
Fusarium, Scedosporium and Other Rare Mold Invasive Infections: Over Twenty-Five-Year Experience of a European Tertiary-Care Center

 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
3. Results
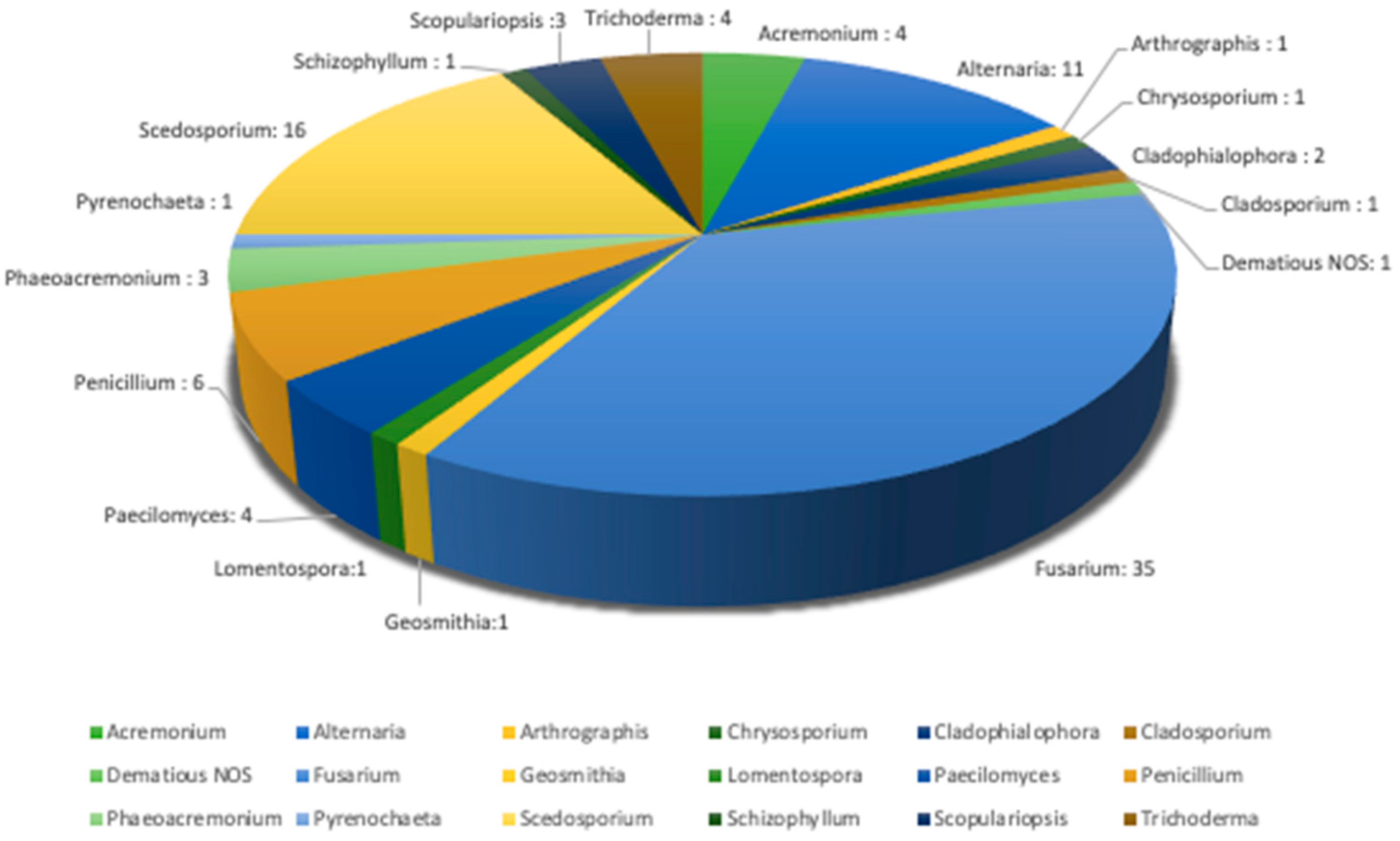
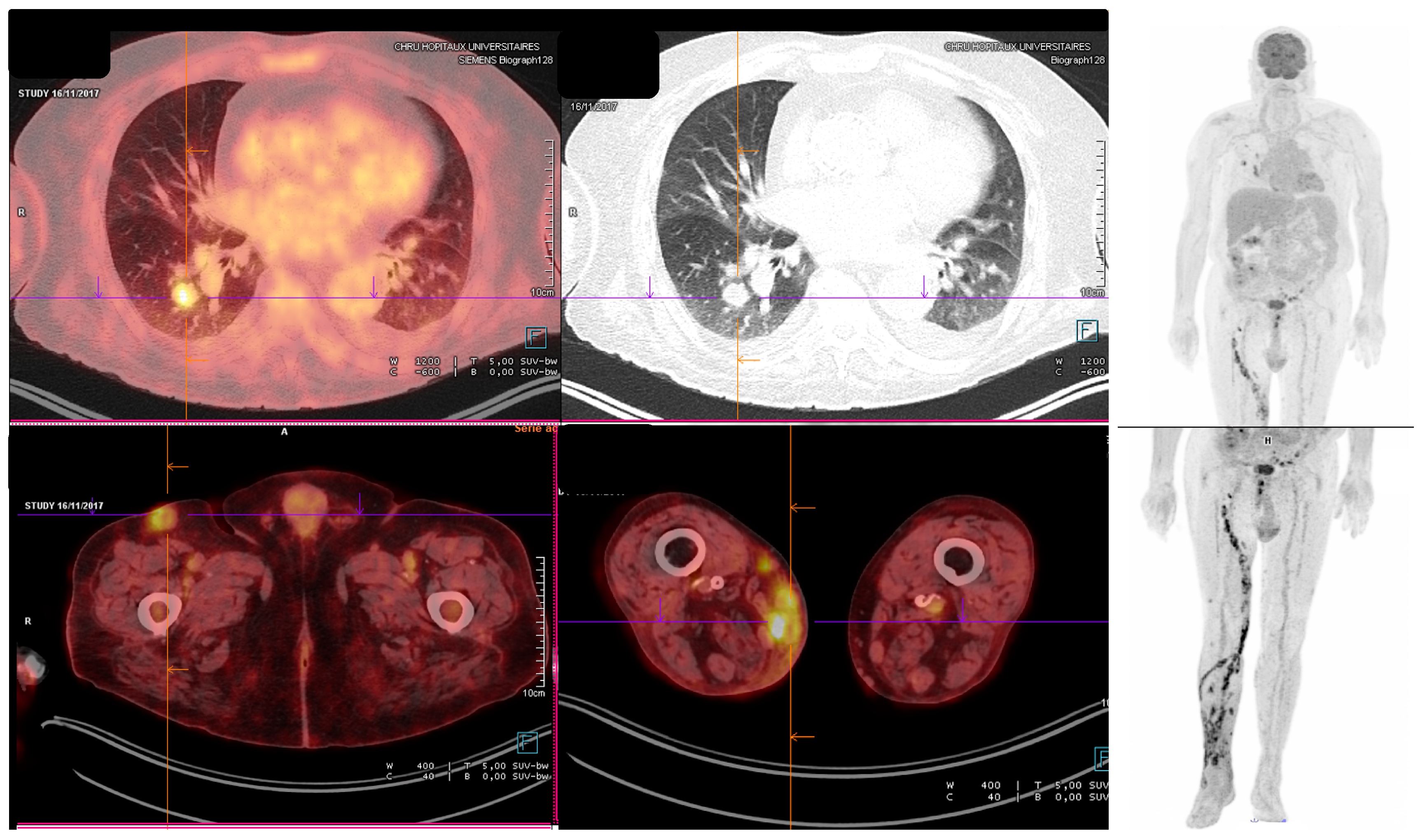
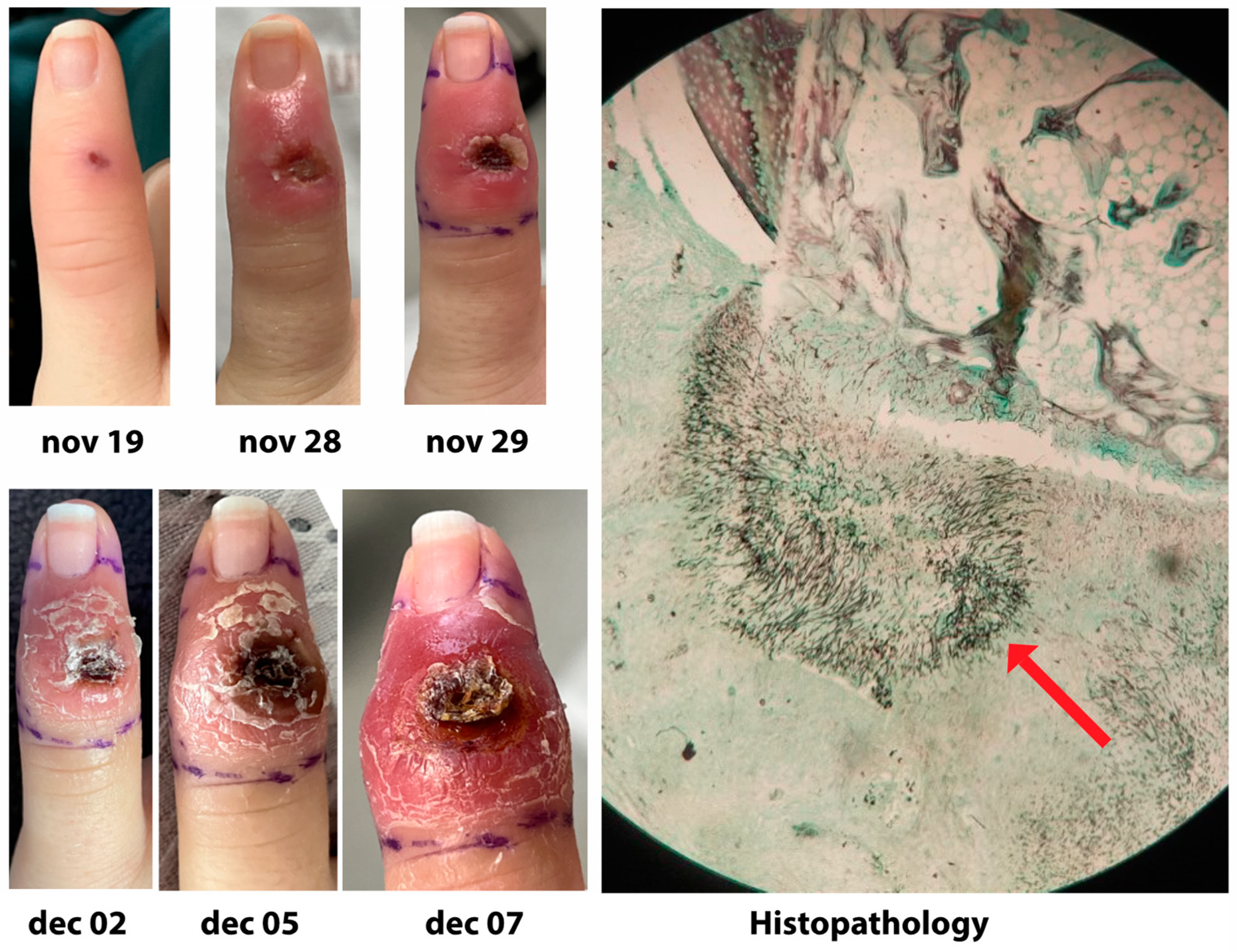
3.1. Fungi and Clinical Presentation
3.2. Biomarkers
3.3. Antifungal Susceptibility
3.4. Treatment
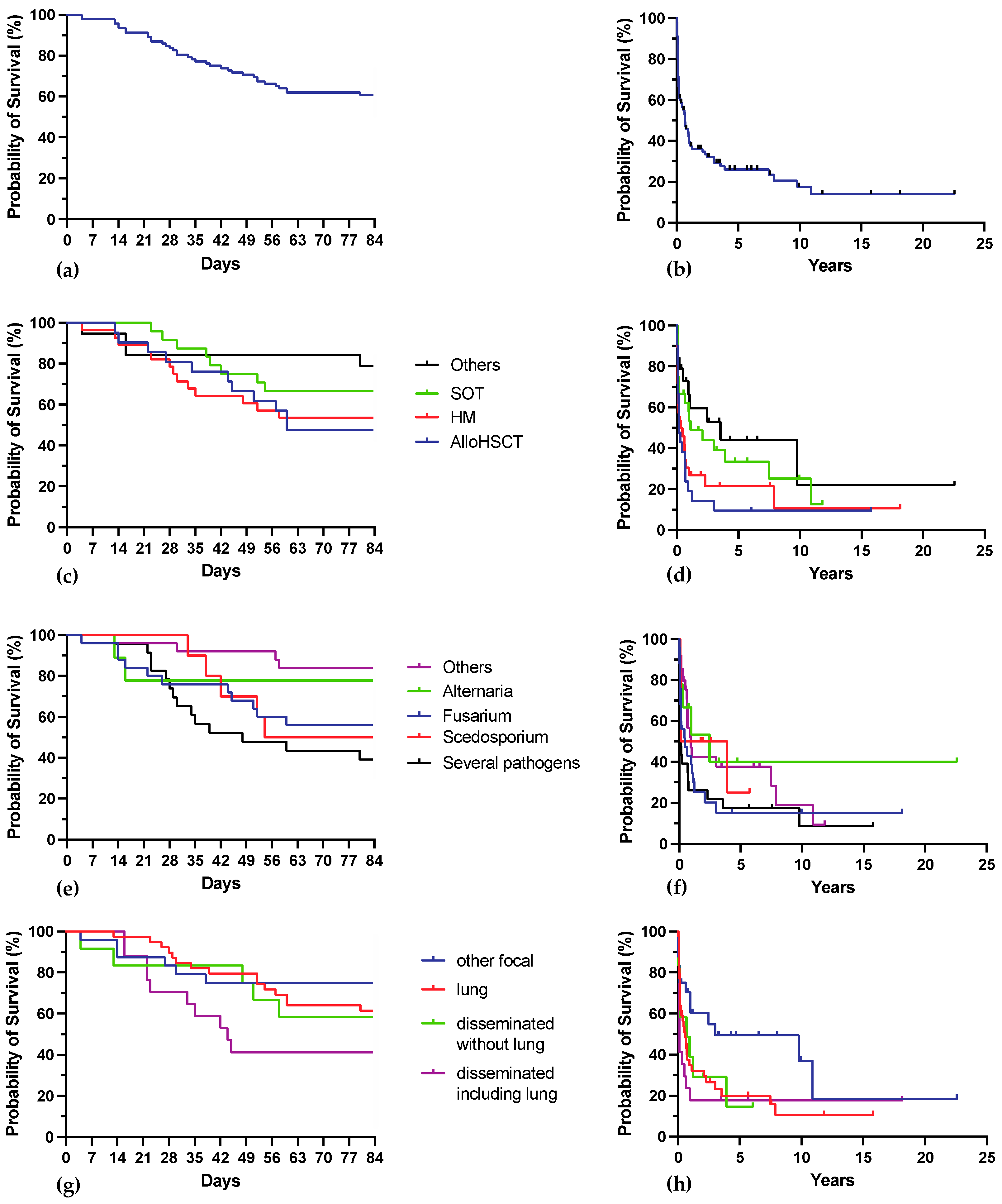
3.5. Outcome
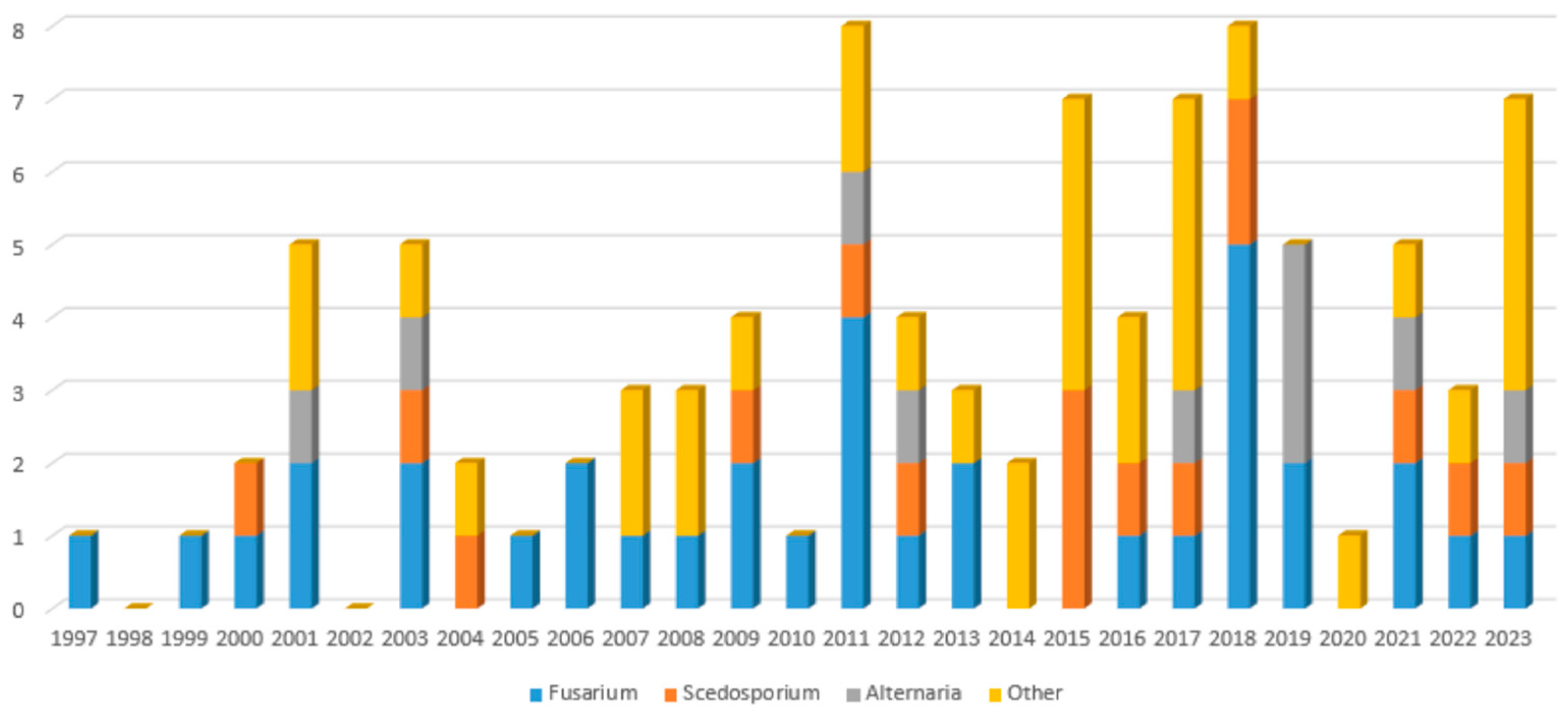
3.6. Trends over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ledoux, M.-P.; Herbrecht, R. Invasive Pulmonary Aspergillosis. J. Fungi 2023, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Lynch, J.P.; Fishbein, M.C.; Clark, N.M. Mucormycosis. Semin. Respir. Crit. Care Med. 2020, 41, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Nucci, M.; Anaissie, E. Fusarium Infections in Immunocompromised Patients. Clin. Microbiol. Rev. 2007, 20, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Seidel, D.; Meißner, A.; Lackner, M.; Piepenbrock, E.; Salmanton-García, J.; Stecher, M.; Mellinghoff, S.; Hamprecht, A.; Graeff, L.D.; Köhler, P.; et al. Prognostic factors in 264 adults with invasive Scedosporium spp. and Lomentospora prolificans infection reported in the literature and FungiScope®. Crit. Rev. Microbiol. 2019, 45, 1–21, Erratum in Crit. Rev. Microbiol. 2019, 45, 238. [Google Scholar] [CrossRef] [PubMed]
- Tyrellis, G.; Siopi, M.; Leventakou, D.; Delides, A.; Maragkoudakis, P.; Korres, G.; Apostolopoulou, C.; Gouloumi, A.-R.; Pappa, V.; Pournaras, S.; et al. Breakthrough Acute Necrotizing Invasive Fungal Rhinosinusitis by Alternariaalternata in a Patient with Acute Lymphoblastic Leukemia on Anidulafungin Therapy and Case-Based Literature Review. J. Fungi 2022, 8, 879. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Meis, J.F.; Guarro, J.; de Hoog, G.S.; Kathuria, S.; Arendrup, M.C.; Arikan-Akdagli, S.; Akova, M.; Boekhout, T.; Caira, M.; et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of systemic phaeohyphomycosis: Diseases caused by black fungi. Clin. Microbiol. Infect. 2014, 20, 47–75. [Google Scholar] [CrossRef] [PubMed]
- Tortorano, A.M.; Richardson, M.; Roilides, E.; van Diepeningen, A.; Caira, M.; Munoz, P.; Johnson, E.; Meletiadis, J.; Pana, Z.-D.; Lackner, M.; et al. ESCMID and ECMM joint guidelines on diagnosis and management of hyalohyphomycosis: Fusarium spp., Scedosporium spp. and others. Clin. Microbiol. Infect. 2014, 20 (Suppl. S3), 27–46. [Google Scholar] [CrossRef]
