
Interactive Cascaded Network for Prostate Cancer Segmentation from Multimodality MRI with Automated Quality Assessment

Abstract
:
1. Introduction
2. Related Works
2.1. Deep Learning for Prostate Cancer Segmentation
2.2. Automated Quality Assessment of Segmentation Results
3. Method
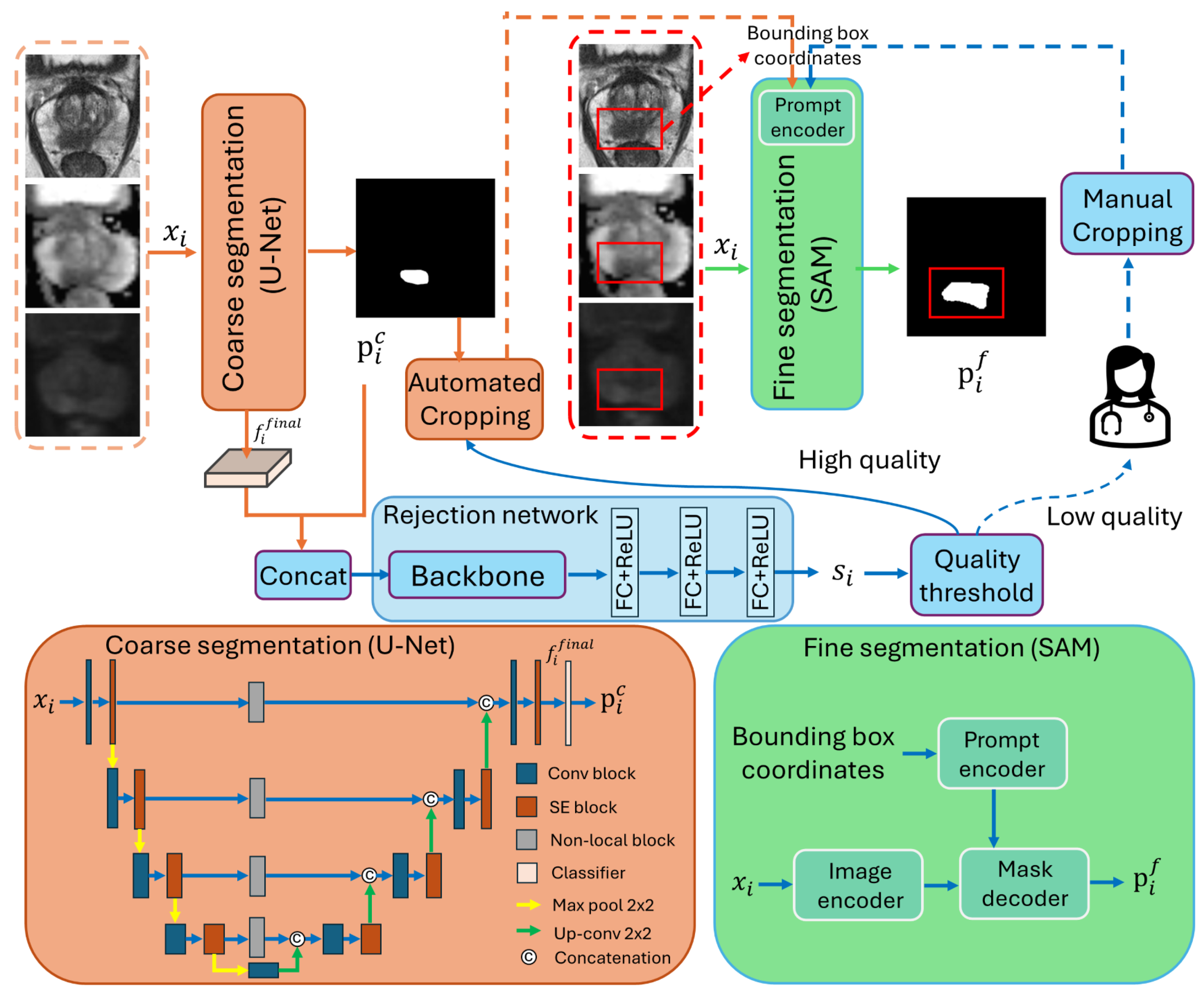
3.1. Overall Workflow
3.2. Network Structure
3.2.1. Coarse Segmentation Network
3.2.2. Rejection Network
3.2.3. Fine Segmentation Network
3.3. Model Training
4. Experimental Setup
4.1. Data
4.2. Evaluation Metrics
4.3. Implementation Details
5. Experimental Results
5.1. Comparison with State-of-the-Art Methods
5.1.1. Comparison with Automated Segmentation Methods
5.1.2. Comparison with Fully Interactive Segmentation Methods
5.1.3. Lesion-Level Analysis
5.2. Analysis of Rejection Ratio
5.3. Influence of Different Bounding Box Extension Ratio
5.4. Training and Inference Time
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Olajide, A.O.; Eziyi, A.K.; Kolawole, O.A.; Sabageh, D.O.; Ajayi, I.A.; Olajide, F.O. A comparative study of the relevance of digital rectal examination, transrectal ultrasound, and prostate-specific antigen in the diagnostic evaluation of patients with advanced carcinoma of the prostate in a resource poor environment. Sahel Med. J. 2016, 19, 27. [Google Scholar]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-targeted or standard biopsy for prostate-cancer diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Van der Leest, M.; Cornel, E.; Israel, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head comparison of transrectal ultrasound-guided prostate biopsy versus multiparametric prostate resonance imaging with subsequent magnetic resonance-guided biopsy in biopsy-naïve men with elevated prostate-specific antigen: A large prospective multicenter clinical study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [PubMed]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging – Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Steiger, P.; Thoeny, H.C. Prostate MRI based on PI-RADS version 2: How we review and report. Cancer Imaging 2016, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Purysko, A.S.; Rosenkrantz, A.B.; Turkbey, I.B.; Macura, K.J. RadioGraphics update: PI-RADS version 2.1—A pictorial update. Radiographics 2020, 40, E33–E37. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional networks for biomedical image segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015: 18th International Conference, Munich, Germany, 5–9 October 2015; Springer: Berlin/Heidelberg, Germany, 2015; pp. 234–241. [Google Scholar]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.; Petersen, J.; Maier-Hein, K.H. nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, C.; Cheng, D.; Wang, L.; Yang, X.; Cheng, K.T. Automated detection of clinically significant prostate cancer in mp-MRI images based on an end-to-end deep neural network. IEEE Trans. Med. Imaging 2018, 37, 1127–1139. [Google Scholar] [CrossRef]
