

Changes of the Alveolar Bone Ridge Using Bone Mineral Grafts and Collagen Membranes after Tooth Extraction: A Systematic Review and Meta-Analysis




Abstract
1. Introduction
2. Materials and Methods
2.1. Development of the Protocol and Registration
2.2. Focused Interest Question
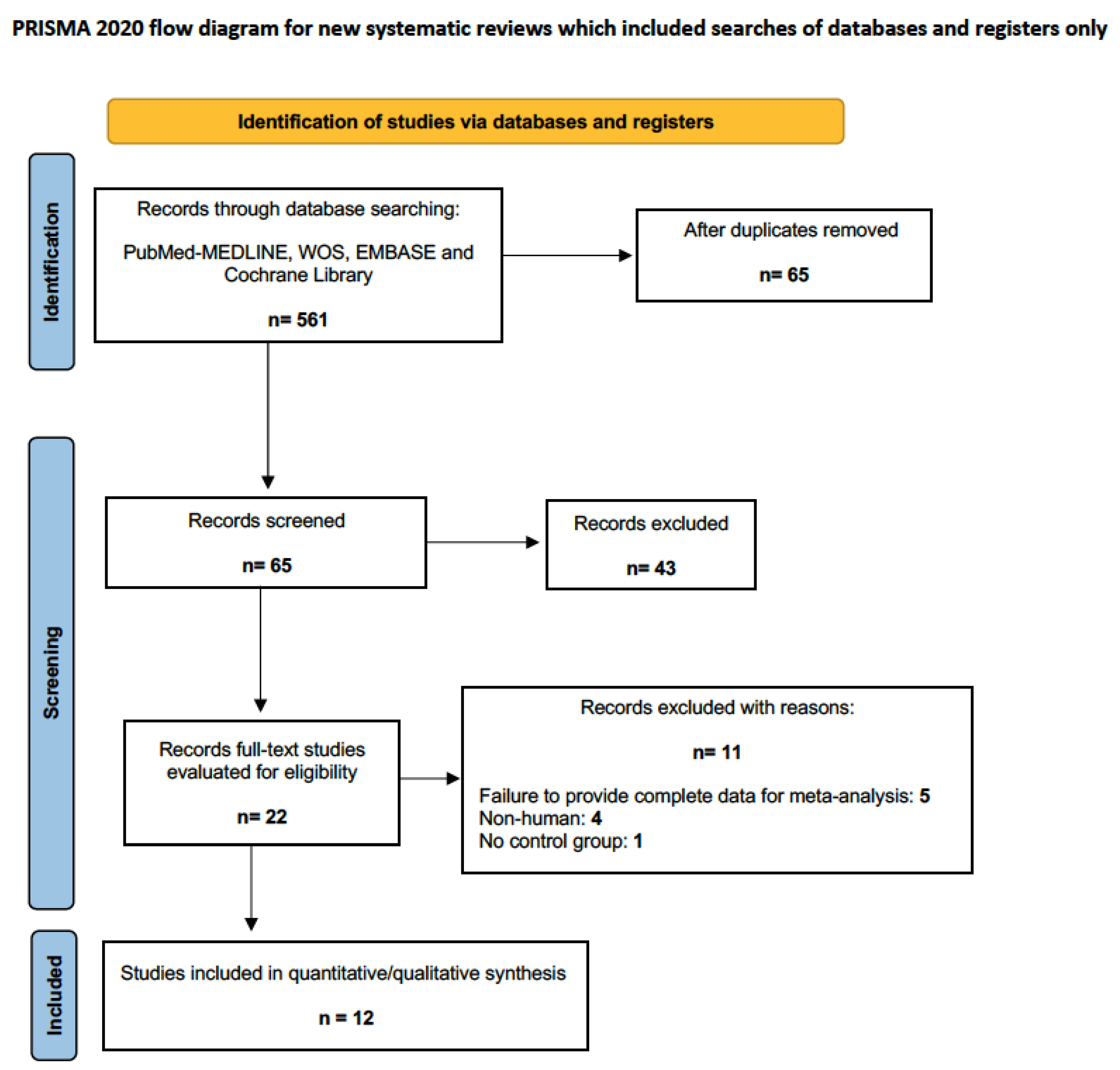
2.3. Data Sources and Literature Search Method
2.4. Inclusion and Exclusion Criteria
2.5. Assessment of the Quality of the Reports
2.6. Risk of Bias in Selected Studies
