Author Contributions
Conceptualization, A.T.-C. and E.S.-W.; methodology, A.T.-C. and B.D.; validation, A.T.-C., E.S.-W., B.D. and J.-L.C.; investigation, A.T.-C. and E.S.-W.; resources, A.T.-C., E.S.-W. and B.D.; writing—original draft preparation, A.T.-C.; writing—review and editing, A.T.-C., E.S.-W., B.D. and J.-L.C.; visualization, A.T.-C.; supervision, A.T.-C., E.S.-W., B.D. and J.-L.C.; project administration, A.T.-C.; All authors have read and agreed to the published version of the manuscript.
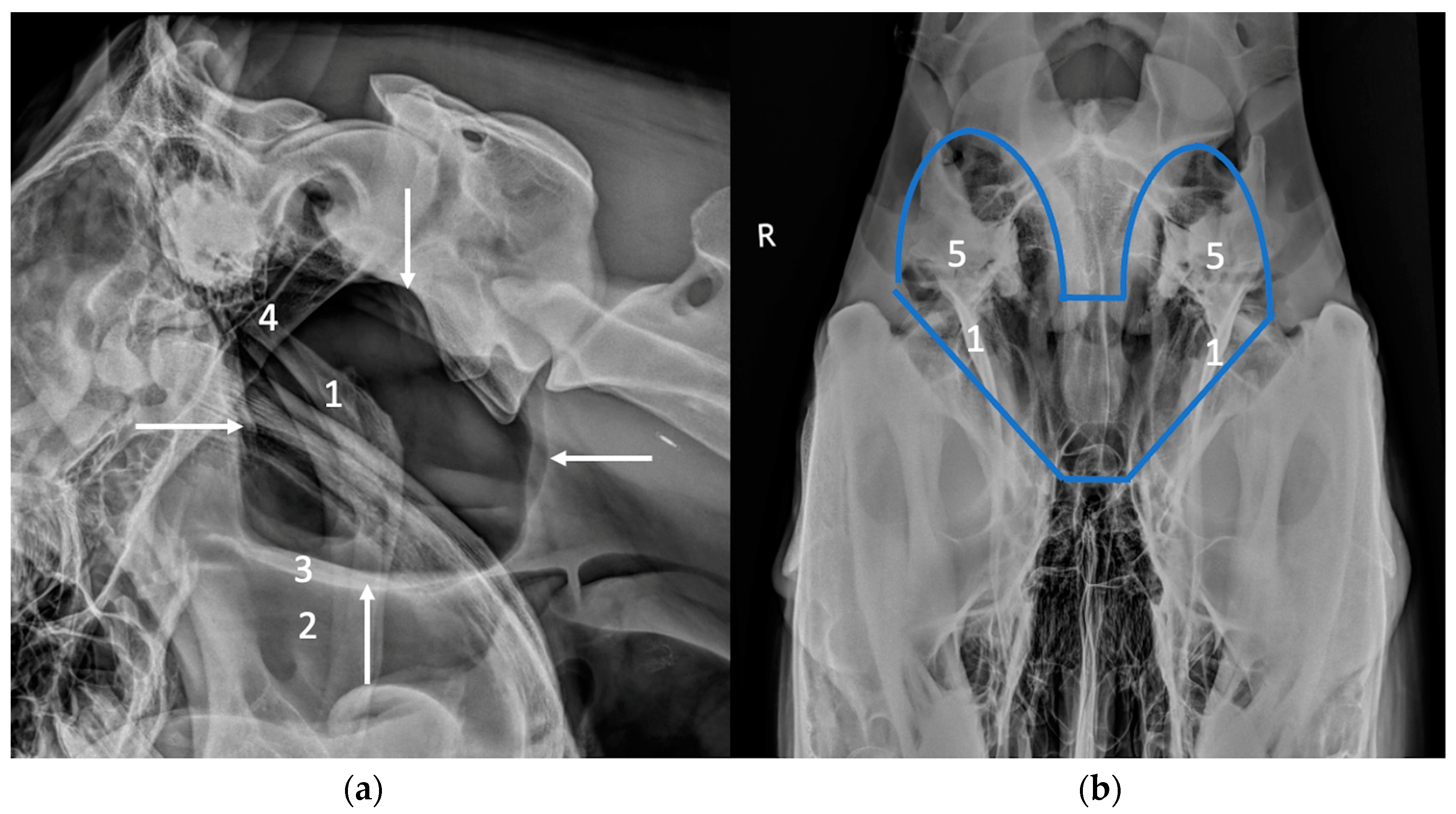
Figure 1.
