

Pulsing Addition to Modulated Electro-Hyperthermia


Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
- It destroys the tumor cells by absorbing energy;
- It has immunogenic effect;
- In the most frequent application, it sensitizes the conventional oncotherapies, like radiotherapy and chemotherapy.
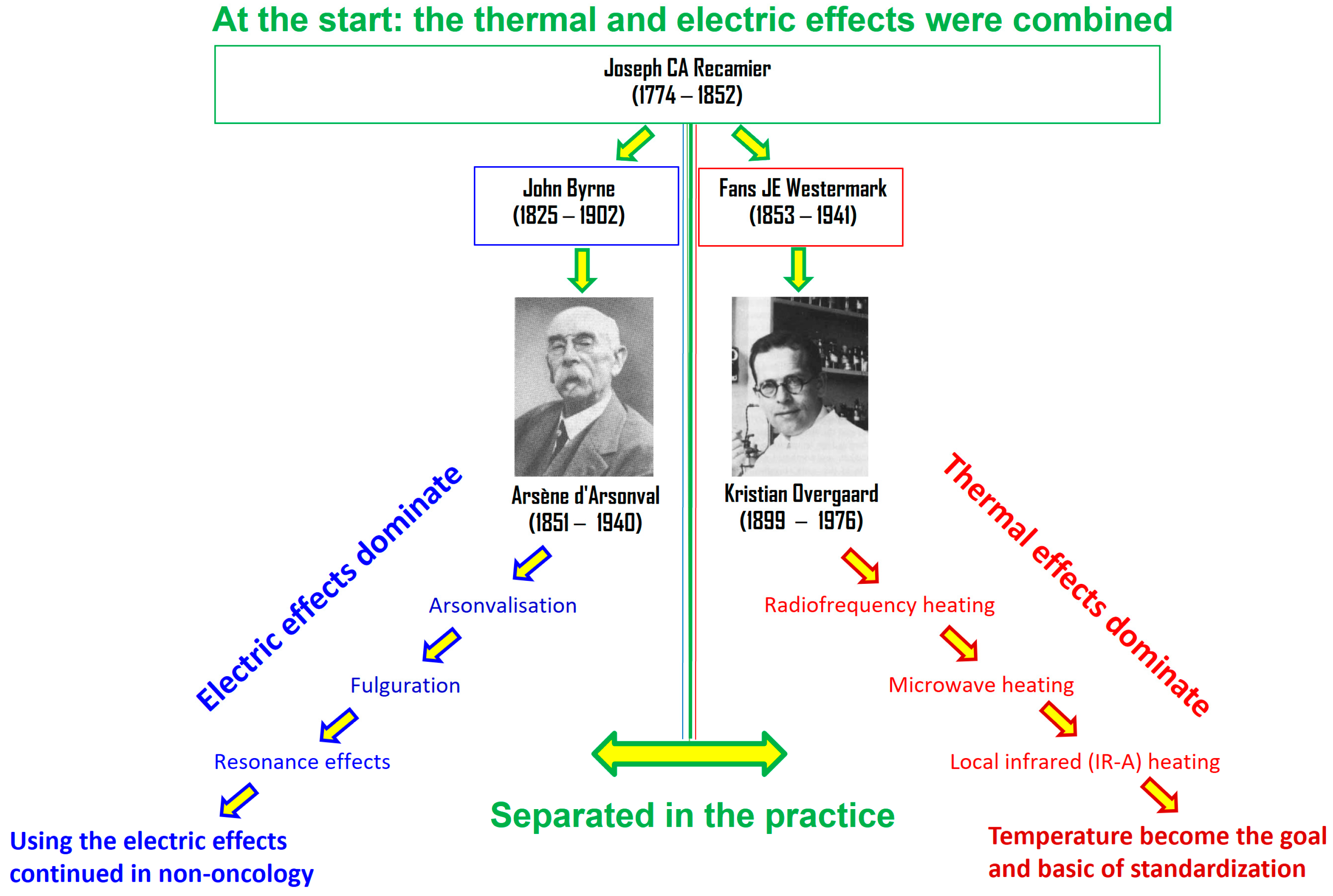
2. Electrothermal Complexity
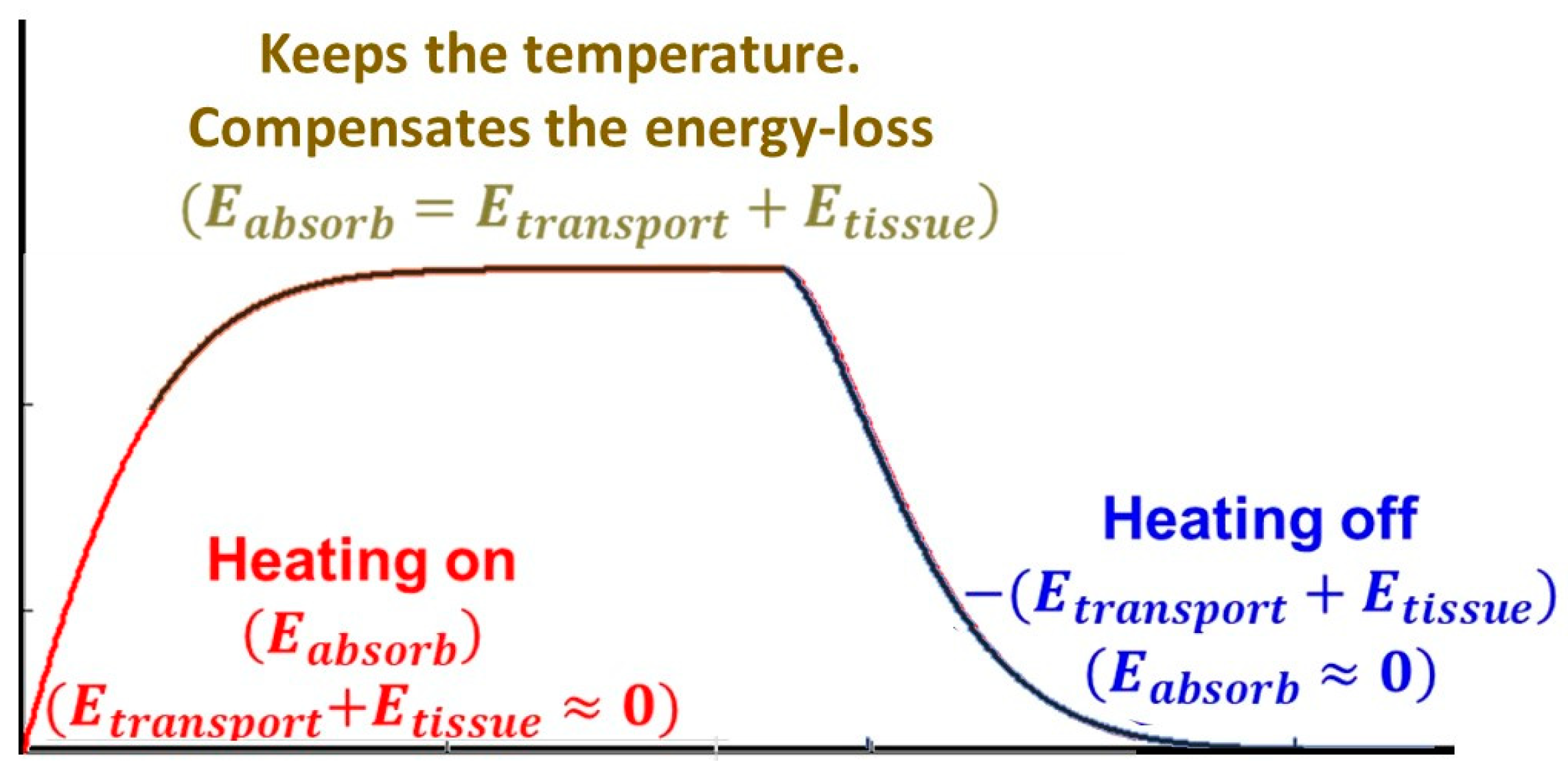
2.1. Temperature Development
2.2. Selection
2.3. Nonthermal Effects
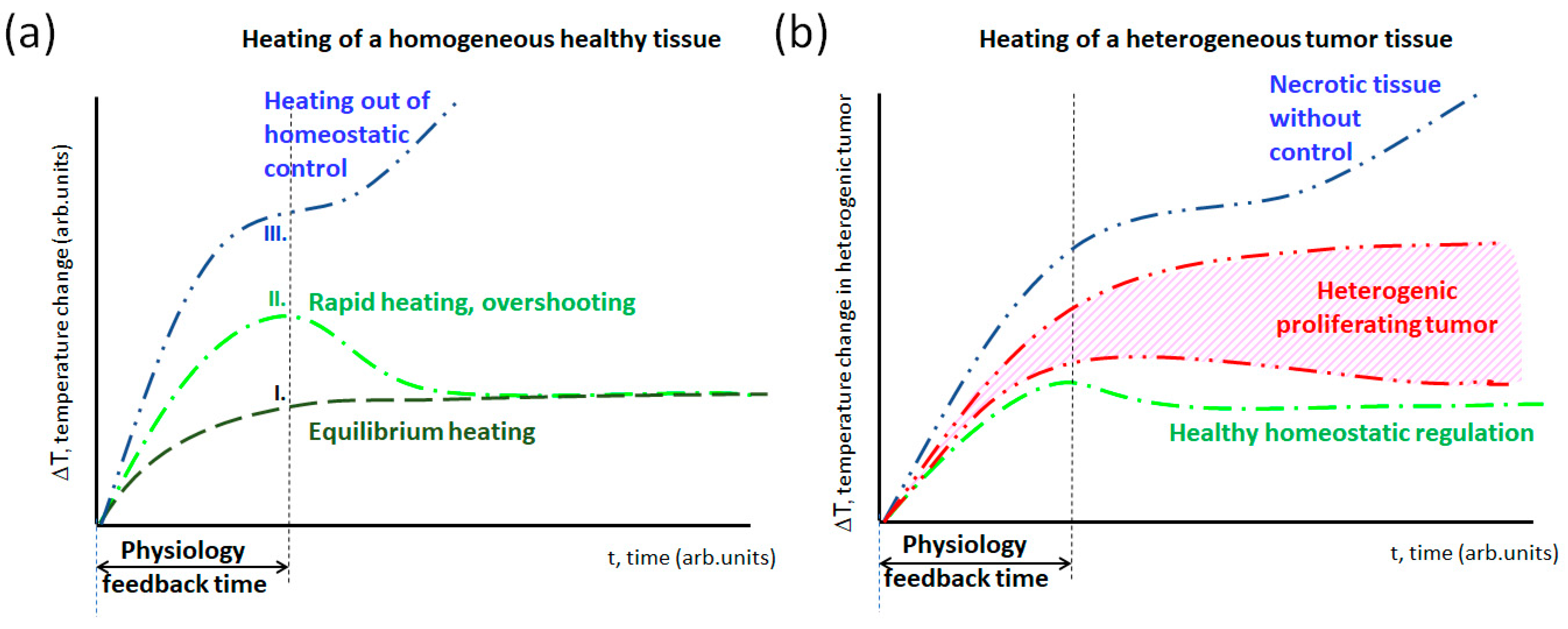
2.4. Thermal Homeostasis
