
Preclinical and Preliminary Evaluation of Perceived Image Quality of AI-Processed Low-Dose CBCT Analysis of a Single Tooth


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
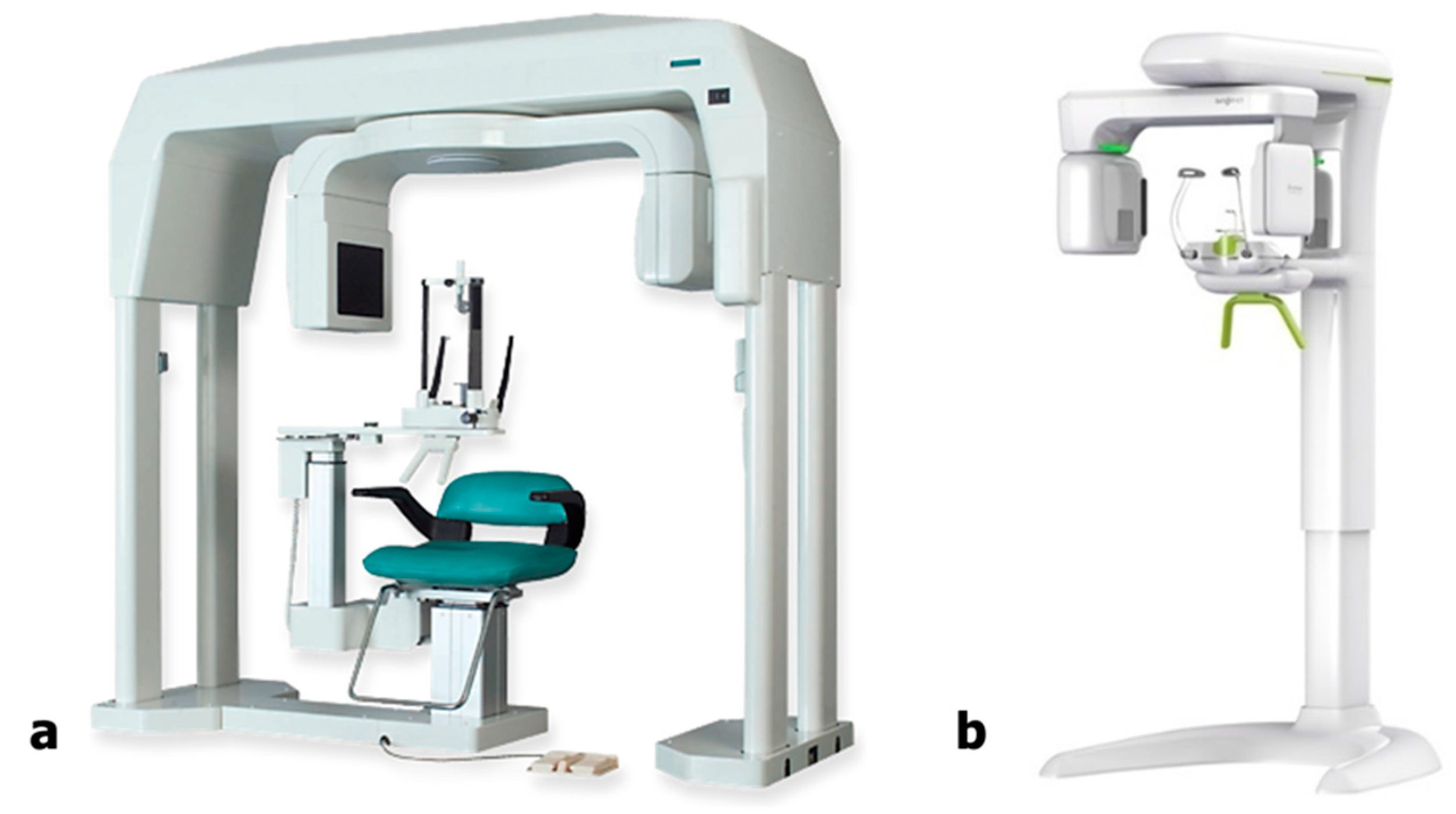
2.1. CBCT Scanning Protocol
2.2. Dose-Area Product Measurement
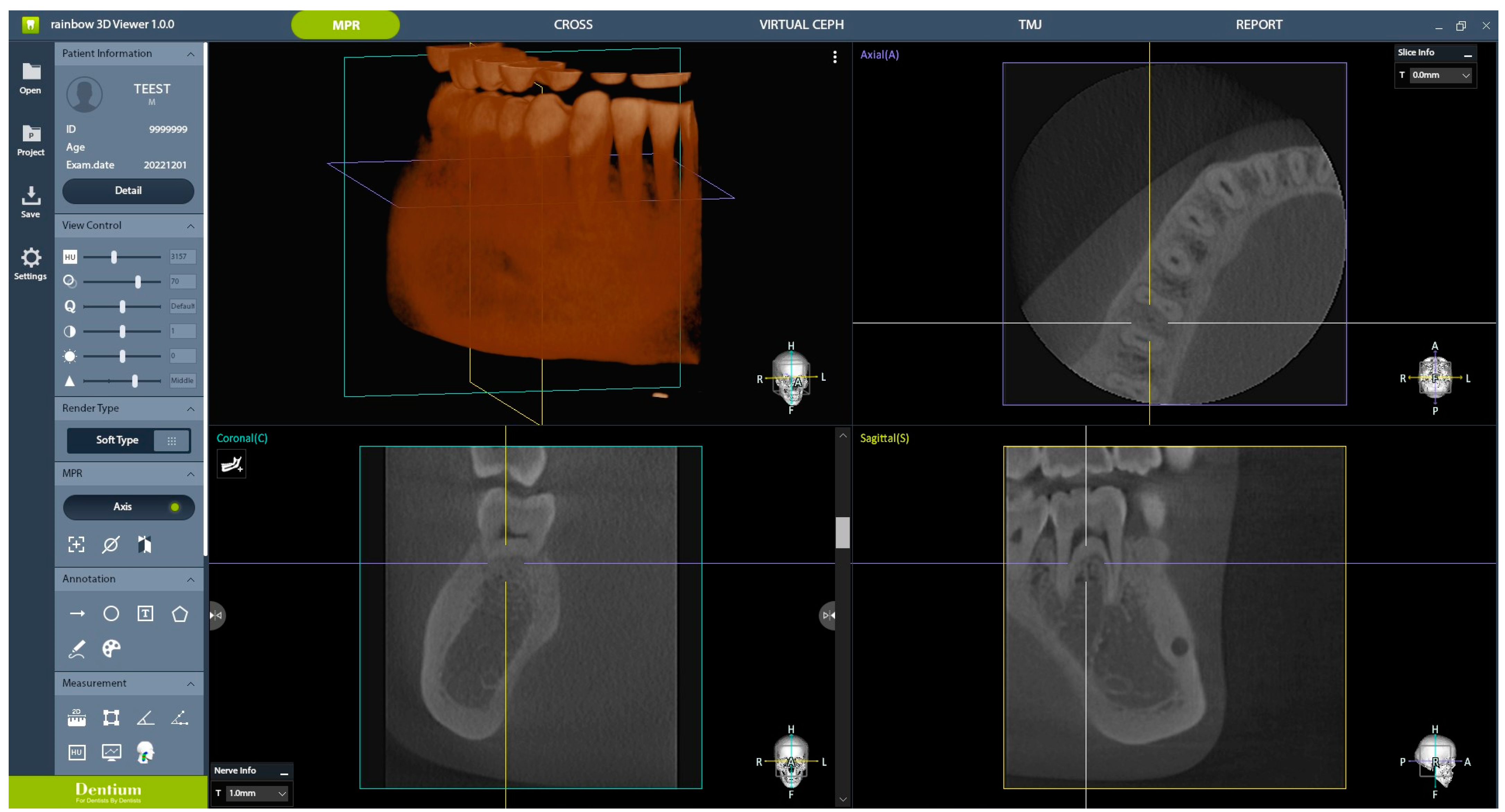
2.3. AI Processing
2.4. Subjective Clinical Image Quality Evaluation
2.5. Statistical Analyses
3. Results
3.1. DAP Measurement
3.2. Subjective Image Quality Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ee, J.; Fayad, M.I.; Johnson, B.R. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J. Endod. 2014, 40, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Chia, H.N.; Wu, B.M. Recent advances in 3D printing of biomaterials. J. Biol. Eng. 2015, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Velvart, P.; Hecker, H.; Tillinger, G. Detection of the apical lesion and the mandibular canal in conventional radiography and computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont. 2001, 92, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.J.; Yang, B.E.; Park, I.Y.; Yi, S.; On, S.W.; Kim, Y.H.; Kang, S.H.; Byun, S.H. Effectiveness of cone-beam computed tomography-generated cephalograms using artificial intelligence cephalometric analysis. Sci. Rep. 2022, 12, 20585. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, F.; Minorati, D.; Nessi, R.; Gagliani, M.; Uslenghi, C. The measurement parameters in dental radiography: A comparison between traditional and digital technics. Radiol. Medica 1996, 91, 364–369. [Google Scholar]
- Paurazas, S.B.; Geist, J.R.; Pink, F.E.; Hoen, M.M.; Steiman, H.R. Comparison of diagnostic accuracy of digital imaging by using CCD and CMOS-APS sensors with E-speed film in the detection of periapical bony lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont. 2000, 89, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R. Cone beam CT for dental and maxillofacial imaging: Dose matters. Radiat. Prot. Dosim. 2015, 165, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Lofthag-Hansen, S.; Huumonen, S.; Gröndahl, K.; Gröndahl, H.-G. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont. 2007, 103, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Son, J.; Lee, D.J.; Ahn, K.M. Radiological features of Stafne mandibular bone cavity in panoramic image and cone beam computed tomography. Maxillofac. Plast. Reconstr. Surg. 2024, 46, 9. [Google Scholar] [CrossRef] [PubMed]