2.7. Meta-Analysis
3. Results
3.1. Study Characteristics
3.2. Methodological Rigor of the Studies
3.3. Risk of Bias within Studies
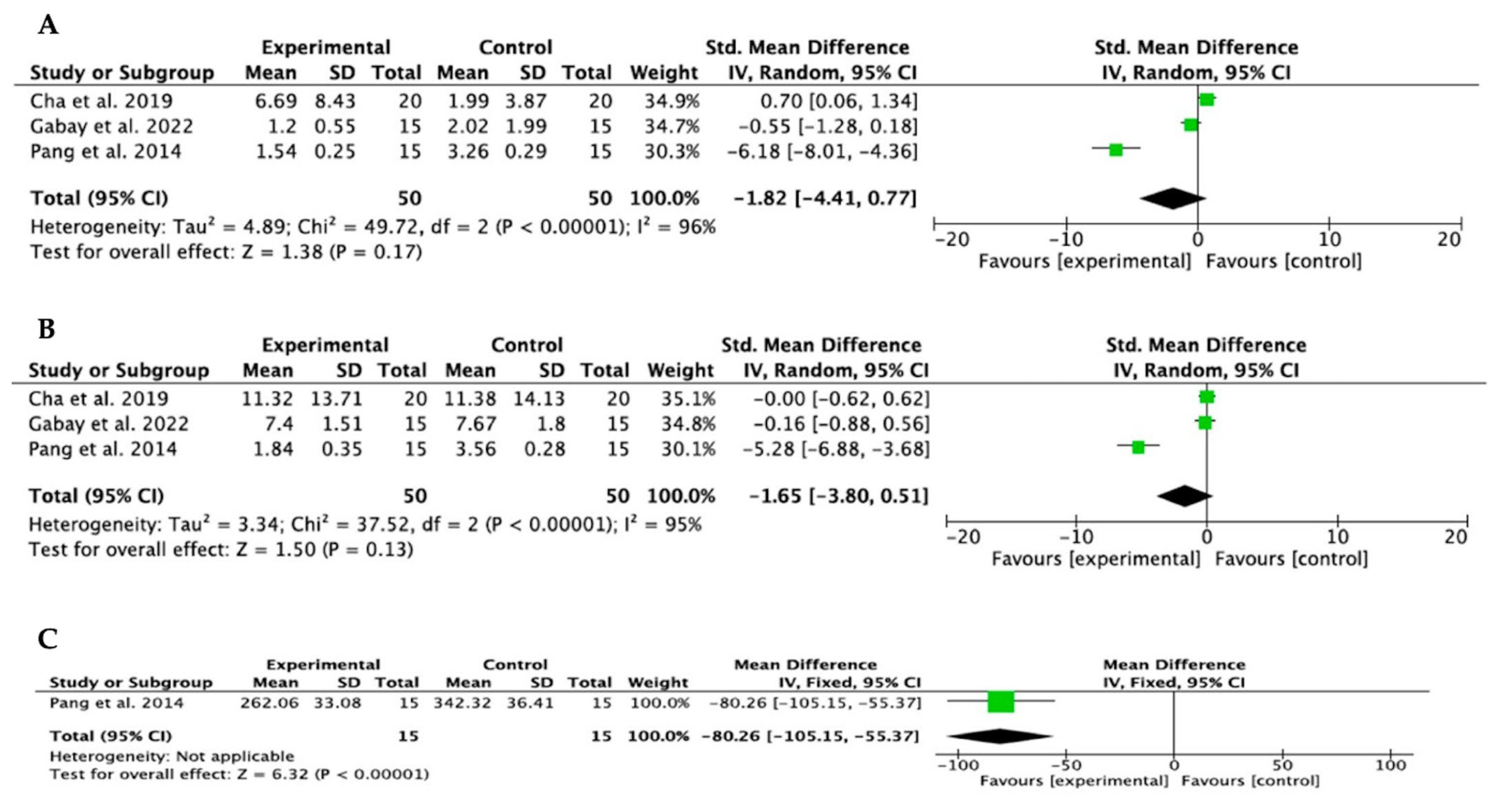
3.4. Meta-Analysis
3.5. Publication Bias
4. Discussion
Previous Literature
5. Conclusions
- The results of subgroup analyses demonstrated that ABRP using bone mineral grafts in combination with resorbable collagen barriers manifests a tendency for greater alveolar ridge preservation, both in height and width, than spontaneous healing.