- Hoenigl, M.; Salmanton-García, J.; Walsh, T.J.; Nucci, M.; Neoh, C.F.; Jenks, J.D.; Lackner, M.; Sprute, R.; Al-Hatmi, A.M.S.; Bassetti, M.; et al. Global guideline for the diagnosis and management of rare mould infections: An initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology and the American Society for Microbiology. Lancet Infect. Dis. 2021, 21, e246–e257, Erratum in Lancet Infect Dis. 2021, 21, e81. [Google Scholar] [CrossRef]
- Groll, A.; Walsh, T. Uncommon opportunistic fungi: New nosocomial threats. Clin. Microbiol. Infect. 2001, 7 (Suppl. S2), 8–24. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.F. Risk stratification for invasive aspergillosis: Early assessment of host susceptibility. Med. Mycol. 2009, 47 (Suppl. S1), S255–S260. [Google Scholar] [CrossRef]
- Schumacher, H.R.; Ginns, D.A.; Warren, W.J. Fungus infection complicating leukemia. Am. J. Med. Sci. 1964, 247, 313–323. [Google Scholar] [CrossRef]
- Jantunen, E.; Ruutu, P.; Niskanen, L.; Volin, L.; Parkkali, T.; Koukila-Kähkölä, P.; Ruutu, T. Incidence and risk factors for invasive fungal infections in allogeneic BMT recipients. Bone Marrow Transplant. 1997, 19, 801–808. [Google Scholar] [CrossRef]
- Neofytos, D.; Horn, D.; Anaissie, E.; Steinbach, W.; Olyaei, A.; Fishman, J.; Pfaller, M.; Chang, C.; Webster, K.; Marr, K. Epidemiology and Outcome of Invasive Fungal Infection in Adult Hematopoietic Stem Cell Transplant Recipients: Analysis of Multicenter Prospective Antifungal Therapy (PATH) Alliance Registry. Clin. Infect. Dis. 2009, 48, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Kontoyiannis, D.P.; Marr, K.A.; Park, B.J.; Alexander, B.D.; Anaissie, E.J.; Walsh, T.J.; Ito, J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; et al. Prospective Surveillance for Invasive Fungal Infections in Hematopoietic Stem Cell Transplant Recipients, 2001–2006: Overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin. Infect. Dis. 2010, 50, 1091–1100. [Google Scholar] [CrossRef]
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Ito, J.; et al. Invasive Fungal Infections among Organ Transplant Recipients: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Pappas, P.G.; Wannemuehler, K.A.; Alexander, B.D.; Anaissie, E.J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; Brumble, L.M.; Freifeld, A.G.; et al. Invasive Non-Aspergillus Mold Infections in Transplant Recipients, United States, 2001–2006. Emerg. Infect. Dis. 2011, 17, 1855–1864. [Google Scholar] [CrossRef]
- McCarty, T.P.; Baddley, J.W.; Walsh, T.J.; Alexander, B.D.; Kontoyiannis, D.P.; Perl, T.M.; Walker, R.; Patterson, T.F.; Schuster, M.G.; Lyon, G.M.; et al. Phaeohyphomycosis in transplant recipients: Results from the Transplant Associated Infection Surveillance Network (TRANSNET). Med. Mycol. 2015, 53, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Varughese, T.; Taur, Y.; Cohen, N.; Palomba, M.L.; Seo, S.K.; Hohl, T.M.; Redelman-Sidi, G. Serious Infections in Patients Receiving Ibrutinib for Treatment of Lymphoid Cancer. Clin. Infect. Dis. 2018, 67, 687–692. [Google Scholar] [CrossRef]
