

Ultrasound Elastography Assessment of Knee Intra-Articular Adhesions at Varying Knee Angles



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Subjective Assessments
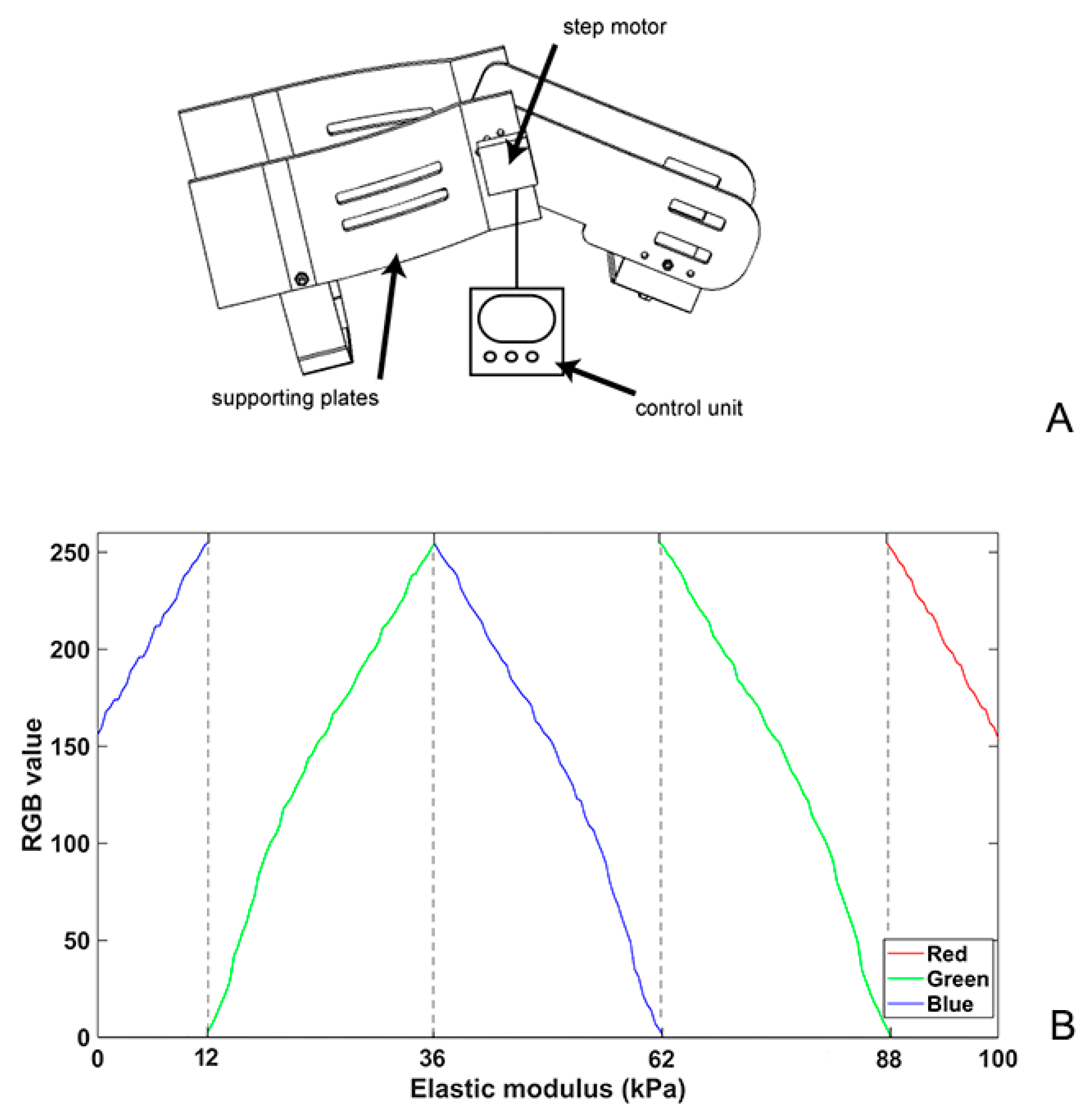
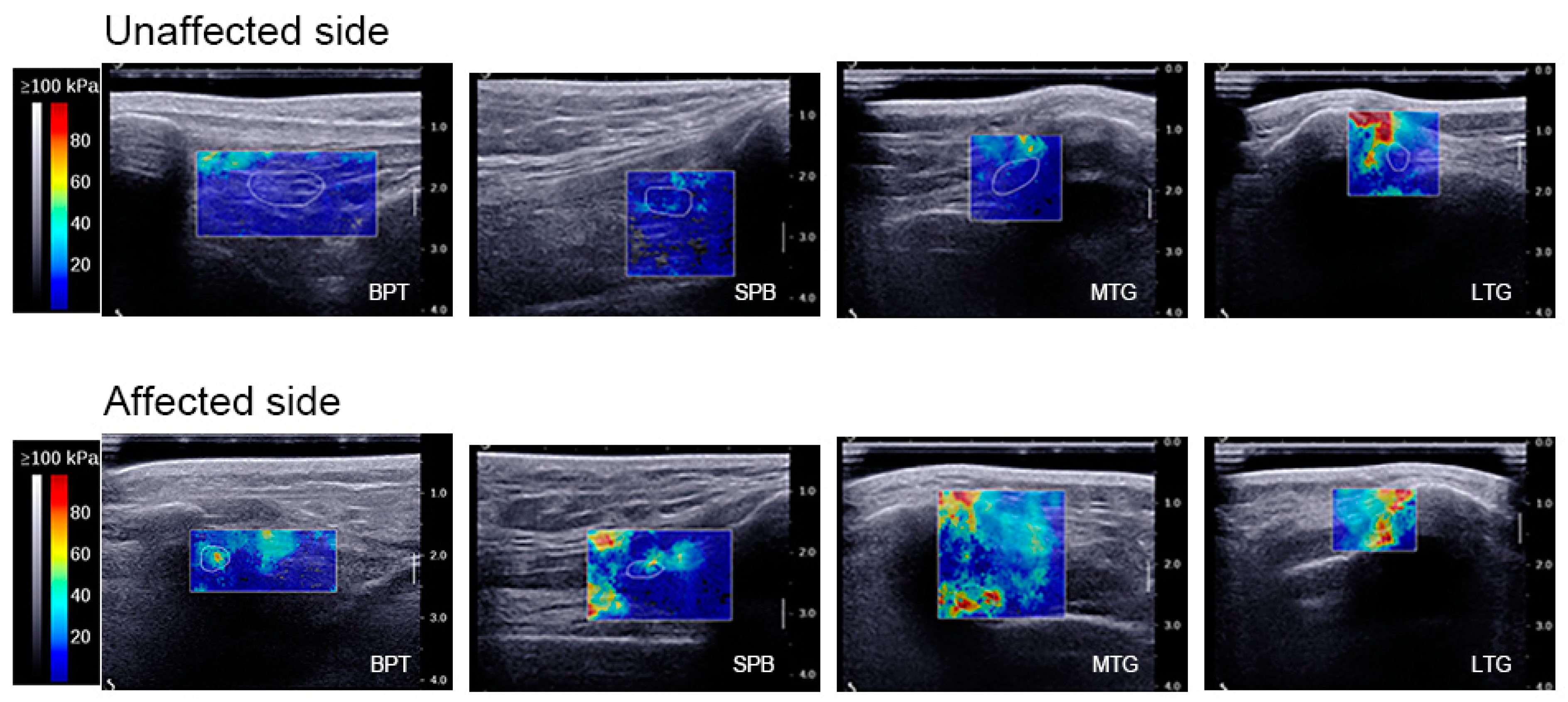
2.3.1. SWE
2.3.2. Knee ROM
2.3.3. Knee Injury and Osteoarthritis Outcome Score (KOOS)
2.3.4. The ICC Test
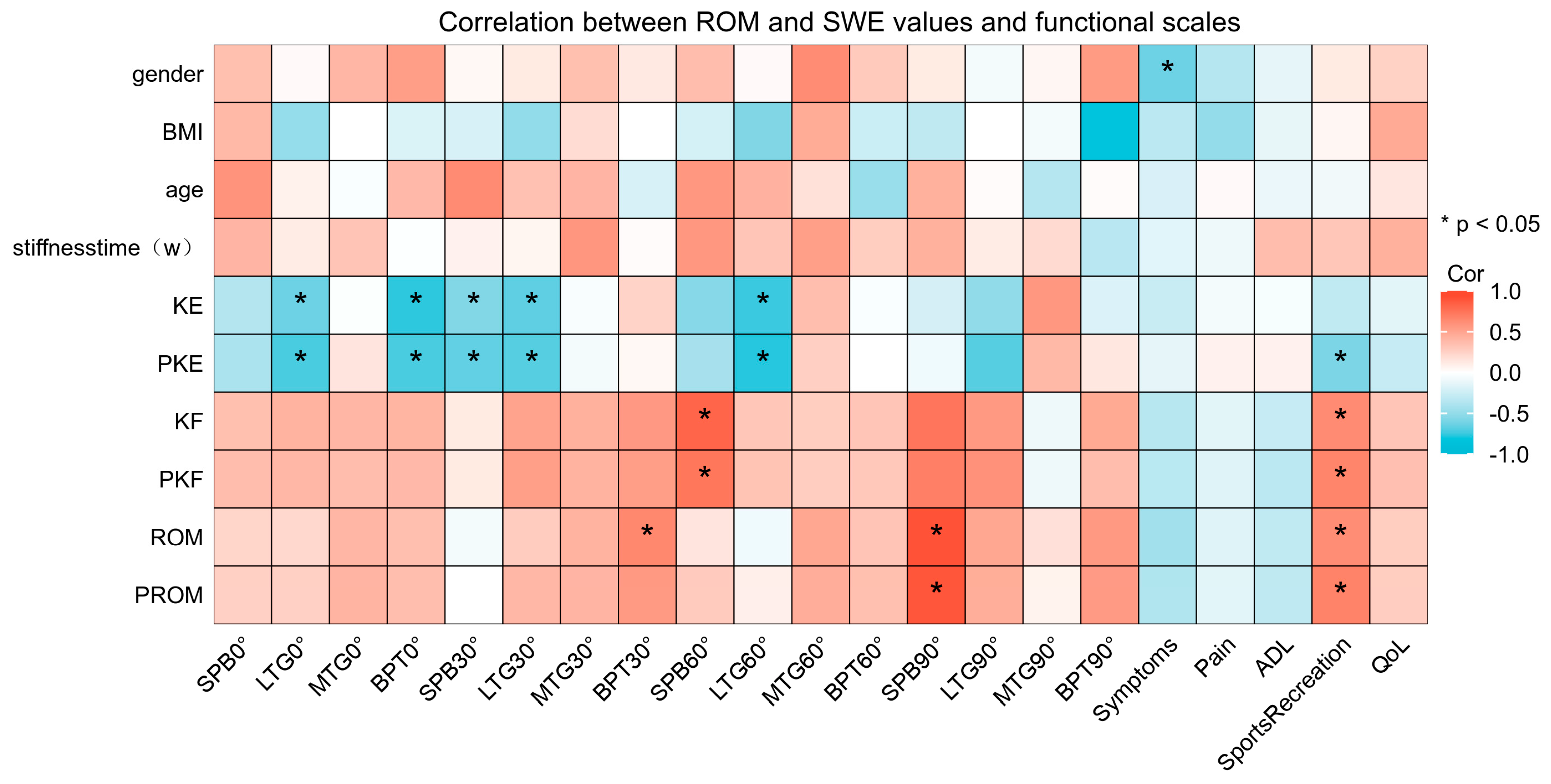
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Egol, K.; Tejwani, N.; Capla, E.; Wolinsky, P.; Koval, K. Staged management of high-energy proximal tibia fractures (OTA types 41): The results of a prospective, standardized protocol. J. Orthop. Trauma 2005, 19, 448–455. [Google Scholar] [CrossRef]
- Harner, C.; Irrgang, J.; Paul, J.; Dearwater, S.; Fu, F. Loss of motion after anterior cruciate ligament reconstruction. Am. J. Sports Med. 1992, 20, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Magit, D.; Wolff, A.; Sutton, K.; Medvecky, M. Arthrofibrosis of the knee. J. Am. Acad. Orthop. Surg. 2007, 15, 682–694. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.; Brandt, C.; Weig, T.; Koehne, M.; Bernstein, A.; Suedkamp, N.P.; Hube, R.; Stoehr, A. Long-term results of arthroscopic arthrolysis for arthrofibrosis after anterior cruciate ligament reconstruction. Arthroscopy 2017, 33, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ye, L.; Liu, H.; Wen, H. Quadriceps tendon pie-crusting release of stiff knees in total knee arthroplasty. J. Orthop. Sci. 2015, 20, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Pujol, N.; Boisrenoult, P.; Beaufils, P. Post-traumatic knee stiffness: Surgical techniques. Orthop. Traumatol. Surg. Res. 2015, 101, S179–S186. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, E.A. Quadricepsplasty. J. Bone Joint Surg. Br. 1963, 45, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Abdul, N.; Dixon, D.; Walker, A.; Horabin, J.; Smith, N.; Weir, D.J.; Brewster, N.T.; Deehan, D.J.; Mann, D.A.; Borthwick, L.A. Fibrosis is a common outcome following total knee arthroplasty. Sci. Rep. 2015, 5, 16469. [Google Scholar] [CrossRef] [PubMed]