- The CBV, although assessed in only one study, showed the highest tendency to statistical significance, although it could not be evaluated in the meta-analysis.
- Clinical practice can be focused in a certain direction, according to the characteristics and specific situation of each clinical case.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23 (Suppl. S5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Vittorini Orgeas, G.; Clementini, M.; De Risi, V.; de Sanctis, M. Surgical techniques for alveolar socket preservation: A systematic review. Int. J. Oral Maxillofac. Implants 2013, 28, 1049–1061. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.T.V.; Guillen, G.A.; Macêdo, F.G.C.; Goulart, D.R.; Nóia, C.F. Comparative Effects of Different Materials on Alveolar Preservation. J. Oral Maxillofac. Surg. 2023, 81, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 195–223. [Google Scholar] [CrossRef] [PubMed]
- Ayari, H. The use of periodontal membranes in the field of periodontology: Spotlight on collagen membranes. J. Appl. Biomed. 2022, 20, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Lynn, A.K.; Yannas, I.V.; Bonfield, W. Antigenicity and immunogenicity of collagen. J. Biomed. Mater. Res. B Appl. Biomater. 2004, 71, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.; Shan, T.; Ma, Y.X.; Tay, F.R.; Niu, L. Novel Biomedical Applications of Crosslinked Collagen. Trends Biotechnol. 2019, 37, 464–491. [Google Scholar] [CrossRef] [PubMed]
- Radenković, M.; Alkildani, S.; Stoewe, I.; Bielenstein, J.; Sundag, B.; Bellmann, O.; Jung, O.; Najman, S.; Stojanović, S.; Barbeck, M. Comparative In Vivo Analysis of the Integration Behavior and Immune Response of Collagen-Based Dental Barrier Membranes for Guided Bone Regeneration (GBR). Membranes 2021, 11, 712. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.A.; Mealey, B.L. Histologic comparison of healing after tooth extraction with ridge preservation using mineralized versus demineralized freeze-dried bone allograft. J. Periodontol. 2012, 83, 329–336. [Google Scholar] [CrossRef]
- Quisiguiña Salem, C.; Ruiz Delgado, E.; Crespo Reinoso, P.A.; Robalino, J.J. Alveolar ridge preservation: A review of concepts and controversies. Natl. J. Maxillofac. Surg. 2023, 14, 167–176. [Google Scholar] [CrossRef]
- Temmerman, A.; Vandessel, J.; Castro, A.; Jacobs, R.; Teughels, W.; Pinto, N.; Quirynen, M. The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: A split-mouth, randomized, controlled clinical trial. J. Clin. Periodontol. 2016, 43, 990–999. [Google Scholar] [CrossRef]
- Milillo, L.; Cinone, F.; Lo Presti, F.; Lauritano, D.; Petruzzi, M. The Role of Blood Clot in Guided Bone Regeneration: Biological Considerations and Clinical Applications with Titanium Foil. Materials 2021, 14, 6642. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Sánchez, I.; Sanz-Martín, I.; Ortiz-Vigón, A.; Molina, A.; Sanz, M. Complications in bone-grafting procedures: Classification and management. Periodontol 2000 2022, 88, 86–102. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Graham, R.; Mancher, M.; Miller Wolman, D.; Greenfield, S.; Steinberg, E. Washington (DC) US, Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines. In Clinical Practice Guidelines We Can Trust; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Tufanaru, C.; Leonardi-Bee, J.; Aromataris, E.; Munn, Z. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid. Synth. 2023, 21, 494–506. [Google Scholar] [CrossRef] [PubMed]
- Minozzi, S.; Cinquini, M.; Gianola, S.; Gonzalez-Lorenzo, M.; Banzi, R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J. Clin. Epidemiol. 2020, 126, 37–44. [Google Scholar] [CrossRef]
- Casagrande, A.; Fabris, F.; Girometti, R. Beyond kappa: An informational index for diagnostic agreement in dichotomous and multivalue ordered-categorical ratings. Med. Biol. Eng. Comput. 2020, 58, 3089–3099. [Google Scholar] [CrossRef]