- Infante, M.S.; Fernández-Cruz, A.; Núñez, L.; Carpio, C.; Jiménez-Ubieto, A.; López-Jiménez, J.; Vásquez, L.; Del Campo, R.; Romero, S.; Alonso, C.; et al. Severe infections in patients with lymphoproliferative diseases treated with new targeted drugs: A multicentric real-world study. Cancer Med. 2021, 10, 7629–7640. [Google Scholar] [CrossRef]
- Chamilos, G.; Lionakis, M.S.; Kontoyiannis, D.P. Call for Action: Invasive Fungal Infections Associated with Ibrutinib and Other Small Molecule Kinase Inhibitors Targeting Immune Signaling Pathways. Clin. Infect. Dis. 2018, 66, 140–148. [Google Scholar] [CrossRef]
- Garner, W.; Samanta, P.; Haidar, G. Invasive Fungal Infections after Anti-CD19 Chimeric Antigen Receptor-Modified T-Cell Therapy: State of the Evidence and Future Directions. J. Fungi 2021, 7, 156. [Google Scholar] [CrossRef]
- Garnacho-Montero, J.; Olaechea, P.; Alvarez-Lerma, F.; Alvarez-Rocha, L.; Blanquer, J.; Galván, B.; Rodriguez, A.; Zaragoza, R.; Aguado, J.-M.; Mensa, J.; et al. Epidemiology, diagnosis and treatment of fungal respiratory infections in the critically ill patient. Rev. Esp. Quimioter. 2013, 26, 173–188. [Google Scholar] [PubMed]
- Lamoth, F.; Chung, S.J.; Damonti, L.; Alexander, B.D. Changing Epidemiology of Invasive Mold Infections in Patients Receiving Azole Prophylaxis. Clin. Infect. Dis. 2017, 64, 1619–1621, Erratum in Clin. Infect. Dis. 2009, 48, 690. [Google Scholar] [CrossRef] [PubMed]
- Nucci, M.; Garnica, M.; Gloria, A.B.; Lehugeur, D.S.; Dias, V.; Palma, L.C.; Cappellano, P.; Fertrin, K.Y.; Carlesse, F.; Simões, B.; et al. Invasive fungal diseases in haematopoietic cell transplant recipients and in patients with acute myeloid leukaemia or myelodysplasia in Brazil. Clin. Microbiol. Infect. 2013, 19, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Lortholary, O.; Obenga, G.; Biswas, P.; Caillot, D.; Chachaty, E.; Bienvenu, A.-L.; Cornet, M.; Greene, J.; Herbrecht, R.; Lacroix, C.; et al. International Retrospective Analysis of 73 Cases of Invasive Fusariosis Treated with Voriconazole. Antimicrob. Agents Chemother. 2010, 54, 4446–4450. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Tudela, J.L.; Berenguer, J.; Guarro, J.; Kantarcioglu, A.S.; Horre, R.; De Hoog, G.S.; Cuenca-Estrella, M. Epidemiology and outcome of Scedosporium prolificans infection, a review of 162 cases. Med. Mycol. 2009, 47, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Wingard, J.R.; Ribaud, P.; Schlamm, H.T.; Herbrecht, R. Changes in causes of death over time after treatment for invasive aspergillosis. Cancer 2008, 112, 2309–2312. [Google Scholar] [CrossRef]