- Abella, F.; Mercadé, M.; Duran-Sindreu, F.; Roig, M. Managing severe curvature of radix entomolaris: Three-dimensional analysis with cone beam computed tomography. Int. Endod. J. 2011, 44, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Cohenca, N.; Simon, J.H.; Roges, R.; Morag, Y.; Malfaz, J.M. Clinical indications for digital imaging in dento-alveolar trauma. Part 1: Traumatic injuries. Dent. Traumatol. 2007, 23, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Shemesh, H.; Cristescu, R.C.; Wesselink, P.R.; Wu, M.-K. The use of cone-beam computed tomography and digital periapical radiographs to diagnose root perforations. J. Endod. 2011, 37, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Jeon, T.H.; Jun, S.H.; Kwon, J.J. Evaluation of mandibular lingula and foramen location using 3-dimensional mandible models reconstructed by cone-beam computed tomography. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 30. [Google Scholar] [CrossRef] [PubMed]
- Nakata, K.; Naitoh, M.; Izumi, M.; Inamoto, K.; Ariji, E.; Nakamura, H. Effectiveness of dental computed tomography in diagnostic imaging of periradicular lesion of each root of a multirooted tooth: A case report. J. Endod. 2006, 32, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, S.J. Effective dose equivalent and effective dose: Comparison for common projections in oral and maxillofacial radiology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont. 2000, 90, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Berkhout, W. The ALARA-principle. Backgrounds and enforcement in dental practices. Ned. Tijdschr. Voor Tandheelkd. 2015, 122, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Brendlin, A.S.; Plajer, D.; Chaika, M.; Wrazidlo, R.; Estler, A.; Tsiflikas, I.; Artzner, C.P.; Afat, S.; Bongers, M.N. Ai denoising significantly improves image quality in whole-body low-dose computed tomography staging. Diagnostics 2022, 12, 225. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Lim, C.Y.; Shin, J.; Chung, M.J.; Jung, Y.G. Enhanced artificial intelligence-based diagnosis using CBCT with internal denoising: Clinical validation for discrimination of fungal ball, sinusitis, and normal cases in the maxillary sinus. Comput. Methods Programs Biom. 2023, 240, 107708. