
Improvement in Biocompatibility and Biointegration of Human Acellular Dermal Matrix through Vacuum Plasma Surface Treatment

 and
and 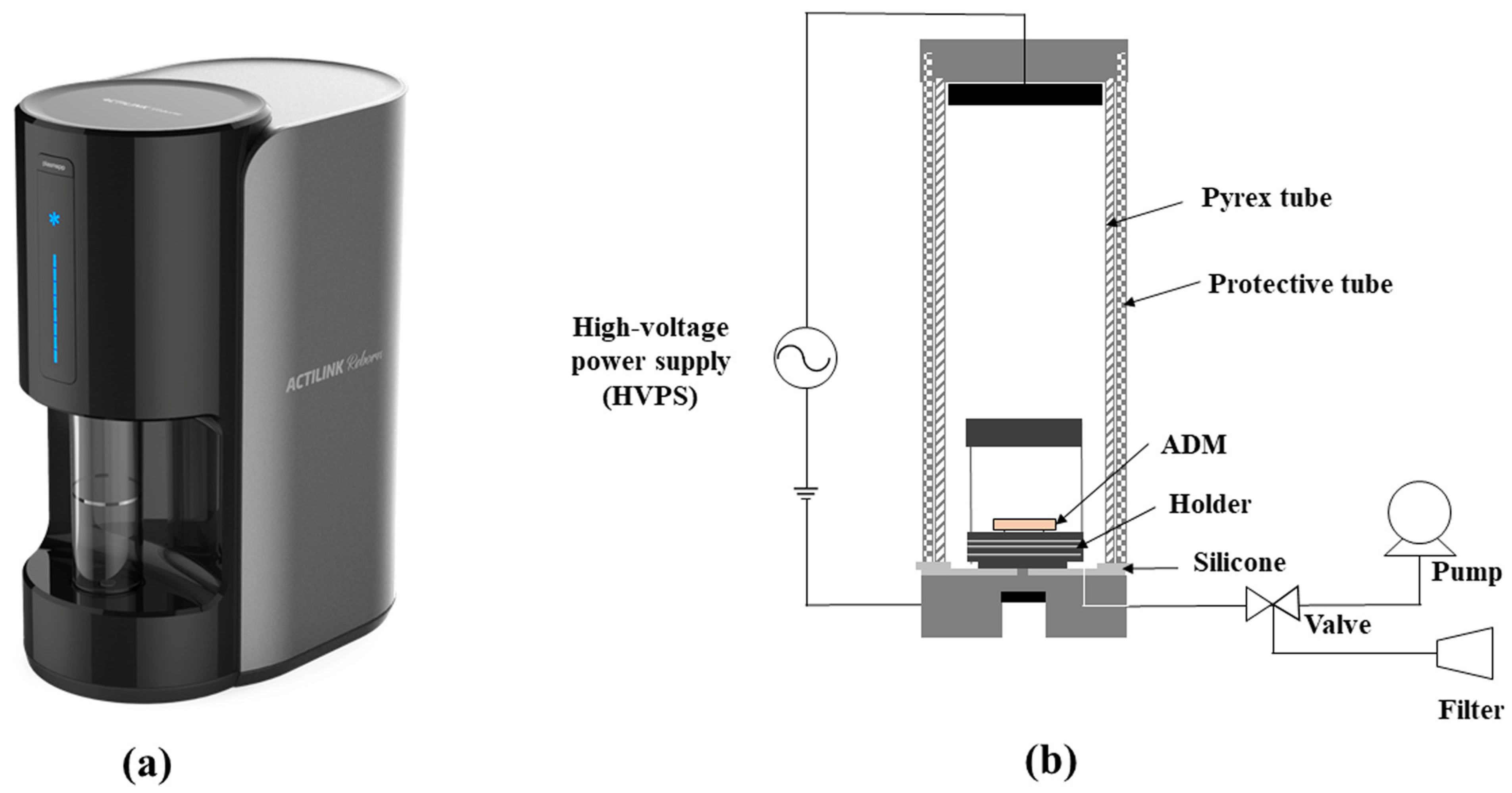{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Device and Setup
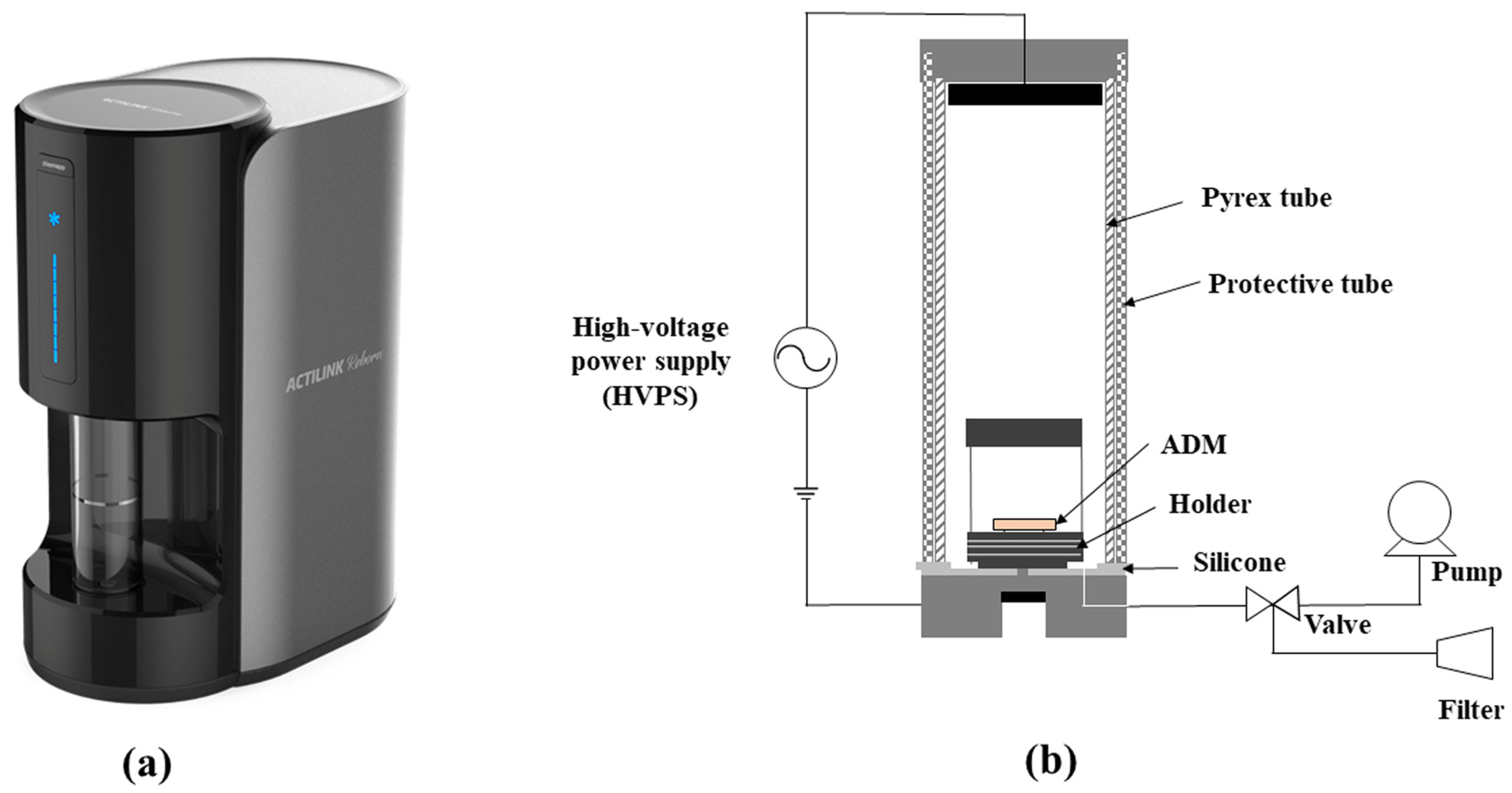
2.1.1. Plasma Device
2.1.2. ADM Treatment Process
2.2. In Vitro Study
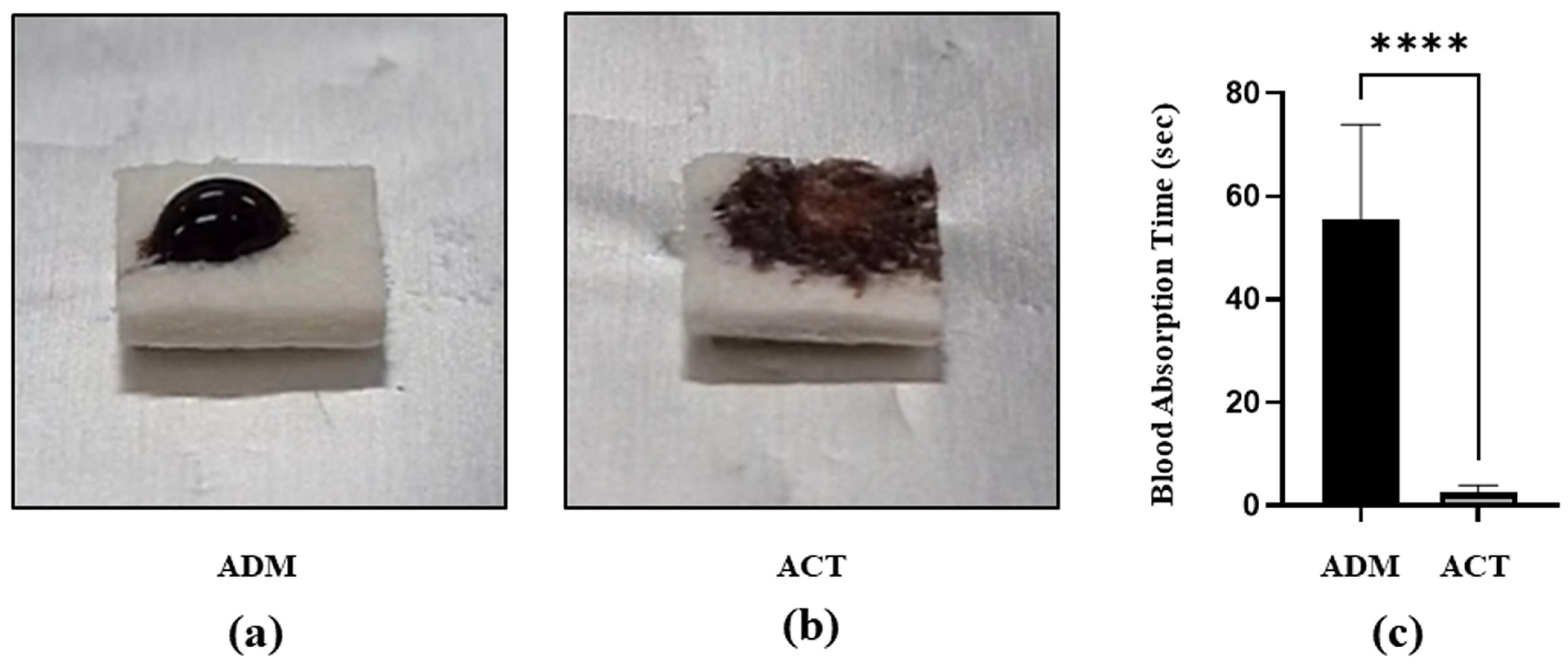
2.2.1. Hydrophilicity Test of ADM Surface
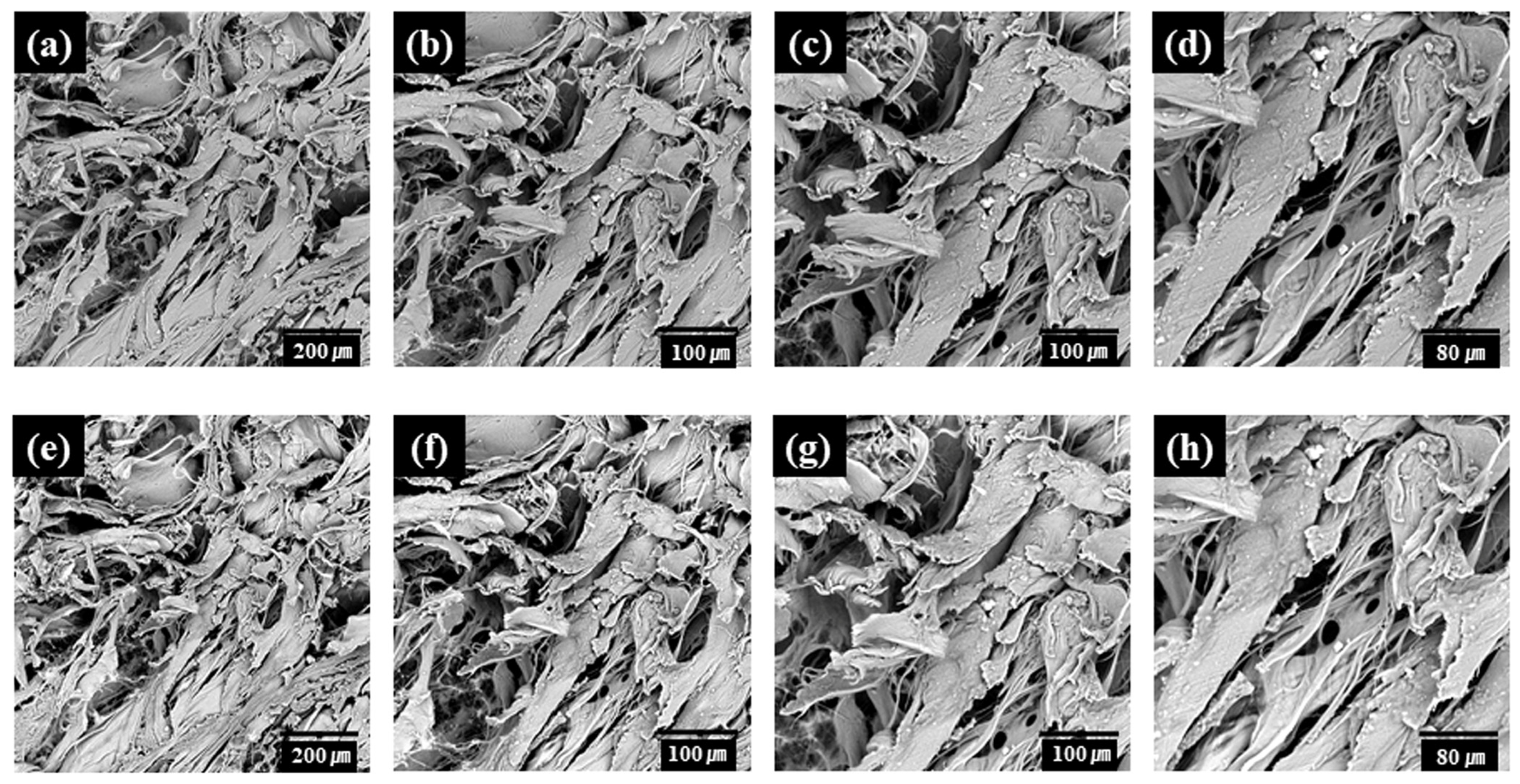
2.2.2. Evaluating Characteristics of ADM Surface Using Scanning Electron Microscope
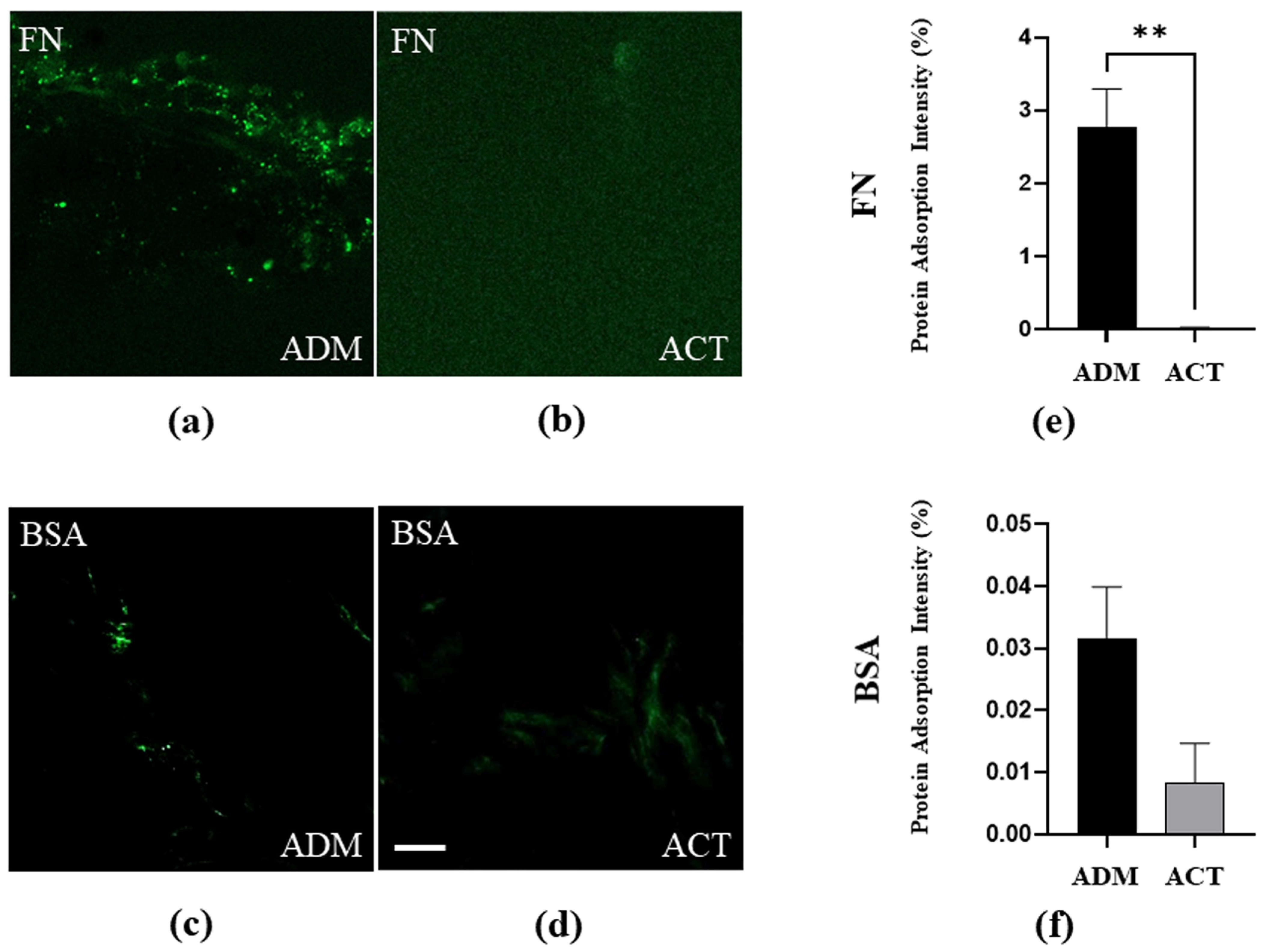
2.2.3. Protein Adsorption Experiment
2.3. In Vivo Study
2.3.1. Experimental Animals
2.3.2. Histological Analysis
2.3.3. Immunofluorescence Microscopy
2.4. Statistical Analysis
3. Results
3.1. In Vitro Study
3.1.1. Hydrophilicity of hADM Surface before and after Plasma Treatment
3.1.2. Surface Characteristics of hADMs before and after Plasma Treatment
3.1.3. Inhibition of Protein Adsorption by Plasma Treatment
3.2. In Vivo Study
