
Conceptualizing Scaffold Guided Breast Tissue Regeneration in a Preclinical Large Animal Model
 , , , ,
, , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scaffold Design, Manufacturing, and Characterization
2.2. Large Animal Study
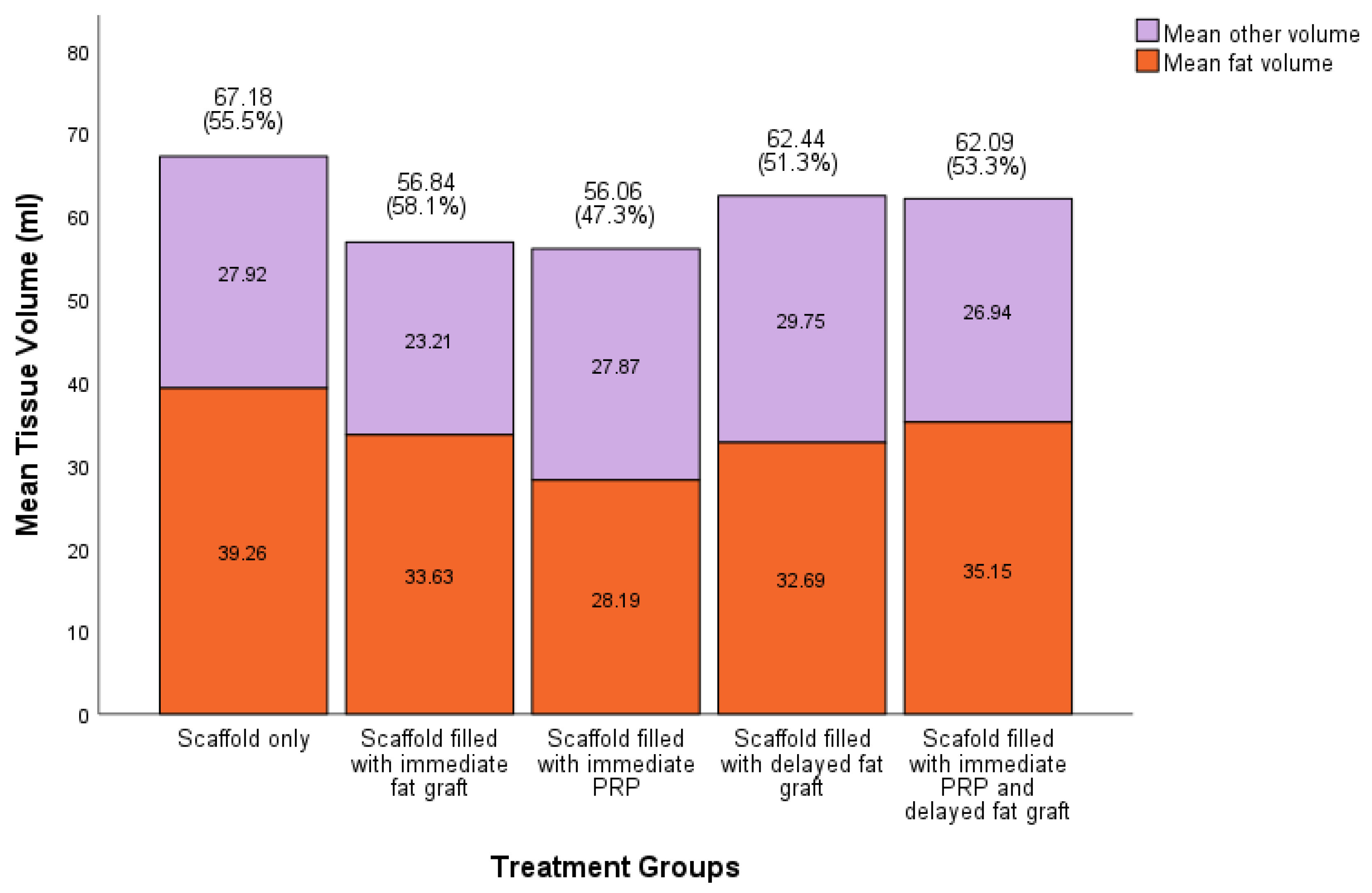
- 50 mL fat graft injection only, no scaffold implanted (control);
- Scaffold only implanted (control);
- Scaffold implanted and filled with 50 mL immediate fat graft;
- Scaffold implanted and filled with 50 mL immediate platelet-rich plasma;
- Scaffold implanted and filled with 50 mL delayed fat graft after four weeks;
- Scaffold implanted and filled with 50 mL immediate platelet-rich plasma, then 50 mL delayed fat graft after four weeks.
