
Investigating User Identification in Remote Patient Monitoring Devices

Abstract
:1. Introduction
1.1. Terminologies
1.2. Theoretical Framework for Technology Acceptance
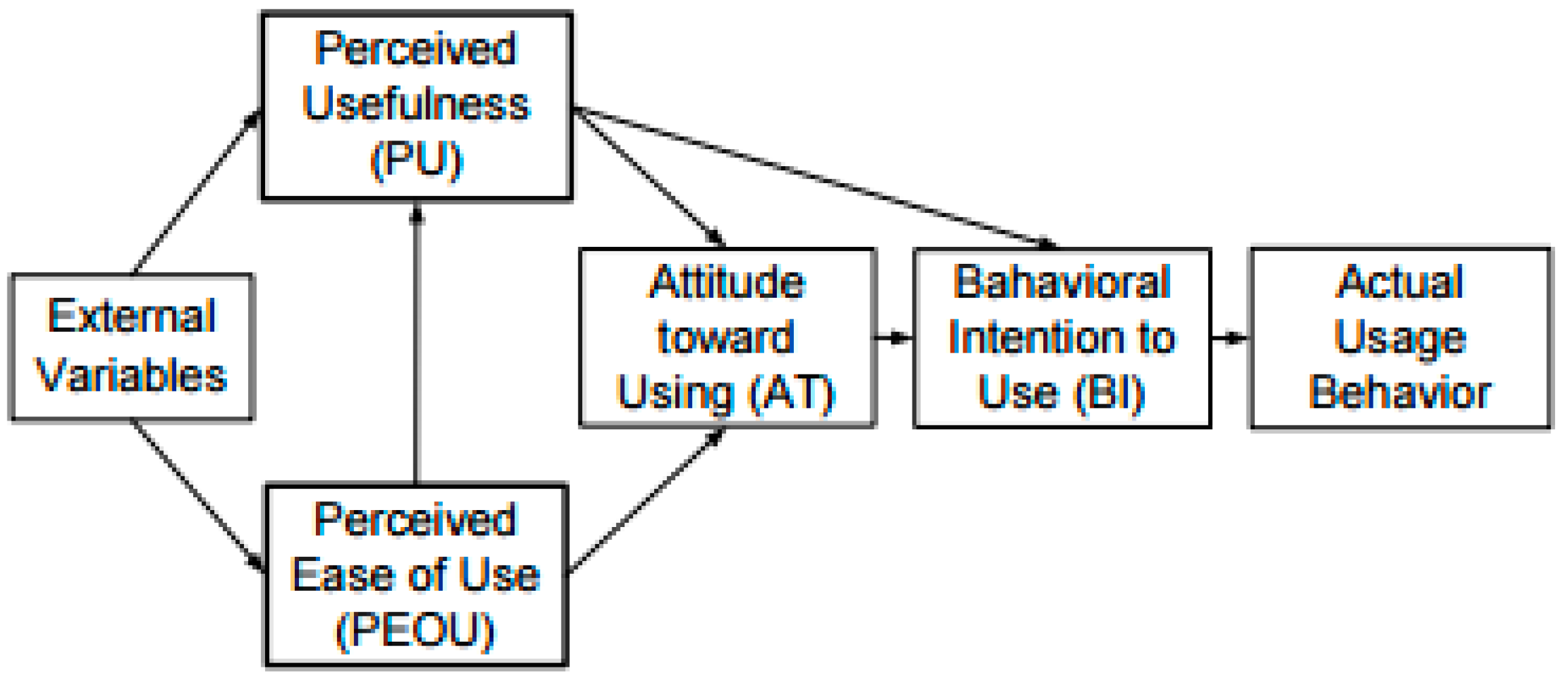
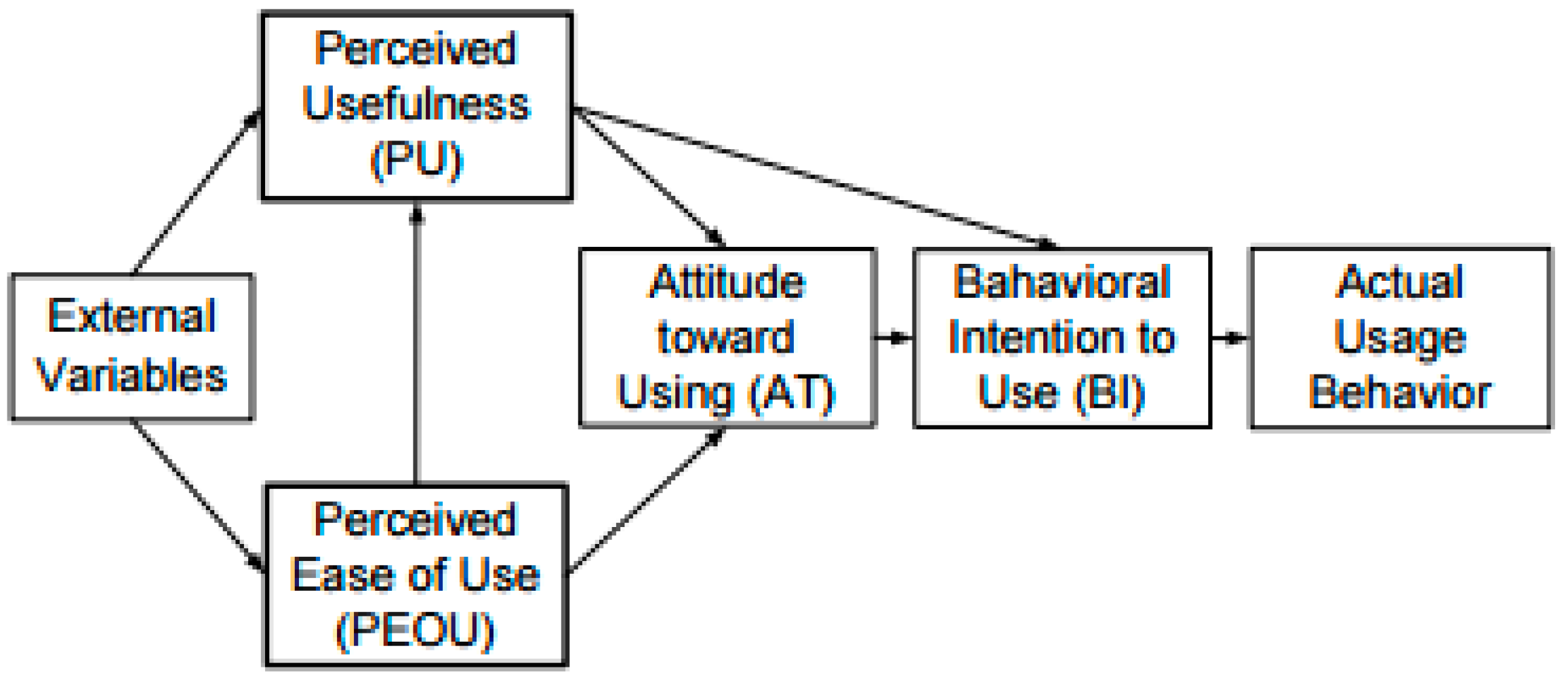
1.2.1. Technology Acceptance Model
1.2.2. Theory of Reasoned Action
- Develop RPM device modified with identification technology.
- Involve elderly in the design and development process.
- Investigate the experience of elderly people with the modified RPM to determine issues of continued use and if they would continue to use.
2. Materials and Methods
2.1. Study Design
2.1.1. Phase 1: Pre-Trial Focus Group
Sample
- Able to communicate in English language
- Age 64 years or above
- Registered with Chorleywood Health Centre or living in either of the two residential homes, a2Dominion and ISLAD
- Currently suffering from diabetes or hypertension.
2.1.2. Phase 2
2.1.3. Phase 3: Post Trial
- The patient touches their card/tag on the NFC reader until the LED indicates the card/tag has been recognised—the identification is sent to the PC.
- The patient takes their blood pressure using the modified prototype monitor—the measurement is sent to the PC.
- The PC saves the measurement and identification in a local database.