- Nucci, M.; Marr, K.A.; Vehreschild, M.J.; de Souza, C.A.; Velasco, E.; Cappellano, P.; Carlesse, F.; Queiroz-Telles, F.; Sheppard, D.C.; Kindo, A.; et al. Improvement in the outcome of invasive fusariosis in the last decade. Clin. Microbiol. Infect. 2014, 20, 580–585. [Google Scholar] [CrossRef]
- Pastor, F.J.; Guarro, J. Alternaria infections: Laboratory diagnosis and relevant clinical features. Clin. Microbiol. Infect. 2008, 14, 734–746. [Google Scholar] [CrossRef]
- Guarro, J. Fusariosis, a complex infection caused by a high diversity of fungal species refractory to treatment. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 1491–1500. [Google Scholar] [CrossRef]
- Mikulska, M.; Furfaro, E.; Del Bono, V.; Gualandi, F.; Raiola, A.M.; Molinari, M.P.; Gritti, P.; Sanguinetti, M.; Posteraro, B.; Bacigalupo, A.; et al. Galactomannan testing might be useful for early diagnosis of fusariosis. Diagn. Microbiol. Infect. Dis. 2012, 72, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Tortorano, A.M.; Esposto, M.C.; Prigitano, A.; Grancini, A.; Ossi, C.; Cavanna, C.; Cascio, G.L. Cross-Reactivity of Fusarium spp. in the Aspergillus Galactomannan Enzyme-Linked Immunosorbent Assay. J. Clin. Microbiol. 2012, 50, 1051–1053. [Google Scholar] [CrossRef] [PubMed]
- Nucci, M.; Anaissie, E. Invasive fusariosis. Clin. Microbiol. Rev. 2023, 36, e0015922. [Google Scholar] [CrossRef] [PubMed]
- Danion, F.; Duval, C.; Séverac, F.; Bachellier, P.; Candolfi, E.; Castelain, V.; Clere-Jehl, R.; Denis, J.; Dillenseger, L.; Epailly, E.; et al. Factors associated with coinfections in invasive aspergillosis: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.; Audonneau, N.C.; Machouart, M.; Debourgogne, A. Fusarium infections: Epidemiological aspects over 10 years in a university hospital in France. J. Infect. Public Health 2020, 13, 1089–1093. [Google Scholar] [CrossRef]
- Muhammed, M.; Anagnostou, T.; Desalermos, A.; Kourkoumpetis, T.K.; Carneiro, H.A.; Glavis-Bloom, J.; Coleman, J.J.; Mylonakis, E. Fusarium infection: Report of 26 cases and review of 97 cases from the literature. Medicine 2013, 92, 305–316. [Google Scholar] [CrossRef]
- Seidel, D.; Hassler, A.; Salmanton-García, J.; Koehler, P.; Mellinghoff, S.C.; Carlesse, F.; Cheng, M.P.; Falces-Romero, I.; Herbrecht, R.; Jover Sáenz, A.; et al. Invasive Scedosporium spp. and Lomentospora prolificans infections in pediatric patients: Analysis of 55 cases from FungiScope® and the literature. Int. J. Infect. Dis. 2020, 92, 114–122. [Google Scholar] [CrossRef]