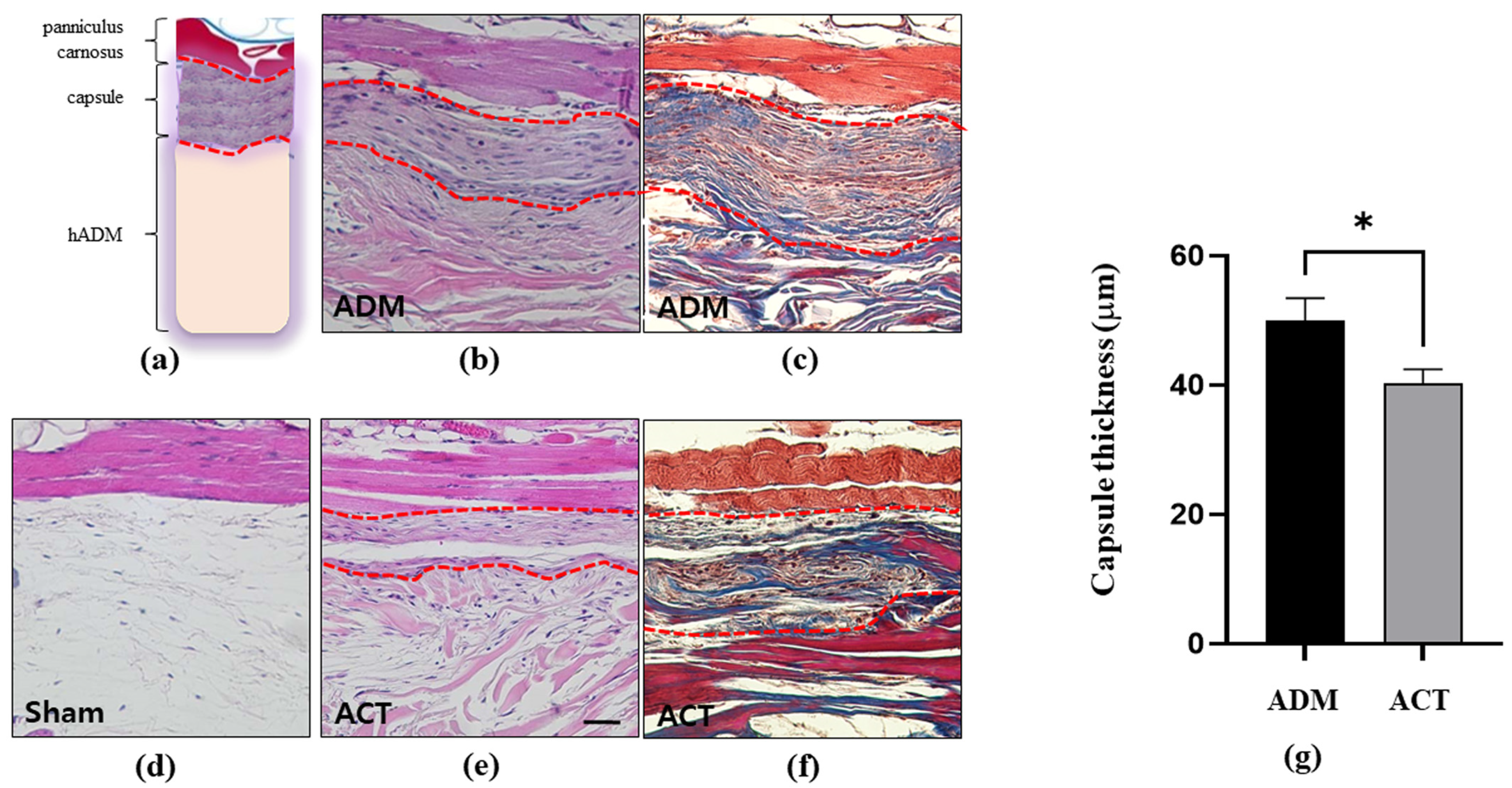
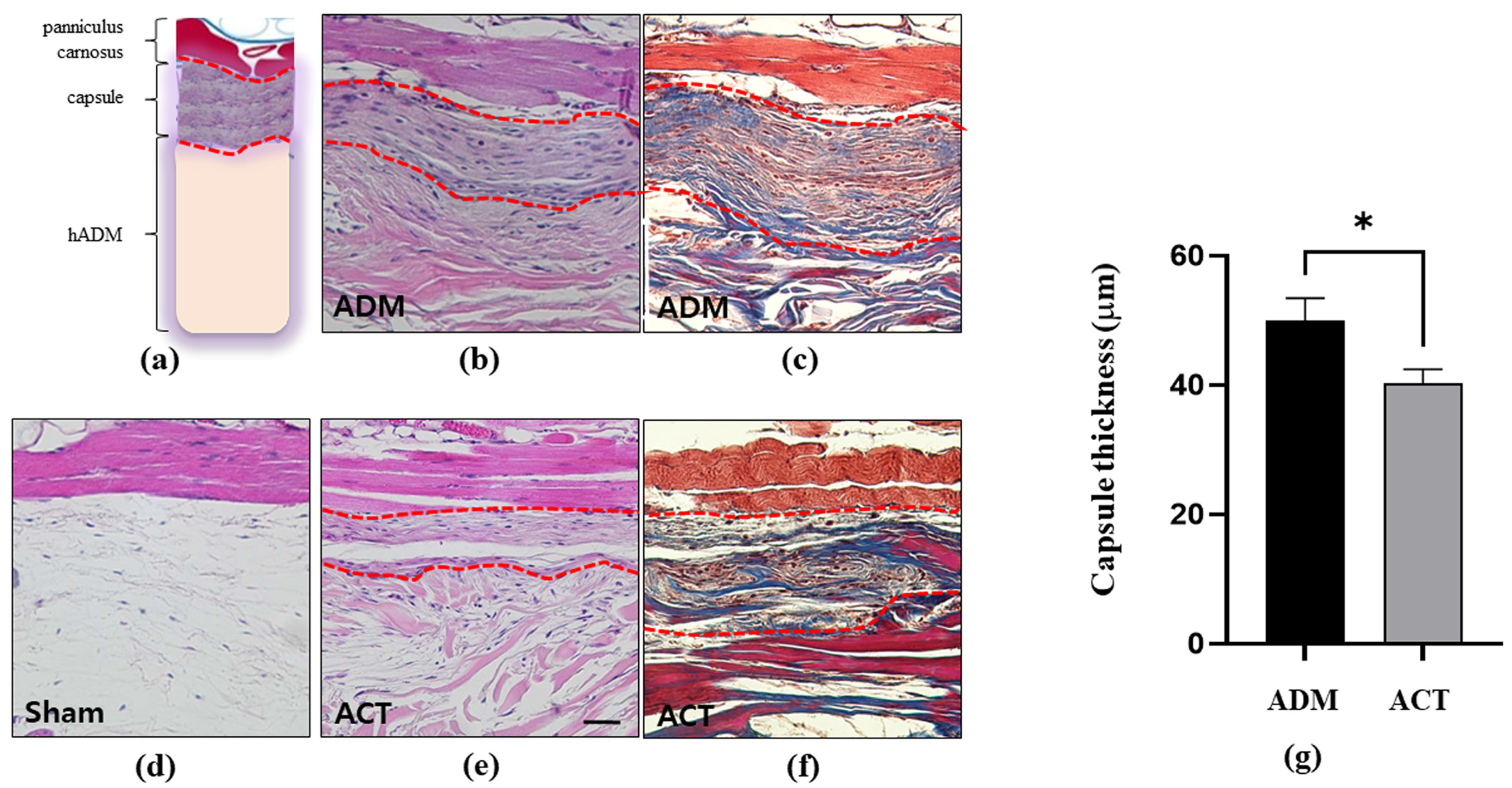
3.2.1. Changes in the Thickness of Capsules around Implanted hADMs
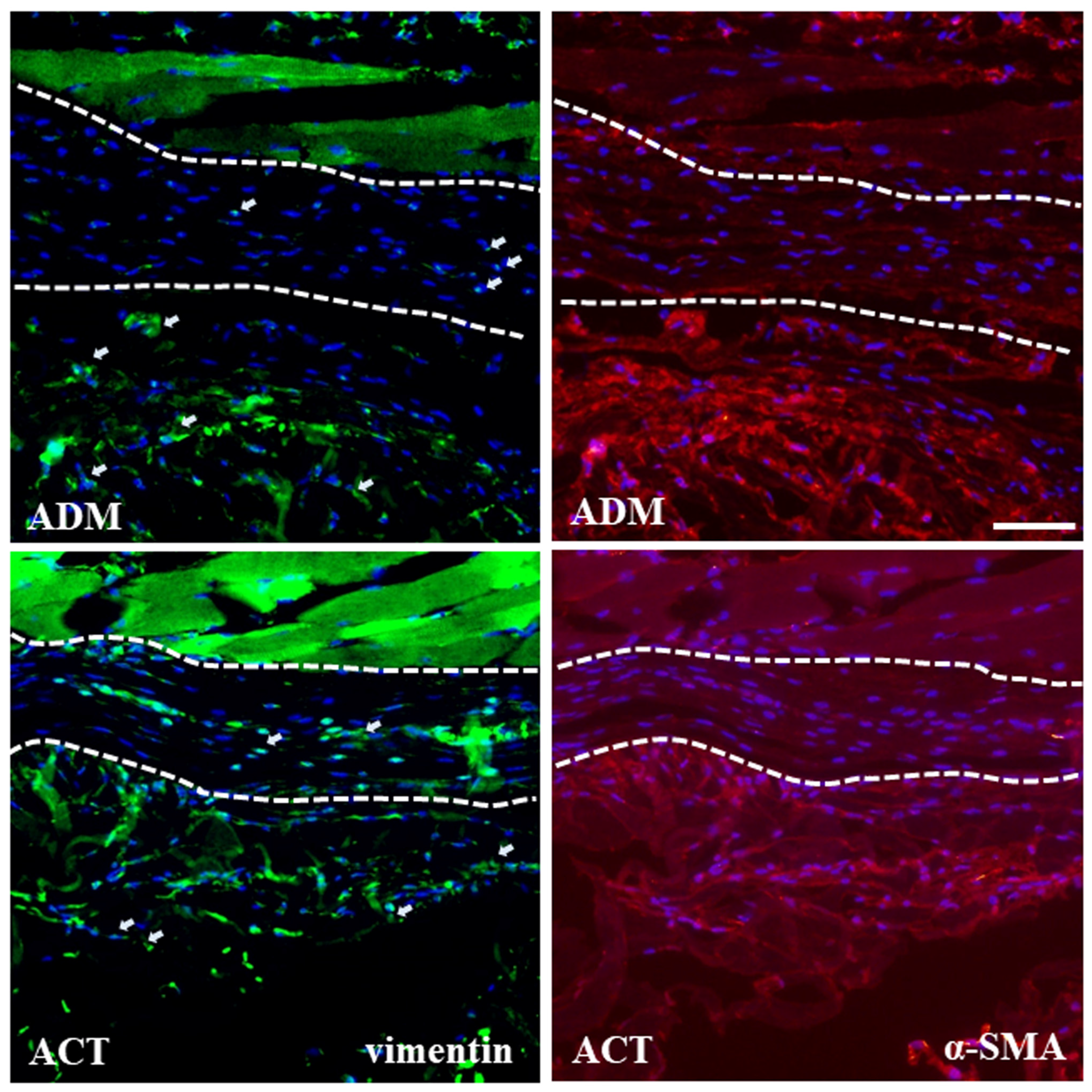
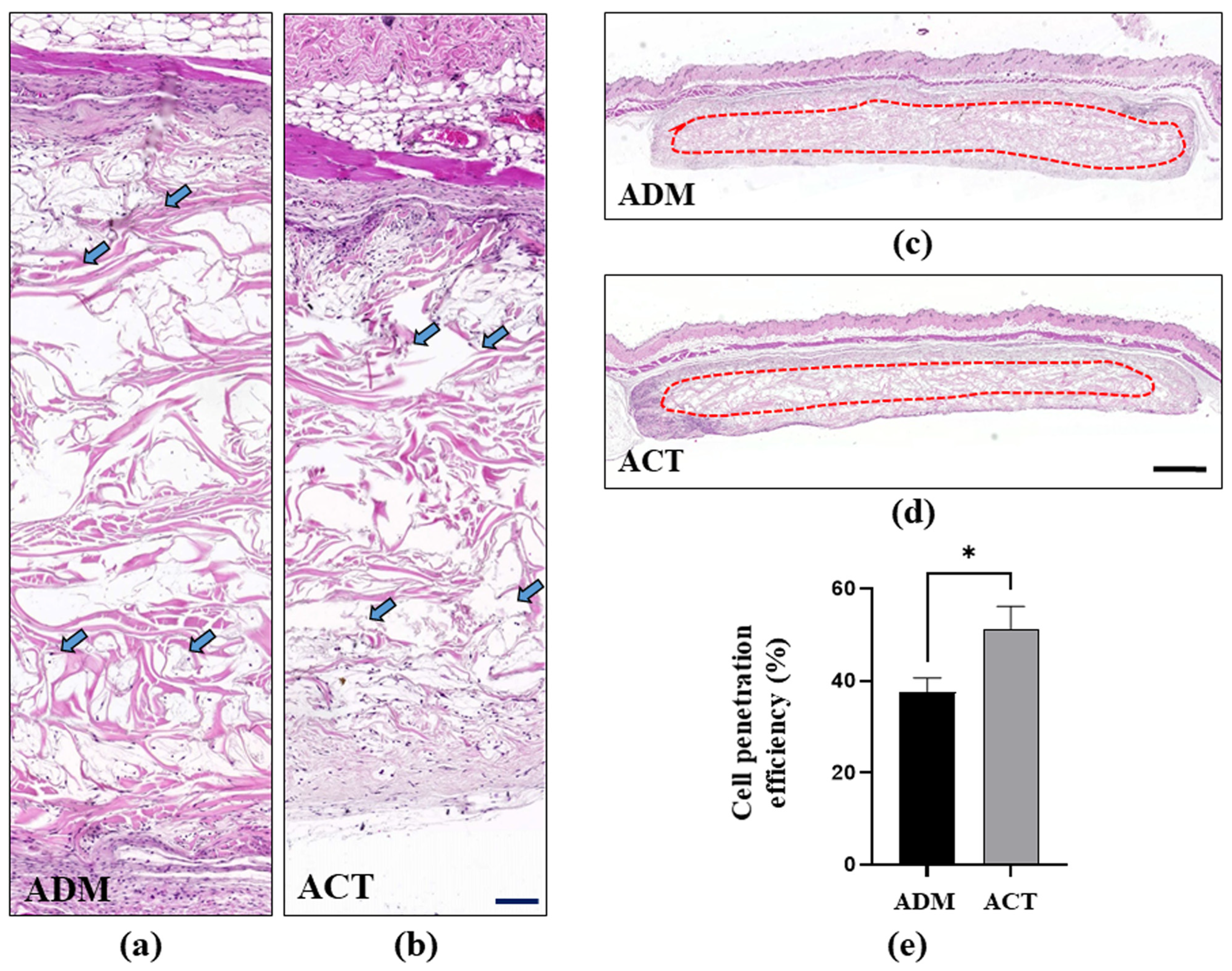
3.2.2. Fibroblast Infiltration and Proliferation in hADMs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wainwright, D.J. Use of an acellular allograft dermal matrix (AlloDerm) in the management of full-thickness burns. Burns 1995, 21, 243–248. [Google Scholar] [CrossRef]
- Janis, J.E.; O’Neill, A.C.; Ahmad, J.; Zhong, T.; Hofer, S.O.P. Acellular dermal matrices in abdominal wall reconstruction: A systematic review of the current evidence. Plast. Reconstr. Surg. 2012, 130, 183S–193S. [Google Scholar] [CrossRef] [PubMed]
- DeLong, M.R.; Tandon, V.J.; Farajzadeh, M.; Berlin, N.L.; MacEachern, M.P.; Rudkin, G.H.; Da Lio, A.L.; Cederna, P.S. Systematic Review of the Impact of Acellular Dermal Matrix on Aesthetics and Patient Satisfaction in Tissue Expander-to-Implant Breast Reconstructions. Plast. Reconstr. Surg. 2019, 144, 967e–974e. [Google Scholar] [CrossRef]
