
Mapping of Chronic Pulmonary Aspergillosis in Africa

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
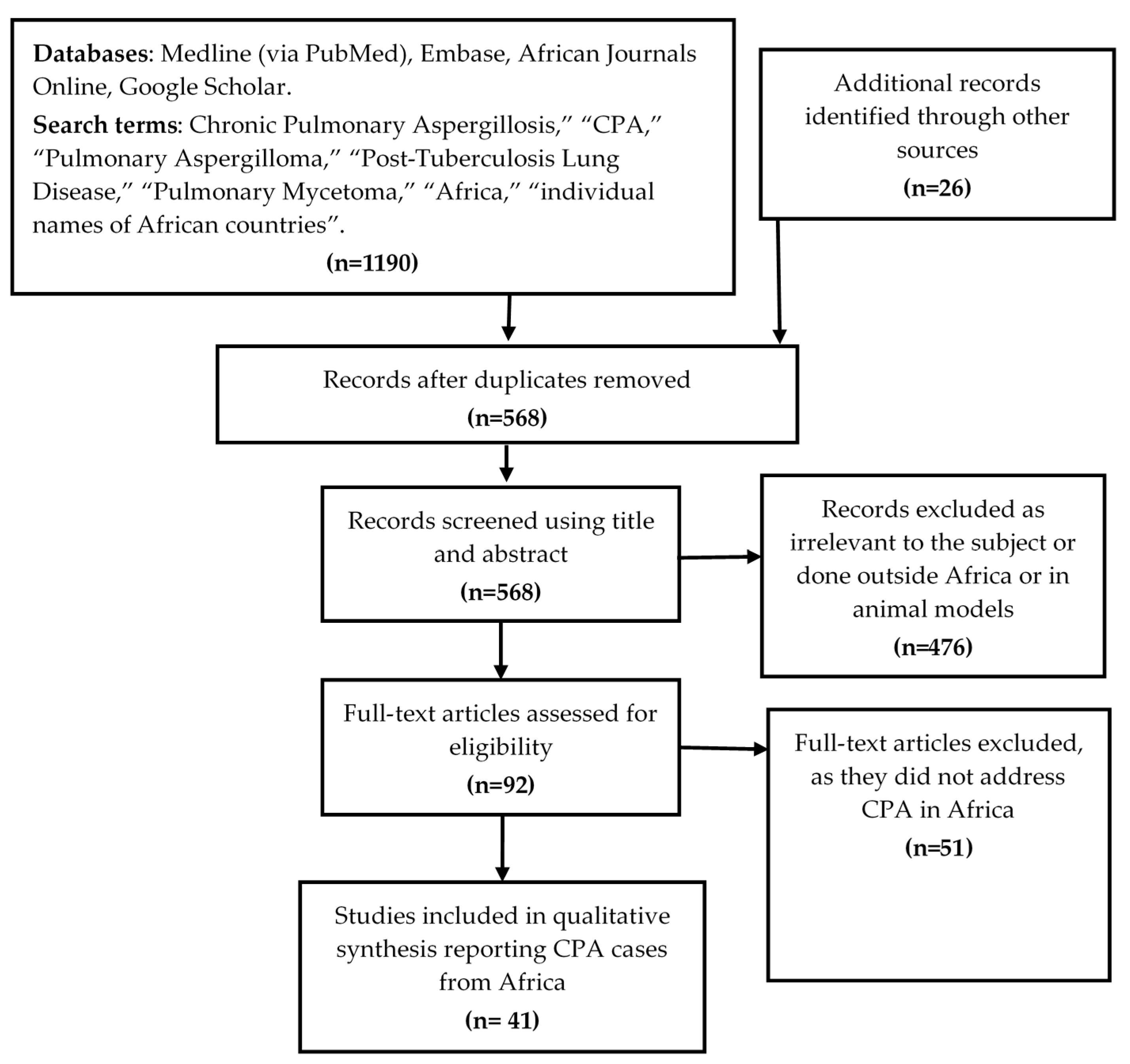
3.1. Search Results
3.2. Summary of Studies
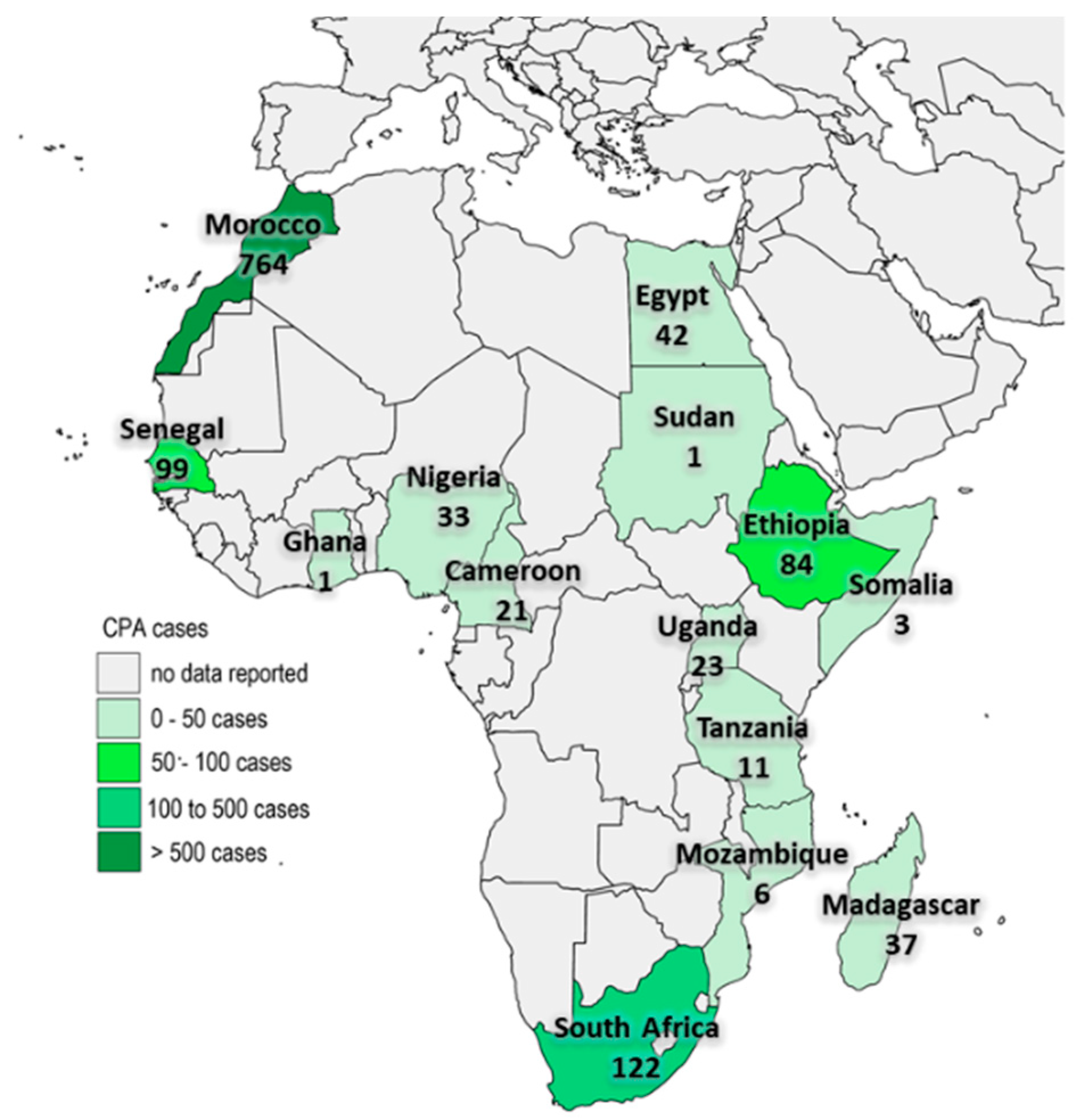
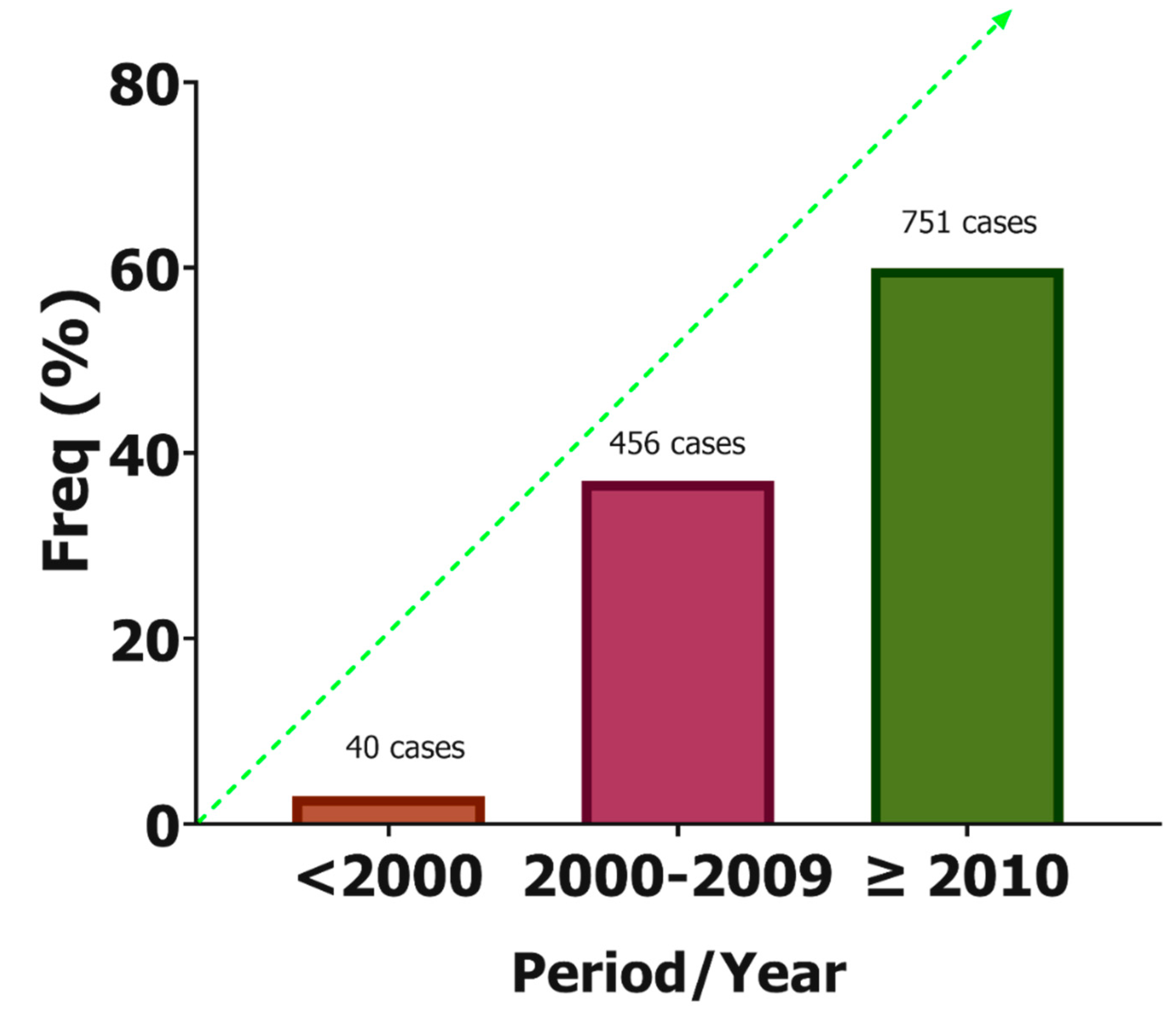
3.3. Cases of CPA in Africa
3.4. Underlying Comorbidities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denning, D.W.; Riniotis, K.; Dobrashian, R.; Sambatakou, H. Chronic cavitary and fibrosing pulmonary and pleural aspergillosis: Case series, proposed nomenclature change, and review. Clin. Infect. Dis. 2003, 37, S265–S280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowes, D.; Al-Shair, K.; Newton, P.J.; Morris, J.; Harris, C.; Rautemaa-Richardson, R.; Denning, D.W. Predictors of mortality in chronic pul-monary aspergillosis. Eur. Respir. J. 2017, 49, 1601062. [Google Scholar] [CrossRef]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2015, 47, 45–68. [Google Scholar] [CrossRef]
- Denning, D.W.; Page, I.; Chakaya, J.; Jabeen, K.; Jude, C.M.; Cornet, M.; Alastruey-Izquierdo, A.; Bongomin, F.; Bowyer, P.; Chakrabarti, A.; et al. Case definition of chronic pulmonary aspergillosis in resource-constrained settings. Emerg. Infect. Dis. 2018, 24, e171312. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F. Post-tuberculosis chronic pulmonary aspergillosis: An emerging public health concern. PLoS Pathog. 2020, 16, e1008742. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.L.; Denning, D.W. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur. Respir. J. 2010, 37, 865–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and multi-national prevalence of fungal diseases—estimate precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Kwizera, R.; Katende, A.; Bongomin, F.; Nakiyingi, L.; Kirenga, B.J. Misdiagnosis of chronic pulmonary aspergillosis as pulmonary tuberculosis at a tertiary care center in Uganda: A case series. J. Med. Case Rep. 2021, 15, 140. [Google Scholar] [CrossRef]
- Ohba, H.; Miwa, S.; Shirai, M.; Kanai, M.; Eifuku, T.; Suda, T.; Hayakawa, H.; Chida, K. Clinical characteristics and prognosis of chronic pulmonary aspergillosis. Respir. Med. 2012, 106, 724–729. [Google Scholar] [CrossRef] [Green Version]
- Hay, R.; Denning, D.W.; Bonifaz, A.; Queiroz-Telles, F.; Beer, K.; Bustamante, B.; Chakrabarti, A.; Chavez-Lopez, M.D.G.; Chiller, T.; Cornet, M.; et al. The diagnosis of fungal neglected tropical diseases (fungal NTDs) and the role of investigation and laboratory tests: An expert consensus report. Trop. Med. Infect. Dis. 2019, 4, 122. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; PRISMA-P Group; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alemu, B.N. Surgical outcome of chronic pulmonary aspergilloma: An experience from two tertiary referral hos-pitals in addis Ababa, Ethiopia. Ethiop. J. Health Sci. 2020, 30, 521–530. [Google Scholar] [PubMed]
- Harmouchi, H.; Lakranbi, M.; Issoufou, I.; Ouadnouni, Y.; Smahi, M. Pulmonary aspergilloma: Surgical outcome of 79 patients in a Moroccan center. Asian Cardiovasc. Thorac. Ann. 2019, 27, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Salami, M.A.; Sanusi, A.A.; Adegboye, V.O. Current indications and outcome of pulmonary resections for tuberculosis complications in Ibadan, Nigeria. Med. Princ. Pract. 2017, 27, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Masoud, S.; Irusen, E.; Koegelenberg, C.; Du Preez, L.; Allwood, B. Outcomes of resectable pulmonary aspergilloma and the per-formance gap in a high tuberculosis prevalence setting: A retrospective study. Afr. J. Thorac. Crit. Care Med. 2017, 23, 8–13. [Google Scholar]