- Mardas, N.; Chadha, V.; Donos, N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: A randomized, controlled clinical trial. Clin. Oral Implants Res. 2010, 21, 688–698. [Google Scholar] [CrossRef] [PubMed]
- Mardas, N.; D’Aiuto, F.; Mezzomo, L.; Arzoumanidi, M.; Donos, N. Radiographic alveolar bone changes following ridge preservation with two different biomaterials. Clin. Oral Implants Res. 2011, 22, 416–423. [Google Scholar] [CrossRef]
- Perelman-Karmon, M.; Kozlovsky, A.; Liloy, R.; Artzi, Z. Socket site preservation using bovine bone mineral with and without a bioresorbable collagen membrane. Int. J. Periodontics Restor. Dent. 2012, 32, 459–465. [Google Scholar]
- Cook, D.C.; Mealey, B.L. Histologic comparison of healing following tooth extraction with ridge preservation using two different xenograft protocols. J. Periodontol. 2013, 84, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Pang, C.; Ding, Y.; Zhou, H.; Qin, R.; Hou, R.; Zhang, G.; Hu, K. Alveolar ridge preservation with deproteinized bovine bone graft and collagen membrane and delayed implants. J. Craniofac. Surg. 2014, 25, 1698–1702. [Google Scholar] [CrossRef] [PubMed]
- Scheyer, E.T.; Heard, R.; Janakievski, J.; Mandelaris, G.; Nevins, M.L.; Pickering, S.R.; Richardson, C.R.; Pope, B.; Toback, G.; Velásquez, D.; et al. A randomized, controlled, multicentre clinical trial of post-extraction alveolar ridge preservation. J. Clin. Periodontol. 2016, 3, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Nart, J.; Barallat, L.; Jimenez, D.; Mestres, J.; Gómez, A.; Carrasco, M.A.; Violant, D.; Ruíz-Magaz, V. Radiographic and histological evaluation of deproteinized bovine bone mineral vs. deproteinized bovine bone mineral with 10% collagen in ridge preservation. A randomized controlled clinical trial. Clin. Oral Implants Res. 2017, 28, 840–848. [Google Scholar] [CrossRef]
- Jung, R.E.; Sapata, V.M.; Hämmerle, C.H.F.; Wu, H.; Hu, X.L.; Lin, Y. Combined use of xenogeneic bone substitute material covered with a native bilayer collagen membrane for alveolar ridge preservation: A randomized controlled clinical trial. Clin. Oral Implants Res. 2018, 29, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.C.; Shin, H.S.; Cho, I.W.; Koo, K.T.; Park, J.C. Ridge preservation in molar extraction sites with an open-healing approach: A randomized controlled clinical trial. J. Clin. Periodontol. 2019, 46, 1144–1154. [Google Scholar] [CrossRef]
- Cha, J.K.; Song, Y.W.; Park, S.H.; Jung, R.E.; Jung, U.W.; Thoma, D.S. Alveolar ridge preservation in the posterior maxilla reduces vertical dimensional change: A randomized controlled clinical trial. Clin. Oral Implants Res. 2019, 30, 515–523. [Google Scholar] [CrossRef]
- Stumbras, A.; Januzis, G.; Gervickas, A.; Kubilius, R.; Juodzbalys, G. Randomized and Controlled Clinical Trial of Bone Healing After Alveolar Ridge Preservation Using Xenografts and Allografts versus Plasma Rich in Growth Factors. J. Oral Implantol. 2020, 46, 515–525. [Google Scholar] [CrossRef]
- Gabay, E.; Katorza, A.; Zigdon-Giladi, H.; Horwitz, J.; Machtei, E.E. Histological and dimensional changes of the alveolar ridge following tooth extraction when using collagen matrix and collagen-embedded xenogenic bone substitute: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2022, 24, 382–390. [Google Scholar] [CrossRef]
- Vergara-Merino, L.; Verdejo, C.; Carrasco, C.; Vargas-Peirano, M. Living systematic review: New inputs and challenges. Medwave 2020, 20, e8092. [Google Scholar] [CrossRef]