- Arif, M.; Schoots, I.G.; Castillo Tovar, J.; Bangma, C.H.; Krestin, G.P.; Roobol, M.J.; Niessen, W.; Veenland, J.F. Clinically significant prostate cancer detection and segmentation in low-risk patients using a convolutional neural network on multi-parametric MRI. Eur. Radiol. 2020, 30, 6582–6592. [Google Scholar] [CrossRef] [PubMed]
- Hambarde, P.; Talbar, S.; Mahajan, A.; Chavan, S.; Thakur, M.; Sable, N. Prostate lesion segmentation in MR images using radiomics based deeply supervised U-Net. Biocybern. Biomed. Eng. 2020, 40, 1421–1435. [Google Scholar] [CrossRef]
- Qian, Y.; Zhang, Z.; Wang, B. ProCDet: A new method for prostate cancer detection based on mr images. IEEE Access 2021, 9, 143495–143505. [Google Scholar] [CrossRef]
- Seetharaman, A.; Bhattacharya, I.; Chen, L.C.; Kunder, C.A.; Shao, W.; Soerensen, S.J.; Wang, J.B.; Teslovich, N.C.; Fan, R.E.; Ghanouni, P.; et al. Automated detection of aggressive and indolent prostate cancer on magnetic resonance imaging. Med. Phys. 2021, 48, 2960–2972. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Shen, X.; Zhang, Y.D.; Luo, Y.; Luo, J.; Zhu, D.; Yang, H.; Wang, W.; Zhao, B.; Lu, J. Cross-modal prostate cancer segmentation via self-attention distillation. IEEE J. Biomed. Health Inform. 2021, 26, 5298–5309. [Google Scholar] [CrossRef] [PubMed]
- Mehralivand, S.; Yang, D.; Harmon, S.A.; Xu, D.; Xu, Z.; Roth, H.; Masoudi, S.; Sanford, T.H.; Kesani, D.; Lay, N.S.; et al. A cascaded deep learning–based artificial intelligence algorithm for automated lesion detection and classification on biparametric prostate magnetic resonance imaging. Acad. Radiol. 2022, 29, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Pellicer-Valero, O.J.; Marenco Jimenez, J.L.; Gonzalez-Perez, V.; Casanova Ramon-Borja, J.L.; Martín García, I.; Barrios Benito, M.; Pelechano Gomez, P.; Rubio-Briones, J.; Rupérez, M.J.; Martín-Guerrero, J.D. Deep learning for fully automatic detection, segmentation, and Gleason grade estimation of prostate cancer in multiparametric magnetic resonance images. Sci. Rep. 2022, 12, 2975. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Yuan, B.; Kou, W.; Yan, W.; Marshall, H.; Yang, Q.; Syer, T.; Punwani, S.; Emberton, M.; Barratt, D.C.; et al. Prostate cancer segmentation from MRI by a multistream fusion encoder. Med. Phys. 2023, 50, 5489–5504. [Google Scholar] [CrossRef]