Latero-lateral (a) and ventro-dorsal views (b) illustrating the normal radiographic appearance of the guttural pouches, delineated by white arrows in (a) and by a blue line in (b). The guttural pouches are less visible in the ventro-dorsal view due to surperimposition with several bony structures. (1) Stylohyoid bones, (2) pharynx, (3) pharyngeal roof, (4) basioccipital and basisphenoid bones, (5) petrous part of the temporal bone.
Figure 1.
Latero-lateral (a) and ventro-dorsal views (b) illustrating the normal radiographic appearance of the guttural pouches, delineated by white arrows in (a) and by a blue line in (b). The guttural pouches are less visible in the ventro-dorsal view due to surperimposition with several bony structures. (1) Stylohyoid bones, (2) pharynx, (3) pharyngeal roof, (4) basioccipital and basisphenoid bones, (5) petrous part of the temporal bone.
Figure 2.
Transverse ultrasonographic images (Aloka Alpha 7, microconvex probe 5–10 MHz) of the area of Viborg’s triangle caudal to the vertical ramus of the mandible. Cranial is to the left. (1) Caudal border of the mandible, (2) parotid gland, (3) external carotid artery, (4) lateral recess of the guttural pouch, (5) dorsal extremity of the stylohyoid bone, (6) medial recess of the guttural pouch, (7) muscles lying lateral to the guttural pouch (digastric and occipitohyoid muscles).
Figure 2.