- El Hammoumi, M.M.; Slaoui, O.; El Oueriachi, F.; Kabiri, E.H. Lung resection in pulmonary aspergilloma: Experience of a Moroccan center vascular and thoracic surgery. BMC Surg. 2015, 15, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ba, P.; Ndiaye, A.R.; Diatta, S.; Ciss, A.; Dieng, P.; Gaye, M.; Fall, M.; Ndiaye, M. Results of surgical treatment for pulmonary aspergilloma. Med. Sante Trop. 2015, 25, 92–96. [Google Scholar] [CrossRef]
- Benjelloun, H.; Zaghba, N.; Yassine, N.; Bakhatar, A.; Karkouri, M.; Ridai, M.; Bahlaoui, A. Chronic pulmonary aspergillosis: A frequent and potentially severe disease. Méd. Mal. Infect. 2015, 45, 128–132. [Google Scholar] [CrossRef]
- Ade, S.S.; Touré, N.O.; Ndiaye, A.; Diarra, O.; Dia Kane, Y.; Diatta, A.; Ndiayeb, M.; Hanea, A.A. Aspects épidémiologiques, cliniques, thérapeutiques et évolutifs de l’aspergillome pulmonaire à Dakar. Rev. Mal. Respir. 2011, 28, 322–327. [Google Scholar] [CrossRef]
- Bekele, A.; Gulilat, D.; Kassa, S.; Ali, A. Aspergilloma of the lungs: Operative experience from Tikur Anbessa Hospital, Ethiopia. East Cent. Afr. J. Surg. 2009, 14, 44–49. [Google Scholar]
- Brik, A.; Salem, A.M.; Kamal, A.R.; Abdel-Sadek, M.; Essa, M.; El Sharawy, M.; Deebes, A.; Bary, K.A. Surgical outcome of pulmonary aspergilloma. Eur. J. Cardio-Thorac. Surg. 2008, 34, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Van Den Heuvel, M.M.; Els, Z.; Koegelenberg, C.F.; Naidu, K.M.; Bolliger, C.T.; Diacon, A.H. Risk factors for recurrence of haemoptysis following bronchial artery embolisation for life-threatening haemoptysis. Int. J. Tuberc. Lung Dis. 2007, 11, 909–914. [Google Scholar] [PubMed]