2.2. Ethics and Consent
2.3. Data Collection Instrument and Method
3. Results
3.1. Technology Assessment
3.2. Themes Phase 1: Pre-Trial
3.2.1. Patient Characteristics
Sub-Theme: Disease and Physiological Characteristics
Sub-Theme: Attitude to Learning and Technology Self-Efficacy
Sub-Theme: Exploration
Sub-Theme: Patient Involvement
Sub-Theme: Education, Training and Reviews
3.2.2. Theme 2: Technology Concerns
Sub-Theme: Technology Trust and Security
Sub-Theme: Cost
Sub-Theme: Reliability and Performance
Sub-Theme: Technology Benefit
3.2.3. Theme 3: Clinician Trust
3.3. Phase 2: Trial Data Analysis
3.3.1. Demographics
3.3.2. Observed Data Analysis
3.3.3. Overall Usage
3.3.4. Analysis of Multiple Use of the Same Card
3.3.5. Analysis of Tag Not Placed Properly on the Reader
3.3.6. Errors Made
- Multiple use of the same card; and
- Card not placed properly on the reader (reading alone).
3.3.7. Multiple Use of the Same Card
Example
3.3.8. Tag not Placed Properly on the Reader
3.3.9. Adherence to Monitoring Regimen
Missing Usage
3.4. Phase 3: Post Trial Focus Groups
3.4.1. Theme 1: Technology
Sub-Theme: Technology Design Preferences
3.4.2. Theme 2: Patient Characteristics
Sub-Theme: Trialling
Sub-Theme 2: Attitude and Support
4. Discussions
4.1. Phase 1