- Cardaropoli, D.; De Luca, N.; Tamagnone, L.; Leonardi, R. Bone and Soft Tissue Modifications in Immediate Implants Versus Delayed Implants Inserted Following Alveolar Ridge Preservation: A Randomized Controlled Clinical Trial. Part I: Esthetic Outcomes. Int. J. Periodontics Restor. Dent. 2022, 42, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.J.; Prihoda, T.J.; Mealey, B.L.; Lasho, D.J.; Noujeim, M.; Huynh-Ba, G. Evaluation of Healing at Molar Extraction Sites with and without Ridge Preservation: A Randomized Controlled Clinical Trial. J. Periodontol. 2017, 88, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Borg, T.D.; Mealey, B.L. Histologic healing following tooth extraction with ridge preservation using mineralized versus combined mineralized-demineralized freeze-dried bone allograft: A randomized controlled clinical trial. J. Periodontol. 2015, 86, 348–355. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Deflorian, M.; Testori, T.; Mandell, F.; Nagursky, H.; Vinci, R. Alveolar socket preservation with demineralised bovine bone mineral and a collagen matrix. J. Periodontal Implant Sci. 2017, 47, 194–210. [Google Scholar] [CrossRef]
- Sun, D.J.; Lim, H.C.; Lee, D.W. Alveolar ridge preservation using an open membrane approach for sockets with bone deficiency: A randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, Y.K.; Kim, H.S.; Yun, P.Y.; Kim, S.G.; Choi, Y.H. Extraction socket sealing using palatal gingival grafts and resorbable collagen membranes. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 39. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, R.; Di Nardo, D.; Di Giorgio, G.; Miccoli, G.; Testarell, L. Effectiveness of Xenograft and Porcine-Derived Resorbable Membrane in Augmentation of Posterior Extraction Sockets with a Severe Wall Defect. A Radiographic/Tomographic Evaluation. J. Oral Maxillofac. Res. 2019, 10, e3. [Google Scholar] [CrossRef]
- You, S.; Yu, F.; Fan, Q.; Xia, T.; Liang, L.; Yan, Q.; Zeng, H.; Shi, B. Radiographic comparison of atelocollagen versus deproteinized bovine bone minerals covered with a collagen membrane in alveolar ridge preservation: A retrospective study. BMC Oral Health 2023, 23, 901. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92, 195S–201S. [Google Scholar] [CrossRef]
- Karaca, Ç.; Er, N.; Gülşahı, A.; Köseoğlu, O.T. Alveolar ridge preservation with a free gingival graft in the anterior maxilla: Volumetric evaluation in a randomized clinical trial. Int. J. Oral Maxillofac. Surg. 2015, 44, 774–780. [Google Scholar] [CrossRef]
- Jambhekar, S.; Kernen, F.; Bidra, A.S. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: A systematic review of randomized controlled clinical trials. J. Prosthet. Dent. 2015, 113, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Alsabeeha, N.H.; Payne, A.G.; Ali, S.; Faggion, C.M.J.; Esposito, M. Interventions for replacing missing teeth: Alveolar ridge preservation techniques for dental implant site development. Cochrane Database Syst. Rev. 2021, 4, CD010176. [Google Scholar] [CrossRef] [PubMed]
- Han, H.S.; Lee, J.T.; Oh, S.; Cho, Y.D.; Kim, S. Effectiveness of a collagen matrix seal and xenograft in alveolar ridge preservation: An experimental study in dogs. Sci. Rep. 2024, 14, 163. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Bassir, S.H.; Alhareky, M.; Wangsrimongkol, B.; Jia, Y.; Karimbux, N. Systematic Review and Meta-Analysis of Hard Tissue Outcomes of Alveolar Ridge Preservation. Int. J. Oral Maxillofac. Implants 2018, 33, 979–994. [Google Scholar] [CrossRef]
- Apaza-Bedoya, K.; Magrin, G.L.; Romandini, M.; Blanco-Carrión, J.; Benfatti, C.A.M. Efficacy of alveolar ridge preservation with xenografts and resorbable socket sealing materials in the esthetic region: A systematic review with meta-analyses. Clin. Implant Dent. Relat. Res. 2024, 26, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Lin, D.; Li, B.; Hong, H.; Jiang, C.; Yuan, Y.; Wang, J.; Hu, R.; Li, B.; Liu, C. BMP-2/CPC scaffold with dexamethasone-loaded blood clot embedment accelerates clinical bone regeneration. Am. J. Transl. Res. 2022, 14, 2874–2893. [Google Scholar]