3. Semi-Adiabatic Synergy (SAR)
3.1. Semi-Adiabatic Synergy (SAS) Promotes Apoptosis
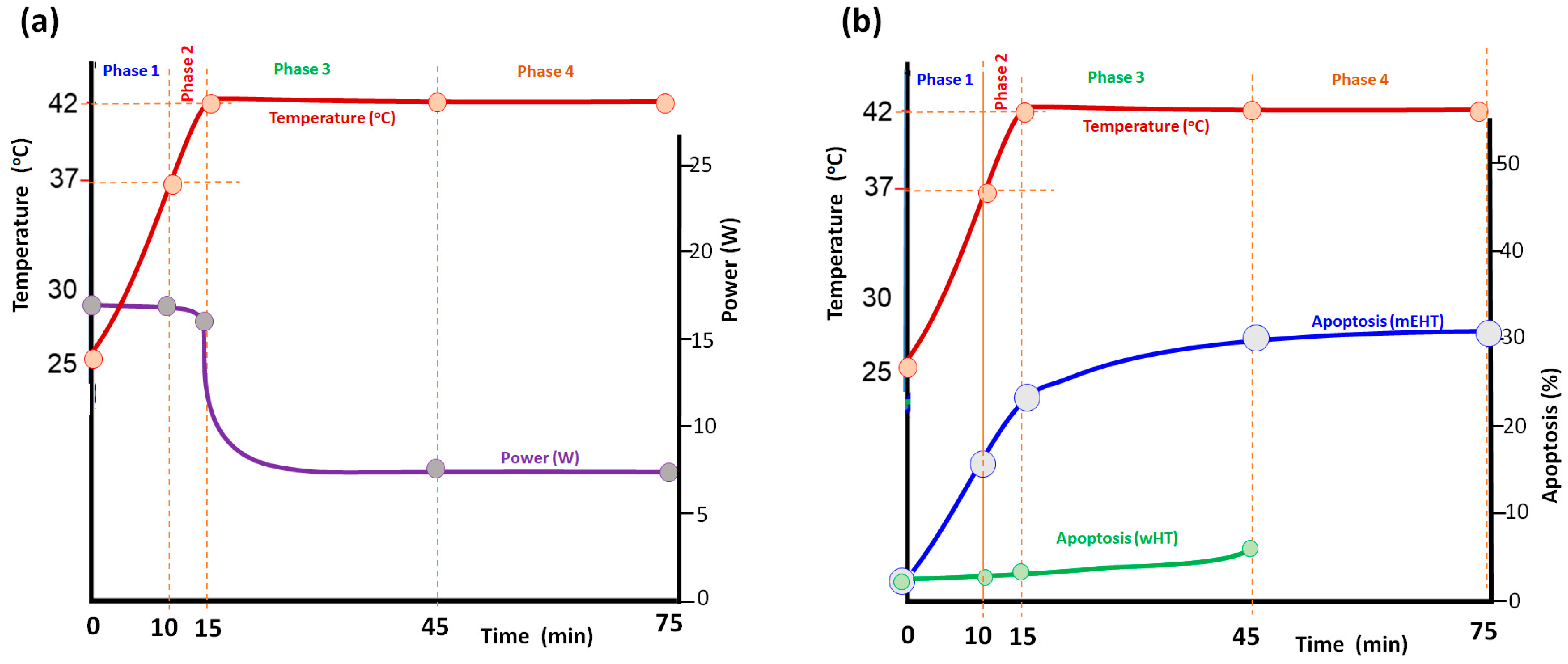
3.2. In Vitro Verification
- Phase 1. heated the cells from the room temperature to the usual starting temperature of the in vitro experiments, the human body temperature (;
- Phase 2. heated the cell culture from 37 °C to 42 °C, which is the equilibrium temperature of many standard hyperthermia treatments expecting the thermal impact;
- Phase 3. kept the equilibrium °C for ;
- Phase 4. continued the equilibrium heating at °C for the next .