- Bronnimann, D.; Garcia-Hermoso, D.; Dromer, F.; Lanternier, F.; Maulin, L.; Leprince, Y.; Brieu, N.; Gruson, B.; El-Samad, Y.; Chouaki, T.; et al. Characterization of the isolates at the NRCMA. Scedosporiosis/lomentosporiosis observational study (SOS): Clinical significance of Scedosporium species identification. Med. Mycol. 2021, 59, 486–497. [Google Scholar] [CrossRef]
- Ramirez-Garcia, A.; Pellon, A.; Rementeria, A.; Buldain, I.; Barreto-Bergter, E.; Rollin-Pinheiro, R.; de Meirelles, J.V.; Xisto, M.I.D.S.; Ranque, S.; Havlicek, V.; et al. Scedosporium and Lomentospora: An updated overview of underrated opportunists. Med. Mycol. 2018, 56 (Suppl. S1), S102–S125. [Google Scholar] [CrossRef]
- Jain, P.; Nagarajan, P.; Prayag, P.; Benton, C.B.; Kadia, T.; Groisberg, R.; Kontoyiannis, D.P.; Mulanovich, V.E.; Pemmaraju, N. Mixed angioinvasive exserohilum and scedosporium infection in a patient with AML. Am. J. Hematol. 2017, 92, 119–120. [Google Scholar] [CrossRef]
- Aragón-Miguel, R.; Calleja-Algarra, A.; Morales-Raya, C.; López-Medrano, F.; Pérez-Ayala, A.; Rodríguez-Peralto, J.L.; Ortiz-Romero, P.L.; Maroñas-Jiménez, L. Alternaria infectoria skin infection in a renal transplant recipient: An emerging phaeohyphomycosis of occidental countries? Int. J. Dermatol. 2017, 56, e153–e155. [Google Scholar] [CrossRef] [PubMed]
- Salmanton-García, J.; Koehler, P.; Kindo, A.; Falces-Romero, I.; García-Rodríguez, J.; Ráčil, Z.; Chen, S.C.-A.; Klimko, N.; Desoubeaux, G.; Thompson, G.R., III; et al. Needles in a haystack: Extremely rare invasive fungal infections reported in FungiScopeⓇ—Global Registry for Emerging Fungal Infections. J. Infect. 2020, 81, 802–815. [Google Scholar] [CrossRef] [PubMed]
- Colombier, M.-A.; Alanio, A.; Denis, B.; Melica, G.; Garcia-Hermoso, D.; Levy, B.; Peraldi, M.-N.; Glotz, D.; Bretagne, S.; Gallien, S. Dual Invasive Infection with Phaeoacremonium parasiticum and Paraconiothyrium cyclothyrioides in a Renal Transplant Recipient: Case Report and Comprehensive Review of the Literature of Phaeoacremonium Phaeohyphomycosis. J. Clin. Microbiol. 2015, 53, 2084–2094. [Google Scholar] [CrossRef] [PubMed]
- Machouart, M.; Garcia-Hermoso, D.; Rivier, A.; Hassouni, N.; Catherinot, E.; Salmon, A.; Debourgogne, A.; Coignard, H.; Lecuit, M.; Bougnoux, M.-E.; et al. Emergence of Disseminated Infections Due to Geosmithia argillacea in Patients with Chronic Granulomatous Disease Receiving Long-Term Azole Antifungal Prophylaxis. J. Clin. Microbiol. 2011, 49, 1681–1683. [Google Scholar] [CrossRef]
- Sprute, R.; Salmanton-García, J.; Sal, E.; Malaj, X.; Falces-Romero, I.; Hatvani, L.; Heinemann, M.; Klimko, N.; López-Soria, L.; Meletiadis, J.; et al. Characterization and outcome of invasive infections due to Paecilomyces variotii: Analysis of patients from the FungiScope® registry and literature reports. J. Antimicrob. Chemother. 2021, 76, 765–774. [Google Scholar] [CrossRef]