- Mercer, P.; Chambers, R. Coagulation and coagulation signalling in fibrosis. Biochim. Biophys. Acta 2013, 1832, 1018–1027. [Google Scholar] [CrossRef]
- Newman, E.; Herschmiller, T.; Attarian, D.; Vail, T.; Bolognesi, M.; Wellman, S. Risk factors, outcomes, and timing of manipulation under anesthesia after total knee arthroplasty. J. Arthroplasty 2018, 33, 245–249. [Google Scholar] [CrossRef]
- Haffar, A.; Goh, G.S.; Fillingham, Y.A.; Torchia, M.T.; Lonner, J.H. Treatment of arthrofibrosis and stiffness after total knee arthroplasty: An updated review of the literature. Int. Orthop. 2022, 46, 1253–1279. [Google Scholar] [CrossRef]
- Flick, T.; Wang, C.; Patel, A.; Hodo, T.; Sherman, W.; Sanchez, F. Arthrofibrosis after total knee arthroplasty: Patients with keloids at risk. J. Orthop. Traumatol. 2021, 22, 1. [Google Scholar] [CrossRef]
- Attard, V.; Li, C.Y.; Self, A.; Mann, D.A.; Borthwick, L.A.; O’Connor, P.; Deehan, D.J.; Kalson, N.S. Quantification of intra-articular fibrosis in patients with stiff knee arthroplasties using metal-reduction MRI. Bone Joint J. 2020, 102-B, 1331–1340. [Google Scholar] [CrossRef]
- Ophir, J.; Céspedes, I.; Ponnekanti, H.; Yazdi, Y.; Li, X. Elastography: A quantitative method for imaging the elasticity of biological tissues. Ultrason. Imaging 1991, 13, 111–134. [Google Scholar] [CrossRef] [PubMed]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: Basic principles and technology. Ultraschall Med. 2013, 34, 169–184. [Google Scholar] [CrossRef]