3.3. In Vivo Verification
4. Pulsing Modulated Electro Hyperthermia
- Reduced risk of damage to healthy tissues: since healthy tissues cool down faster than tumors, they experience less heating during the resting phase;
- Potentially enhanced tumor damage: some tumor cells might be more susceptible to heat when exposed to pulsed heating than continuous heat;
- Improved treatment tolerability: patients may experience fewer side effects due to reduced overall heat exposure.
4.1. The Pulsing Technique
4.2. Advantages
- Enhanced Efficacy:
- The active factor of the mEHT is the RF current, which selectively flows through the target. In pulsing conditions, the extreme power gives a proportionally sizeable current density, which causes an effect. Pulsed heating can be more effective at killing cancer cells than continuous heating at the same average temperature;
- The pulsing induces the semi-adiabatic start of temperature growth, which accounts for the most significant part of apoptosis and induces immunogenic processes;
- In a low-duty cycle, increased blood flow to the tumor during the off pulses can bring in more oxygen and nutrients needed for the heat to damage the cells.
- The high-power pulse may induce reversible electroporation, increasing synergic efficacy with complementary chemo and immune therapies;
- Pulsed heating does not drastically influence homeostatic regulation as continuous heating does. So, the treatment and natural regulations are more effective in cooperative harmony;
- Studies show that pulsed electric fields effectively relieve pain, improving patients’ quality of life.
- Control and Flexibility:
- Pulsed heating allows for finer control over the temperature delivered to the target area. The pulse duration, frequency, and power can be adjusted to achieve the desired therapeutic effect while minimizing the heating of surrounding tissue;
- The power in the pulses may be kept constant; only the duty cycle changes the average power, which determines the temperature. Like digital technologies, the continuous power (and constant energy absorption in a pulse) makes the dose more controllable;
- The associated side effects are reduced due to the pulsed heating and its relatively long relaxing time with a low-duty cycle;
- The synergy of the thermal and nonthermal electric absorption is more reliable;
- Despite the large pulse power, skin and adipose burns are less likely because the subcutaneous blood flow is active, may quickly reduce the heat stress in the pausing period, the pulse is short to burn, and the low-duty cycle ensures the low average temperature on the surface, too.
- Potential Dose Reduction:
- Due to potentially higher efficacy, pulsed heating might require lower overall heat doses than continuous heating, potentially reducing treatment time;
- The specific benefits of pulsed heating may vary depending on the type of cancer, tumor size, location, and other factors.
- Technical advantages:
- The reduced cooling facility makes designing a simpler and more efficient electrode system possible;
- Forcing step-up heating is unnecessary; choosing the semi-adiabatic phase is automatic and self-adjusted;
- The tuning is more accessible because the power (the pulse intensity) is constant during all the processes;
- Having in continuous heating, the power is at a depth (the heaviest patient) and is of the incident field, which is . In the pulsed case, reaching the same temperature with 800 cap W pulses with 0.24 duty cycle (average power is also 200 cap W like it was in the continuous case), the power at will be in pulses, which is a significant increase. I propose the idea that this method treats all depths in humans equally.
4.3. Limitations
- Local tissue damage: Although pulsed heating reduces overall heating time, localized areas within the treatment zone may still experience high temperatures, potentially leading to extended tissue damage. The selection mechanisms on the tumor localize it, so the host tissues are likely safe. Still, we may lose part of the immunogenic advantages by the necrotic way of tumor cell death;
- Pain: The heating process can cause discomfort, and individual sensitivity varies. Some patients might experience more intense pain with pulsed heating than continuous heating, but the overall pain reduction after the treatment likely works for all;
- Nerve effect: Depending on the location, pulsed mEHT could lead to local numbness, tingling, or other nerve-related issues, depending on the patient’s state;
- Systemic effects: Like any hyperthermia treatment, pulsed heating can cause systemic effects like thirstiness, fever, chills, fatigue, nausea, and vomiting. The severity of these effects depends on factors like individual health, treatment parameters, underlying medical conditions, and complementary medical applications;
- Tumor-specific risks: The significantly high-power intensity in the pulses may cause rapid tumor lysis syndrome, which is toxic;
- Unforeseen complications: As with any new medical technology, unforeseen complications are always possible. More research is needed to fully understand the long-term effects and potential rare side effects of pulsed mEHT. Open communication and regular monitoring during treatment are crucial to identify and promptly manage any adverse effects;
- Technical challenge:
- The pulsing power and temperature averages could differ depending on the tumor’s thermal washout physiology, which patients may have differently.
- The average power depends on the duty-cycle, so it does not serve as a dose in the mEHT as it was in continuous power. The dose could be only the integrative absorbed energy.
- The pulsing can change the original modulation depending on its duty cycle.
5. Conclusions
Funding
Conflicts of Interest
References
- Lurito, P.W. The message was electric. IEEE Spectr. 1984, 21, 84–96. [Google Scholar] [CrossRef]
- Advertisement of German Electric Appliance Agency. In Free Lance; 1902; II, p. 18. Available online: https://paperspast.natlib.govt.nz/newspapers/NZFL19020419.2.21.1 (accessed on 24 June 2024).