- Chen, S.C.-A.; Halliday, C.L.; Hoenigl, M.; Cornely, O.A.; Meyer, W. Scedosporium and Lomentospora Infections: Contemporary Microbiological Tools for the Diagnosis of Invasive Disease. J. Fungi 2021, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Alanio, A.; Brethon, B.; de Chauvin, M.F.; de Kerviler, E.; Leblanc, T.; Lacroix, C.; Baruchel, A.; Menotti, J. Invasive Pulmonary Infection Due to Trichoderma longibrachiatum Mimicking Invasive Aspergillosis in a Neutropenic Patient Successfully Treated with Voriconazole Combined with Caspofungin. Clin. Infect. Dis. 2008, 46, e116–e118. [Google Scholar] [CrossRef]
- Jenks, J.D.; Reed, S.L.; Seidel, D.; Koehler, P.; Cornely, O.A.; Mehta, S.R.; Hoenigl, M. Rare mould infections caused by Mucorales, Lomentospora prolificans and Fusarium, in San Diego, CA: The role of antifungal combination therapy. Int. J. Antimicrob. Agents 2018, 52, 706–712. [Google Scholar] [CrossRef]
- Huang, S.-F.; Wu, A.Y.-J.; Lee, S.S.-J.; Huang, Y.-S.; Lee, C.-Y.; Yang, T.-L.; Wang, H.-W.; Chen, H.J.; Chen, Y.C.; Ho, T.-S.; et al. COVID-19 associated mold infections: Review of COVID-19 associated pulmonary aspergillosis and mucormycosis. J. Microbiol. Immunol. Infect. 2023, 56, 442–454. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name Used in the Study | Current Nomenclature |
|---|---|
| Acremonium brunnescens | Brunneomyces brunnescens |
| Acremonium strictum | Sarocladium strictum |
| Fusarium dimerum | Bisifusarium dimerum |
| Fusarium petroliphilum | Neocosmospora petroliphila |
| Fusarium solani | Neocosmospora solani |
| Geosmithia argillacea | Rasamsonia argillacea |
| Pyrenochaeta romeroi | Medicopsis romeroi |
| Scopulariopsis gracilis | Microascus gracilis |
| Characteristics | N (Range) | % | |||||
|---|---|---|---|---|---|---|---|
| Median age, years | 56 (8; 80) | ||||||
| Age IQR, years | 45–65 | ||||||
| Male/Female | 57/35 | 62.0/38.0 | |||||
| Main host factor (N = 92) | |||||||
| Hematological malignancies (without alloHSCT) | 28 | 30.4 | |||||
| Allogeneic hematopoietic stem cell transplant | 21 | 22.8 | |||||
| Solid organ transplant | 24 | 26.1 | |||||
| Benign hematological/immunological disorder | 5 | 5.4 | |||||
| Solid organ cancer | 2 | 2.2 | |||||
| AIDS | 1 | 1.1 | |||||
| Other | 11 | 12.0 | |||||
| Other risk factors | |||||||
| Neutropenia on day of first symptoms (<0.5 G/L) | 26 | 28.3 | |||||
| Median duration of neutropenia before diagnosis (days) | 28 (1; 274) | ||||||
| Duration of neutropenia IQR (days) | 9–45 | ||||||
| Lymphopenia on day of first symptoms (<1 G/L) | 62 | 67.4 | |||||