- Caidi, M.; Kabiri, H.; Al Aziz, S.; El Maslout, A.; Benosman, A. Chirurgie des aspergillomes pulmonaires. La Presse Med. 2006, 35, 1819–1824. [Google Scholar] [CrossRef]
- Mbembati, N.A.A.; Lema, L.E.K. Pulmonary aspergilloma: A 15 years experience in Dar es Salaam, Tanzania. East Cent. Afr. J. Surg. 2001, 6. Available online: https://www.ajol.info/index.php/ecajs/article/view/136632 (accessed on 17 September 2021).
- Ba, M.; Ciss, G.; Diarra, O.; Kane, O.; Ndiaye, M. Surgical aspects of pulmonary aspergilloma in 24 patients. Dakar Med. 2000, 45, 144–146. [Google Scholar] [PubMed]
- Kabiri, E.H.; Lahlou, K.; Achir, A.; Al Aziz, S.; El Meslout, A.; Benosman, A. Les aspergillomes pulmonaires: Résultats du traitement chirurgical. À propos d’une série de 206 cas. Chirurgie 1999, 124, 655–660. [Google Scholar] [CrossRef]
- Conlan, A.; Abramor, E.; Moyes, D.G. Pulmonary aspergilloma-indications for surgical intervention. An analysis of 22 cases. S. Afr. Med. J. 1987, 71, 285–288. [Google Scholar]
- Adeyemo, A.O.; Odelowo, E.O.; Makanjuola, D.I. Management of pulmonary aspergilloma in the presence of active tuberculosis. Thorax 1984, 39, 862–867. [Google Scholar] [CrossRef] [Green Version]
- Kwizera, R.; Katende, A.; Teu, A.; Apolot, D.; Worodria, W.; Kirenga, B.J.; Bongomin, F. Algorithm-aided diagnosis of chronic pulmonary aspergillosis in low- and middle-income countries by use of a lateral flow device. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 39, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Bongomin, F.; Kwizera, R.; Atukunda, A.; Kirenga, B.J. Cor pulmonale complicating chronic pulmonary aspergillosis with fatal consequences: Experience from Uganda. Med. Mycol. Case Rep. 2019, 25, 22–24. [Google Scholar] [CrossRef]