- Nahabedian, M.Y. Acellular dermal matrices in primary breast reconstruction: Principles, concepts, and indications. Plast. Reconstr. Surg. 2012, 130, 44S–53S. [Google Scholar] [CrossRef] [PubMed]
- Ricci, J.A.; Treiser, M.D.; Tao, R.; Jiang, W.; Guldbrandsen, G.; Halvorson, E.; Hergrueter, C.A.; Chun, Y.S. Predictors of Complications and Comparison of Outcomes Using SurgiMend Fetal Bovine and AlloDerm Human Cadaveric Acellular Dermal Matrices in Implant-Based Breast Reconstruction. Plast. Reconstr. Surg. 2016, 138, 583e–591e. [Google Scholar] [CrossRef] [PubMed]
- Dussoyer, M.; Michopoulou, A.; Rousselle, P. Decellularized Scaffolds for Skin Repair and Regeneration. Appl. Sci. 2020, 10, 3435. [Google Scholar] [CrossRef]
- Ko, H.; Kim, D.; Shin, C.; Gong, N.Y.; You, B.; Oh, H.S.; Lee, J.; Oh, S.H. In Vivo Efficacy of an Injectable Human Acellular Dermal Matrix. Aesthetic Plast. Surg. 2023, 47, 2833–2840. [Google Scholar] [CrossRef] [PubMed]