- Villers, A.; Lemaitre, L.; Haffner, J.; Puech, P. Current status of MRI for the diagnosis, staging and prognosis of prostate cancer: Implications for focal therapy and active surveillance. Curr. Opin. Urol. 2009, 19, 274–282. [Google Scholar] [CrossRef]
- Zhao, F.; Xie, X. An overview of interactive medical image segmentation. Ann. BMVA 2013, 2013, 1–22. [Google Scholar]
- Kirillov, A.; Mintun, E.; Ravi, N.; Mao, H.; Rolland, C.; Gustafson, L.; Xiao, T.; Whitehead, S.; Berg, A.C.; Lo, W.Y.; et al. Segment anything. arXiv 2023, arXiv:2304.02643. [Google Scholar]
- Litjens, G.; Debats, O.; Barentsz, J.; Karssemeijer, N.; Huisman, H. Computer-aided detection of prostate cancer in MRI. IEEE Trans. Med. Imaging 2014, 33, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Li, L.; Bredell, G.; Li, J.; Unkelbach, J.; Konukoglu, E. Volumetric memory network for interactive medical image segmentation. Med. Image Anal. 2023, 83, 102599. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Luo, R.; Mao, J.; Xiao, T.; Jiang, Y. Acquisition of localization confidence for accurate object detection. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 784–799. [Google Scholar]
- Huang, Z.; Huang, L.; Gong, Y.; Huang, C.; Wang, X. Mask Scoring R-CNN. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019; pp. 6409–6418. [Google Scholar]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask R-CNN. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2961–2969. [Google Scholar]
- Eidex, Z.A.; Wang, T.; Lei, Y.; Axente, M.; Akin-Akintayo, O.O.; Ojo, O.A.A.; Akintayo, A.A.; Roper, J.; Bradley, J.D.; Liu, T.; et al. MRI-based prostate and dominant lesion segmentation using cascaded scoring convolutional neural network. Med. Phys. 2022, 49, 5216–5224. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Shen, L.; Sun, G. Squeeze-and-excitation networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 19–23 June 2018; pp. 7132–7141. [Google Scholar]
- Wang, X.; Girshick, R.; Gupta, A.; He, K. Non-local neural networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 19–23 June 2018; pp. 7794–7803. [Google Scholar]
- Tan, M.; Le, Q. EfficientNet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, PMLR, Long Beach, CA, USA, 9–15 June 2019; pp. 6105–6114. [Google Scholar]
- Ma, J.; He, Y.; Li, F.; Han, L.; You, C.; Wang, B. Segment anything in medical images. Nat. Commun. 2024, 15, 654. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.C.; Makowski, M.R.; Engel, G.; Rattunde, M.; Busch, F.; Asbach, P.; Niehues, S.M.; Vinayahalingam, S.; van Ginneken, B.; Litjens, G.; et al. Prostate158-An expert-annotated 3T MRI dataset and algorithm for prostate cancer detection. Comput. Biol. Med. 2022, 148, 105817. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef]
