
Learning from conect4children: A Collaborative Approach towards Standardisation of Disease-Specific Paediatric Research Data
 , , , , , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
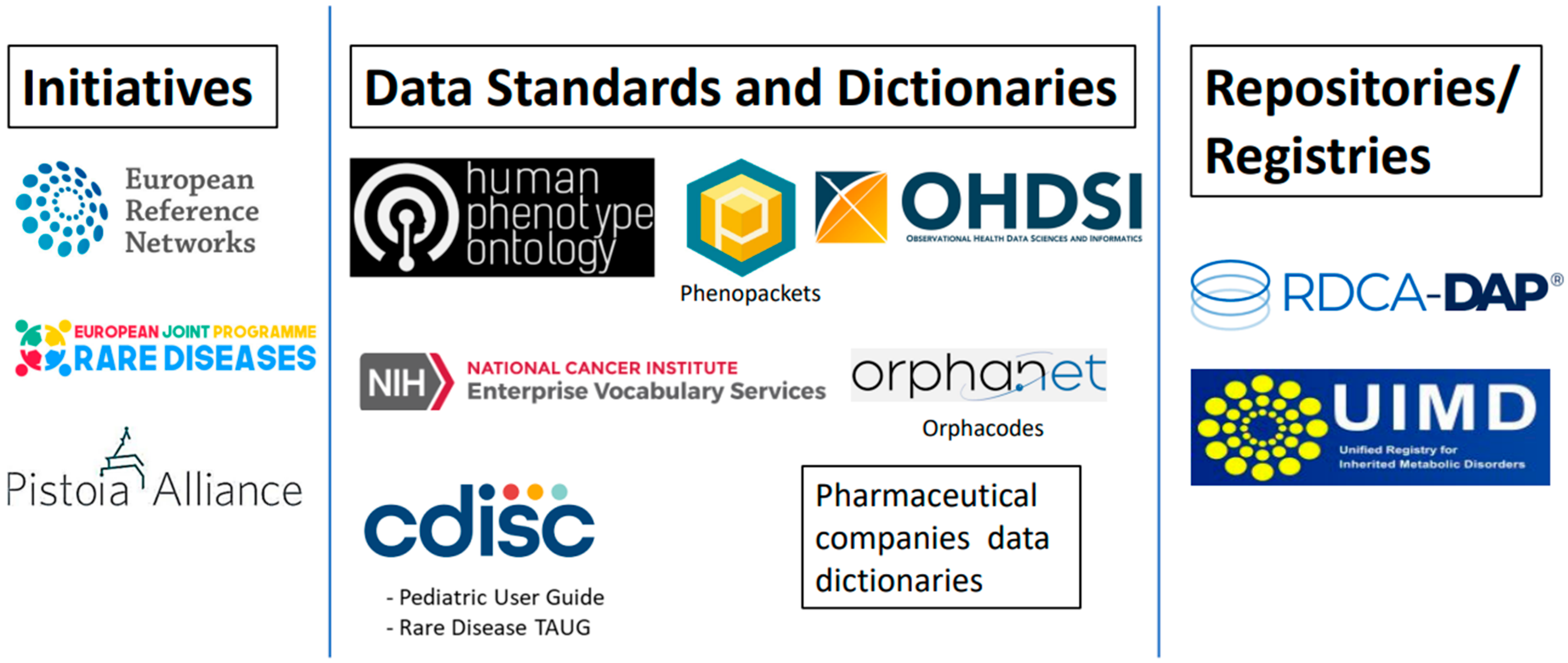
2.1. Large Initiatives
2.1.1. European Reference Network (ERN)
2.1.2. European Joint Programme on Rare Disease (EJP RD)
2.1.3. Pistoia Alliance
2.1.4. Other Initiatives of Relevance to Paediatrics
2.2. Data Repositories and Registries
2.2.1. Rare Disease Cures Accelerator—Data Analytics Platform (RDCA-DAP)
2.2.2. Unified European Registry for Inherited Metabolic Disorders (U-IMD)
2.2.3. Other Repositories
2.3. Data Standards and Dictionaries
2.3.1. Clinical Data Interchange Standards Consortium (CDISC) Therapeutic Area Standards
2.3.2. Observational Medical Outcomes Partnership (OMOP) Common Data Model (CDM)
2.3.3. National Cancer Institute (NCI) Enterprise Vocabulary Service (EVS)
2.3.4. Human Phenotype Ontology (HPO) and the GA4GH Phenopacket Schema
2.3.5. Orphacodes
2.3.6. Industry Data Dictionaries
2.3.7. Other Data Standards and Dictionaries Relevant to Paediatrics
3. Results
Plan of Action
- Formalisation of a multi-stakeholder, multi-project user group consisting of members with a wide range of expertise. This group would be responsible for ensuring the progress of all other action points.