- Andocs, G.; Renner, H.; Balogh, L.; Fonyad, L.; Jakab, C.; Szasz, A. Strong synergy of heat and modulated electro- magnetic field in tumor cell killing, Study of HT29 xenograft tumors in a nude mice model. Strahlenther. Onkol. 2009, 185, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Szasz, A. Thermal and nonthermal effects of radiofrequency on living state and applications as an adjuvant with radiation therapy. J. Radiat. Cancer Res. 2019, 10, 1–17. [Google Scholar] [CrossRef]
- Szasz, A.M.; Lorant, G.; Szasz, A.; Szigeti, G. The immunogenic connection of thermal and nonthermal molecular effects in modulated electro-hyperthermia. Open J. Biophys. 2023, 13, 103–142. [Google Scholar] [CrossRef]
- Szasz, A. Heterogeneous heat absorption is complementary to radiotherapy. Cancers 2022, 14, 901. [Google Scholar] [CrossRef] [PubMed]
- Szasz, A. The capacitive coupling modalities for oncological hyperthermia. Open J. Biophys. 2021, 11, 252–313. [Google Scholar] [CrossRef]
- Kakehi, M.; Ueda, K.; Mukojima, T.; Hiraoka, M.; Seto, O.; Akanuma, A.; Nakatsugawa, S. Multi-institutional Clinical Studies on hyperthermia combined with radiotherapy or chemotherapy or chemotherapy in advanced cancer of deep-seated organs. Int. J. Hyperth. 1990, 6, 719–740. [Google Scholar] [CrossRef]
- Egawa, I.; Watanabe, S.; Ohno, Y.; Morita, K.; Tominaga, S.; Onoyama, Y.; Hashimoto, S. A randomized clinical trial of hyperthermia and radiation versus radiation alone for superficially located cancers. J. Jap. Soc. Ther. Radiol. Oncol. 1989, 1, 135–140. [Google Scholar]
- Otsuka, T.; Yonezawa, M.; Kamiyama, F.; Matsushita, Y.; Matsui, N. Results of surgery and radio-hyperthemo-chemotherapy for patients with soft tissue sarcoma. Int. J. Clin. Oncol. 2001, 6, 253–258. [Google Scholar] [CrossRef]
- Doi, O.; Kodama, K.; Tatsuta, M.; Higashiyama, M.; Aoki, Y.; Kuriyama, K.; Tateishi, R. Effectiveness of intrathoracic chemothermotherapy for malignant pleurisy due to Ewing’s sarcoma: A case report. Int. J. Hyperth. 1990, 6, 947–963. [Google Scholar] [CrossRef]
- Ishikawa, T.; Kokura, S.; Sakamoto, N.; Ando, T.; Imamoto, E.; Hattori, T.; Oyamada, H.; Yoshinami, N.; Sakamoto, M.; Kitagawa, K.; et al. Phase II trial of combined regional hyperthermia and Gemcitabine for locally advanced or metastatic pancreatic cancer. Int. J. Hyperth. 2012, 28, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Masunaga, S.; Hiraoka, M.; Takahashi, M.; Jo, S.; Akuta, K.; Nishimura, Y.; Nagata, Y.; Abe, M. Clinical results of thermoradiotherapy for locally advanced and/or recurrent breast cancer-comparison of results with radiotherapy alone. Int. J. Hyperth. 1990, 6, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Nagata, Y.; Hiraoka, M.; Nishimura, Y.; Masunaga, S.; Mitumori, M.; Okuno, Y.; Fujishiro, M.; Kanamori, S.; Horii, N.; Akuta, K.; et al. Clinical results of radiofrequency hyperthermia for malignant liver tumors. Int. J. Radiat. Oncol. Biol. Phys. 1997, 38, 359–365. [Google Scholar] [CrossRef]
- Asao, T.; Sakurai, H.; Harashima, K.; Yamaguchi, S.; Tsutsumi, S.; Nonaka, T.; Shioya, M.; Nakano, T.; Kuwano, H. The synchronization of chemotherapy to circadian rhythms and irradiation in pre-operative chemoradiation therapy with hyperthermia for local advanced rectal cancer. Int. J. Hyperth. 2006, 22, 399–406. [Google Scholar] [CrossRef]
- Nishimura, Y.; Hiraoka, M.; Akuta, K.; Jo, S.; Nagata, Y.; Masunaga, S.-I.; Takahashi, M.; Abe, M. Hyperthermia combined with radiation therapy for primarily unresectable and recurrent colorectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 1992, 23, 759–768. [Google Scholar] [CrossRef] [PubMed]
- Ohguri, T.; Imada, H.; Kato, F.; Yahara, K.; Morioka, T.; Nakano, K.; Korogi, Y. Radiotherapy with 8MHz radiofrequency-capacitive regional hyperthermia for pain relief of unresectable and recurrent colorectal cancer. Int. J. Hyperth. 2006, 22, 1–14. [Google Scholar] [CrossRef]
- Mochiki, E.; Shioya, M.; Sakurai, H.; Andoh, H.; Ohno, T.; Aihara, R.; Asao, T.; Kuwano, H. Feasibility study of postoperative intraperitoneal hyperthermotherapy by radiofrequency capacitive heating system for advanced gastric cancer with peritoneal seeding. Int. J. Hyperth. 2007, 23, 493–500. [Google Scholar] [CrossRef]
- Matsui, K.; Takebayashi, S.; Watai, K.; Kakehi, M.; Kubota, Y.; Yao, M.; Shuin, T. Combination radiotherapy of urinary bladder carcinoma with chemohyperthermia. Int J. Hyperth. 1991, 7, 19–26. [Google Scholar] [CrossRef]
- Arends, T.J.H.; Nativ, O.; Maffezzini, M.; de Cobelli, O.; Canepa, G.; Verweij, F.; Moskovitz, B.; van der Heijden, A.G.; Witjes, J.A. Results of a randomized chemohyperthermia with Mitomycin C versus Bacillus Calmette-Guérin for adjuvant treatment of patients with intermediate—And high-risk non-muscle-invasive bladder cancer. Eur. Urol. 2016, 69, 1046–1052. [Google Scholar] [CrossRef]
- Sugimach, K.; Kuwano, H.; Ide, H.; Toge, T.; Saku, M.; Oshiumi, Y. Chemotherapy combined with or without hyperthermia for patients with oesophagael carcinoma: A prospective randomized trial. Int. J. Hyperth. 1994, 10, 485–493. [Google Scholar] [CrossRef]