- Litjens, G.; Debats, O.; Barentsz, J.; Karssemeijer, N.; Huisman, H. ProstateX challenge data. Cancer Imaging Arch. 2017, 10, K9TCIA. [Google Scholar]
- Yan, W.; Yang, Q.; Syer, T.; Min, Z.; Punwani, S.; Emberton, M.; Barratt, D.; Chiu, B.; Hu, Y. The impact of using voxel-level segmentation metrics on evaluating multifocal prostate cancer localisation. In Proceedings of the International Workshop on Applications of Medical AI, Singapore, 18 September 2022; Springer: Berlin/Heidelberg, Germany, 2022; pp. 128–138. [Google Scholar]
- Le Nobin, J.; Rosenkrantz, A.B.; Villers, A.; Orczyk, C.; Deng, F.M.; Melamed, J.; Mikheev, A.; Rusinek, H.; Taneja, S.S. Image guided focal therapy for magnetic resonance imaging visible prostate cancer: Defining a 3-dimensional treatment margin based on magnetic resonance imaging histology co-registration analysis. J. Urol. 2015, 194, 364–370. [Google Scholar] [CrossRef]
- Gibson, E.; Bauman, G.S.; Romagnoli, C.; Cool, D.W.; Bastian-Jordan, M.; Kassam, Z.; Gaed, M.; Moussa, M.; Gómez, J.A.; Pautler, S.E.; et al. Toward prostate cancer contouring guidelines on magnetic resonance imaging: Dominant lesion gross and clinical target volume coverage via accurate histology fusion. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 188–196. [Google Scholar] [CrossRef]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. Pytorch: An imperative style, high-performance deep learning library. Adv. Neural Inf. Process. Syst. 2019, 32, 8026–8037. [Google Scholar]
- Loshchilov, I.; Hutter, F. Decoupled weight decay regularization. arXiv 2017, arXiv:1711.05101. [Google Scholar]
- Hatamizadeh, A.; Tang, Y.; Nath, V.; Yang, D.; Myronenko, A.; Landman, B.; Roth, H.R.; Xu, D. UNETR: Transformers for 3D medical image segmentation. In Proceedings of the IEEE/CVF Winter Conference on Applications of Computer Vision, Waikoloa, HI, USA, 3–8 January 2022; pp. 574–584. [Google Scholar]
- Luo, X.; Wang, G.; Song, T.; Zhang, J.; Aertsen, M.; Deprest, J.; Ourselin, S.; Vercauteren, T.; Zhang, S. MIDeepSeg: Minimally interactive segmentation of unseen objects from medical images using deep learning. Med. Image Anal. 2021, 72, 102102. [Google Scholar] [CrossRef] [PubMed]
- David, H.A.; Gunnink, J.L. The paired t test under artificial pairing. Am. Stat. 1997, 51, 9–12. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Ayoola, A.; Hoffman, D.; Khasgiwala, A.; Prabhu, V.; Smereka, P.; Somberg, M.; Taneja, S.S. The learning curve in prostate MRI interpretation: Self-directed learning versus continual reader feedback. Am. J. Roentgenol. 2017, 208, W92–W100. [Google Scholar] [CrossRef]
