
Diagnostic Imaging of Diseases Affecting the Guttural Pouch

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Use and Interest of the Different Imaging Techniques for Assessing the Guttural Pouches and Associated Structures
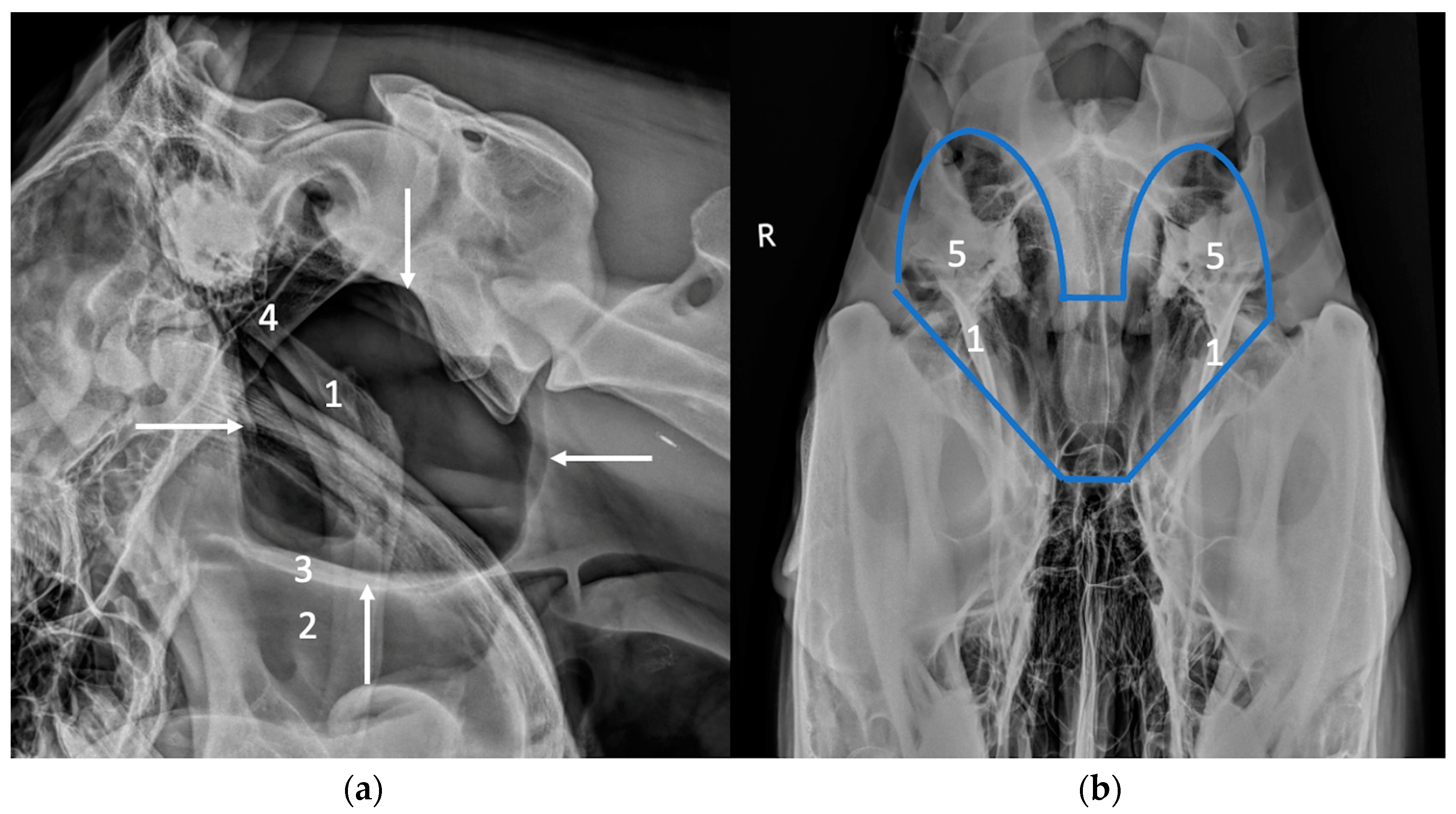
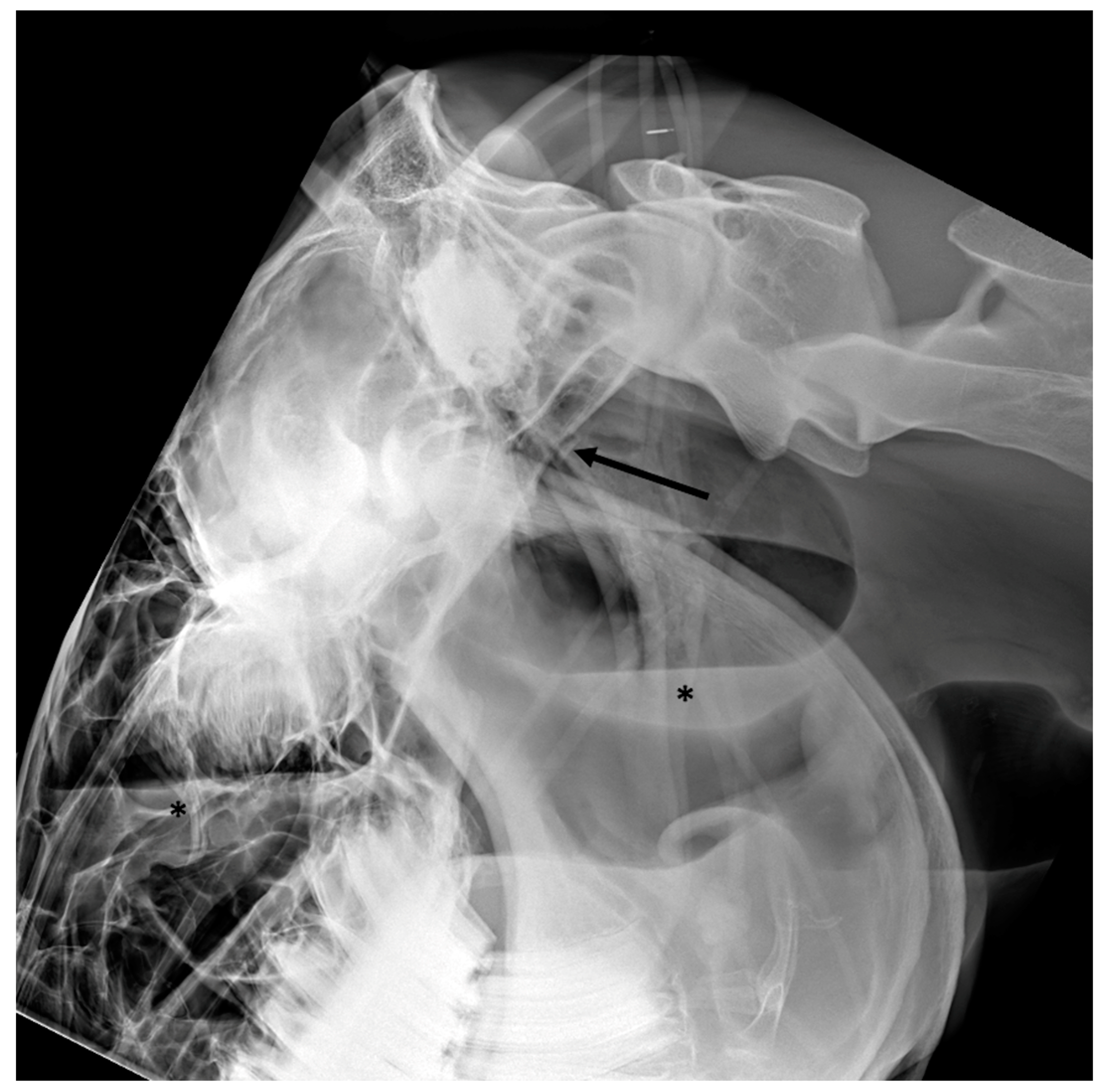
2.1. Radiography
2.2. Ultrasound
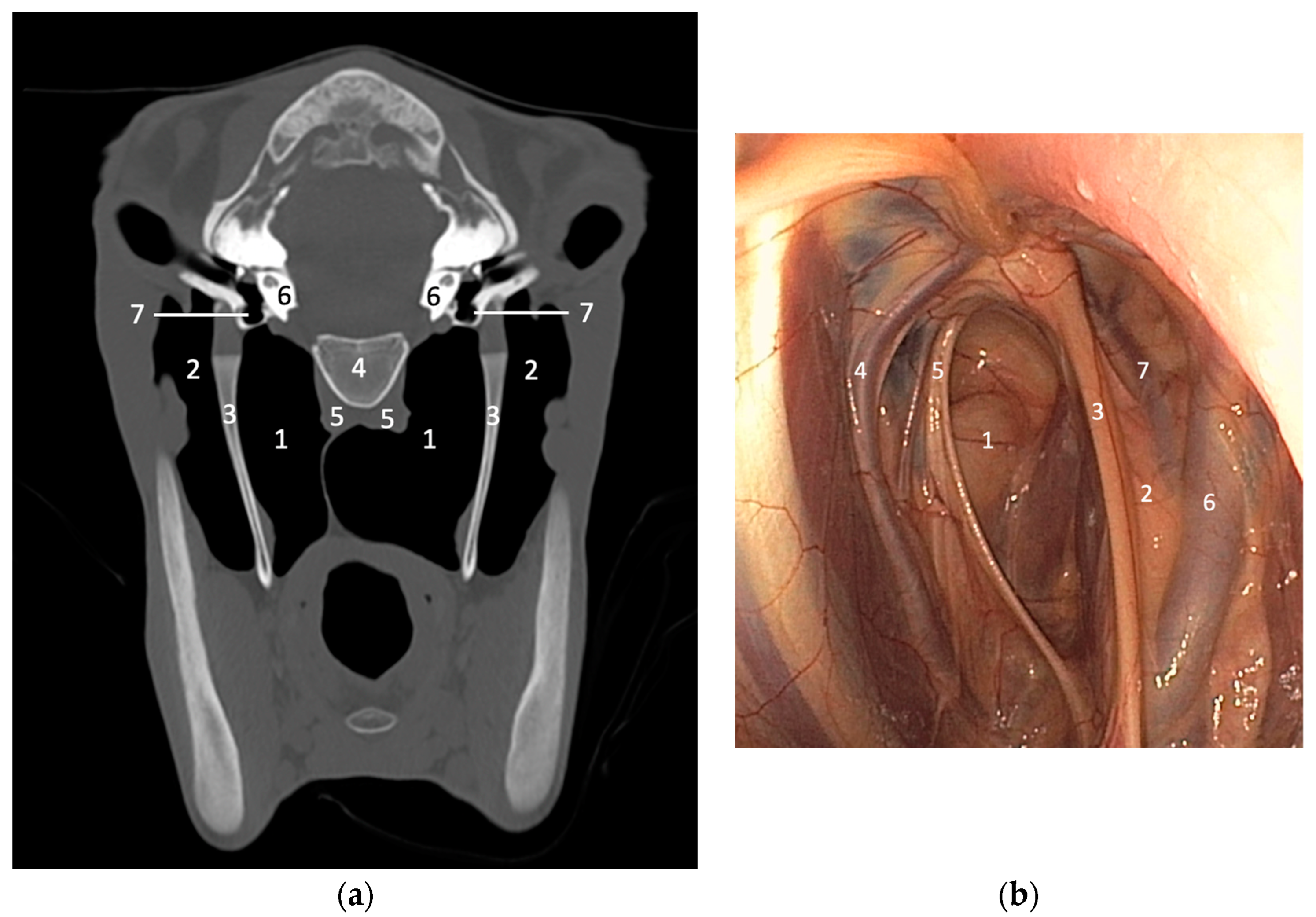
2.3. Cross-Sectional Imaging
3. Imaging Features of Diseases Affecting the Guttural Pouch
3.1. Guttural Pouch Empyema
3.2. Guttural Pouch Tympany
3.3. Guttural Pouch Hemorrhage
3.4. Temporohyoid Osteoarthropathy
3.5. Masses Involving the Guttural Pouches
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Budras, K.; Sack, W.O.; Röck, S. The head. In Anatomy of the Horse, 5th ed.; Schlütersche: Hannover, Germany, 2009; pp. 32–52. [Google Scholar]
- Borges, A.S.; Watanabe, M.J. Guttural pouch disease causing neurologic dysfunction in the horse. Vet. Clin. Equine 2011, 27, 545–572. [Google Scholar] [CrossRef] [PubMed]
- Hardy, J.; Léveillé, R. Diseases of the guttural pouches. Vet. Clin. Equine 2003, 19, 123–158. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.E. Update on disorders and treatment of the guttural pouch. Vet. Clin. Equine 2015, 31, 63–89. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.A.; Colles, C.M.; Dyson, S.J.; Kold, S.E.; Poulos, P.W. The head. In Clinical Radiology of the Horse, 4th ed.; John Wiley and Son: Chichester, UK, 2017; pp. 32–52. [Google Scholar]
