, G.R.; Wilson, C.D.; Stewart, W.; Hammonds, K.A.P.; Baruch, N.H.; Ward, R.A.; Robin, B.N. Intraoperative navigation and preoperative templating software are associated with increased glenoid baseplate screw length and use of augmented baseplates in reverse total shoulder arthroplasty. JSES Int. 2021, 5, 102–108. [Google Scholar] [CrossRef]
- Venne, G.; Rasquinha, B.J.; Pichora, D.; Ellis, R.E.; Bicknell, R. Comparing conventional and computer-assisted surgery baseplate and screw placement in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2015, 24, 1112–1119. [Google Scholar] [CrossRef]
- Rojas, J.T.; Lädermann, A.; Ho, S.W.L.; Rashid, M.S.; Zumstein, M.A. Glenoid Component Placement Assisted by Augmented Reality Through a Head-Mounted Display During Reverse Shoulder Arthroplasty. Arthrosc. Tech. 2022, 11, e863–e874. [Google Scholar] [CrossRef]
- Werner, B.S.; Hudek, R.; Burkhart, K.J.; Gohlke, F. The influence of three-dimensional planning on decision-making in total shoulder arthroplasty. J. Shoulder Elb. Surg. 2017, 26, 1477–1483. [Google Scholar] [CrossRef]
- Boutsiadis, A.; Lenoir, H.; Denard, P.J.; Panisset, J.C.; Brossard, P.; Delsol, P.; Guichard, F.; Barth, J. The lateralization and distalization shoulder angles are important determinants of clinical outcomes in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2018, 27, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Berthold, D.P.; Morikawa, D.; Muench, L.N.; Baldino, J.B.; Cote, M.P.; Creighton, R.A.; Denard, P.J.; Gobezie, R.; Lederman, E.; Romeo, A.A.; et al. Negligible Correlation between Radiographic Measurements and Clinical Outcomes in Patients Following Primary Reverse Total Shoulder Arthroplasty. J. Clin. Med. 2021, 10, 809. [Google Scholar] [CrossRef]
- Erickson, B.J.; Werner, B.C.; Griffin, J.W.; Gobezie, R.; Lederman, E.; Sears, B.W.; Bents, E.; Denard, P.J. A comprehensive evaluation of the association of radiographic measures of lateralization on clinical outcomes following reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2022, 31, 963–970. [Google Scholar] [CrossRef]
- Carrazana-Suarez, L.F.; Panico, L.C.; Smolinski, M.P.; Blake, R.J.; McCroskey, M.A.; Sykes, J.B.; Lin, A. Humeral offset as a predictor of outcomes after reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2022, 31, S158–S165. [Google Scholar] [CrossRef]
- Roberson, T.A.; Shanley, E.; Abildgaard, J.T.; Granade, C.M.; Adams, K.J.; Griscom, J.T.; Hunt, Q.; Nix, Q.; Kissenberth, M.J.; Tolan, S.J.; et al. The influence of radiographic markers of biomechanical variables on outcomes in reverse shoulder arthroplasty. JSES Open Access 2019, 3, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Van Raalte, V.; Malian, V. Diagnosis of SLAP lesions with Grashey-view arthrography. Skelet. Radiol. 2003, 32, 388–395. [Google Scholar] [CrossRef]
- Longo, U.G.; Vasta, S.; Maffulli, N.; Denaro, V. Scoring systems for the functional assessment of patients with rotator cuff pathology. Sports Med. Arthrosc. Rev. 2011, 19, 310–320. [Google Scholar] [CrossRef]
- Gowd, A.K.; Charles, M.D.; Liu, J.N.; Lalehzarian, S.P.; Cabarcas, B.C.; Manderle, B.J.; Nicholson, G.P.; Romeo, A.A.; Verma, N.N. Single Assessment Numeric Evaluation (SANE) is a reliable metric to measure clinically significant improvements following shoulder arthroplasty. J. Shoulder Elb. Surg. 2019, 28, 2238–2246. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; van der Helm, F.C.; Veeger, H.E.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Cappozzo, A.; Cappello, A.; Della Croce, U.; Pensalfini, F. Surface-marker cluster design criteria for 3-D bone movement reconstruction. IEEE Trans. Biomed. Eng. 1997, 44, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Kontaxis, A.; Cutti, A.G.; Johnson, G.R.; Veeger, H.E. A framework for the definition of standardized protocols for measuring upper-extremity kinematics. Clin. Biomech. 2009, 24, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Parel, I.; Raggi, M.; Petracci, E.; Pellegrini, A.; Accardo, A.P.; Sacchetti, R.; Porcellini, G. Prediction bands and intervals for the scapulo-humeral coordination based on the Bootstrap and two Gaussian methods. J. Biomech. 2014, 47, 1035–1044. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Bishara, A.J.; Hittner, J.B. Reducing Bias and Error in the Correlation Coefficient Due to Nonnormality. Educ. Psychol. Meas. 2015, 75, 785–804. [Google Scholar] [CrossRef]