- Nonga, B.N.; Jemea, B.; Pondy, A.O.; Handy Eone, D.; Bitchong, M.C.; Fola, O.; Nkolaka, A.; Londji, G.M. Unusual Life-Threatening Pneumothorax Com-plicating a Ruptured Complex Aspergilloma in an Immunocompetent Patient in Cameroon. Case Rep. Surg. 2018, 2018, 8648732. [Google Scholar] [PubMed] [Green Version]
- Gbaja-Biamila, T.; Bongomin, F.; Irurhe, N.; Nwosu, A.; Oladele, R. Chronic Pulmonary Aspergillosis Misdiagnosed as Smear-Negative Pulmonary Tuberculosis in a TB Clinic in Nigeria. J. Adv. Med. Med. Res. 2018, 26, 41816. [Google Scholar] [CrossRef]
- Ofori, A.; Steinmetz, A.R.; Akaasi, J.; Frimpong, G.A.; Norman, B.R.; Obeng-Baah, J.; Bedu-Addo, G.; Phillips, R.O. Pulmonary aspergilloma: An evasive disease. Int. J. Mycobacteriol. 2016, 5, 235–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekwueme, C.; Otu, A.A.; Chinenye, S.; Unachukwu, C.; Oputa, R.N.; Korubo, I.; Enang, O.E. Haemoptysis in a female with diabetes mellitus: A unique presentation of chronic pulmonary aspergillosis, pulmonary tuberculosis, and Klebsiella peumoniae co-infection. Clin. Case Rep. 2016, 4, 432–436. [Google Scholar] [CrossRef]
- Koegelenberg, C.F.; Bruwer, J.W.; Bolliger, C.T. Endobronchial valves in the management of recurrent haemoptysis. Respiration 2014, 87, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Pohl, C.; Jugheli, L.; Haraka, F.; Mfinanga, E.; Said, K.; Reither, K. Pulmonary aspergilloma: A treatment challenge in Sub-Saharan Africa. PLoS Negl. Trop. Dis. 2013, 7, e2352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Hammoumi, M.; Traibi, A.; El Oueriachi, F.; Arsalane, A.; Kabiri, E. Surgical treatment of aspergilloma grafted in hydatid cyst cavity. Rev. Port. Pneumol. 