- Use the FAIR4Clin guide for the FAIRification of metadata for industrial and academic paediatric clinical trials.
- Conduct a Phenopackets pilot that would standardise data from multiple studies in RDCA-DAP and test how pooled data could be used.
- Using Orphacodes in case report forms for industrial and academic clinical trials.
- Introducing and educating ERNs with the use of CDISC standards.
- Exploring applications of the CDISC PUG (potentially using data from all mentioned data sources—RDCA-DAP and U-IMD).
- Organisation of workshops and educational materials to foster collaboration.
4. Discussion
4.1. Action 1—Establishment of the Global Paediatric Data (GLOPAD) Forum
4.2. Action 2—FAIRification of Metadata
4.3. Action 3—Phenopackets Pilot
4.4. Action 4—Orpahcodes in CRFs
4.5. Action 5—Educating ERNs about CDISC Standards
4.6. Action 6—Applications of the PUG
4.7. Action 7—Workshops and Educational Materials
4.7.1. Wider Dissemination
4.7.2. Future beyond c4c
4.7.3. Challenges
4.7.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Turner, M.A.; Hildebrand, H.; Fernandes, R.M.; de Wildt, S.N.; Mahler, F.; Hankard, R.; Leary, R.; Bonifazi, F.; Nobels, P.; Cheng, K.; et al. The conect4children (c4c) Consortium: Potential for Improving European Clinical Research into Medicines for Children. Pharm. Med. 2021, 35, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.; Cranswick, N. Clinical trials, ethical issues and patient recruitment: An Australian perspective. Paediatr. Perinat. Drug Ther. 2003, 5, 183–187. [Google Scholar] [CrossRef]
- Joseph, P.D.; Craig, J.C.; Caldwell, P.H.Y. Clinical trials in children. Br. J. Clin. Pharmacol. 2015, 79, 357–369. [Google Scholar] [CrossRef] [PubMed]
- von Baeyer, C.L. Children’s self-reports of pain intensity: Scale selection, limitations and interpretation. Pain. Res. Manag. 2006, 11, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Toma, M.; Felisi, M.; Bonifazi, D.; Bonifazi, F.; Giannuzzi, V.; Reggiardo, G.; De Wildt, S.; Ceci, A. Paediatric Medicines in Europe: The Paediatric Regulation-Is It Time for Reform? Front. Med. 2021, 8, 593281. [Google Scholar] [CrossRef] [PubMed]
- Ollivier, C.; Sun, H.; Amchin, W.; Beghetti, M.; Berger, R.M.; Breitenstein, S.; Garnett, C.; Gullberg, N.; Hassel, P.; Ivy, D. New strategies for the conduct of clinical trials in pediatric pulmonary arterial hypertension: Outcome of a multistakeholder meeting with patients, academia, industry, and regulators, held at the European Medicines Agency on Monday, June 12, 2017. J. Am. Heart Assoc. 2019, 8, e011306. [Google Scholar] [CrossRef] [PubMed]
- Horton, D.B.; Blum, M.D.; Burcu, M. Real-World Evidence for Assessing Treatment Effectiveness and Safety in Pediatric Populations. J. Pediatr. 2021, 238, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, J.C. The Scarcity of Approved Pediatric High-Risk Medical Devices. JAMA Netw. Open 2021, 4, e2112760. [Google Scholar] [CrossRef] [PubMed]
- Goulooze, S.C.; Zwep, L.B.; Vogt, J.E.; Krekels, E.H.J.; Hankemeier, T.; van den Anker, J.N.; Knibbe, C.A.J. Beyond the Randomized Clinical Trial: Innovative Data Science to Close the Pediatric Evidence Gap. Clin. Pharmacol. Ther. 2020, 107, 786–795. [Google Scholar] [CrossRef] [PubMed]
- van der Steen, J.; Kruse, R.; Szafara, K.; Mehr, D.; van der Wal, G.; Ribbe, M.; D’Agostino, R. Benefits and pitfalls of pooling datasets from comparable observational studies: Combining US and Dutch nursing home studies. Palliat. Med. 2008, 22, 750–759. [Google Scholar] [CrossRef]