- Mattiola, A.; Bosshardt, D.; Schmidlin, P.R. The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation. Dent. J. 2018, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Aravena, P.C.; Sandoval, S.P.; Pizarro, F.E.; Simpson, M.I.; Castro-Adams, N.; Serandour, G.; Rosas, C. Leukocyte and Platelet-Rich Fibrin Have Same Effect as Blood Clot in the 3-Dimensional Alveolar Ridge Preservation. A Split-Mouth Randomized Clinical Trial. J. Oral Maxillofac. Surg. 2021, 79, 575–584. [Google Scholar] [CrossRef]
- Murray, G.; Holden, R.; Roschlau, W. Experimental and clinical study of new growth of bone in a cavity. Am. J. Surg. 1957, 93, 385–387. [Google Scholar] [CrossRef]
- Melcher, A.H.; Dreyer, C.J. Protection of the Blood Clot in Healing Circumscribed Bone Defects. J. Bone Jt. Surg. Br. Vol. 1962, 44, 424–430. [Google Scholar] [CrossRef]
- Barootchi, S.; Tavelli, L.; Majzoub, J.; Stefanini, M.; Wang, H.L.; Avila-Ortiz, G. Alveolar ridge preservation: Complications and cost-effectiveness. Periodontology 2000 2023, 92, 235–262. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Adult Subjects Undergoing Dental Extractions |
|---|---|
| Intervention | Bone mineral grafts and Collagen membranes |
| Comparisons | Spontaneous healing or other grafting materials |
| Outcomes | To observe the effects of treatment on the clinical and radiological measurements. (Δ BCW; Δ BCH; Δ CBV) |
| Study design | RCTs |
| Study, Year | Type of Study | Subjects | Experimental Area | Grafted Material | Barrier Products | Comparison | Follow-Up | Dropouts | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Mardas et al., 2010 [19] | RCCT | 30 | Incisor, canine and premolar area (Maxilla and mandible) | BBM | Collagen | DBBM | 8 months | 4 | The use of bone mineral grafts and collagen barrier in the alveolus preserved crestal height, but no differences in buccal and palatal bone plate width were observed between the groups. |
| Mardas et al., 2011 [20] | RCCT | 30 | Incisor, canine and premolar area (Maxilla and mandible) | BBM | Collagen | DBBM | 4 and 8 months | 3 | Preservation of the alveolar ridge with bovine xenograft or synthetic bone substitute and collagen barrier also preserves radiographic bone levels. |
| Perelman-Karmon et al., 2012 [21] | RCT | 23 | Incisors and premolar area (Maxilla and mandible) | BBM | Collagen | BBM without resorbable membrane coverage. | 9 months | 0 | The biomaterial grafted in fresh extraction sockets, together with resorbable collagen membranes, maintained its volume and favored the formation of new bone for future implant placement. |
| Cook et al., 2013 [22] | RCCT | 44 | Non-molar area | BBM | Non-cross-linked and cross-linked porcine collagen types I and III | Xenograft sponge (70% cross-linked bovine collagen type I) | 21 weeks | 6 | The use of xenograft material along with a resorbable collagen membrane for ridge preservation in non-molar extraction sites produced significantly more vital bone. |
| Pang et al., 2014 [23] | RCT | 30 | Molar area | BBM | Collagen | Spontaneous healing | 3 and 6 months | 0 | Bovine bone grafting together with absorbable collagen membrane were effective in preserving the alveolar ridge; however, the neoformed bone in the experimental group was of poor quality. |
| Scheyer et al., 2016 [24] | RCMCT | 40 | Molar | BBM | Collagen | DBBM with native collagen | 6 months | 3 | The horizontal measurements of the extraction socket were significantly higher for those treated with BBM y bilayer collagen membrane. Vertical bone changes were not significant between the two treatment modalities. At 6 months, 37 of the 40 sites assessed had sufficient ridge dimension for implant placement. sufficient for implant placement |
| Nart et al., 2017 [25] | RCCT | 26 | Non-molar area | BBM | Bilayer collagen | DBBM with 10% collagen | 5 months | 5 | A significant reduction in height and width was observed at the end of healing, but no statistically significant differences were observed between the BBM and DBBM-Collagen groups. Neoformed bone was similar in the experimental and control groups. |