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, N.K.; Zou, B.; Park, J.H.; Choi, T.H. Reliability of Artificial Intelligence-based Cone Beam Computed Tomography Integration with Digital Dental Images. J. Vis. Exp. 2024, 204, e66014. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Kim, B.K.; Chung, M.J.; Cho, H.B.; Cho, B.H.; Jung, Y.G. Detection of maxillary sinus fungal ball via 3-D CNN-based artificial intelligence: Fully automated system and clinical validation. PLoS ONE 2022, 17, e0263125. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhang, Y.; Kalra, M.K.; Lin, F.; Chen, Y.; Liao, P.; Zhou, J.; Wang, G. Low-dose CT with a residual encoder-decoder convolutional neural network. IEEE Trans. Med. Imaging 2017, 36, 2524–2535. [Google Scholar] [CrossRef] [PubMed]
- Kida, S.; Nakamoto, T.; Nakano, M.; Nawa, K.; Haga, A.; Kotoku Ji Yamashita, H.; Nakagawa, K. Cone beam computed tomography image quality improvement using a deep convolutional neural network. Cureus 2018, 10, e2548. [Google Scholar] [CrossRef] [PubMed]
- Lina, J.; Xu, H.; Aimin, H.; Beibei, J.; Zhiguo, G. A densely connected LDCT image denoising network based on dual-edge extraction and multi-scale attention under compound loss. J. Xray Sci. Technol. 2023, 31, 1207–1226. [Google Scholar] [CrossRef] [PubMed]
- Abdi, A.J.; Mussmann, B.; Mackenzie, A.; Gerke, O.; Jorgensen, G.M.; Bechsgaard, T.E.; Jensen, J.; Olsen, L.B.; Andersen, P.E. Visual Evaluation of Image Quality of a Low Dose 2D/3D Slot Scanner Imaging System Compared to Two Conventional Digital Radiography X-ray Imaging Systems. Diagnostics 2021, 11, 1932. [Google Scholar] [CrossRef] [PubMed]
- Yalcinkaya, S.; Kunzel, A.; Willers, R.; Thoms, M.; Becker, J. Subjective image quality of digitally filtered radiographs acquired by the Durr Vistascan system compared with conventional radiographs. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont. 2006, 101, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Ngan, D.C.; Kharbanda, O.P.; Geenty, J.P.; Darendeliler, M. Comparison of radiation levels from computed tomography and conventional dental radiographs. Aust. Orthod. J. 2003, 19, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzi, T.; Menz, R.; Verna, C.; Bornstein, M.M.; Dagassan-Berndt, D. Effect of field of view (FOV) positioning and shielding on radiation dose in paediatric CBCT. Dentomaxillofacial Radiol. 2022, 51, 20210316. [Google Scholar] [CrossRef] [PubMed]