- Ohguri, T.; Imada, H.; Yahara, K.; Morioka, T.; Nakano, K.; Terashima, H.; Korogi, Y. Radiotherapy with 8-MHz radiofrequency-capacitive regional hyperthermia for stage III non-small cell lung cancer: The radiofrequency-output power correlates with the intraesophageal temperature and clinical outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2009, 1, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Ohguri, T.; Imada, H.; Yahara, K.; Morioka, T.; Nakano, K.; Terashima, H.; Korogi, Y. Deep regional hyperthermia for the whole thoracic region using 8MHz radiofrequency-capacitive heating device: Relationship between the radiofrequency-output power and the intra-oesophageal temperature and predictive factors for a good heating in 59 patients. Int. J. Hyperth. 2011, 27, 20–26. [Google Scholar]
- Huilgol, N.G.; Gupta, S.; Sridhar, C.R. Hyperthermia with radiation in the treatment of locally advanced head and neck cancer: A report of randomized trial. J. Cancer Res. Ther. 2010, 6, 492–496. [Google Scholar] [CrossRef]
- Datta, N.R.; Bose, A.K.; Kapoor, H.K.; Gupta, S. Head and neck cancers: Results of thermoradiotherapy versus radiotherapy. Int. J. Hyperth. 1990, 6, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Ohguri, T.; Imada, H.; Narisada, H.; Yahara, K.; Morioka, T.; Nakano, K.; Miyaguni, Y.; Korogi, Y. Systemic chemotherapy using paclitaxel and carboplatin plus regional hyperthermia and hyperbaric oxygen treatment for non-small cell lung cancer with multiple pulmonary metastases: Preliminary results. Int. J. Hyperth. 2009, 25, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Kodama, K.; Doi, O.; Tatsuta, M.; Kuriyama, K.; Tateishi, R. Development of postoperative intrathoracic chemo-thermotherapy for lung cancer with objective of improving local cure. Cancer 1989, 64, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Mitsumori, M.; Zeng, Z.-F.; Oliynychenko, P.; Park, J.H.; Choi, B.I.; Tatsuzaki, H.; Tanaka, Y.; Hitaoka, M. Regional hyperthermia combined with radiotherapy for locally advanced non-small cell lung cancers: A multi-institutional prospective randomized trial of the International Atomic Energy Agency. Int. J. Clin. Oncol. 2007, 12, 192–198. [Google Scholar] [PubMed]
- Kitamura, K.; Kuwano, H.; Watanabe, M.; Nozoe, T.; Yasuda, M.; Sumiyoshi, K.; Saku, M.; Sugimachi, K. Prospective randomized study of hyperthermia combined with chemoradiotherapy for esophageal carcinoma. J. Surg Oncol. 1995, 60, 55–58. [Google Scholar] [CrossRef]
- Szasz, O.; Szigeti, G.; Szasz, A. Connections between the specific absorption rate and the local temperature. Open J. Biophys. 2016, 6, 53–74. [Google Scholar] [CrossRef]
- Papp, E.; Vancsik, T.; Kiss, E.; Szasz, O. Energy absorption by the membrane rafts in the modulated electro-hyperthermia (mEHT). Open J. Biophys. 2017, 7, 216–229. [Google Scholar] [CrossRef]
- Govorov, A.O.; Richardson, H.H. Generating heat with metal nanoparticles. NanoToday 2007, 2, 30–38. [Google Scholar] [CrossRef]
- Szasz, O.; Andocs, G.; Meggyeshazi, N. Modulation effect in oncothermia. Hindawi Publishing Corporation. Conf. Pap. Med. 2013, 2013, 395678. [Google Scholar]
- Szasz, O. Bioelectromagnetic paradigm of cancer treatment—Modulated electro-hyperthermia (mEHT). Open J. Biophys. 2019, 9, 98–109. [Google Scholar] [CrossRef]
- Szasz, A. Bioelectromagnetic Paradigm of Cancer Treatment Oncothermia. In Bioelectromagnetic and Subtle Energy Medicine; Paul, J.R., Ed.; CRC Press: Boca Raton, FL, USA; Taylor & Francis Group: Oxford, UK, 2015; pp. 323–336. [Google Scholar]
- Semenza, G.L. Tumor metabolism: Cancer cells give and take lactate. J. Clin. Investig. 2008, 118, 3835–3837. [Google Scholar] [CrossRef] [PubMed]
- Stoy, R.D.; Foster, K.R.; Schwan, H.P. Dielectric properties of mammalian tissues form 0.1 to 100 MHz: A summary of recent data. Phys. Med. Biol. 1982, 27, 501–513. [Google Scholar] [CrossRef]
- Foster, K.R.; Schepps, J.L. Dielectric properties of tumor and normal tissues at radio through microwave frequencies. J. Microw. Power 1981, 16, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Gershing, E. Monitoring temperature-induced changes in tussue during hyperthermia by impedance methods. In Electrical Bioimpedance Methods; Riu, P.J., Ed.; New York Academy of Sciences: New York, NY, USA, 1999; Volume 873, pp. 13–20. [Google Scholar]
- Oehr, P.; Biersack, H.J.; Coleman, R.E. PET and PET-CT in Oncology; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar]
- Larson, S.M. Positron Emission Tomography-Based Molecular Imaging in Human Cancer: Exploring the Link between Hypoxia and Accelerated Glucose Metabolism. Clin. Cancer Res. 2004, 10, 2203–2204. [Google Scholar] [CrossRef]
- Sha, L.; Ward, E.R.; Story, B. A review of dielectric properties of normal and malignant breast tissue. In Proceedings of the IEEE SoutheastCon 2002 (Cat. No.02CH37283), Columbia, SC, USA, 5–7 April 2002; pp. 457–462. [Google Scholar]
- Blad, B.; Wendel, P.; Jonsson, M.; Lindstrom, K. An electrical impedance index to distinguish between normal and cancerous tissues. J. Med. Eng. Technol. 1999, 23, 57–62. [Google Scholar] [CrossRef]
- Szentgyorgyi, A. Electronic Biology and Cancer; Marcel Dekker: New York, NY, USA, 1998. [Google Scholar]
- Szentgyorgyi, A. The Living State and Cancer; Marcel Dekker: New York, NY, USA, 1978. [Google Scholar]
- Szigeti, G.P.; Szasz, O.; Hegyi, G. Connections between Warburg’s and Szentgyorgyi’s Approach about the Causes of Cancer. J. Neoplasm 2017, 1, 1–13. [Google Scholar]