- Barakzai, S.Z.; Weaver, M.P. Imaging the equine temporohyoid region. Equine Vet. Educ. 2010, 17, 14–15. [Google Scholar] [CrossRef]
- Ségard-Weisse, E.; Thomas-Cancian, A.; Zimmerman, M.; Cadoré, J.L. L’imagerie des poches gutturales chez le cheval. Prat. Vétérinaire Équine 2019, 19, 66–77. [Google Scholar]
- Porter, E.G.; Werpy, N.M. New concepts in standing advanced diagnostic equine imaging. Vet. Clin. Equine 2014, 30, 239–268. [Google Scholar] [CrossRef] [PubMed]
- Koch, C.; Witte, T. Temporohyoid osteoarthropathy in the horse. Equine. Vet. Educ. 2014, 26, 121–125. [Google Scholar] [CrossRef]
- Dias, D.P.M.; Macoris, D.G.; Alessi, A.C. Guttural pouch empyema secondary to a periocular foreign body. Equine. Vet. Educ. 2016, 28, 367–371. [Google Scholar] [CrossRef]
- Cook, W.R. The auditory tube diverticulum (guttural pouch) in the horse: Its radiographic examination. Vet. Radiol. 1973, 14, 51–71. [Google Scholar] [CrossRef]
- Gillen, A.; Cuming, R.; Schumacher, J.; Taylor, D.; Munsterman, A. Guttural pouch perforation caused during nasogastric intubation. Equine. Vet. Educ. 2015, 28, 398–402. [Google Scholar] [CrossRef]
- Baptiste, K.E.; David Moll, H.; Robertson, J.L. Three horses with neoplasia including growth in the guttural pouch. Can. Vet. J. 1996, 37, 499–501. [Google Scholar] [PubMed]