- Patsopoulos, N.A. A pragmatic view on pragmatic trials. Dialogues Clin. Neurosci. 2011, 13, 217–224. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, M.; Krailo, M.; Anderson, J.R.; Reaman, G.H. Progress in childhood cancer: 50 Years of research collaboration, a report from the Children’s Oncology Group. Semin. Oncol. 2008, 35, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Zurynski, Y.; Gonzalez, A.; Deverell, M.; Phu, A.; Leonard, H.; Christodoulou, J.; Elliott, E. Rare disease: A national survey of paediatricians’ experiences and needs. BMJ Paediatr. Open 2017, 1, e000172. [Google Scholar] [CrossRef] [PubMed]
- Bavisetty, S.; Grody, W.W.; Yazdani, S. Emergence of pediatric rare diseases: Review of present policies and opportunities for improvement. Rare Dis. 2013, 1, e23579. [Google Scholar] [CrossRef] [PubMed]
- The Lancet, Diabetes & Endocrinology. Spotlight on rare diseases. Lancet Diabetes Endocrinol. 2019, 7, 75. [Google Scholar] [CrossRef] [PubMed]
- Kempf, L.; Goldsmith, J.C.; Temple, R. Challenges of developing and conducting clinical trials in rare disorders. Am. J. Med. Genet. A 2018, 176, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.; Hedley, V.; Owen, J.; Cornet, R.; Kalra, D.; Engel, C.; Palmeri, A.; Lee, J.; Roze, J.-C.; Standing, J.F.; et al. Standardizing Paediatric Clinical Data: The Development of the conect4children (c4c) Cross Cutting Paediatric Data Dictionary. J. Soc. Clin. Data Manag. 2022, 2. [Google Scholar] [CrossRef]
- Amadi, C.; Leary, R.; Palmeri, A.; Hedley, V.; Sen, A.; Siddiqui, R.Q.; Kalra, D.; Straub, V. How Can a Clinical Data Modelling Tool Be Used to Represent Data Items of Relevance to Paediatric Clinical Trials? Learning from the Conect4children (c4c) Consortium. Appl. Sci. 2022, 12, 1604. [Google Scholar] [CrossRef]
- CDISC. Pediatrics User Guide v1.0. Available online: https://www.cdisc.org/standards/therapeutic-areas/pediatrics/pediatrics-user-guide-v1-0 (accessed on 12 August 2023).
- Hwang, T.J.; Tomasi, P.A.; Bourgeois, F.T. Delays in completion and results reporting of clinical trials under the Paediatric Regulation in the European Union: A cohort study. PLoS Med. 2018, 15, e1002520. [Google Scholar] [CrossRef] [PubMed]
- Randeree, L.; Eslick, G.D. Eteplirsen for paediatric patients with Duchenne muscular dystrophy: A pooled-analysis. J. Clin. Neurosci. 2018, 49, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Aartsma-Rus, A.; Goemans, N. A Sequel to the Eteplirsen Saga: Eteplirsen Is Approved in the United States but Was Not Approved in Europe. Nucleic Acid. Ther. 2019, 29, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.T.; Swain, R.S.; Tian, F.; Okusanya, O.O.; Waldron, P.; Khurana, M.; Durmowicz, E.L.; Ma, Y.; Major, J.M.; Gelperin, K. Effects of deferasirox dose and decreasing serum ferritin concentrations on kidney function in paediatric patients: An analysis of clinical laboratory data from pooled clinical studies. Lancet Child. Adolesc. Health 2019, 3, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Dilleen, M.; Liyanage, W.; Aikman, L.; Szczypa, P.; Dressler, C. Time, Psoriasis Area and Severity Index and Dermatology Life Quality Index of patients with psoriasis who drop out of clinical trials on etanercept because of lack of efficacy: A pooled analysis from 10 clinical trials. Br. J. Dermatol. 2018, 178, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Héon-Klin, V. European Reference networks for rare diseases: What is the conceptual framework? Orphanet J. Rare Dis. 2017, 12, 137. [Google Scholar] [CrossRef] [PubMed]
- European Commision. Set of Common Data Elements. Available online: https://eu-rd-platform.jrc.ec.europa.eu/set-of-common-data-elements_en (accessed on 1 August 2023).