2.3. Post-Humous Analysis
2.4. Statistical Analysis
3. Results
3.1. Macroscopic Analysis
3.2. Volume and Distribution
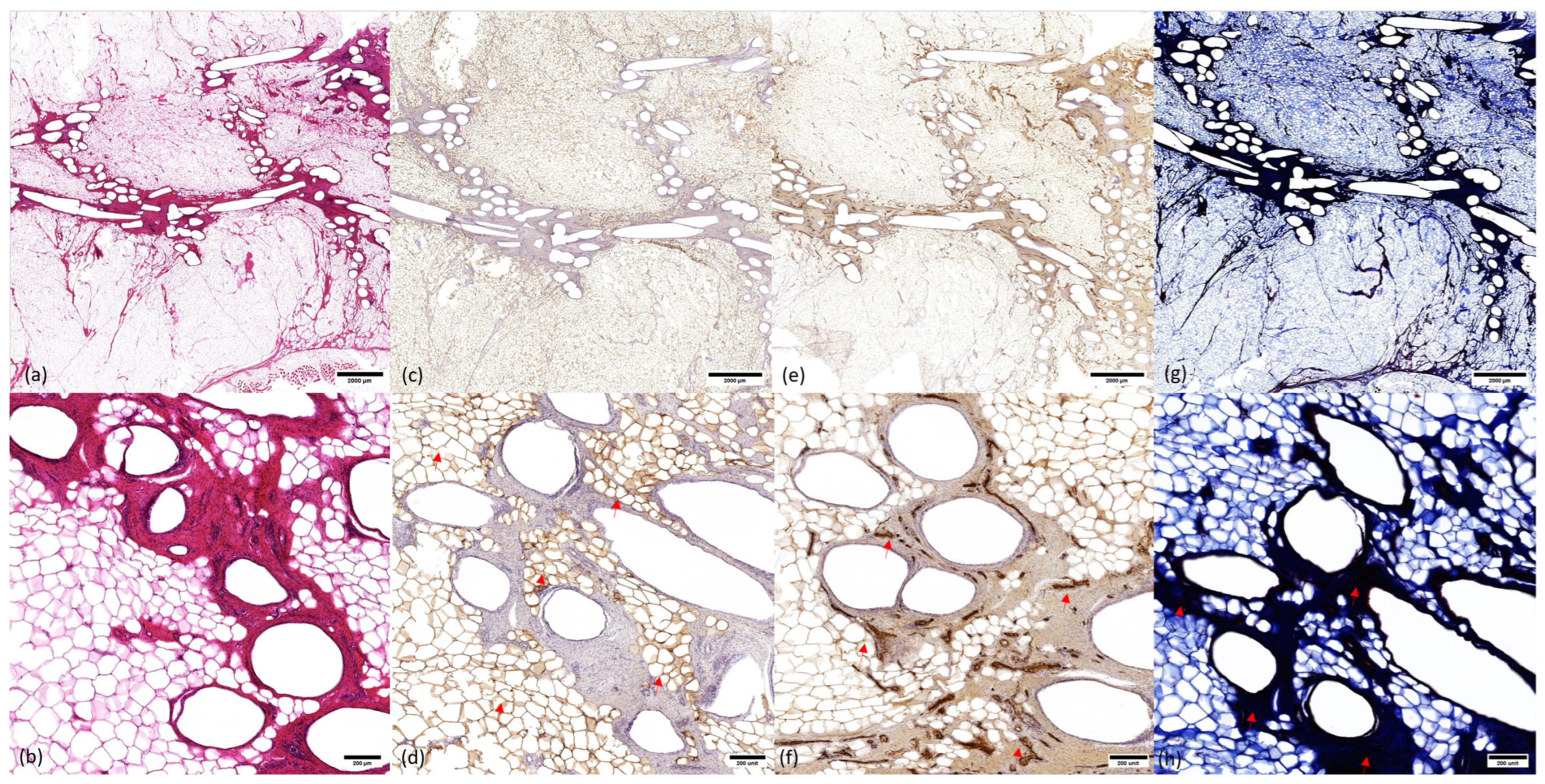
3.3. Microscopic Analysis
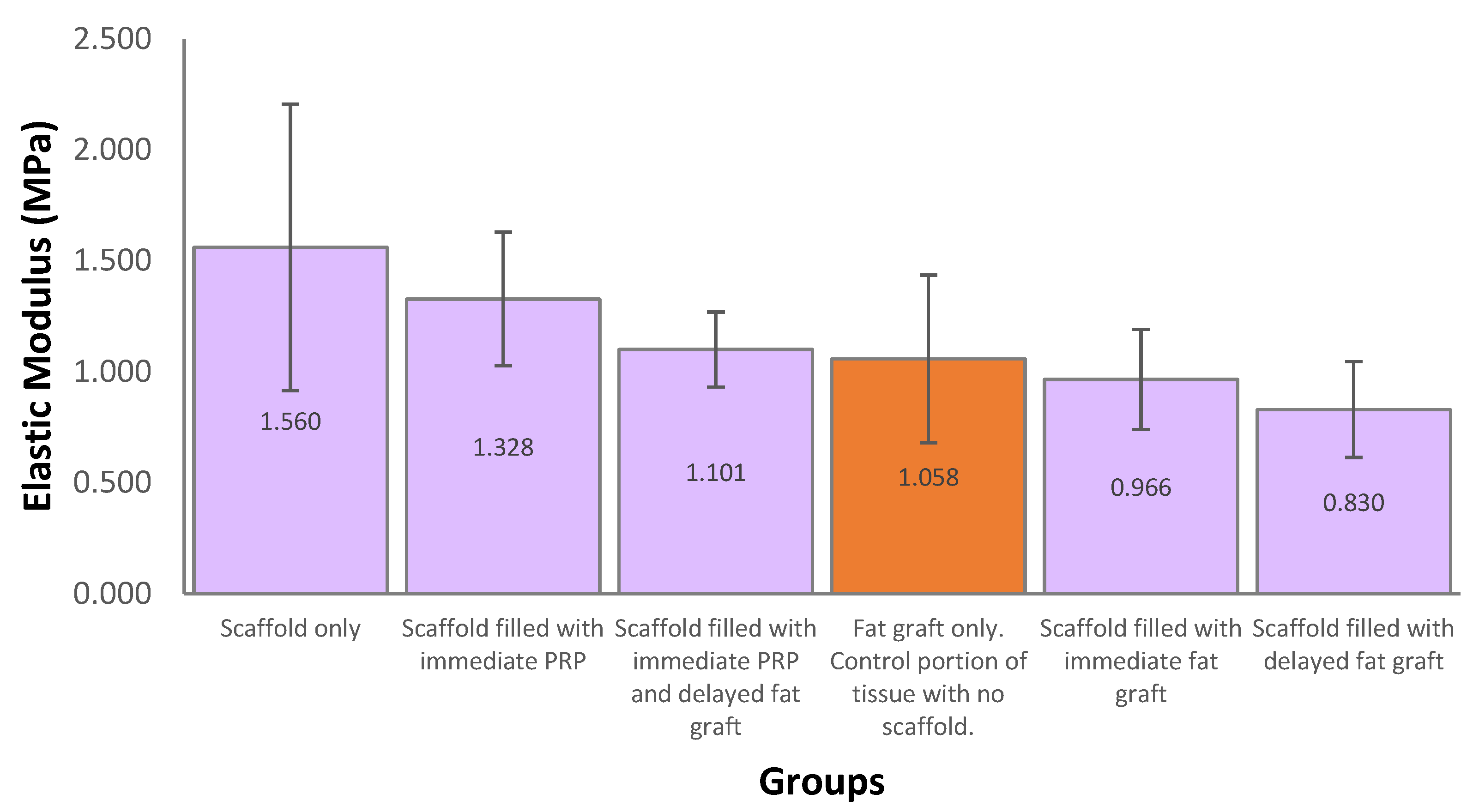
3.4. Mechanical Testing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Rowland, J.H.; Desmond, K.A.; Meyerowitz, B.E.; Belin, T.R.; Wyatt, G.E.; Ganz, P.A. Role of breast reconstructive surgery in physical and emotional outcomes among breast cancer survivors. J. Natl. Cancer Inst. 2000, 92, 1422–1429. [Google Scholar] [CrossRef] [PubMed]
- Lovelace, D.L.; McDaniel, L.R.; Golden, D. Long-term effects of breast cancer surgery, treatment, and survivor care. J. Midwifery Women’s Health 2019, 64, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Panchal, H.; Matros, E. Current Trends in Postmastectomy Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 7s–13s. [Google Scholar] [CrossRef]
- Headon, H.; Kasem, A.; Mokbel, K. Capsular Contracture after Breast Augmentation: An Update for Clinical Practice. Arch. Plast. Surg. 2015, 42, 532–543. [Google Scholar] [CrossRef] [PubMed]
- Handel, N.; Cordray, T.; Gutierrez, J.; Jensen, J.A. A long-term study of outcomes, complications, and patient satisfaction with breast implants. Plast. Reconstr. Surg. 2006, 117, 757–767, discussion 768–772. [Google Scholar] [CrossRef] [PubMed]
- Coroneos, C.J.; Selber, J.C.; Offodile, A.C.I.; Butler, C.E.; Clemens, M.W. US FDA Breast Implant Postapproval Studies: Long-term Outcomes in 99,993 Patients. Ann. Surg. 2019, 269, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Finlay, B.; Kollias, V.; Hall, K.A.; Clement, Z.; Bingham, J.; Whitfield, R.; Kollias, J.; Bochner, M. Long-term outcomes of breast reconstruction and the need for revision surgery. ANZ J. Surg. 2021, 91, 1751–1758. [Google Scholar] [CrossRef] [PubMed]
- Visser, N.J.; Damen, T.H.C.; Timman, R.; Hofer, S.O.P.; Mureau, M.A.M. Surgical Results, Aesthetic Outcome, and Patient Satisfaction after Microsurgical Autologous Breast Reconstruction following Failed Implant Reconstruction. Plast. Reconstr. Surg. 2010, 126, 26–36. [Google Scholar] [CrossRef]