- Ramirez, O.; Jorgensen, J.S.; Thrall, D.E. Imaging basilar skull fractures in the horse: A review. Vet. Radiol. Ultrasound 1998, 39, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Becatti, F.; Angeli, G.; Secco, I.; Contini, A.; Gialetti, R.; Pepe, M. Communited basilar skull fracture in a colt: Use of computed tomography to aid the diagnosis. Equine Vet. Educ. 2011, 23, 327–332. [Google Scholar] [CrossRef]
- Vitale, V.; Gascon, E.; Corradini, I.; Armengou, L.; José-Cunilleras, E. Basisphenoid bone fracture in two juvenile horses with different clinical presentation. Vet. Rec. Case Rep. 2021, 9, e141. [Google Scholar] [CrossRef]
- Walker, A.M.; Sellon, D.C.; Cornelisse, C.J.; Hines, M.T.; Ragle, C.A.; Cohen, N.; Schott, H.C., II. Temporohyoid osteoarthropathy in 33 horses (1993–2000). J. Vet. Intern. Med. 2002, 16, 697–703. [Google Scholar] [PubMed]
- Hilton, H.; Puchalski, S.M.; Aleman, M. The computed tomographic appearance of equine temporohyoid osteoarthropathy. Vet. Radiol. Ultrasound 2009, 50, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Pownder, S.; Scrivani, P.V.; Bezuidenhout, A.; Divers, T.J.; Ducharme, N.G. Computed tomography of temporal bone fractures and temporal region anatomy in horses. J. Vet. Intern. Med. 2010, 24, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J.; Spriet, M.; Espinosa-Mur, P.; Estell, K.E.; Aleman, M. The prevalence of temporal bone fractures