- Bassanese, G.; Wlodkowski, T.; Servais, A.; Heidet, L.; Roccatello, D.; Emma, F.; Levtchenko, E.; Ariceta, G.; Bacchetta, J.; Capasso, G.; et al. The European Rare Kidney Disease Registry (ERKReg): Objectives, design and initial results. Orphanet J. Rare Dis. 2021, 16, 251. [Google Scholar] [CrossRef] [PubMed]
- dos Santos Vieira, B.; Bernabé, C.H.; Zhang, S.; Abaza, H.; Benis, N.; Cámara, A.; Cornet, R.; Le Cornec, C.M.A.; ‘t Hoen, P.A.C.; Schaefer, F.; et al. Towards FAIRification of sensitive and fragmented rare disease patient data: Challenges and solutions in European reference network registries. Orphanet J. Rare Dis. 2022, 17, 436. [Google Scholar] [CrossRef] [PubMed]
- EJPRD. Periodic Reporting for Period 3—EJP RD (European Joint Programme on Rare Diseases). Available online: https://cordis.europa.eu/project/id/825575/reporting (accessed on 15 May 2023).
- EJPRD. Innovation Management Toolbox. Available online: https://imt.ejprarediseases.org/ (accessed on 1 May 2023).
- Wise, J.; de Barron, A.G.; Splendiani, A.; Balali-Mood, B.; Vasant, D.; Little, E.; Mellino, G.; Harrow, I.; Smith, I.; Taubert, J.; et al. Implementation and relevance of FAIR data principles in biopharmaceutical R&D. Drug Discov. Today 2019, 24, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Harrow, I.; Balakrishnan, R.; Küçük McGinty, H.; Plasterer, T.; Romacker, M. Maximizing data value for biopharma through FAIR and quality implementation: FAIR plus Q. Drug Discov. Today 2022, 27, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Elixir and FAIR Cookbook. Available online: https://faircookbook.elixir-europe.org/content/home.html (accessed on 1 June 2023).
- Harrow, I.; Liener, T.; Romacker, M.; Barron, A.G.d.; Plasterer, T.; Juty, N.; Balakrishnan, R.; Gardner, B.; Leerkes, M.; Rocca-Serra, P.; et al. FAIR4Clin. Available online: http://fair4clin.pistoiaalliance.org/ (accessed on 1 August 2023).