4.1.1. Patient Characteristics
4.1.2. Patient Education
4.1.3. Technology
4.1.4. Cost
4.1.5. Performance and Reliability
4.1.6. Clinician Trust
4.2. Study Phase 2: NFC Trial
4.2.1. Technology
4.2.2. Technology Concerns
4.2.3. Technology Design Preferences
4.2.4. Patient Characteristics and Technology Trialling
4.2.5. Clinicians Trust
Issues Encountered by Users
Same Tag Used Twice on the Same Day
Tag Not Placed Properly on the Reader
Adherence to Technology Trial
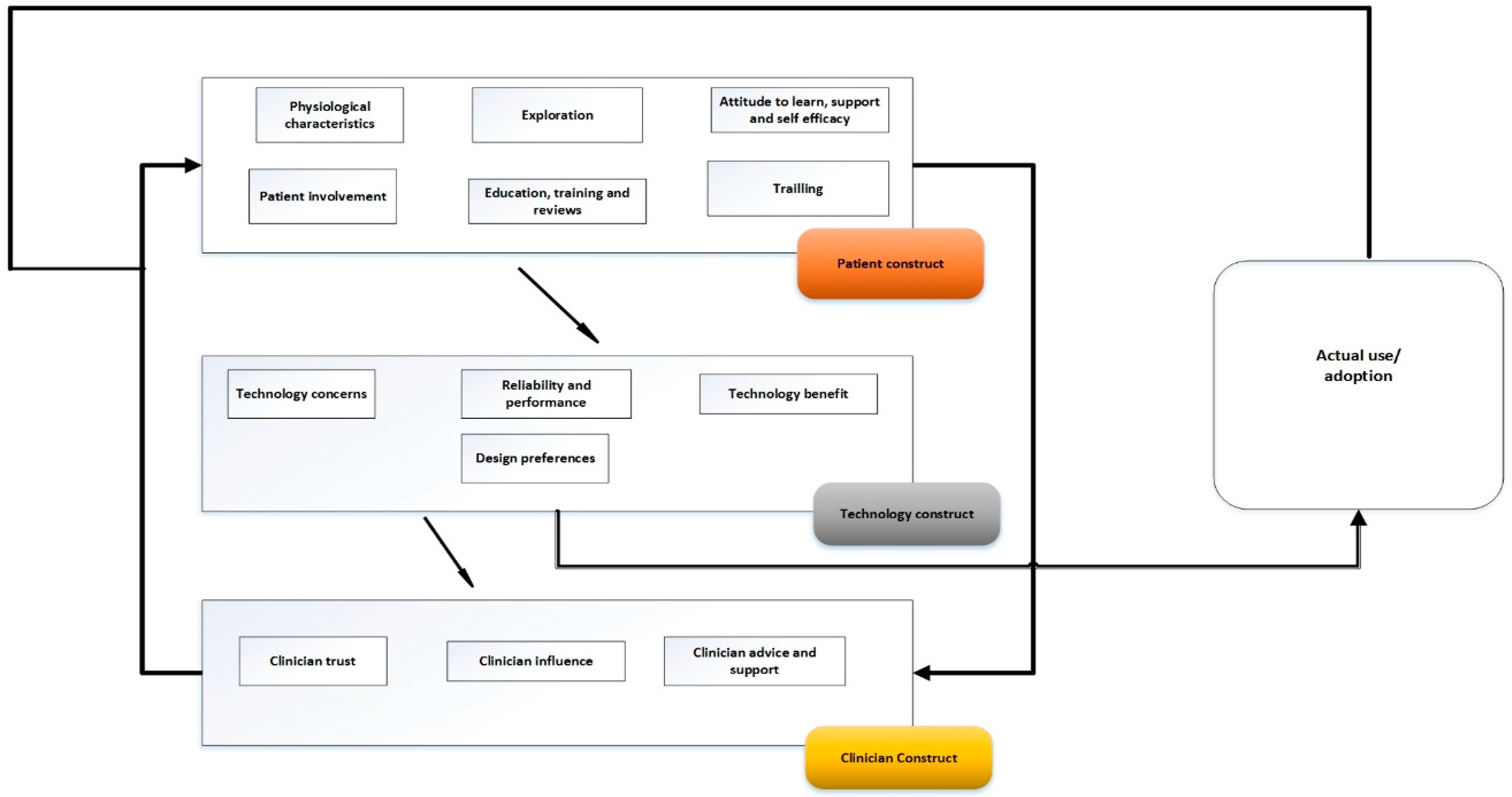
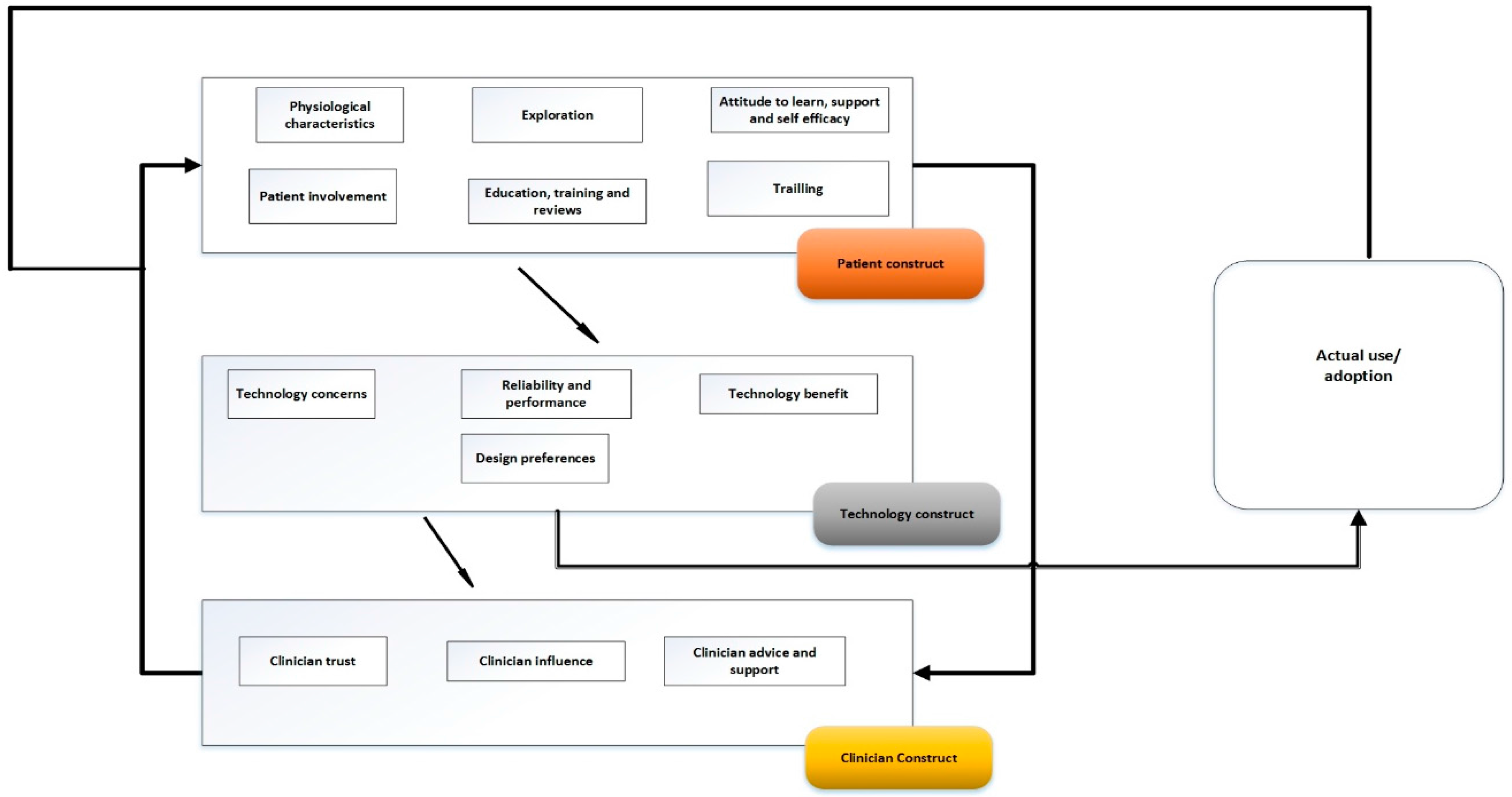
4.3. Proposing Senior Patients Technology Acceptance Model
4.3.1. Advantages of SPTAM
- Including social norms within the patient construct;
- Recognising the importance of user involvement in the design and decision; and
- Recognising the interaction between key players, in this case the effect of the attitude of the clinician towards the technology and their approach to the patient.
4.3.2. Study Limitations
- The limited set of patients from only two similar geographic areas.
- The study was carried out in North London and Berkshire, generally considered as an affluent and rural area.
- Participants were mainly white and results might differ from people of other ethnic origin, culture and customs.
- The use of prototype technology resulted in comments that might not apply to the final form of the technology (e.g., after integration).
4.3.3. Study Strengths
- Although the literature of Nielsen [50] specifies five participants may be sufficient to identify 80% to 85% of problems, in this study, problems were identified during Phase 1 and further problems were identified during Phase 3. This would justify the use of the much larger group of 40 participants (20 couples) to test the RPM technology system through a lived experience.
- The extended period of testing that matched the real-world use of the technology provided a robust testing of NFC for identification of RPM devices and helped to identify many usability issues.
- Identify and compare identification techniques for a multi-user environment where two or more people suffering from the same chronic disease are sharing a single device.
- Select and test an identification technique for a multi-user environment.
- Identify elderly patients’ beliefs, needs, and perceptions about the use of NFC for identification in RPM devices.
- Identify elderly patients’ behavioural usage and issues associated with using NFC for identification in RPM devices through a lived experience.
- Make recommendations for improved design of RPM devices.