- Joy, M.L.G. MR current density and conductivity imaging: The state of the Art, Engineering in Medicine and Biology. In Proceedings of the IEMBS 26th Annual International Conference of the IEEE, San Francisco, CA, USA, 1–5 September 2004; Volume 2, pp. 5315–5319. [Google Scholar]
- Muftuler, L.T.; Hamamura, M.J.; Birgul, O.; Nalcioglu, O. In vivo MRI electrical impedance tomography (MREIT) of tumors. Technol. Cancer Res. Treat. 2006, 5, 381–387. [Google Scholar]
- Kao, P.H.-J.; Chen, C.-H.; Tsang, Y.-W.; Lin, C.-S.; Chiang, H.-C.; Huang, C.-C.; Chi, M.-S.; Yang, K.-L.; Li, W.-T.; Kao, S.-J.; et al. Relationship between energy dosage and apoptotic cell death by modulated electro-hyperthermia. Sci. Rep. 2020, 10, 8936. [Google Scholar] [CrossRef] [PubMed]
- Szasz, O.; Szasz, A. Approaching complexity: Hyperthermia dose and its possible measurement in oncology. Open J. Biophys. 2021, 11, 68–132. [Google Scholar] [CrossRef]
- Lee, I.-H.; Imanaka, M.Y.; Modahl, E.H.; Torres-Ocampo, A.P. Lipid raft phase modulation by membrane-anchored proteins with inherent phase separation properties. ACS Omega 2019, 4, 6551–6559. [Google Scholar] [CrossRef]
- Staunton, J.R.; Agus, D.B.; Alexander, J.F.; Arap, W.; Ashili, S.; Aslan, J.E.; Bonneau, R. The Physical Sciences—Oncology Centers Network; A physical sciences network characterization of non-tumorigenic and metastatic cells. Sci. Rep. 2008, 3, 1449. [Google Scholar]
- Kotnik, T. Theoretical Evaluation of the Distributed Power Dissipation in Biological Cells Exposed to Electric Fields. Bioelectromagnetics 2000, 21, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Campello, E.M.B.; Zohdi, T.I. Design Evaluation of a Particle Bombardment System Used to Deliver Substances into Cells. CMES 2014, 98, 221–245. [Google Scholar]
- Lee, B.W.; Faller, R.; Sum, A.K.; Vattulainen, I.; Patra, M.; Karttunen, M. Structural Effects of Small Molecules on Phospholipid Bilayers Investigated by Molecular Simulations. Fluid Phase Equilibria 2004, 225, 63–68. [Google Scholar] [CrossRef]
- Guest, W.C.; Cashman, N.R.; Plotkin, S.S. A theory for the anisotropic and inhomogeneous dielectric properties of proteins. Phys. Chem. Chem. Phys. 2011, 13, 6286–6295. [Google Scholar] [CrossRef] [PubMed]
- Heikelä, M.; Vattulainen, I.; Hyvönen, M.T. Atomistic simulation studies of cholesteryl oleates: Model for the core of lipoprotein particles. J. Biophys. 2006, 90, 2247–2257. [Google Scholar] [CrossRef]
- Waxham, M.N. Molecular mobility in cells examined with optical methods. In Protein Trafficking in Neurons; Bean, A.J., Ed.; Academic Press: Houston, TX, USA, 2007; pp. 3–27. [Google Scholar]
- Cloutier, M.; Wang, E. Dynamic modeling and analysis of cancer cellular network motifs. Integr. Biol. 2011, 3, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Nunez, L.; Chen, A.; Budelli, G.; Berck, M.E.; Richter, V.; Rist, A.; Thum, A.S.; Cardona, A.; Klein, M.; Garrity, P.; et al. Synchronous and opponent thermosensors use flexible cross-inhibition to orchestrate thermal homeostasis. Sci. Adv. 2021, 7, eabg6707. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mathur-DeVre, R. Biomedical implications of the relaxation behaviour of water related to NMR imaging. Br. J. Radiol. 1984, 57, 955–976. [Google Scholar] [CrossRef]
- Benson, H. The relaxation response: Its subjective and objective historical precedents and physiology. Trends Neurosci. 1983, 6, 281–284. [Google Scholar] [CrossRef]
- Li, X.; Sun, S.; Yao, J.; Sun, Z. Using Relaxation Time to characterize biological effects of different mutagens. Sci. Rep. 2020, 10, 13941. [Google Scholar] [CrossRef] [PubMed]
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Phys. 1948, 1, 93–122. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.-S.; Liu, J. Analytical solutions to 3-D bioheat transfer problems with or without phase change. In Heat Transfer Phenomena and Applications; Intech: London, UK, 2012; Chapter 8; pp. 205–242. [Google Scholar]
- Deng, Z.-S.; Liu, J. Analytical study on bioheat transfer problems with spatial or transient heating on skin surface or inside biological bodies. Trans. ASME 2002, 124, 638–649. [Google Scholar]
- Cundin, L.X.; Roach, W.P.; Millenbaugh, N. Empirical comparison of Pennes’ Bio-Heat equation. Proc. SPIE 2009, 7175, 238–246. [Google Scholar]
- Lakhssassi, A.; Kengne, E.; Semmaoui, H. Modified Pennes’ equation modelling bio-heat transfer in living tissues: Analytical and numerical analysis. Nat. Sci. 2010, 2, 1375–1385. [Google Scholar]
- Gao, B.; Langer, S.; Corry, P.M. Application of the time-dependent Green’s function and Fourier transforms to the solution of the bioheat equation. Int. J. Hyp. 1995, 11, 267–285. [Google Scholar] [CrossRef]
- Erdman, B.; Lang, J.; Seebaas, M. Optimalisation of Temperature Distributions for Regional Hyperthermia Based on a Nonlinear Heat Transfer Model. Ann. N. Y. Acad. Sci. 1998, 858, 36–46. [Google Scholar] [CrossRef]
- Hasegawa, T.; Gu, Y.-H.; Takahashi, T.; Hasegawa, T.; Yamamoto, I. Enhancement of hyperthermic effects using rapid heating. In Thermotherapy for Neoplasia, Inflammation, and Pain; Kosaka, M., Sugahara, T., Schmidt, K.L., Simon, E., Eds.; Springer: Tokyo, Japan; Berlin/Heidelberg, Germany, 2001; pp. 439–444. [Google Scholar]
- IEEE C95.1; IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3 kHz to 300 GHz. IEEE: Piscataway, NJ, USA, 2005.