- Demotes-Mainard, J. ECRIN (European clinical research infrastructures network), a pan-European infrastructure for clinical research. Bull. L’académie Natl. Méd. 2010, 194, 1683–1694. [Google Scholar] [CrossRef]
- Demotes-Mainard, J.; Kubiak, C. A European perspective—the European clinical research infrastructures network. Ann. Oncol. 2011, 22, vii44–vii49. [Google Scholar] [CrossRef] [PubMed]
- Ferlini, A.; Fortunato, F.; Farnè, M.; Selvatici, R.; Blankart, C.; Röttger, R.; Kirschner, J.; Schenk, J.; Zarakowska, K.; Zschüntzsch, J.P. 35 Genetic newborn screening and digital technologies to accelerate rare disease diagnosis: The EU-IMI screen4Care project. Neuromuscul. Disord. 2022, 32, S57. [Google Scholar] [CrossRef]
- Alessandrini, E.; Brako, F.; Scarpa, M.; Lupo, M.; Bonifazi, D.; Pignataro, V.; Cavallo, M.; Cullufe, O.; Enache, C.; Nafria, B.; et al. Children’s Preferences for Oral Dosage Forms and Their Involvement in Formulation Research via EPTRI (European Paediatric Translational Research Infrastructure). Pharmaceutics 2021, 13, 730. [Google Scholar] [CrossRef] [PubMed]
- Scutariu, C.; Bilardi, D.; Ayomoh, F.I.; Roehr, C.C. The Mini-Symposium on Global Child Health: Serving the Children of the World. Pediatr. Res. 2023, 94, 875–877. [Google Scholar] [CrossRef] [PubMed]
- Vassal, G.; Ladenstein, R.; Schrappe, M.; Pritchard-Jones, K.; Biondi, A.; Eggert, A.; Hjorth, L.; Kowalczyk, J.; Perilongo, G.; Pieters, R. The SIOPE strategic plan: A European cancer plan for children and adolescents. J. Cancer Policy 2015, 8, 17–32. [Google Scholar] [CrossRef]
- Ruperto, N.; Martini, A. Networking in paediatrics: The example of the Paediatric Rheumatology International Trials Organisation (PRINTO). Arch. Dis. Child. 2011, 96, 596–601. [Google Scholar] [CrossRef] [PubMed]
- De Boeck, K.; Bulteel, V.; Tiddens, H.; Wagner, T.; Fajac, I.; Conway, S.; Dufour, F.; Smyth, A.; Lee, T.-m.; Sermet, I. Guideline on the design and conduct of cystic fibrosis clinical trials: The European Cystic Fibrosis Society–Clinical Trials Network (ECFS-CTN). J. Cyst. Fibros. 2011, 10, S67–S74. [Google Scholar] [CrossRef] [PubMed]
- Leary, R.; Oyewole, A.O.; Bushby, K.; Aartsma-Rus, A. Translational Research in Europe for the Assessment and Treatment for Neuromuscular Disorders (TREAT-NMD). Neuropediatrics 2017, 48, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Kountouris, P.; Stephanou, C.; Archer, N.; Bonifazi, F.; Giannuzzi, V.; Kuo, K.H.M.; Maggio, A.; Makani, J.; Mañú-Pereira, M.D.M.; Michailidou, K.; et al. The International Hemoglobinopathy Research Network (INHERENT): An international initiative to study the role of genetic modifiers in hemoglobinopathies. Am. J. Hematol. 2021, 96, E416–E420. [Google Scholar] [CrossRef] [PubMed]
- C-PATH. Rare Disease Drug Development. Available online: https://c-path.org/programs/rdca-dap/ (accessed on 1 May 2023).
- Barrett, J.S.; Betourne, A.; Walls, R.L.; Lasater, K.; Russell, S.; Borens, A.; Rohatagi, S.; Roddy, W. The future of rare disease drug development: The rare disease cures accelerator data analytics platform (RDCA-DAP). J. Pharmacokinet. Pharmacodyn. 2023, 50, 507–519. [Google Scholar] [CrossRef]
- Larkindale, J.; Betourne, A.; Borens, A.; Boulanger, V.; Theurer Crider, V.; Gavin, P.; Burton, J.; Liwski, R.; Romero, K.; Walls, R.; et al. Innovations in Therapy Development for Rare Diseases Through the Rare Disease Cures Accelerator-Data and Analytics Platform. Ther. Innov. Regul. Sci. 2022, 56, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Opladen, T.; Gleich, F.; Kozich, V.; Scarpa, M.; Martinelli, D.; Schaefer, F.; Jeltsch, K.; Juliá-Palacios, N.; García-Cazorla, Á.; Dionisi-Vici, C.; et al. U-IMD: The first Unified European registry for inherited metabolic diseases. Orphanet J. Rare Dis. 2021, 16, 95. [Google Scholar] [CrossRef] [PubMed]
- Modi, N. Information technology infrastructure, quality improvement and research: The UK National Neonatal Research Database. Transl. Pediatr. 2019, 8, 193–198. [Google Scholar] [CrossRef] [PubMed]
- FDA. Study Data Standard: What You Need to Know. Available online: https://www.fda.gov/files/drugs/published/Study-Data-Standards--What-You-Need-to-Know.pdf (accessed on 9 February 2022).