- Weltmann, K.D.; Polak, M.; Masur, K.; von Woedtke, T.; Winter, J.; Reuter, S. Plasma Processes and Plasma Sources in Medicine. Contrib. Plasm. Phys. 2012, 52, 644–654. [Google Scholar] [CrossRef]
- Richter, G.T.; Smith, J.E.; Spencer, H.J.; Fan, C.Y.; Vural, E. Histological comparison of implanted cadaveric and porcine dermal matrix grafts. Otolaryngol. Head. Neck Surg. 2007, 137, 239–242. [Google Scholar] [CrossRef]
- Menon, N.G.; Rodriguez, E.D.; Byrnes, C.K.; Girotto, J.A.; Goldberg, N.H.; Silverman, R.P. Revascularization of human acellular dermis in full-thickness abdominal wall reconstruction in the rabbit model. Ann. Plast. Surg. 2003, 50, 523–527. [Google Scholar] [CrossRef]
- Jeon, H.J.; Jung, A.; Kim, H.J.; Seo, J.S.; Kim, J.Y.; Yum, M.S.; Gweon, B.; Lim, Y. Enhanced Osteoblast Adhesion and Proliferation on Vacuum Plasma-Treated Implant Surface. Appl. Sci 2022, 12, 9884. [Google Scholar] [CrossRef]