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Age, UK. Later Life in the United Kingdom; Age UK: London, UK, 2015. [Google Scholar]
- Ondiege, B.; Clarke, M. Healthcare Professionals Perception on Information Security. Presented at the 5th International Conference on Internet Technologies & Society, Taipei, Taiwan, 10–12 December 2014. [Google Scholar]
- Ondiege, B.; Clarke, M.; Mapp, G. Exploring a New Security Framework for Remote Patient Monitoring Devices. Computers 2017, 6, 11. [Google Scholar] [CrossRef]
- Heinz, M.S. Exploring Predictors of Technology Adoption among Older Adults. Ph.D. Thesis, Iowa State University, Ames, Iowa, USA, 2013; p. 13155. [Google Scholar]
- Fischer, S.H.; David, D.; Crotty, B.H.; Dierks, M.; Safran, C. Acceptance and use of health information technology by community-dwelling elders. Int. J. Med. Inform. 2014, 83, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Polisena, J.; Tran, K.; Cimon, K.; Hutton, B.; McGill, S.; Palmer, K. Home telehealth for diabetes management: A systematic review and meta-analysis. Diabetes Obes. Metab. 2009, 11, 913–930. [Google Scholar] [CrossRef] [PubMed]
- Steele, R.; Lo, A.; Secombe, C.; Wong, Y.K. Elderly persons’ perception and acceptance of using wireless sensor networks to assist healthcare. Int. J. Med. Inform. 2009, 78, 788–801. [Google Scholar] [CrossRef] [PubMed]
- Ondiege, B.; Clarke, M. Healthcare professionals’ perception of security of Personal Health Devices. Smart Homecare Technology and TeleHealth 2017. in print. [Google Scholar] [CrossRef]
- Ondiege, B.; Clarke, M.; Mapp, G. Exploring Security of Remote Patient Monitoring Devices using NFC Technology for Identification of the Frail Elderly. In Proceedings of the 8th International Conference e-Health, Funchal, Portugal, 1–3 July 2016; pp. 1–3. [Google Scholar]
- Sylla, I.T. Technologies for remote patient monitoring. Electron. Prod. 2012, 54, 2–5. [Google Scholar]
- TSA. What Is Telehealth. Available online: http://www.telecare.org.uk/consumer-services/what-is-telehealth (accessed on 12 July 2016).
- Renaud, K.; Van Biljon, J. Predicting technology acceptance and adoption by the elderly: A qualitative study. In Proceedings of the 2008 Annual Research Conference of the South African Institute of Computer Scientists and Information Technologists on IT Research in Developing Countries: Riding the Wave of Technology, New York, NY, USA, 6–8 October 2008; pp. 210–219. [Google Scholar]
- Ajzen, I. From intentions to actions: A theory of planned behavior. In Action Control: From Cognition to Behavior; Kuhl, J., Beckmann, J, Eds.; Springer: Heidelberg/Berlin, Germany, 1985; pp. 11–39. [Google Scholar]
- Ogden, J. Some problems with social cognition models: A pragmatic & conceptual analysis. Health Psychol. 2003, 22, 424–428. [Google Scholar] [PubMed]
- INCASA. Grant Agreement No. 250505 inCASA. Integrated Network for Completely Assisted Senior Citizen’s Autonomy, D2. 6 Requirements Consolidation and Prioritisation Iteration 3. INCASA Project: Spain; INCASA: Ambavadi, India, 2012. [Google Scholar]
- REACTION (FP7 248590). D2-1 Scenarios for Usage of the REACTION Platform. Available online: http://www.reaction-project.eu/downloads/deliverables/D2-1_Scenarios_for_usage.pdf (accessed on 13 June 2016).
- Clarke, M.; Fursse, J.; Jones, R.W. Early experiences of the use of remote patient monitoring for the long term management of chronic disease. In Proceedings of Engineering in Medicine and Biology Society, the 30th Annual International Conference of the IEEE, Vancouver, BC, Canada, 20–25 August 2008; pp. 5863–5866. [Google Scholar]
- NICE. Information for the Public: High Blood Pressure. Available online: https://www.nice.org.uk/guidance/cg127/resources/information-for-the-public-high-blood-pressure-pdf (accessed on 21 November 2016).
- NICE Quality Standard [QS6] Diabetes in Adults Quality Standard. Available online: http://www.nice.org.uk/Guidance/QS6? (accessed on 13 June 2016).