- Facile, R.; Muhlbradt, E.E.; Gong, M.; Li, Q.; Popat, V.; Pétavy, F.; Cornet, R.; Ruan, Y.; Koide, D.; Saito, T.I.; et al. Use of Clinical Data Interchange Standards Consortium (CDISC) Standards for Real-world Data: Expert Perspectives From a Qualitative Delphi Survey. JMIR Med. Inform. 2022, 10, e30363. [Google Scholar] [CrossRef] [PubMed]
- Bobbitt, D.R.; LeRoy, B.; Palmer, A.; Hamidi, M.; Facile, R.; Ueno, S.; Hume, S.; Van Reusel, P.; Neville, J. Clinical data standards and the new world of research science, technology, and data sources. J. Natl. Inst. Public. Health 2019, 68, 194–201. [Google Scholar] [CrossRef]
- EMA. European Medicines Regulatory Network Data Standardisation Strategy. Available online: https://www.ema.europa.eu/en/documents/other/european-medicines-regulatory-network-data-standardisation-strategy_en.pdf (accessed on 1 July 2023).
- CDISC. Rare Diseases Therapeutic Area User Guide. Available online: https://www.cdisc.org/public-review/rare-diseases-therapeutic-area-user-guide (accessed on 1 May 2023).
- Blacketer, C. The Common Data Model. In The Book of OHDSI; Observational Health Data Sciences and Informatics: New York, NY, USA, 2019. [Google Scholar]
- Biedermann, P.; Ong, R.; Davydov, A.; Orlova, A.; Solovyev, P.; Sun, H.; Wetherill, G.; Brand, M.; Didden, E.-M. Standardizing registry data to the OMOP Common Data Model: Experience from three pulmonary hypertension databases. BMC Med. Res. Methodol. 2021, 21, 238. [Google Scholar] [CrossRef] [PubMed]
- Lima, D.M.; Rodrigues-Jr, J.F.; Traina, A.J.M.; Pires, F.A.; Gutierrez, M.A. Transforming Two Decades of ePR Data to OMOP CDM for Clinical Research. Stud. Health Technol. Inform. 2019, 264, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Takahara, S.; Saito, T.I.; Imai, Y.; Kawakami, T.; Murayama, T. A use-case analysis of Clinical Data Interchange Standards Consortium/Study Data Tabulation Model in academia in an investigator-initiated clinical trial. Nagoya J. Med. Sci. 2022, 84, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Sioutos, N.; Coronado, S.d.; Haber, M.W.; Hartel, F.W.; Shaiu, W.-L.; Wright, L.W. NCI Thesaurus: A semantic model integrating cancer-related clinical and molecular information. J. Biomed. Inform. 2007, 40, 30–43. [Google Scholar] [CrossRef] [PubMed]
- de Coronado, S.; Wright, L.W.; Fragoso, G.; Haber, M.W.; Hahn-Dantona, E.A.; Hartel, F.W.; Quan, S.L.; Safran, T.; Thomas, N.; Whiteman, L. The NCI Thesaurus quality assurance life cycle. J. Biomed. Inform. 2009, 42, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Gipson, D.S.; Kirkendall, E.S.; Gumbs-Petty, B.; Quinn, T.; Steen, A.; Hicks, A.; McMahon, A.; Nicholas, S.; Zhao-Wong, A.; Taylor-Zapata, P.; et al. Development of a Pediatric Adverse Events Terminology. Pediatrics 2017, 139, e20160985. [Google Scholar] [CrossRef] [PubMed]
- Bonhoeffer, J.; Kochhar, S.; Hirschfeld, S.; Heath, P.T.; Jones, C.E.; Bauwens, J.; Honrado, Á.; Heininger, U.; Muñoz, F.M.; Eckert, L.; et al. Global alignment of immunization safety assessment in pregnancy—The GAIA project. Vaccine 2016, 34, 5993–5997. [Google Scholar] [CrossRef] [PubMed]