- de Reuver, S.; Moens, A.; Kruyt, M.; Nievelstein, R.; Ito, K.; Castelein, R. Ultrasound shear wave elastography of the intervertebral disc and idiopathic scoliosis: A systematic review. Ultrasound Med. Biol. 2022, 48, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Tan, H.; Zhang, X.; Zhen, Y.; Gao, F.; Lu, X. Prediction of high-risk esophageal varices in patients with chronic liver disease with point and 2D shear wave elastography: A systematic review and meta-analysis. Eur. Radiol. 2022, 32, 4616–4627. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Lim, H.; Ni, M.; Yan, W.; Wong, D.; Cheung, J. Breast tumour classification using ultrasound elastography with machine learning: A systematic scoping review. Cancers 2022, 14, 367. [Google Scholar] [CrossRef]
- Hughes, L.; Rosenblatt, B.; Haddad, F.; Gissane, C.; McCarthy, D.; Clarke, T.; Ferris, G.; Dawes, J.; Paton, B.; Patterson, S.D. Comparing the effectiveness of blood flow restriction and traditional heavy load resistance training in the post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: A UK national health service randomised controlled trial. Sports Med. 2019, 49, 1787–1805. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Benner, R.W.; Gray, T. Results of anterior cruciate ligament reconstruction with patellar tendon autografts: Objective factors associated with the development of osteoarthritis at 20 to 33 years after surgery. Am. J. Sports Med. 2017, 45, 2730–2738. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.J.; Prinsen, C.A.; Christensen, R.; Bartels, E.M.; Terwee, C.B.; Roos, E.M. Knee Injury and Osteoarthritis Outcome Score (KOOS): Systematic review and meta-analysis of measurement properties. Osteoarthritis Cartilage 2016, 24, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Bieger, R.; Kappe, T.; Fraitzl, C.; Reichel, H. The aetiology of total knee arthroplasty failure influences the improvement in knee function. Arch. Orthop. Trauma Surg. 2013, 133, 237–241. [Google Scholar] [CrossRef]
- Wang, M.; Liu, C.; Xiao, W. Intra-articular injection of hyaluronic acid for the reduction in joint adhesion formation in a rabbit model of knee injury. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1536–1540. [Google Scholar] [CrossRef] [PubMed]