Transverse ultrasonographic images (Aloka Alpha 7, microconvex probe 5–10 MHz) of the area of Viborg’s triangle caudal to the vertical ramus of the mandible. Cranial is to the left. (1) Caudal border of the mandible, (2) parotid gland, (3) external carotid artery, (4) lateral recess of the guttural pouch, (5) dorsal extremity of the stylohyoid bone, (6) medial recess of the guttural pouch, (7) muscles lying lateral to the guttural pouch (digastric and occipitohyoid muscles).
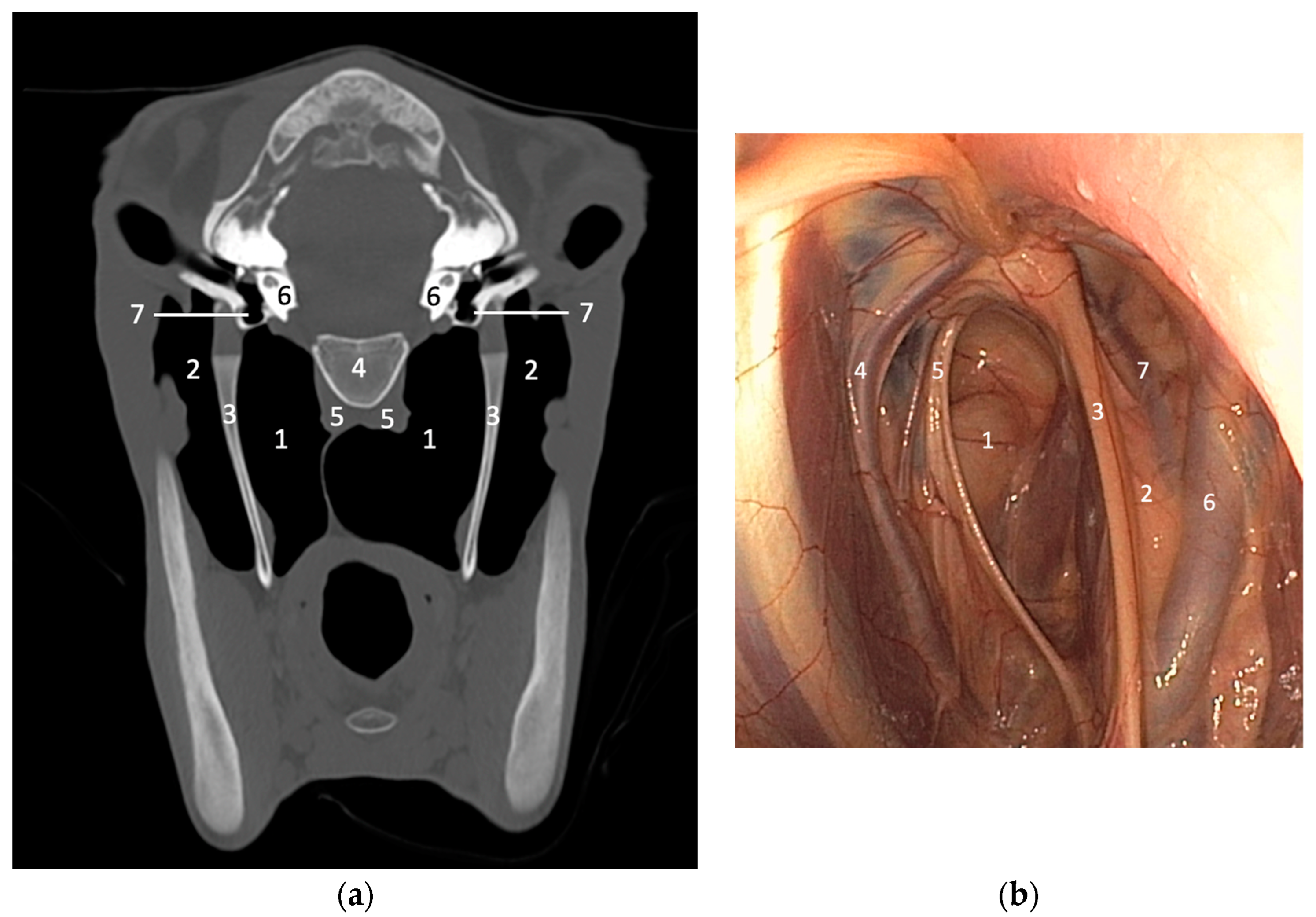
Figure 3.
(a) CT transverse image (bone window) of a normal young horse at the level of the inner ear. Right is to the left. The guttural pouches and related structures can be clearly identified and evaluated without superimposition. (1) Medial compartment of the guttural pouch, (2) lateral compartment of the guttural pouch, (3) stylohyoid bone, (4) basioccipital bone, (5) rectus capitis and longus capitis muscles, (6) petrous part of the temporal bone, (7) tympanic bullae. Image courtesy of Dr Mickaël Robert. (b) Endoscopy of the guttural pouch of a normal horse for comparison (medial is to the left). The inside of the guttural pouch can be observed directly but the evaluation of some related structures remains incomplete compared to CT. (1) Medial compartment of the guttural pouch, (2) lateral compartment of the guttural pouch, (3) stylohyoid bone, (4) external carotid artery, (5) cranial nerves IX, X, XI and XII, (6) maxillary artery, (7) internal carotid artery.
Figure 3.