| Treatment within the last 90 days before diagnosis | |||||||
| Immuno suppressant | Cancer chemo-therapy | Cancer targeted therapy | Cortico-steroids | ||||
| - | - | - | - | 14 | 15.2 | ||
| + | - | - | - | 5 | 5.4 | ||
| - | + | - | - | 16 | 17.4 | ||
| - | - | + | - | 5 | 5.4 | ||
| - | - | - | + | 4 | 4.3 | ||
| + | + | - | - | 5 | 5.4 | ||
| - | + | - | + | 6 | 6.5 | ||
| + | - | - | + | 29 | 31.5 | ||
| - | - | + | + | 1 | 1.1 | ||
| + | + | - | + | 7 | 7.6 | ||
| Total | 46 | 34 | 6 | 47 | 92 | 100 | |
| Smoking or history of smoking | 37 | 40.2 | |||||
| Prior respiratory diseases | 28 | 30.4 | |||||
| Diabetes mellitus | 24 | 26.1 | |||||
| Mechanical ventilation on day of first symptoms | 12 | 13.0 | |||||
| Antifungal (as prophylaxis or preceding treatment) before diagnosis | |||||||
| Caspofungin | 7 | 7.6 | |||||
| Fluconazole | 10 | 10.9 | |||||
| Itraconazole | 2 | 2.2 | |||||
| Voriconazole * | 11 | 12.0 | |||||
| Posaconazole | 12 | 13.0 | |||||
| Isavuconazole | 1 | 1.1 | |||||
| Amphotericin B (oral) | 1 | 1.1 | |||||
| Amphotericin B (IV) * | 2 | 2.2 | |||||
| Characteristics | N | % | |
|---|---|---|---|
| Species involved in infections by one mold (n = 69) | |||
| Fusarium spp. | 25 | 27.2 | |
| Scedosporium spp. | 10 | 10.9 | |
| Alternaria spp. | 9 | 9.8 | |
| Penicillium spp. | 6 | 6.5 | |
| Trichoderma spp. | 4 | 4.3 | |
| Phaeoacremonium spp. | 3 | 3.2 | |
| Acremonium spp. | 2 | 2.2 | |
| Cladophialophora bantiana | 2 | 2.2 | |
| Scopulariopsis spp. | 2 | 2.2 | |
| Cladosporium spp. | 1 | 1.1 | |
| Chrysosporium spp. | 1 | 1.1 | |
| Geosmithia argillacea | 1 | 1.1 | |
| Pyrenochaeta romeroi | 1 | 1.1 | |
| Schizophyllum commune | 1 | 1.1 | |
| Dematious mold not further identified | 1 | 1.1 | |
| Species involved in infections by several molds (n = 23) | |||
| Fusarium spp. + Aspergillus spp. | 6 | 6.5 | |
| Scedosporium spp. + Aspergillus spp. | 4 | 4.3 | |
| Acremonium spp. + Aspergillus spp. | 2 | 2.2 | |
| Paecilomyces spp. + Aspergillus spp. | 2 | 2.2 | |
| Alternaria sp. + Aspergillus fumigatus | 1 | 1.1 | |
| Alternaria alternata + Fusarium sp. + Aspergillus fumigatus | 1 | 1.1 | |
| Arthrographis kalrae + Aspergillus fumigatus | 1 | 1.1 | |
| Fusarium dimerum + Lichtheimia corymbifera | 1 | 1.1 | |
| Fusarium sp. + Paecilomyces sp. | 1 | 1.1 | |
| Fusarium proliferatum + Scedosporium apiospermum + Rhizopus oryzae | 1 | 1.1 | |
| Lomentospora prolificans + Scedosporium apiospermum + Lichtheimia sp. | 1 | 1.1 | |
| Paecilomyces sp. + Mucor sp. | 1 | 1.1 | |
| Scopulariopsis sp. + Aspergillus lentulus + Rhizomucor sp. | 1 | 1.1 | |
| Infection site | |||
| Pulmonary infection without further extension | 39 | 42.4 | |