| Jung et al., 2018 [26] | RCCT | 24 | Posterior areas (upper and lower jaw) | BBM | Bilayer collagen | Spontaneous healing | 3 and 6 months | 6 | At 3 and 6 months crestal height and width were significantly higher in the test group vs. control group. |
| Lim et al., 2019 [27] | RCCT | 33 | Molar areas | BBM | Bilayer collagen and native bilayer collagen | Spontaneous healing | 4 months | 4 | Despite the small sample size (29 sites), preservation of the horizontal alveolar ridge by open healing was advantageous; however, bone neoformation was better in the group treated with double collagen membrane, even though there was no statistical synification. |
| Cha et al., 2019 [28] | RCCT | 40 | Posterior upper molar area | BBM | Collagen | Spontaneous healing | 1,3 and 6 months | 1 | Preservation of the alveolar ridge in the posterior maxilla using BBM grafting was more effective and resulted in less need for sinus augmentation procedures at 6 months, compared to spontaneous healing of the alveolus. |
| Stumbras et al., 2020 [29] | RCT | 40 | Anterior maxilla (Incisor, canine area) | BBM | Native collagen | Spontaneous healing | 12 months | 8 | Significantly greater new bone formation at sites grafted with BBM and collagen membrane, compared to spontaneous healing. |
| Gabay et al., 2022 [30] | RCT | 30 | Premolar, canine or incisor area | BBM | Collagen | Spontaneous healing | 6 months | 2 | Preservation of the alveolar ridge by DBBM resulted in a tendency to reduce the vertical and horizontal dimension. |
| Study and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mardas et al. [19] | 1 | 1 | 0 | ? | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Mardas et al. [20] | 1 | 1 | 0 | ? | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Perelman-Karmon et al. [21] | ? | ? | 1 | ? | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ? | 8 |
| Cook et al. [22] | 1 | 1 | 0 | ? | ? | ? | 1 | 1 | 1 | 1 | 1 | 1 | ? | 8 |
| Pang et al. [23] | 1 | ? | 1 | ? | ? | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Scheyer et al. [24] | 1 | 1 | 1 | ? | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 |
| Nart et al. [25] | 1 | 1 | 1 | ? | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 |
| Jung et al. [26] | 1 | 1 | 1 | 1 | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| Lim et al. [27] | 1 | 1 | 1 | 1 | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| Cha et al. [28] | 1 | 1 | 1 | 1 | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| Stumbras et al. [29] | 1 | 1 | 1 | 1 | 1 | ? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| Gabay et al. [30] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Valverde, N.; Macedo de Sousa, B.; Blanco Rueda, J.A. Changes of the Alveolar Bone Ridge Using Bone Mineral Grafts and Collagen Membranes after Tooth Extraction: A Systematic Review and Meta-Analysis. Bioengineering 2024, 11, 565. https://doi.org/10.3390/bioengineering11060565
López-Valverde N, Macedo de Sousa B, Blanco Rueda JA. Changes of the Alveolar Bone Ridge Using Bone Mineral Grafts and Collagen Membranes after Tooth Extraction: A Systematic Review and Meta-Analysis. Bioengineering. 2024; 11(6):565. https://doi.org/10.3390/bioengineering11060565
Chicago/Turabian StyleLópez-Valverde, Nansi, Bruno Macedo de Sousa, and José Antonio Blanco Rueda. 2024. "Changes of the Alveolar Bone Ridge Using Bone Mineral Grafts and Collagen Membranes after Tooth Extraction: A Systematic Review and Meta-Analysis" Bioengineering 11, no. 6: 565. https://doi.org/10.3390/bioengineering11060565
APA StyleLópez-Valverde, N., Macedo de Sousa, B., & Blanco Rueda, J. A. (2024). Changes of the Alveolar Bone Ridge Using Bone Mineral Grafts and Collagen Membranes after Tooth Extraction: A Systematic Review and Meta-Analysis. Bioengineering, 11(6), 565. https://doi.org/10.3390/bioengineering11060565