is high in horses with severe temporohyoid osteoarthropathy. Vet. Radiol. Ultrasound 2019, 60, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Drew, S.J.; Meehan, L.; Reardon, J.M.; McGorum, B.C.; Dixon, P.M.; Del Pozo, J. Guttural pouch leiomyosarcoma causing nasopharyngeal compression in a pony. Equine. Vet. Educ. 2018, 30, 64–69. [Google Scholar] [CrossRef]
- Shell, K.; Rijkenhuizen, A. Extensive and invasive guttural pouch granuloma in a 2-year-old gelding. Equine Vet. Educ. 2020, 32, 289–293. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas-Cancian, A.; Ségard-Weisse, E.; Drumond, B.; Cadoré, J.-L. Diagnostic Imaging of Diseases Affecting the Guttural Pouch. Vet. Sci. 2023, 10, 525. https://doi.org/10.3390/vetsci10080525
Thomas-Cancian A, Ségard-Weisse E, Drumond B, Cadoré J-L. Diagnostic Imaging of Diseases Affecting the Guttural Pouch. Veterinary Sciences. 2023; 10(8):525. https://doi.org/10.3390/vetsci10080525
Chicago/Turabian StyleThomas-Cancian, Aurélie, Emilie Ségard-Weisse, Bianca Drumond, and Jean-Luc Cadoré. 2023. "Diagnostic Imaging of Diseases Affecting the Guttural Pouch" Veterinary Sciences 10, no. 8: 525. https://doi.org/10.3390/vetsci10080525
APA StyleThomas-Cancian, A., Ségard-Weisse, E., Drumond, B., & Cadoré, J.-L. (2023). Diagnostic Imaging of Diseases Affecting the Guttural Pouch. Veterinary Sciences, 10(8), 525. https://doi.org/10.3390/vetsci10080525