- Van Boxtel, J.J.; Tsuchiya, N.; Koch, C. Consciousness and attention: on sufficiency and necessity. Front. Psychol. 2010, 1, 217. [Google Scholar] [CrossRef] [PubMed]
- Bagozzi, R.P. The legacy of the technology acceptance model and a proposal for a paradigm shift. J. Assoc. Inform. Syst. 2017, 8, 244–254. [Google Scholar]
- Chen, K.; Chan, A.H.S. A review of technology acceptance by older adults. Gerontechnology 2011, 10. [Google Scholar] [CrossRef]
- Fazio, R.H. How Do Attitudes Guide Behavior? In The Handbook of Motivation and Cognition: Foundation of Social Behavior; Sorrentino, R.M., Higgins, E.T., Eds.; Guilford Press: New York, NY, USA, 1986; pp. 204–243. [Google Scholar]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar]
- Cimperman, M.; Brenčič, M.M.; Trkman, P.; Stanonik, M.D.L. Older adults’ perceptions of home telehealth services. Telemed. e-Health 2013, 19, 786–790. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, R.A.; Hueros, A.D. Motivational factors that influence the acceptance of Moodle using TAM. Comput. Hum. Behav. 2010, 26, 1632–1640. [Google Scholar] [CrossRef]
- Brandtzæg, P.B.; Heim, J.; Karahasanović, A. Understanding the new digital divide—A typology of Internet users in Europe. Int. J. Hum.-Comput. Stud. 2011, 69, 123–138. [Google Scholar] [CrossRef]
- Gefen, D.; Straub, D. The relative importance of perceived ease of use in IS adoption: A study of e-commerce adoption. J. Assoc. Inform. Syst. 2000, 1, 8. [Google Scholar]
- De Folter, J.; Gokalp, H.; Fursse, J.; Sharma, U.; Clarke, M. Designing effective visualizations of habits data to aid clinical decision making. BMC Med. Inform. Decis. Mak. 2014, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, H.K. What does an e-mail address add?—Doing health and technology at home. Soc. Sci. Med. 2011, 72, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Saito, D.; Saito, K.; Notomi, K.; Saito, M. The effect of age on web-safe color visibility for a white background. In Proceedings of Engineering in Medicine and Biology Society, the 28th Annual International Conference of the IEEE, New York, NY, USA, 30 August–3 September 2006; pp. 5145–5148. [Google Scholar]
- Money, A.G.; Barnett, J.; Kuljis, J. Public claims about automatic external defibrillators: An online consumer opinions study. BMC Public Health 2011, 11, 332. [Google Scholar] [CrossRef] [PubMed]
- Mitzner, T.L.; Boron, J.B.; Fausset, C.B.; Adams, A.E.; Charness, N.; Czaja, S.J.; Dijkstra, K.; Fisk, A.D.; Rogers, W.A.; Sharit, J. Older adults talk technology: Technology usage and attitudes. Comput. Hum. Behav. 2010, 26, 1710–1721. [Google Scholar] [CrossRef] [PubMed]
- Welsh, S.; Hassiotis, A.; O’mahoney, G.; Deahl, M. Big brother is watching you—The ethical implications of electronic surveillance measures in the elderly with dementia and in adults with learning difficulties. Aging Ment. Health 2003, 7, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.G.S.; Fitton, R.; Hannan, A.; Fisher, B.; Young, T.; Barnett, J. Accessing personal medical records online: A means to what ends? Int. J. Med. Inform. 2015, 84, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.G.S.; Barnet, J.; Kuljis, J.; Hone, K.; Kaczmarski, R. Patients’ experiences with hospital outpatient anticoagulation services: Dimensions and determinants. Int. J. Person Cent. Med. 2012, 2, 669–679. [Google Scholar]
- Venkatesh, V.; Thong, J.Y.; Xu, X. Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar]
- Chou, C.C.; Chang, C.P.; Lee, T.T.; Chou, H.F.; Mills, M.E. Technology acceptance and quality of life of the elderly in a telecare program. Comput. Inform. Nurs. 2013, 31, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.G.S.; Barnett, J.; Kuljis, J.; Hone, K.; Kaczmarski, R. Factors determining patients’ intentions to use point-of-care testing medical devices for self-monitoring: The case of international normalized ratio self-testing. Patient Prefer. Adherence 2013, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wild, K.; Boise, L.; Lundell, J.; Foucek, A. Unobtrusive In-Home Monitoring of Cognitive and Physical Health: Reactions and Perceptions of Older Adults. J. Appl. Gerontol. 2008, 27, 181–200. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.G.; Mahoney, D.F.; Hoenig, H.; Hirth, V.A.; Bonato, P.; Hajjar, I.; Lipsitz, L.A. In situ monitoring of health in older adults: Technologies and issues. J. Am. Geriatr. Soc. 2010, 58, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Abramson, Z.H.; Cohen-Naor, V. Factors associated with performance of influenza immunization among the elderly. Isr. Med. Assoc. J. 2000, 2, 902–907. [Google Scholar] [PubMed]
- Botsis, T.; Hartvigsen, G. Current status and future perspectives in telecare for elderly people suffering from chronic diseases. J. Telemed. Telecare 2008, 14, 195–203. [Google Scholar] [CrossRef] [PubMed]
- The Kings Fund (2016). Five Big Issues for Health and Social Care after the Brexit Vote | The King’s Fund. Available online: https://www.kingsfund.org.uk/publications/articles/brexit-and-nhs (accessed on 5 September 2016).