- Lee, G.H.; Chatterjee, A.; Karademir, I.; Engelmann, R.; Yousuf, A.; Giurcanu, M.; Harmath, C.B.; Karczmar, G.S.; Oto, A. Comparing radiologist performance in diagnosing clinically significant prostate cancer with multiparametric versus hybrid multidimensional MRI. Radiology 2022, 305, 399–407. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Prostate158 | PROSTATEx2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| DSC | 95% HD | TPR | PPV | F1 | DSC | 95% HD | TPR | PPV | F1 | |
| nnU-Net | 49.5 ± 32.4 | 10.4 ± 8.5 | 70.8 | 71.0 | 70.9 | 43.7 ± 34.3 | 12.6 ± 12.7 | 64.5 | 63.6 | 64.0 |
| UNETR | 51.0 ± 26.1 | 14.3 ± 10.7 | 75.0 | 42.1 | 55.1 | 44.3 ± 26.5 | 15.9 ± 10.6 | 71.0 | 49.4 | 58.3 |
| MIDeepSeg | 80.5 ± 10.6 | 8.2 ± 3.5 | 83.3 | 86.3 | 84.8 | 79.2 ± 11.9 | 3.0 ± 2.2 | 93.5 | 89.7 | 91.6 |
| SAM | 84.1 ± 8.6 | 6.5 ± 4.5 | 91.7 | 93.5 | 92.6 | 81.9 ± 10.7 | 10.8 ± 6.7 | 93.5 | 90.9 | 92.2 |
| ours (t = 0) | 49.3 ± 28.4 | 14.0 ± 12.1 | 62.5 | 46.9 | 53.6 | 42.5 ± 33.2 | 16.7 ± 14.3 | 51.6 | 44.8 | 48.0 |
| ours (t = 0.4) | 73.4 ± 16.2 | 8.7 ± 7.5 | 83.3 | 72.9 | 77.8 | 69.3 ± 21.4 | 14.0 ± 7.9 | 90.3 | 70.1 | 78.9 |
| ours (t = 0.7) | 83.2 ± 8.9 | 6.5 ± 4.6 | 91.7 | 91.8 | 91.7 | 81.0 ± 11.6 | 11.2 ± 7.0 | 93.5 | 88.3 | 90.8 |
| Bounding Box Extension Ratio | DSC | 95% HD | TPR | PPV | F1 |
|---|---|---|---|---|---|
| 10% | 74.0 ± 16.0 | 8.5 ± 7.4 | 83.3 | 72.9 | 77.8 |
| 20% | 73.9 ± 16.0 | 8.5 ± 7.5 | 83.3 | 72.9 | 77.8 |
| 30% | 73.6 ± 16.2 | 8.7 ± 7.5 | 83.3 | 72.9 | 77.8 |
| 40% | 73.4 ± 16.2 | 8.7 ± 7.5 | 83.3 | 72.9 | 77.8 |
| 50% | 72.7 ± 16.4 | 8.8 ± 7.5 | 83.3 | 72.9 | 77.8 |
| 60% | 71.8 ± 16.7 | 9.0 ± 7.8 | 83.3 | 72.9 | 77.8 |
| 80% | 69.4 ± 17.2 | 9.4 ± 8.0 | 83.3 | 71.2 | 76.8 |
| Methods | Training Time (h) | Inference Time (Ms/Image) |
|---|---|---|
| nnU-Net | 101.5 | 91.7 |
| UNETR | 14.6 | 24.4 |
| MIDeepSeg | 18.2 | 20.3 |
| SAM | 15.8 | 140.5 |
| ours | 1.8 + 6.5 + 15.8 | 175.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kou, W.; Rey, C.; Marshall, H.; Chiu, B. Interactive Cascaded Network for Prostate Cancer Segmentation from Multimodality MRI with Automated Quality Assessment. Bioengineering 2024, 11, 796. https://doi.org/10.3390/bioengineering11080796
Kou W, Rey C, Marshall H, Chiu B. Interactive Cascaded Network for Prostate Cancer Segmentation from Multimodality MRI with Automated Quality Assessment. Bioengineering. 2024; 11(8):796. https://doi.org/10.3390/bioengineering11080796
Chicago/Turabian StyleKou, Weixuan, Cristian Rey, Harry Marshall, and Bernard Chiu. 2024. "Interactive Cascaded Network for Prostate Cancer Segmentation from Multimodality MRI with Automated Quality Assessment" Bioengineering 11, no. 8: 796. https://doi.org/10.3390/bioengineering11080796