- Heo, M.-S.; Kim, J.-E.; Hwang, J.-J.; Han, S.-S.; Kim, J.-S.; Yi, W.-J.; Park, I.-W. Artificial intelligence in oral and maxillofacial radiology: What is currently possible? Dentomaxillofacial Radiol. 2021, 50, 20200375. [Google Scholar] [CrossRef]
- Zhang, Y.; Yue, N.; Su, M.Y.; Liu, B.; Ding, Y.; Zhou, Y.; Wang, H.; Kuang, Y.; Nie, K. Improving CBCT quality to CT level using deep learning with generative adversarial network. Med. Phys. 2021, 48, 2816–2826. [Google Scholar] [CrossRef]
- Yan, R.; Liu, Y.; Liu, Y.; Wang, L.; Zhao, R.; Bai, Y.; Gui, Z. Image denoising for low-dose CT via convolutional dictionary learning and neural network. IEEE Trans. Comput. Imaging 2023, 9, 83–93. [Google Scholar] [CrossRef]
- Setzer, F.C.; Hinckley, N.; Kohli, M.R.; Karabucak, B. A survey of cone-beam computed tomographic use among endodontic practitioners in the United States. J. Endod. 2017, 43, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Rajeevan, M.; Chandler, N.P.; Makdissi, J.; San Chong, B. A survey of cone beam computed tomography (CBCT) use among endodontic practitioners in the UK. Endod. Pract. Today 2018, 12, 29. [Google Scholar]
- Costa, F.F.; Pinheiro, L.R.; Umetsubo, O.S.; dos Santos Júnior, O.; Gaia, B.F.; Cavalcanti, M.G.P. Influence of cone-beam computed tomographic scan mode for detection of horizontal root fracture. J. Endod. 2014, 40, 1472–1476. [Google Scholar] [CrossRef] [PubMed]
- Li, G. Patient radiation dose and protection from cone-beam computed tomography. Imaging Sci. Dent. 2013, 43, 63. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Mode | Protocol No. | FOV (cm2) | Voxel Size (µm) | Exposure Time (s) | kVp | mA |
|---|---|---|---|---|---|---|---|
| Experimental group | Non-filter | 1 | 10 × 8 | 249 | 20 | 95 | 10 |
| 2 * | 10 × 8 | 390 | 10 | 95 | 10 | ||
| Filter | 3 | 10 × 8 | 249 | 20 | 95 | 10 | |
| 4 * | 10 × 8 | 390 | 10 | 95 | 10 | ||
| Control group | Standard | 5 | 5 × 5 | 100 | 17 | 80 | 8 |
| Model | Mode | Protocol No. | DAP (µGy·m2) | DAP per FOV (µGy·m2/cm2) |
|---|---|---|---|---|
| Experimental group (10 × 8) | Non-filter | 1 | 261.503 | 3.269 |
| 2 * | 130.693 | 1.634 | ||
| Filter | 3 | 55.49 | 0.694 | |
| 4 * | 27.573 | 0.335 | ||
| Control group (5 × 5) | 5 | 70.575 | 2.823 |