- Eltahir, Y.; Werners, L.L.C.H.; Dreise, M.M.; Zeijlmans van Emmichoven, I.A.; Werker, P.M.N.; de Bock, G.H. Which Breast Is the Best? Successful Autologous or Alloplastic Breast Reconstruction: Patient-Reported Quality-of-Life Outcomes. Plast. Reconstr. Surg. 2015, 135, 43–50. [Google Scholar] [CrossRef]
- Fracon, S.; Renzi, N.; Manara, M.; Ramella, V.; Papa, G.; Arnež, Z. Patient satisfaction after breast reconstruction: Implants vs. autologous tissues. Acta Chir. Plast. 2018, 59, 120–128. [Google Scholar]
- Chang, E.I.; Chang, E.I.; Soto-Miranda, M.A.; Zhang, H.; Nosrati, N.; Robb, G.L.; Chang, D.W. Comprehensive analysis of donor-site morbidity in abdominally based free flap breast reconstruction. Plast. Reconstr. Surg. 2013, 132, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Agha, R.A.; Fowler, A.J.; Herlin, C.; Goodacre, T.E.E.; Orgill, D.P. Use of autologous fat grafting for breast reconstruction: A systematic review with meta-analysis of oncological outcomes. J. Plast. Reconstr. Aesthetic Surg. 2015, 68, 143–161. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.R.; Saboeiro, A.P. Fat Grafting to the Breast Revisited: Safety and Efficacy. Plast. Reconstr. Surg. 2007, 119, 775–785. [Google Scholar] [CrossRef] [PubMed]
- Herly, M.; Ørholt, M.; Larsen, A.; Pipper, C.B.; Bredgaard, R.; Gramkow, C.S.; Katz, A.J.; Drzewiecki, K.T.; Vester-Glowinski, P.V. Efficacy of breast reconstruction with fat grafting: A systematic review and meta-analysis. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 1740–1750. [Google Scholar] [CrossRef]
- Berkane, Y.; Oubari, H.; van Dieren, L.; Charlès, L.; Lupon, E.; McCarthy, M.; Cetrulo, C.L., Jr.; Bertheuil, N.; Uygun, B.E.; Smadja, D.M.; et al. Tissue engineering strategies for breast reconstruction: A literature review of current advances and future directions. Ann. Transl. Med. 2024, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Findlay, M.W.; Dolderer, J.H.; Trost, N.; Craft, R.O.; Cao, Y.; Cooper-White, J.; Stevens, G.; Morrison, W.A. Tissue-engineered breast reconstruction: Bridging the gap toward large-volume tissue engineering in humans. Plast. Reconstr. Surg. 2011, 128, 1206–1215. [Google Scholar] [CrossRef] [PubMed]