- Scuderi, G. The stiff total knee arthroplasty: Causality and solution. J. Arthroplasty 2005, 20, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Hang, J.; Chen, J.; Zhang, W.; Yuan, T.; Xu, Y.; Zhou, B. Correlation between elastic modulus and clinical severity of pathological scars: A cross-sectional study. Sci. Rep. 2021, 11, 23324. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Takahashi, M.; Takamoto, K.; Bito, I. Hamstring strains in professional rugby players result in increased fascial stiffness without muscle quality changes as assessed using shear wave elastography. J. Bodyw. Mov. Ther. 2021, 27, 34–41. [Google Scholar] [CrossRef] [PubMed]
- DeJong, H.; Abbott, S.; Zelesco, M.; Spilsbury, K.; Ziman, M.; Kennedy, B.F.; Martin, L.; Wood, F.M. Objective quantification of burn scar stiffness using shear-wave elastography: Initial evidence of validity. Burns 2020, 46, 1787–1798. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Ha, P.; Yen, E.; Li, C.; Zheng, Z. Small leucine-rich proteoglycans in tendon wound healing. Adv. Wound Care 2022, 11, 202–214. [Google Scholar] [CrossRef]
- Frankewycz, B.; Penz, A.; Weber, J.; da Silva, N.P.; Freimoser, F.; Bell, R.; Nerlich, M.; Jung, E.M.; Docheva, D.; Pfeifer, C.G. Achilles tendon elastic properties remain decreased in long term after rupture. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 2080–2087. [Google Scholar] [CrossRef]
- Cohen, I.K.; Peacock, E.E., Jr. Keloids and hypertophic scars. In Plastic Surgery; McCarthy, J.G., Ed.; Saunders: Philadephia, PA, USA, 1990; pp. 732–747. [Google Scholar]
- Lawrence, W. In search of the optimal treatment of keloids: Report of a series and a review of the literature. Ann. Plast. Surg. 1991, 27, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Abdel, M.P.; Morrey, M.E.; Barlow, J.D.; Kreofsky, C.R.; An, K.N.; Steinmann, S.P.; Morrey, B.F.; Sanchez-Sotelo, J. Myofibroblast