(a) CT transverse image (bone window) of a normal young horse at the level of the inner ear. Right is to the left. The guttural pouches and related structures can be clearly identified and evaluated without superimposition. (1) Medial compartment of the guttural pouch, (2) lateral compartment of the guttural pouch, (3) stylohyoid bone, (4) basioccipital bone, (5) rectus capitis and longus capitis muscles, (6) petrous part of the temporal bone, (7) tympanic bullae. Image courtesy of Dr Mickaël Robert. (b) Endoscopy of the guttural pouch of a normal horse for comparison (medial is to the left). The inside of the guttural pouch can be observed directly but the evaluation of some related structures remains incomplete compared to CT. (1) Medial compartment of the guttural pouch, (2) lateral compartment of the guttural pouch, (3) stylohyoid bone, (4) external carotid artery, (5) cranial nerves IX, X, XI and XII, (6) maxillary artery, (7) internal carotid artery.
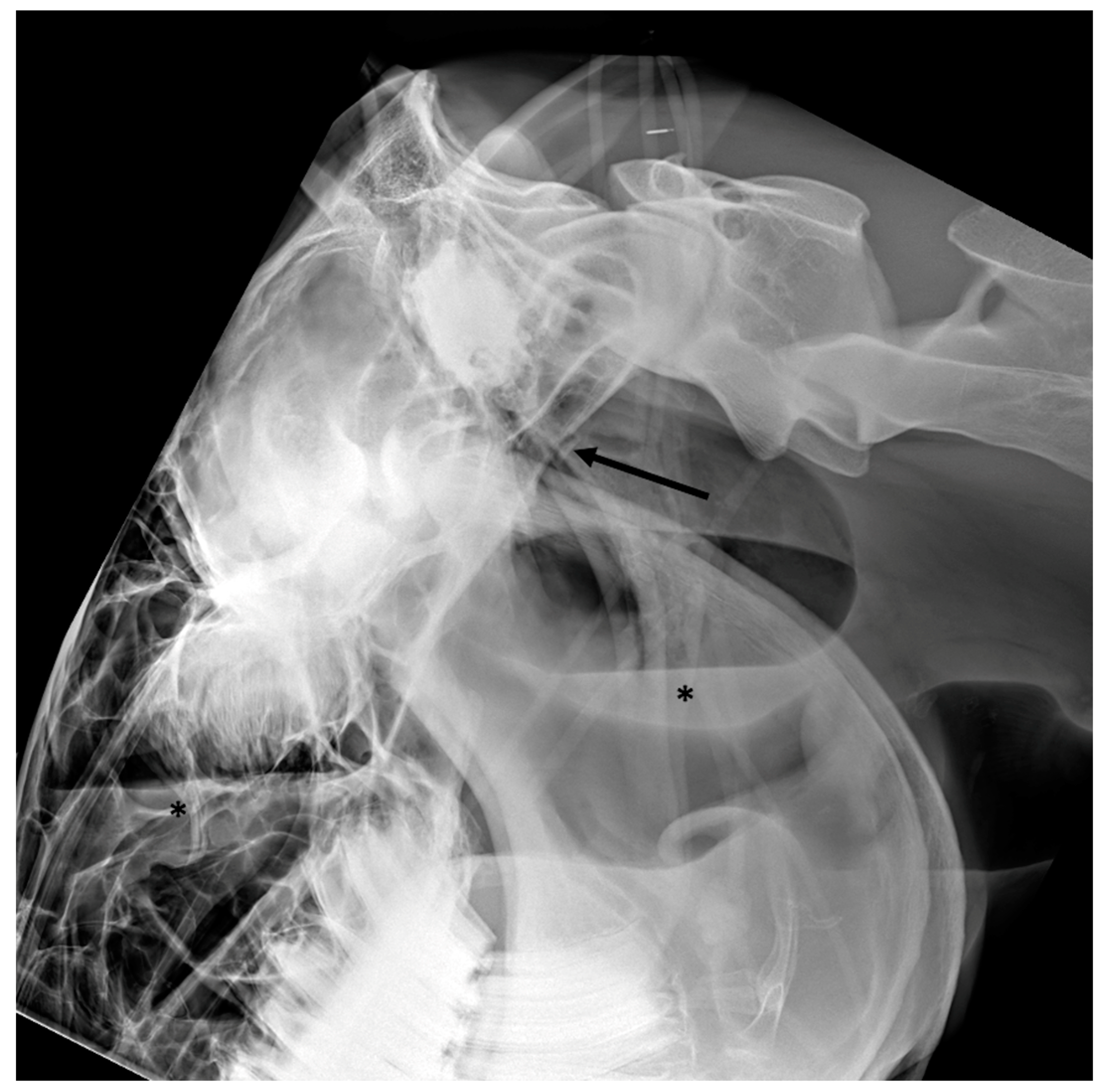
Figure 4.