- Morrison, W.A.; Marre, D.; Grinsell, D.; Batty, A.; Trost, N.; O’Connor, A.J. Creation of a large adipose tissue construct in humans using a tissue-engineering chamber: A step forward in the clinical application of soft tissue engineering. EBioMedicine 2016, 6, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Rehnke, R.D.; M Asher Schusterman, I.; Clarke, J.M.; Price, B.C.; Waheed, U.; Debski, R.E.; Badylak, S.F.; Rubin, J.P. Breast reconstruction using a three-dimensional absorbable mesh scaffold and autologous fat grafting: A composite strategy based on tissue-engineering principles. Plast. Reconstr. Surg. 2020, 146, 409e–413e. [Google Scholar] [CrossRef]
- Hwang, K.; Wu, X. Breast Reconstruction Using a Three-Dimensional Absorbable Mesh Scaffold and Autologous Fat Grafting: A Composite Strategy Based on Tissue-Engineering Principles. Plast. Reconstr. Surg. 2021, 148, 660e–661e. [Google Scholar] [CrossRef]
- Woodruff, M.A.; Hutmacher, D.W. The return of a forgotten polymer—Polycaprolactone in the 21st century. Prog. Polym. Sci. 2010, 35, 1217–1256. [Google Scholar] [CrossRef]
- Lam, C.X.; Hutmacher, D.W.; Schantz, J.T.; Woodruff, M.A.; Teoh, S.H. Evaluation of polycaprolactone scaffold degradation for 6 months in vitro and in vivo. J. Biomed. Mater. Res. A 2009, 90, 906–919. [Google Scholar] [CrossRef] [PubMed]
- Mohseni, M.; Bas, O.; Castro, N.J.; Schmutz, B.; Hutmacher, D.W. Additive biomanufacturing of scaffolds for breast reconstruction. Addit. Manuf. 2019, 30, 100845. [Google Scholar] [CrossRef]
- ISO 11137-1:2006; Sterilization of Health Care Products—Radiation. International Organization for Standardization: Geneva, Switzerland. Available online: https://www.iso.org/standard/33952.html (accessed on 3 June 2024).