cells are preferentially expressed early in a rabbit model of joint contracture. J. Orthop. Res. 2012, 30, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, K.A.; Sutherland, C.; Zhang, M. Rabbit knee model of post-traumatic joint contractures: The long-term natural history of motion loss and myofibroblasts. J. Orthop. Res. 2004, 22, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Harkos, C.; Svensson, S.; Emblem, K.; Stylianopoulos, T. Inducing biomechanical heterogeneity in brain tumor modeling by MR elastography: Effects on tumor growth, vascular density and delivery of therapeutics. Cancers 2022, 14, 884. [Google Scholar] [CrossRef] [PubMed]
- Wadugodapitiya, S.; Sakamoto, M.; Sugita, K.; Morise, Y.; Tanaka, M.; Kobayashi, K. Ultrasound elastographic assessment of the stiffness of the anteromedial knee joint capsule at varying knee angles. Biomed. Mater. Eng. 2019, 30, 219–230. [Google Scholar] [CrossRef]
- Taljanovic, M.S.; Gimber, L.H.; Becker, G.W.; Latt, L.D.; Klauser, A.S.; Melville, D.M.; Gao, L.; Witte, R.S. Shear-wave elastography: Basic physics and musculoskeletal applications. Radiographics 2017, 37, 855–870. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | |
|---|---|
| Male | 7 |
| Female | 9 |
| Age (years) | 30.3 ± 10.7 |
| Height (cm) | 169.2 ± 8.7 |
| BMI (kg/m2) | 22.4 ± 3.1 |
| Time of adhesion (weeks) | 14.8 ± 5.7 |
| ACLR | 8 |
| PCLR | 2 |
| Patellar dislocation | 2 |
| Meniscus repair | 2 |
| ACLR + MCLR | 1 |
| Patellar fracture | 1 |
| Inter-Rater Reliability | |
|---|---|
| BPT | 0.907 |
| SPB | 0.861 |
| MTG | 0.899 |
| LTG | 0.897 |
| Parameters | Unaffected Side | Affected Side | |
|---|---|---|---|
| KE | 2.92 ± 2.94 | −9.83 ± 7.94 | |
| PKE | 5.33 ± 3.60 | −5.42 ± 7.14 | |
| KF | 135.67 ± 8.02 | 70.58 ± 24.02 | |
| PKF | 142.08 ± 8.69 | 76.75 ± 26.04 | |
| ROM | 138.58 ± 7.49 | 60.75 ± 23.81 | |
| PROM | 147.42 ± 9.17 | 71.33 ± 25.74 | |
| Symptoms | 67.86 ± 15.00 | ||