- Wall, B.; Nové-Josserand, L.; O’Connor, D.P.; Edwards, T.B.; Walch, G. Reverse total shoulder arthroplasty: A review of results according to etiology. J. Bone Jt. Surg. Am. 2007, 89, 1476–1485. [Google Scholar] [CrossRef]
- Friedman, R.J.; Flurin, P.H.; Wright, T.W.; Zuckerman, J.D.; Roche, C.P. Comparison of reverse total shoulder arthroplasty outcomes with and without subscapularis repair. J. Shoulder Elb. Surg. 2017, 26, 662–668. [Google Scholar] [CrossRef]
- Goetti, P.; Denard, P.J.; Collin, P.; Ibrahim, M.; Mazzolari, A.; Lädermann, A. Biomechanics of anatomic and reverse shoulder arthroplasty. EFORT Open Rev. 2021, 6, 918–931. [Google Scholar] [CrossRef]
- de Wilde, L.F.; Poncet, D.; Middernacht, B.; Ekelund, A. Prosthetic overhang is the most effective way to prevent scapular conflict in a reverse total shoulder prosthesis. Acta Orthop. 2010, 81, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Kazley, J.M.; Cole, K.P.; Desai, K.J.; Zonshayn, S.; Morse, A.S.; Banerjee, S. Prostheses for reverse total shoulder arthroplasty. Expert. Rev. Med. Devices 2019, 16, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; De Salvatore, S.; Carnevale, A.; Tecce, S.M.; Bandini, B.; Lalli, A.; Schena, E.; Denaro, V. Optical Motion Capture Systems for 3D Kinematic Analysis in Patients with Shoulder Disorders. Int. J. Environ. Res. Public Health 2022, 19, 12033. [Google Scholar] [CrossRef]
- Schoch, B.S.; King, J.J.; Fan, W.; Flurin, P.H.; Wright, T.W.; Zuckerman, J.D.; Roche, C.P. Characteristics of anatomic and reverse total shoulder arthroplasty patients who achieve ceiling scores with 3 common patient-reported outcome measures. J. Shoulder Elb. Surg. 2022, 31, 1647–1657. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Jeong, H.Y.; Kim, J.D.; Ro, K.H.; Rhee, S.M.; Rhee, Y.G. Difficulty in performing activities of daily living associated with internal rotation after reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2020, 29, 86–94. [Google Scholar] [CrossRef]
- Rugg, C.M.; Coughlan, M.J.; Lansdown, D.A. Reverse Total Shoulder Arthroplasty: Biomechanics and Indications. Curr. Rev. Musculoskelet. Med. 2019, 12, 542–553. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Knutson, Z.; Choi, D.; Lobatto, D.; Lipman, J.; Craig, E.V.; Warren, R.F.; Gulotta, L.V. Effects of glenosphere positioning on impingement-free internal and external rotation after reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2013, 22, 807–813. [Google Scholar] [CrossRef]
- Friedman, R.J.; Cheung, E.V.; Flurin, P.H.; Wright, T.; Simovitch, R.W.; Bolch, C.; Roche, C.P.; Zuckerman, J.D. Are Age and Patient Gender Associated With Different Rates and Magnitudes of Clinical Improvement After Reverse Shoulder Arthroplasty? Clin. Orthop. Relat. Res. 2018, 476, 1264–1273. [Google Scholar] [CrossRef]
- Leathers, M.P.; Ialenti, M.N.; Feeley, B.T.; Zhang, A.L.; Ma, C.B. Do younger patients have better results after reverse total shoulder arthroplasty? J. Shoulder Elb. Surg. 2018, 27, S24–S28. [Google Scholar] [CrossRef]
- Theodoulou, A.; Krishnan, J.; Aromataris, E. Risk of poor outcomes in patients who are obese following total shoulder arthroplasty and reverse total shoulder arthroplasty: A systematic review and meta-analysis. J. Shoulder Elb. Surg. 2019, 28, e359–e376. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Subject | Humeral Retroversion (°) | Eccentricity (mm) | Glenosphere Diameter (mm) | LSA (°) | DSA (°) |