- Kim, S.J.; Yang, H.; Shin, C.; Choi, Y.; Oh, S.H. Qualitative and Quantitative Analyses of Donor Site Morbidity Following a Graft of the Acellular Dermal Matrix Versus Primary Fascial Repair After ALT Flap Harvesting. Plast. Surg. 2021, 29, 153–159. [Google Scholar] [CrossRef]
- Skowronek, K.; Labus, W.; Stojko, R.; Kitala, D.; Sadlocha, M.; Drosdzol-Cop, A. Application of Acellular Dermal Matrix in Gynaecology—A Current Review. J. Clin. Med. 2022, 11, 4030. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Park, K.R.; Kim, T.G.; Ha, J.H.; Chung, K.J.; Kim, Y.H.; Lee, S.J.; Kang, S.H. A Comparative Study of CG CryoDerm and AlloDerm in Direct-to-Implant Immediate Breast Reconstruction. Arch. Plast. Surg. 2013, 40, 374–379. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, Q.; Yu, Q.S.; Wang, Y. Nonthermal Atmospheric Plasmas in Dental Restoration. J. Dent. Res. 2016, 95, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.Y.; Manolache, S.; Somers, E.B.; Wong, A.C.L.; Denes, F.S. Generation of antifouling layers on stainless steel surfaces by plasma-enhanced crosslinking of polyethylene glycol. J. Appl. Polym. Sci. 2005, 97, 485–497. [Google Scholar] [CrossRef]