- Song, C.W.; Park, H.; Griffin, R.J. Theoretical and Experimental Basis of Hyperthermia, Thermotherapy for Neoplasia, Inflammation, and Pain; Kosaka, M., Sugahara, T., Schmidt, K.L., Simon, E., Eds.; Springer: Tokyo, Japan, 2001; pp. 394–407. [Google Scholar]
- Bassingthwaighte, J.B. Physiology and theory of tracer washout techniques for the estimation of myocardial blood flow: Flow estimation from tracer washout. Prog. Cardiovasc. Dis. 1977, 20, 165–189. [Google Scholar] [CrossRef] [PubMed]
- Bassingthwaighte, J.B.; Yipintosoi, T. Organ blood flow, wash-in, washout, and clearance of nutrients and metabolites. Mayo Clin. Proc. 1974, 49, 248–255. [Google Scholar] [PubMed]
- Feldmann, H.J.; Molls, M.; Hoederath, A.; Krümpelmann, S.; Sack, H. Blood flow and steady state temperatures in deep-seated tumors and normal tissues. Int. J. Radiat. Oncol. Biol. Phys. 1992, 23, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Fatehi, D.; van der Zee, J.; Notenboom, A.; van Rhoon, G.C. Comparison of intratumor and intraluminal temperatures during loco-regional deep hyperthermia of pelvic tumors. Strahlenther. Und Onkol. 2007, 183, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Szasz, A. Immunogenic Effect of Modulated Electro-hyperthermia (mEHT) in Solid Tumors. In Interdisciplinary Cancer Research; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Tsang, Y.-W.; Huang, C.-C.; Yang, K.-L.; Chi, M.-S.; Chiang, H.-C.; Wang, Y.-S.; Andocs, G.; Szasz, A.; Li, W.-T.; Chi, K.-H. Improving immunological tumor microenvironment using electro-hyperthermia followed by dendritic cell immunotherapy. BMC Cancer 2015, 15, 708. [Google Scholar] [CrossRef]
- Qin, W.; Akutsu, Y.; Andocs, G.; Suganami, A.; Hu, X.; Yusup, G.; Komatsu-Akimoto, A.; Hoshino, I.; Hanari, N.; Mori, M.; et al. Modulated electro-hyperthermia enhances dendritic cell therapy through an abscopal effect in mice. Oncol. Rep. 2014, 32, 2373–2379. [Google Scholar] [CrossRef] [PubMed]
- Vancsik, T.; Kovago, C.; Kiss, E.; Papp, E.; Forika, G.; Benyo, Z.; Meggyeshazi, N.; Krenacs, T. Modulated electro-hyperthermia induced loco-regional and systemic tumor destruction in colorectal cancer allografts. J. Cancer 2018, 9, 41–53. [Google Scholar] [CrossRef]
- Minnaar, C.A.; Kotzen, J.A.; Ayeni, O.A.; Vangu, M.-D.-T.; Baeyens, A. Potentiation of the abscopal effect by modulated electro-hyperthermia in locally advanced cervical cancer patients. Front. Oncol. 2020, 10, 376. [Google Scholar] [CrossRef]
- Chi, M.-S.; Mehta, M.P.; Yang, K.-L.; Lai, H.-C.; Lin, Y.-C.; Ko, H.-L.; Wang, Y.-S.; Liao, K.-W.; Chi, K.-H. Putative abscopal effect in three patients treated by combined radiotherapy and modulated electrohyperthermia. Front. Oncol. 2020, 10, 254. [Google Scholar] [CrossRef]
- Wust, P.; Stein, U.; Ghadjar, P. Non-thermal membrane effects of electromagnetic fields and therapeutic applications in oncology. Int. J. Hyperth. 2021, 38, 715–731. [Google Scholar] [CrossRef]
- Wust, P.; Kortüm, B.; Strauss, U.; Nadobny, J.; Zschaeck, S.; Beck, M.; Stein, U.; Ghadjar, P. Non-thermal effects of radiofrequency electromagnetic fields. Sci. Rep. 2020, 10, 13488. [Google Scholar] [CrossRef]
- Yang, K.-L.; Huang, C.-C.; Chi, M.-S.; Chiang, H.-C.; Wang, Y.-S.; Hsia, C.-C.; Andocs, G.; Wang, H.-E.; Chi, K.-H. In vitro comparison of conventional hyperthermia and modulated electro-hyperthermia. Oncotarget 2016, 7, 84082–84092. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.; Jeon, T.-W.; Lee, C.G.; Oh, S.T.; Yang, H.-B.; Choi, K.-J.; Seo, D.; Yun, I.; Baik, I.H.; Park, K.R.; et al. Electro-hyperthermia inhibits glioma tumorigenicity through the induction of E2F1-mediated apoptosis. Int. J. Hyperth. 2015, 31, 784–792. [Google Scholar] [CrossRef]
- Andocs, G.; Rehman, M.U.; Zhao, Q.-L.; Tabuchi, Y.; Kanamori, M.; Kondo, T. Comparison of biological effects of modulated electro-hyperthermia and conventional heat treatment in human lymphoma U937 cell. Cell Death Discov. 2016, 2, 16039. [Google Scholar] [CrossRef] [PubMed]
- Vancsik, T.; Forika, G.; Balogh, A.; Kiss, E.; Krenacs, T. Modulated electro-hyperthermia induced p53 driven apoptosis and cell cycle arrest additively support doxorubicin chemotherapy of colorectal cancer in vitro. Cancer Med. 2019, 8, 4292–4303. [Google Scholar] [CrossRef]
- Forika, G.; Balogh, A.; Vancsik, T.; Zalatnai, A.; Petovari, G.; Benyo, Z.; Krenacs, T. Modulated electro-hyperthermia resolves radioresistance of Panc1 pancreas adenocarcinoma and promotes DNA damage and apoptosis in vitro. Int. J. Mol. Sci. 2020, 21, 5100. [Google Scholar] [CrossRef] [PubMed]
- Wust, P.; Veltsista, P.D.; Oberacker, E.; Yavvari, P.; Walther, W.; Bengtsson, O.; Sterner-Kock, A.; Weinhart, M.; Heyd, F.; Grabowski, P.; et al. Radiofrequency electromagnetic fields cause non-temperature-induced physical and biological effects in cancer cells. Cancers 2022, 14, 5349. [Google Scholar] [CrossRef]
- Portoro, I.; Danics, L.; Veres, D. Increased efficacy in treatment of glioma by a new modulated electro-hyperthermia (mEHT) protocol. Oncothermia J. 2018, 24, 344–356. [Google Scholar]
- Aas, A.T.; Brun, A.; Blennow, C.; Stromblad, S.; Salford, L.G. The RG2 rat glioma model. J. Neurooncol. 1995, 23, 175–183. [Google Scholar] [CrossRef]
- Danics, L.; Schvarcz, C.A.; Viana, P.; Vancsik, T.; Krenács, T.; Benyó, Z.; Kaucsár, T.; Hamar, P. Exhaustion of protective heat shock response induces significant tumor damage by apoptosis after modulated electro-hyperthermia treatment of triple negative breast cancer isografts in mice. Cancers 2020, 12, 2581. [Google Scholar] [CrossRef]
- Minnaar, C.A.; Szasz, A. Forcing the antitumor effects of HSPs using a modulated electric field. Cells 2022, 11, 1838. [Google Scholar] [CrossRef] [PubMed]