| Pain | 28.24 ± 13.29 | ||
| ADL | 27.45 ± 12.23 | ||
| Sports Reactions | 17.50 ± 18.03 | ||
| QoL | 19.79 ± 13.80 | ||
| SWE values of BPT (kPa) | 0° KF | 16.04 ± 11.84 | 34.04 ± 11.52 |
| 30° KF | 17.13 ± 13.75 | 39.41 ± 18.38 | |
| 60° KF | 26.76 ± 21.96 | 68.63 ± 33.63 | |
| 90° KF | 30.46 ± 23.51 | 122.93 ± 42.50 | |
| SWE values of the SPB (kPa) | 0° KF | 21.35 ± 12.96 | 28.21 ± 11.41 |
| 30° KF | 29.00 ± 10.81 | 51.49 ± 19.96 | |
| 60° KF | 41.44 ± 29.32 | 98.74 ± 47.27 | |
| 90° KF | 47.52 ± 16.18 | 108.32 ± 45.25 | |
| SWE values of the MTG (kPa) | 0° KF | 25.98 ± 13.90 | 39.57 ± 14.80 |
| 30° KF | 25.92 ± 7.30 | 53.62 ± 18.58 | |
| 60° KF | 36.06 ± 13.88 | 72.60 ± 30.68 | |
| 90° KF | 41.05 ± 13.65 | 85.58 ± 20.40 | |
| SWE values of the LTG (kPa) | 0° KF | 34.68 ± 15.24 | 55.82 ± 20.93 |
| 30° KF | 48.25 ± 26.16 | 81.77 ± 31.97 | |
| 60° KF | 56.34 ± 25.12 | 94.92 ± 34.93 | |
| 90° KF | 64.00 ± 31.86 | 107.19 ± 35.71 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, J.; Peng, L.; Ding, A.; Chen, S.; Cai, B.; Yao, Y. Ultrasound Elastography Assessment of Knee Intra-Articular Adhesions at Varying Knee Angles. Bioengineering 2024, 11, 706. https://doi.org/10.3390/bioengineering11070706
Ye J, Peng L, Ding A, Chen S, Cai B, Yao Y. Ultrasound Elastography Assessment of Knee Intra-Articular Adhesions at Varying Knee Angles. Bioengineering. 2024; 11(7):706. https://doi.org/10.3390/bioengineering11070706
Chicago/Turabian StyleYe, Jiling, Linjing Peng, Angang Ding, Shijie Chen, Bin Cai, and Yifei Yao. 2024. "Ultrasound Elastography Assessment of Knee Intra-Articular Adhesions at Varying Knee Angles" Bioengineering 11, no. 7: 706. https://doi.org/10.3390/bioengineering11070706
APA StyleYe, J., Peng, L., Ding, A., Chen, S., Cai, B., & Yao, Y. (2024). Ultrasound Elastography Assessment of Knee Intra-Articular Adhesions at Varying Knee Angles. Bioengineering, 11(7), 706. https://doi.org/10.3390/bioengineering11070706