- Tendero, C.; Tixier, C.; Tristant, P.; Desmaison, J.; Leprince, P. Atmospheric pressure plasmas: A review. Spectrochim. Acta B 2006, 61, 2–30. [Google Scholar] [CrossRef]
- Nam, S.H.; Choi, B.B.R.; Kim, G.C. The Whitening Effect and Histological Safety of Nonthermal Atmospheric Plasma Inducing Tooth Bleaching. Int. J. Environ. Res. Public. Health 2021, 18, 4714. [Google Scholar] [CrossRef]
- Ozdemir, E.; Basaran, P.; Kartal, S.; Akan, T. Cold plasma application to fresh green leafy vegetables: Impact on microbiology and product quality. Compr. Rev. Food Sci. Food Saf. 2023, 22, 4484–4515. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Jeon, H.J.; Jung, A.; Kim, J.; Kim, J.Y.; Lee, S.H.; Kim, H.; Yeom, M.S.; Choe, W.; Gweon, B.; et al. Improvement of osseointegration efficacy of titanium implant through plasma surface treatment. Biomed. Eng. Lett. 2022, 12, 421–432. [Google Scholar] [CrossRef]
- Chau Nguyen, T.T.; Shin, C.M.; Lee, S.J.; Koh, E.S.; Kwon, H.H.; Park, H.; Kim, D.H.; Choi, C.H.; Oh, S.H.; Kim, D.W.; et al. Ultrathin Nanostructured Films of Hyaluronic Acid and Functionalized beta-Cyclodextrin Polymer Suppress Bacterial Infection and Capsular Formation of Medical Silicone Implants. Biomacromolecules 2022, 23, 4547–4561. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Ahn, M.; Piao, Y.; Ha, Y.; Choi, D.K.; Yi, M.H.; Shin, N.; Kim, D.W.; Oh, S.H. Effect of Botulinum Toxin Type A on TGF-beta/Smad Pathway Signaling: Implications for Silicone-Induced Capsule Formation. Plast. Reconstr. Surg. 2016, 138, 821e–829e. [Google Scholar] [CrossRef] [PubMed]
- Carlson, T.L.; Lee, K.W.; Pierce, L.M. Effect of cross-linked and non-cross-linked acellular dermal matrices on the expression of mediators involved in wound healing and matrix remodeling. Plast. Reconstr. Surg. 2013, 131, 697–705. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.J.; Lee, B.; Shin, C.; You, B.; Oh, H.S.; Lee, J.; Lee, J.; Oh, S.K.; Oh, S.-H. Improvement in Biocompatibility and Biointegration of Human Acellular Dermal Matrix through Vacuum Plasma Surface Treatment. Bioengineering 2024, 11, 359. https://doi.org/10.3390/bioengineering11040359
Yang HJ, Lee B, Shin C, You B, Oh HS, Lee J, Lee J, Oh SK, Oh S-H. Improvement in Biocompatibility and Biointegration of Human Acellular Dermal Matrix through Vacuum Plasma Surface Treatment. Bioengineering. 2024; 11(4):359. https://doi.org/10.3390/bioengineering11040359
Chicago/Turabian StyleYang, Ho Jik, Byungchul Lee, Chungmin Shin, Boram You, Han Seul Oh, Jeonghoon Lee, Jinsun Lee, Se Kwang Oh, and Sang-Ha Oh. 2024. "Improvement in Biocompatibility and Biointegration of Human Acellular Dermal Matrix through Vacuum Plasma Surface Treatment" Bioengineering 11, no. 4: 359. https://doi.org/10.3390/bioengineering11040359
APA StyleYang, H. J., Lee, B., Shin, C., You, B., Oh, H. S., Lee, J., Lee, J., Oh, S. K., & Oh, S.-H. (2024). Improvement in Biocompatibility and Biointegration of Human Acellular Dermal Matrix through Vacuum Plasma Surface Treatment. Bioengineering, 11(4), 359. https://doi.org/10.3390/bioengineering11040359