- Szasz, O. Local Treatment with Systemic Effect: Abscopal Outcome. In Challenges and Solutions of Oncological Hyperthermia; Szasz, A., Ed.; Cambridge Scholars: Cambridge, UK, 2020; Chapter 11; pp. 192–205. [Google Scholar]
- Reinhold, H.S.; van den Berg-Blok, A. The influence of a heat pulse on the thermally induced damage to tumour microcirculation. Eur. J. Cancer Clin. Oncol. 1983, 19, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Tisa, T.A.; Nisha, Z.A.; Kiber, M.A. Design of an Enhanced Temperature Control System for Neonatal Incubator. Bangladesh J. Med. Phys. 2013, 5, 53–61. [Google Scholar] [CrossRef]
- Lu, C.H.; Chen, W.T.; Hsieh, C.H.; Kuo, Y.Y.; Chao, C.Y. Thermal cycling-hyperthermia in combination with polyphenols, epigallocatechin gallate and chlorogenic acid, exerts synergistic anticancer effect against human pancreatic cancer PANC-1 cells. PLoS ONE 2019, 14, e0217676. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Hernandez, D.; Lee, S.Y. Time-multiplexed two-channel capacitive radiofrequency hyperthermia with nanoparticle mediation. Biomed. Eng. Online 2015, 14, 95. [Google Scholar] [CrossRef] [PubMed]
- Yaghmazadeh, O. Pulsed high-power radio frequency energy can cause non-thermal harmful effects on the brain. arXiv 2023, arXiv:2309.03479v1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, C.-Y.; Lin, S.-M.; Wan, Y.-Y. Prediction of Temperature Field and Thermal Damage of Multilayer Skin Tissues Subjected to Time-Varying Laser Heating and Fluid Cooling by a Semianalytical Method. Math. Probl. Eng. 2020, 2020, 5074280. [Google Scholar] [CrossRef]
- Chung, M.-K.; Güler, A.D.; Caterina, M.J. Biphasic currents evoked by chemical or thermal activation of the heat-gated ion channel. J. Biol. Chem. 2005, 280, 15928–15941. [Google Scholar] [CrossRef] [PubMed]
- Ding, G.R.; Li, K.C.; Wang, X.W.; Zhou, Y.C.; Qiu, L.B.; Tan, J.; Xu, S.L.; Guo, G.Z. Effect of electromagnetic pulse exposure on brain micro vascular permeability in rats. Biomed. Environ. Sci. 2009, 22, 265–268. [Google Scholar] [CrossRef]
- Wang, Q. The study of dose-response relationship of pulsed electromagnetic radiation on rat blood-brain-barrier. Chin. J. Dis. Control Prev. 2003, 7, 401–404. [Google Scholar]
- Li, K.; Zhang, K.; Xu, S.; Wang, X.; Zhou, Y.; Zhou, Y.; Gao, P.; Lin, J.; Ding, G.; Guo, G. EMP-induced BBB-disruption enhances drug delivery to glioma and increases treatment efficacy in rats. Bioelectromagnetics 2018, 39, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Song, Z.; Yuan, Y.; Guo, G.; Kang, J. Effects of pulse parameters on the temperature distribution of a human head exposed to the electromagnetic pulse. Sci Rep. 2021, 11, 22938. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sorrell, R.G.; Muhlenfeld, J.; Moffett, J.; Stevens, G.; Kesten, S. Evaluation of pulsed electromagnetic field therapy for the treatment of chronic postoperative pain following lumbar surgery: A pilot, double-blind, randomized, sham-controlled clinical trial. J. Pain Res. 2018, 11, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
- Lisi, A.J.; Scheinowitz, M.; Saporito, R.; Onorato, A.A. Pulsed Electromagnetic Field Therapy Device for Non-Specific Low Back Pain: A Pilot Randomized Controlled Trial. Pain Ther. 2019, 8, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Sersa, G.; Heller, R. Editorial: Pulsed electric field based technologies for oncology applications. Front. Oncol. 2023, 13, 1183900. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nuccitelli, R. Application of Pulsed Electric Fields to Cancer Therapy. Bioelectricity 2019, 1, 30–34. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cao, T.L.; Le, T.A.; Hadadian, Y.; Yoon, J. Theoretical Analysis for Using Pulsed Heating Power in Magnetic Hyperthermia Therapy of Breast Cancer. Int. J. Mol. Sci. 2021, 22, 8895. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mir, L.M.; Belehradek, M.; Domenge, C.; Orlowski, S.; Poddevin, B.; Belehradek, J., Jr.; Schwaab, G.; Luboinski, B.; Paoletti, C. Electrochemotherapy, a new antitumor treatment: First clinical trial. Comptes Rendus L’academie Des Sci. Ser. III 1991, 313, 613–618. [Google Scholar]
- Galvano- or Electrochemical Tumor Therapy (ECT). Available online: https://www.klinik-st-georg.de/en/klinik-st-georg/st-george-hospital/therapies/galvano-or-electrochemical-tumor-therapy-ect/ (accessed on 15 February 2024).
- Campana, L.G.; Daud, A.; Lancellotti, F.; Arroyo, J.P.; Davalos, R.V.; Di Prata, C.; Gehl, J. Pulsed Electric Fields in Oncology: A Snapshot of Current Clinical Practices and Research Directions from the 4th World Congress of Electroporation. Cancers 2023, 15, 3340. [Google Scholar] [CrossRef]
- Preta, G. New Insights Into Targeting Membrane Lipids for Cancer Therapy. Front. Cell Dev. Biol. 2020, 8, 571237. [Google Scholar] [CrossRef]
- Robinson, V.S.; Garner, A.L.; Loveless, A.M.; Neculaes, V.B. Calculated plasma membrane voltage induced by applying electric pulses using capacitive coupling. Biomed. Phys. Eng. Express 2017, 3, 025016. [Google Scholar] [CrossRef]



















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szasz, A. Pulsing Addition to Modulated Electro-Hyperthermia. Bioengineering 2024, 11, 725. https://doi.org/10.3390/bioengineering11070725
Szasz A. Pulsing Addition to Modulated Electro-Hyperthermia. Bioengineering. 2024; 11(7):725. https://doi.org/10.3390/bioengineering11070725
Chicago/Turabian StyleSzasz, Andras. 2024. "Pulsing Addition to Modulated Electro-Hyperthermia" Bioengineering 11, no. 7: 725. https://doi.org/10.3390/bioengineering11070725
APA StyleSzasz, A. (2024). Pulsing Addition to Modulated Electro-Hyperthermia. Bioengineering, 11(7), 725. https://doi.org/10.3390/bioengineering11070725