- Barnard, Y.; Bradley, M.D.; Hodgson, F.; Lloyd, A.D. Learning to use new technologies by older adults: Perceived difficulties, experimentation behaviour and usability. Comput. Hum. Behav. 2013, 29, 1715–1724. [Google Scholar] [CrossRef]
- Shah, S.G.S.; Robinson, I. Medical device technologies: Who is the user? Int. J. Healthc. Technol. Manag. 2008, 9, 181–197. [Google Scholar] [CrossRef]
- Heart, T.; Kalderon, E. Older adults: Are they ready to adopt health-related ICT? Int. J. Med. Inform. 2013, 82, 209–231. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.G.S.; Robinson, I. Benefits of and barriers to involving users in medical device technology development and evaluation. Int. J. Technol. Assess. Healthc. 2007, 23, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, B. Factors Affecting Computer Use among Older Adult Users: A Study in the Backdrop of Florida State University; ProQuest Dissertations Publishing: Ann Arbor, MI, USA, 2008; p. 217. [Google Scholar]
- Nielsen, J.; Landauert, T.K. A mathematical model of the finding of usability problems. In Proceedings of the INTERACT’93 and CHI’93 Conference on Human Factors in Computing Systems, Amsterdam, The Netherlands, 24–29 April 1993; pp. 206–213. [Google Scholar]

{kind=link}
{kind=link}
| Age (Years) | Gender | Participants |
|---|---|---|
| 65–75 | M | 8 |
| F | 10 | |
| 75–85 | M | 8 |
| F | 7 | |
| 86–95 | M | 4 |
| F | 3 | |
| Total | 40 | |
| Errors Made (%) | Day | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
| Multiple Use of the Same Card | 2.5 | 0 | 0 | 0 | 5 | 0 | 0 | 7.5 | 0 | 0 | 0 | 0 | 0 | 2.5 |
| Tag not Placed Properly on the Reader | 2.5 | 5 | 2.5 | 0 | 5 | 2.5 | 0 | 2.5 | 0 | 0 | 2.5 | 0 | 2.5 | 0 |
| Total | 5 | 5 | 2.5 | 0 | 10 | 2.5 | 0 | 10 | 0 | 0 | 2.5 | 0 | 2.5 | 2.5 |
| Missing Usage (%) | Day | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
| 2.5 | 0 | 0 | 0 | 5 | 0 | 0 | 7.5 | 2.5 | 0 | 0 | 0 | 0 | 2.5 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ondiege, B.; Clarke, M. Investigating User Identification in Remote Patient Monitoring Devices. Bioengineering 2017, 4, 76. https://doi.org/10.3390/bioengineering4030076
Ondiege B, Clarke M. Investigating User Identification in Remote Patient Monitoring Devices. Bioengineering. 2017; 4(3):76. https://doi.org/10.3390/bioengineering4030076
Chicago/Turabian StyleOndiege, Brian, and Malcolm Clarke. 2017. "Investigating User Identification in Remote Patient Monitoring Devices" Bioengineering 4, no. 3: 76. https://doi.org/10.3390/bioengineering4030076
APA StyleOndiege, B., & Clarke, M. (2017). Investigating User Identification in Remote Patient Monitoring Devices. Bioengineering, 4(3), 76. https://doi.org/10.3390/bioengineering4030076