Latero-lateral views of three different horses with guttural pouch empyema illustrating the variable appearance and quantity of the material filling the guttural pouch. In (a), only a small amount of homogeneous fluid delineated dorsally by a gas/fluid interface (black asterisk) is visible in the ventral part of the guttural pouch. In (b), the pus is thicker with a convex dorsal border (white arrows) and almost completely fills the guttural pouch. In (c), the guttural pouch is completely filled with heterogenous thick pus with a mottled appearance (white asterisk), creating a mass effect. In (b,c) the roof of the pharynx is displaced by the filled guttural pouch (black arrows), inducing a reduction of the lumen of the pharynx and the larynx, causing respiratory distress.
Figure 4.
Latero-lateral views of three different horses with guttural pouch empyema illustrating the variable appearance and quantity of the material filling the guttural pouch. In (a), only a small amount of homogeneous fluid delineated dorsally by a gas/fluid interface (black asterisk) is visible in the ventral part of the guttural pouch. In (b), the pus is thicker with a convex dorsal border (white arrows) and almost completely fills the guttural pouch. In (c), the guttural pouch is completely filled with heterogenous thick pus with a mottled appearance (white asterisk), creating a mass effect. In (b,c) the roof of the pharynx is displaced by the filled guttural pouch (black arrows), inducing a reduction of the lumen of the pharynx and the larynx, causing respiratory distress.
Figure 5.
Latero-lateral view of a horse with chronic guttural pouch empyema. Several radio-opaque nodules of various size (black asterisks) are filling the guttural pouch, creating a mass effect displacing the roof of the pharynx ventrally (black arrows). A metal opaque coil can be observed along the cranial border of the guttural pouch secondary to a previous surgical embolization of the internal carotid artery.
Figure 5.
Latero-lateral view of a horse with chronic guttural pouch empyema. Several radio-opaque nodules of various size (black asterisks) are filling the guttural pouch, creating a mass effect displacing the roof of the pharynx ventrally (black arrows). A metal opaque coil can be observed along the cranial border of the guttural pouch secondary to a previous surgical embolization of the internal carotid artery.
Figure 6.
Latero-lateral view of a horse with guttural pouch empyema and severe retropharyngeal abscessation. Note the severe mass effect caused by the severely enlarged retropharyngeal lymph nodes (black asterisk), displacing the caudal border of the guttural pouch and the roof of the pharynx (black arrows).
Figure 6.
Latero-lateral view of a horse with guttural pouch empyema and severe retropharyngeal abscessation. Note the severe mass effect caused by the severely enlarged retropharyngeal lymph nodes (black asterisk), displacing the caudal border of the guttural pouch and the roof of the pharynx (black arrows).
Figure 7.
Transverse ultrasonographic image (Aloka Alpha 7, microconvex probe 5–10 MHz) of the pharyngeal area of a horse with guttural pouch empyema showing the guttural pouch markedly dilated and filled with heterogenous hypoechoic fluid. Cranial is to the left.
Figure 7.
Transverse ultrasonographic image (Aloka Alpha 7, microconvex probe 5–10 MHz) of the pharyngeal area of a horse with guttural pouch empyema showing the guttural pouch markedly dilated and filled with heterogenous hypoechoic fluid. Cranial is to the left.