- Cheng, M.; Janzekovic, J.; Mohseni, M.; Medeiros Savi, F.; McGovern, J.; Galloway, G.; Wong, C.; Saifzadeh, S.; Wagels, M.; Hutmacher, D.W. A preclinical animal model for the study of scaffold-guided breast tissue engineering. Tissue Eng. Part. C Methods 2021, 27, 366–377. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, F.J.; Madsen, M.T.; Strathe, A.B.; Svalastoga, E. Hounsfield Unit dynamics of adipose tissue and non-adipose soft tissues in growing pigs. Res. Vet. Sci. 2008, 84, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Eto, H.; Kato, H.; Suga, H.; Aoi, N.; Doi, K.; Kuno, S.; Yoshimura, K. The fate of adipocytes after nonvascularized fat grafting: Evidence of early death and replacement of adipocytes. Plast. Reconstr. Surg. 2012, 129, 1081–1092. [Google Scholar] [CrossRef] [PubMed]
- Shim, K.-S.; Ryu, D.H.; Jo, H.-S.; Kim, K.-B.; Kim, D.-H.; Park, Y.-K.; Heo, M.; Cho, H.-E.; Yoon, E.-S.; Lee, W.J. Breast tissue reconstruction using polycaprolactone ball scaffolds in a partial mastectomy pig model. Tissue Eng. Regen. Med. 2023, 20, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Chhaya, M.P.; Balmayor, E.R.; Hutmacher, D.W.; Schantz, J.T. Transformation of Breast Reconstruction via Additive Biomanufacturing. Sci. Rep. 2016, 6, 28030. [Google Scholar] [CrossRef] [PubMed]
- Vandeweyer, E.; Hertens, D. Quantification of glands and fat in breast tissue: An experimental determination. Ann. Anat.-Anat. Anz. 2002, 184, 181–184. [Google Scholar] [CrossRef]
- Gaskin, K.M.; Peoples, G.E.; McGhee, D.E. The fibro-adipose structure of the female breast: A dissection study. Clin. Anat. 2020, 33, 146–155. [Google Scholar] [CrossRef]
- Faglin, P.; Gradwohl, M.; Depoortere, C.; Germain, N.; Drucbert, A.-S.; Brun, S.; Nahon, C.; Dekiouk, S.; Rech, A.; Azaroual, N.; et al. Rationale for the design of 3D-printable bioresorbable tissue-engineering chambers to promote the growth of adipose tissue. Sci. Rep. 2020, 10, 11779. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.M.; Papadimitrakopoulos, F.; Burgess, D.J. Biomaterials/tissue interactions: Possible solutions to overcome foreign body response. AAPS J. 2010, 12, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.W.; Fligor, J.E.; Janes, L.E.; Dumanian, G.A. Implant porosity and the foreign body response. Plast. Reconstr. Surg. 2018, 141, 103e–112e. [Google Scholar] [CrossRef] [PubMed]