- Haber, M.W.; Kisler, B.W.; Lenzen, M.; Wright, L.W. Controlled Terminology for Clinical Research: A Collaboration between CDISC and NCI Enterprise Vocabulary Services. Drug Inf. J. 2007, 41, 405–412. [Google Scholar] [CrossRef]
- Robinson, P.N.; Köhler, S.; Bauer, S.; Seelow, D.; Horn, D.; Mundlos, S. The Human Phenotype Ontology: A tool for annotating and analyzing human hereditary disease. Am. J. Hum. Genet. 2008, 83, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Robinson, P.N. Deep phenotyping for precision medicine. Human. Mutat. 2012, 33, 777–780. [Google Scholar] [CrossRef]
- Köhler, S.; Vasilevsky, N.A.; Engelstad, M.; Foster, E.; McMurry, J.; Aymé, S.; Baynam, G.; Bello, S.M.; Boerkoel, C.F.; Boycott, K.M.; et al. The Human Phenotype Ontology in 2017. Nucleic Acids Res 2017, 45, D865–D876. [Google Scholar] [CrossRef] [PubMed]
- Ladewig, M.S.; Jacobsen, J.O.B.; Wagner, A.H.; Danis, D.; El Kassaby, B.; Gargano, M.; Groza, T.; Baudis, M.; Steinhaus, R.; Seelow, D.; et al. GA4GH Phenopackets: A Practical Introduction. Adv. Genet. 2022, 4, 2200016. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, J.O.B.; Baudis, M.; Baynam, G.S.; Beckmann, J.S.; Beltran, S.; Buske, O.J.; Callahan, T.J.; Chute, C.G.; Courtot, M.; Danis, D.; et al. The GA4GH Phenopacket schema defines a computable representation of clinical data. Nat. Biotechnol. 2022, 40, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Aymé, S.; Bellet, B.; Rath, A. Rare diseases in ICD11: Making rare diseases visible in health information systems through appropriate coding. Orphanet J. Rare Dis. 2015, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.; Palmeri, A.; Lee, J.; Hedley, V.; Thuet, J.; Lignon, P.; Cotonnec, V.; Leary, R.; Nally, S.; Straub, V. Understanding paediatric data standards challenges through academia-industry partnerships: A conect4children (c4c) qualitative study. Int. J. Health Plan. Manag. 2022, 38, 416–429. [Google Scholar] [CrossRef] [PubMed]
- Aurich, B.; Apele-Freimane, D.; Banaschewski, T.; Chouchana, L.; Day, S.; Kaguelidou, F.; Kelly, L.E.; Kindblom, J.M.; Neubert, A.; Wong, I.C.K. c4c: Paediatric pharmacovigilance: Methodological considerations in research and development of medicines for children—A c4c expert group white paper. Br. J. Clin. Pharmacol. 2021, 88, 4997–5016. [Google Scholar] [CrossRef] [PubMed]
- Picoraro, J.A.; Lee, D.; Heller, C.A.; Weaver, A.; Hyams, J.S.; Conklin, L.S.; Otley, A.; Ziring, D.; Kugathasan, S.; Rosh, J.R.; et al. Pediatric Inflammatory Bowel Disease Clinical Innovations Meeting of the Crohn’s & Colitis Foundation: Charting the Future of Pediatric IBD. Inflamm. Bowel Dis. 2019, 25, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Palmeri, A.; Leary, R.; Sen, A.; Cornet, R.; Welter, D.; Rocca-Serra, P. Creating a metadata profile for clinical trial protocols. In FAIR Cookbook; Elixer: Cambridgeshire, UK, 2023. [Google Scholar] [CrossRef]
- Pistoia Alliance. Applying the FAIR Data Principles to Paediatric Clinical Trials—Lessons learned and Progress Under the Conect4children Initiative. Available online: https://www.pistoiaalliance.org/pistoia-webinars/paediatric-clinical-trials/ (accessed on 1 June 2023).