Figure 8.
Latero-lateral view of a foal with guttural pouch tympany. The guttural pouch is markedly distended with its caudal border extending caudally up to the level of the caudal endplate of the axis (black arrow). The ventral border of the guttural pouch is displaced ventrally (black asterisks), compressing the airways.
Figure 8.
Latero-lateral view of a foal with guttural pouch tympany. The guttural pouch is markedly distended with its caudal border extending caudally up to the level of the caudal endplate of the axis (black arrow). The ventral border of the guttural pouch is displaced ventrally (black asterisks), compressing the airways.
Figure 9.
Postoperative latero-lateral (a) and ventro-dorsal (b) views of a horse after surgical embolization of the internal and external carotid arteries to treat a right-sided guttural pouch mycosis. The position of the metallic coils can be easily identified in the two radiographic views (white arrows).
Figure 9.
Postoperative latero-lateral (a) and ventro-dorsal (b) views of a horse after surgical embolization of the internal and external carotid arteries to treat a right-sided guttural pouch mycosis. The position of the metallic coils can be easily identified in the two radiographic views (white arrows).
Figure 10.
Latero-lateral view of a horse with basilar skull trauma. A bony fragment (black arrow) can be observed caudal to a defect in the basioccipital bone. There is increased and slightly heterogeneous opacity of the longus capitis and rectus capitis muscles. The associated guttural pouch hemorrhage is characterized by homogeneous increased opacity in the ventral part of the guttural pouch (black asterisk) delineated dorsally by a gas/fluid interface. The roof of the pharynx is displaced ventrally.
Figure 10.
Latero-lateral view of a horse with basilar skull trauma. A bony fragment (black arrow) can be observed caudal to a defect in the basioccipital bone. There is increased and slightly heterogeneous opacity of the longus capitis and rectus capitis muscles. The associated guttural pouch hemorrhage is characterized by homogeneous increased opacity in the ventral part of the guttural pouch (black asterisk) delineated dorsally by a gas/fluid interface. The roof of the pharynx is displaced ventrally.
Figure 11.
Transverse (a,b) and sagittal (c) CT images (bone window) of a pony with temporohyoid osteoarthropathy. Right is to the left. New bone formation and ankylosis can be observed at the level of the left temporohyoid joint associated with severe thickening of the left stylohyoid bone (white arrows). Several associated fracture lines are present through the left temporal bone (black arrows). Images courtesy of Dr Mickaël Robert.
Figure 11.
Transverse (a,b) and sagittal (c) CT images (bone window) of a pony with temporohyoid osteoarthropathy. Right is to the left. New bone formation and ankylosis can be observed at the level of the left temporohyoid joint associated with severe thickening of the left stylohyoid bone (white arrows). Several associated fracture lines are present through the left temporal bone (black arrows). Images courtesy of Dr Mickaël Robert.
Figure 12.
Transverse CT images (bone window (a) and soft tissue window (b)) of a horse with a squamous cell carcinoma of the right guttural pouch. Right is to the left. A large soft tissue attenuating mass is filling the medial compartment of the right guttural pouch (white arrows) and there is extensive associated lysis of the right tympanic bulla (black asterisk). CT allows a clear understanding of the location and margins of the mass, degree of involvement of the guttural pouch and any associated bony changes. Images courtesy of Dr Mickaël Robert.
Figure 12.
Transverse CT images (bone window (a) and soft tissue window (b)) of a horse with a squamous cell carcinoma of the right guttural pouch. Right is to the left. A large soft tissue attenuating mass is filling the medial compartment of the right guttural pouch (white arrows) and there is extensive associated lysis of the right tympanic bulla (black asterisk). CT allows a clear understanding of the location and margins of the mass, degree of involvement of the guttural pouch and any associated bony changes. Images courtesy of Dr Mickaël Robert.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}