| Protocol No. | 1 | 1 | 2 * | 2 * | 3 | 3 | 4 * | 4 * | 5 |
|---|---|---|---|---|---|---|---|---|---|
| Parameter | (AI) | (AI) | (AI) | (AI) | |||||
| Number of roots | 5.625 | 5.75 | 5.5 | 5.375 | 5.375 | 4.75 | 4.25 | 3.5 | 5.5 |
| Number of root canals | 5.875 | 5.75 | 5.375 | 5.25 | 5.625 | 4.75 | 3.75 | 3.125 | 5.5 |
| Enamel–dentin differentiation | 5.125 | 5.625 | 5.5 | 4.375 | 4.375 | 4 | 3.875 | 2.75 | 4.375 |
| Lamina dura | 4.5 | 3.5 | 4.5 | 3.625 | 3.875 | 2.75 | 3.375 | 2 | 4 |
| PDL space | 5 | 4.625 | 4.5 | 4.5 | 4.125 | 3.625 | 3.375 | 2.375 | 5.25 |
| Trabecular pattern | 5.25 | 4 | 4.5 | 3.75 | 4.375 | 2.125 | 3.25 | 1.75 | 5.375 |
| Cortex of alveolar crest | 5.625 | 5 | 5.25 | 4.5 | 4.625 | 3.5 | 3.875 | 2.875 | 5.125 |
| Cortex of mandibular canal | 5.75 | 5.5 | 5.625 | 5.125 | 5.25 | 4 | 4.125 | 3.75 | 5.5 |
| Furcation | 5.5 | 5.5 | 5.25 | 4.5 | 5 | 3.75 | 3.75 | 3 | 5 |
| Cortex of mandible | 5.5 | 5.5 | 5.75 | 5.5 | 5.5 | 5 | 4.75 | 4.25 | 5 |
| Overall image quality for PA lesion diagnosis | 4.75 | 4.375 | 4.75 | 4 | 4 | 2.5 | 2.75 | 2.25 | 5.25 |
| Average | 5.32 | 5.01 | 5.14 | 4.59 | 4.74 | 3.71 | 3.74 | 2.86 | 5.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, N.-H.; Yang, B.-E.; Kang, S.-H.; Kim, Y.-H.; Na, J.-Y.; Kim, J.-E.; Byun, S.-H. Preclinical and Preliminary Evaluation of Perceived Image Quality of AI-Processed Low-Dose CBCT Analysis of a Single Tooth. Bioengineering 2024, 11, 576. https://doi.org/10.3390/bioengineering11060576
Kim N-H, Yang B-E, Kang S-H, Kim Y-H, Na J-Y, Kim J-E, Byun S-H. Preclinical and Preliminary Evaluation of Perceived Image Quality of AI-Processed Low-Dose CBCT Analysis of a Single Tooth. Bioengineering. 2024; 11(6):576. https://doi.org/10.3390/bioengineering11060576
Chicago/Turabian StyleKim, Na-Hyun, Byoung-Eun Yang, Sam-Hee Kang, Young-Hee Kim, Ji-Yeon Na, Jo-Eun Kim, and Soo-Hwan Byun. 2024. "Preclinical and Preliminary Evaluation of Perceived Image Quality of AI-Processed Low-Dose CBCT Analysis of a Single Tooth" Bioengineering 11, no. 6: 576. https://doi.org/10.3390/bioengineering11060576
APA StyleKim, N.-H., Yang, B.-E., Kang, S.-H., Kim, Y.-H., Na, J.-Y., Kim, J.-E., & Byun, S.-H. (2024). Preclinical and Preliminary Evaluation of Perceived Image Quality of AI-Processed Low-Dose CBCT Analysis of a Single Tooth. Bioengineering, 11(6), 576. https://doi.org/10.3390/bioengineering11060576