- Ramiao, N.G.; Martins, P.S.; Rynkevic, R.; Fernandes, A.A.; Barroso, M.; Santos, D.C. Biomechanical properties of breast tissue, a state-of-the-art review. Biomech. Model. Mechanobiol. 2016, 15, 1307–1323. [Google Scholar] [CrossRef] [PubMed]
- Janzekovic, J.; Hunt, J.; Peltz, T.; Wagels, M.; Brown, T.; Hutmacher, D.W. Biomechanical principles of breast implants and current state of research in soft tissue engineering for cosmetic breast augmentation. Aesthetic Plast. Surg. 2022, 46, 1–10. [Google Scholar] [CrossRef]
- Rinker, B.; Veneracion, M.; Walsh, C.P. Breast ptosis: Causes and cure. Ann. Plast. Surg. 2010, 64, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Cao, L.; Wei, H.; Zhu, D.; Zhou, G.; Wang, J.; Guo, S. Effect of 3D printed polycaprolactone scaffold with a bionic structure on the early stage of fat grafting. Mater. Sci. Eng. C 2021, 123, 111973. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.E.; Janzekovic, J.; Theile, H.J.; Rutherford-Heard, C.; Wille, M.-L.; Cole, C.; Lloyd, T.B.; Theile, R.J.; Wagels, M.; Hutmacher, D.W. Pectus excavatum camouflage: A new technique using a tissue engineered scaffold. Eur. J. Plast. Surg. 2022, 45, 177–182. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, M.; Janzekovic, J.; Finze, R.; Mohseni, M.; Saifzadeh, S.; Savi, F.M.; Ung, O.; Wagels, M.; Hutmacher, D.W. Conceptualizing Scaffold Guided Breast Tissue Regeneration in a Preclinical Large Animal Model. Bioengineering 2024, 11, 593. https://doi.org/10.3390/bioengineering11060593
Cheng M, Janzekovic J, Finze R, Mohseni M, Saifzadeh S, Savi FM, Ung O, Wagels M, Hutmacher DW. Conceptualizing Scaffold Guided Breast Tissue Regeneration in a Preclinical Large Animal Model. Bioengineering. 2024; 11(6):593. https://doi.org/10.3390/bioengineering11060593
Chicago/Turabian StyleCheng, Matthew, Jan Janzekovic, Ronja Finze, Mina Mohseni, Siamak Saifzadeh, Flavia M. Savi, Owen Ung, Michael Wagels, and Dietmar W. Hutmacher. 2024. "Conceptualizing Scaffold Guided Breast Tissue Regeneration in a Preclinical Large Animal Model" Bioengineering 11, no. 6: 593. https://doi.org/10.3390/bioengineering11060593