| Extra-pulmonary focal infection (Of which 12 acral, 5 sinusal, 5 abdominal, 1 cerebral and 1 tonsillar) | 24 | 26.1 | |
| Disseminated infection without pulmonary involvement | 12 | 13.0 | |
| Disseminated infection with pulmonary involvement | 17 | 18.5 | |
| Proportion MIC Test Available | Percentage with MIC > 2 mg/L among Available Ones (Number Tested) | |||||||
|---|---|---|---|---|---|---|---|---|
| AmB | ITZ | VRZ | PSZ | ISZ | CAS | 5FC | ||
| Acremonium spp. | 1/4 | 100 (1) | 0 (1) | 0 (1) | 0 (1) | - (0) | 100 (1) | - (0) |
| Alternaria spp. | 3/11 | 0 (3) | 33 (3) | 67 (3) | 0 (3) | 67 (3) | 67 (3) | - (0) |
| Chrysosporium | 1/1 | 0 (1) | 100 (1) | 0 (1) | 0 (1) | - (0) | 0 (1) | - (0) |
| Fusarium spp. | 21/35 | 86 (21) | 100 (21) | 81 (21) | 90 a (21) | 100 (10) | 100 (21) | 100 (2) |
| G. argilacea | 1/1 | 100 (1) | 100 (1) | 100 (1) | 100 (1) | - (0) | 0 (1) | - (0) |
| Paecylomyces spp. | 2/4 | 50 (2) | 50 (2) | 100 (2) | 50 b (2) | - (0) | 50 (2) | - (0) |
| Penicillium spp. | 4/6 | 0 (4) | 50 (4) | 50 (4) | 25 (4) | 33 (3) | 25 (4) | - (0) |
| Phaeoacremonium spp. | 2/3 | 50 (2) | 50 (2) | 50 (2) | 100 (2) | 0 (1) | 100 (2) | - (0) |
| Scedosporium spp. | 12/16 | 100 (12) | 83 (12) | 0 (12) | 33 c (12) | 75 (4) | 50 (12) | 100 (2) |
| Scopulariopsis spp. | 1/3 | 100 (1) | 100 (1) | 100 (1) | 100 (1) | - (0) | 0 d (1) | - (0) |
| Trichoderma spp. | 4/4 | 25 (4) | 75 (4) | 0 (4) | 50 (4) | 75 (4) | 0 (4) | - (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ledoux, M.-P.; Dicop, E.; Sabou, M.; Letscher-Bru, V.; Castelain, V.; Danion, F.; Herbrecht, R. Fusarium, Scedosporium and Other Rare Mold Invasive Infections: Over Twenty-Five-Year Experience of a European Tertiary-Care Center. J. Fungi 2024, 10, 289. https://doi.org/10.3390/jof10040289
Ledoux M-P, Dicop E, Sabou M, Letscher-Bru V, Castelain V, Danion F, Herbrecht R. Fusarium, Scedosporium and Other Rare Mold Invasive Infections: Over Twenty-Five-Year Experience of a European Tertiary-Care Center. Journal of Fungi. 2024; 10(4):289. https://doi.org/10.3390/jof10040289
Chicago/Turabian StyleLedoux, Marie-Pierre, Elise Dicop, Marcela Sabou, Valérie Letscher-Bru, Vincent Castelain, François Danion, and Raoul Herbrecht. 2024. "Fusarium, Scedosporium and Other Rare Mold Invasive Infections: Over Twenty-Five-Year Experience of a European Tertiary-Care Center" Journal of Fungi 10, no. 4: 289. https://doi.org/10.3390/jof10040289
APA StyleLedoux, M.-P., Dicop, E., Sabou, M., Letscher-Bru, V., Castelain, V., Danion, F., & Herbrecht, R. (2024). Fusarium, Scedosporium and Other Rare Mold Invasive Infections: Over Twenty-Five-Year Experience of a European Tertiary-Care Center. Journal of Fungi, 10(4), 289. https://doi.org/10.3390/jof10040289