|---|---|---|---|---|---|
| 1 | 10 | 3.5 | 39 | 93.03 | 48.96 |
| 2 | 10 | 1.5 | 36 | 82.98 | 62.46 |
| 3 | 10 | 1.5 | 36 | 80.94 | 56.62 |
| 4 | 20 | 1.5 | 36 | 89.94 | 57.79 |
| 5 | 10 | 3.5 | 39 | 91.68 | 34.46 |
| 6 | 10 | 1.5 | 36 | 81.06 | 54.10 |
| 7 | 30 | 3.5 | 39 | 89.97 | 53.14 |
| 8 | 10 | 1.5 | 36 | 81.18 | 53.38 |
| 9 | 10 | 1.5 | 36 | 76.70 | 59.10 |
| 10 | 20 | 3.5 | 36 | 84.23 | 57.84 |
| 11 | 20 | 3.5 | 39 | 72.32 | 70.66 |
| 12 | 10 | 1.5 | 36 | 86.07 | 52.65 |
| 13 | 10 | 3.5 | 39 | 94.75 | 35.80 |
| 14 | 10 | 3.5 | 42 | 93.24 | 45.71 |
| 15 | 20 | 1.5 | 36 | 80.18 | 51.68 |
| 16 | 10 | 1.5 | 36 | 83.62 | 59.01 |
| 17 | 10 | 3.5 | 36 | 78.23 | 51.48 |
| 18 | 20 | 1.5 | 36 | 90.76 | 41.25 |
| 19 | 10 | 1.5 | 36 | 88.56 | 59.00 |
| 20 | 10 | 3.5 | 39 | 54.87 | 102.37 |
| 21 | 10 | 3.5 | 39 | 79.31 | 60.19 |
| 22 | 10 | 1.5 | 36 | 89.44 | 47.43 |
| 23 | 10 | 1.5 | 36 | 96.62 | 31.15 |
| 24 | 10 | 1.5 | 36 | 81.49 | 57.34 |
| 25 | 20 | 3.5 | 36 | 70.56 | 72.10 |
| 26 | 10 | 1.5 | 36 | 73.74 | 63.43 |
| 27 | 10 | 3.5 | 42 | 89.38 | 45.72 |
| 28 | 10 | 3.5 | 39 | 84.32 | 55.95 |
| 29 | 10 | 3.5 | 39 | 77.68 | 63.40 |
| 30 | 10 | 3.5 | 42 | 77.71 | 55.02 |
| 31 | 10 | 1.5 | 36 | 77.04 | 64.03 |
| 32 | 20 | 1.5 | 36 | 88.90 | 54.97 |
| 33 | 10 | 1.5 | 36 | 73.40 | 72.62 |
| Peaks | VAS | SANE | CMS | SST | ||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| FE | 0.138 | 0.444 | 0.105 | 0.561 | 0.083 | 0.645 | −0.009 | 0.962 |
| SCAP | −0.013 | 0.943 | 0.132 | 0.463 | 0.022 | 0.901 | −0.045 | 0.805 |
| ABD | −0.026 | 0.885 | 0.365 | 0.037 * | 0.435 | 0.011 * | 0.320 | 0.070 |
| ABD_HN | −0.233 | 0.193 | 0.018 | 0.920 | 0.046 | 0.798 | 0.009 | 0.961 |
| ER | −0.404 | 0.020 * | 0.449 | 0.009 * | 0.376 | 0.031 * | 0.388 | 0.026 * |
| ABD_HB | 0.151 | 0.401 | 0.202 | 0.912 | 0.209 | 0.244 | 0.165 | 0.358 |
| IR | −0.237 | 0.184 | −0.066 | 0.714 | −0.129 | 0.473 | −0.067 | 0.710 |
| ROMs | VAS | SANE | CMS | SST | ||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| FE | 0.099 | 0.582 | 0.121 | 0.503 | 0.043 | 0.813 | −0.012 | 0.948 |
| SCAP | −0.078 | 0.644 | 0.261 | 0.142 | 0.015 | 0.934 | 0.017 | 0.927 |
| ABD | −0.057 | 0.753 | 0.377 | 0.031 * | 0.426 | 0.014 * | 0.293 | 0.098 |
| ABD_HN | −0.225 | 0.209 | 0.106 | 0.556 | 0.027 | 0.883 | 0.023 | 0.889 |
| ER | −0.156 | 0.385 | 0.239 | 0.180 | 0.194 | 0.280 | 0.165 | 0.359 |
| ABD_HB | 0.040 | 0.827 | 0.134 | 0.459 | 0.158 | 0.381 | 0.191 | 0.287 |
| IR | 0.198 | 0.269 | 0.257 | 0.150 | 0.173 | 0.335 | 0.182 | 0.311 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; Franceschetti, E.; Carnevale, A.; Schena, E.; Cozza, G.; Perricone, G.; Cardinale, M.E.; Papalia, R. Influence of Lateralization and Distalization on Joint Function after Primary Reverse Total Shoulder Arthroplasty. Bioengineering 2023, 10, 1409. https://doi.org/10.3390/bioengineering10121409
Longo UG, Franceschetti E, Carnevale A, Schena E, Cozza G, Perricone G, Cardinale ME, Papalia R. Influence of Lateralization and Distalization on Joint Function after Primary Reverse Total Shoulder Arthroplasty. Bioengineering. 2023; 10(12):1409. https://doi.org/10.3390/bioengineering10121409
Chicago/Turabian StyleLongo, Umile Giuseppe, Edoardo Franceschetti, Arianna Carnevale, Emiliano Schena, Giulia Cozza, Giovanni Perricone, Marco Edoardo Cardinale, and Rocco Papalia. 2023. "Influence of Lateralization and Distalization on Joint Function after Primary Reverse Total Shoulder Arthroplasty" Bioengineering 10, no. 12: 1409. https://doi.org/10.3390/bioengineering10121409
APA StyleLongo, U. G., Franceschetti, E., Carnevale, A., Schena, E., Cozza, G., Perricone, G., Cardinale, M. E., & Papalia, R. (2023). Influence of Lateralization and Distalization on Joint Function after Primary Reverse Total Shoulder Arthroplasty. Bioengineering, 10(12), 1409. https://doi.org/10.3390/bioengineering10121409