- Spence, O.M.; Onwuchekwa Uba, R.; Shin, S.; Doshi, P. Patient consent to publication and data sharing in industry and NIH-funded clinical trials. Trials 2018, 19, 269. [Google Scholar] [CrossRef] [PubMed]
- Lundqvist, B. Data Collaboration, Pooling and Hoarding under Competition Law; Faculty of Law, Stockholm University Research Paper; Stockholm University: Stockholm, Sweden, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Initiative | Resource | Description |
|---|---|---|
| ERNs | Registries | 24 pseudo-anonymised registries with patient-level data, each tackling a different therapeutic area |
| Data dictionaries including Common Data Elements (CDE) | Can contain thousands of elements related to the registry including 16 mandatory CDE | |
| EJPRD | Single-point access Virtual Platform | Single access point for registries, repositories, libraries, biobanks, and analysis platforms related to rare disease |
| Innovation Management Toolbox | Library of self-help resources in rare disease translational medicine | |
| Pistoia Alliance | FAIR Toolkit | Highlights methods and use cases of FAIR implementation in industry |
| FAIR4clin guide | FAIR guiding principles for clinical trial and real-world data |
| Resource 1 | Resource 2 (and Higher) | Collaborating on |
|---|---|---|
| NCI-EVS | CDISC | General partnership |
| C-Path | NORD | Jointly working on RDCA-DAP |
| CDISC | NORD | Rare disease TAUG |
| C-Path | CDISC, OMOP | C-Path using CDISC and OMOP standards for its datasets |
| CDISC | OMOP, FHIR | Guidelines on conversions between CDISC, OMOP and FHIR |
| EJP RD | OMOP, ERNs | Mapping between OMOP and CDEs (introduced by ERNs) |
| EJP RD | C-Path, ERNs | Aligning ontologies that are being developed by the ERNs |
| ERNs | EJP RD | FAIRification of data |
| ErkNet (an ERN) | Orphacodes, HPO | ERkNet using Orphacodes for diagnoses and HPO for phenotypes |
| MetabERN, ErkNet (ERNs) | U-IMD | ErkNet and MetabERN contributing to U-IMD standards |
| Phenopackets | OMOP, FHIR | OMOP and FHIR implementations for phenopackets |
| Pharmaceutical companies | CDISC | Regular correspondence when companies encounter non-CDISC data in their studies |
| Action Item | Current Status | |
|---|---|---|
| 1 | Establishment of multi-stakeholder multi-project user group |
|
| 2 | Use the FAIR4Clin guide for the FAIRification of metadata |
|
| 3 | Phenopackets pilot |
|
| 4 | Orphacodes in CRFs |
|
| 5 | Educating ERNs about CDISC standards |
|
| 6 | Applications of the Paediatric Use Guide |
|
| 7 | Workshops and educational material |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sen, A.; Hedley, V.; Degraeuwe, E.; Hirschfeld, S.; Cornet, R.; Walls, R.; Owen, J.; Robinson, P.N.; Neilan, E.G.; Liener, T.; et al. Learning from conect4children: A Collaborative Approach towards Standardisation of Disease-Specific Paediatric Research Data. Data 2024, 9, 55. https://doi.org/10.3390/data9040055
Sen A, Hedley V, Degraeuwe E, Hirschfeld S, Cornet R, Walls R, Owen J, Robinson PN, Neilan EG, Liener T, et al. Learning from conect4children: A Collaborative Approach towards Standardisation of Disease-Specific Paediatric Research Data. Data. 2024; 9(4):55. https://doi.org/10.3390/data9040055
Chicago/Turabian StyleSen, Anando, Victoria Hedley, Eva Degraeuwe, Steven Hirschfeld, Ronald Cornet, Ramona Walls, John Owen, Peter N. Robinson, Edward G. Neilan, Thomas Liener, and et al. 2024. "Learning from conect4children: A Collaborative Approach towards Standardisation of Disease-Specific Paediatric Research Data" Data 9, no. 4: 55. https://doi.org/10.3390/data9040055