2013, 19, 281–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smahi, M.; Serraj, M.; Ouadnouni, Y.; Chbani, L.; Znati, K.; Amarti, A. Aspergilloma in combination with adenocarcinoma of the lung. World J. Surg. Oncol. 2011, 9, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aderaye, G.; Jajaw, A. Bilateral pulmonary aspergilloma: Case report. East Afr. Med. J. 1996, 73, 487–488. [Google Scholar]
- Mahgoub, E.S.; El Hassan, A.M. Pulmonary aspergillosis caused by Aspergillus flavus. Thorax 1972, 27, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Issoufou, I.; Sani, R.; Belliraj, L.; Ammor, F.Z.; Moussa Ounteini, A.; Ghalimi, J.; Lakranbi, M.; Ouadnouni, Y.; Smahi, M. Pneumonectomie pour poumon détruit post-tuberculeux: Une série de 26 cas opérés. Rev. Pneumol. Clin. 2016, 72, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.Y.; Hospital, M.; Elmi, M.-S.A.M.; Surgeon, S.; Baldan, M.-S.M. Experience of Thoracic Surgery Performed Under Difficult Conditions in Somalia. Introduction Patients and Methods. East Cent. Afr. J. Surg. 2004, 9. Available online: https://www.ajol.info/index.php/ecajs/article/view/137294 (accessed on 17 September 2021).
- Hassan, M.Y.; Baldan, M. Aspergillus of the Lung with Haemoptysis: A surgical emergency. East Cent. Afr. J. Surg. 2004, 9, 1–2. [Google Scholar]
- Kane, P.A.; Sarr, A.M.; Courbil, J.L.; Derrien, J.C.; Coly, D.; Diop, B.; Nadio, A.; Sankalé, M. Pulmonary aspergillosis. The 1st case in Dakar. Bull. Soc. Med. Afr. Noire Lang. Fr. 1976, 21, 157–160. [Google Scholar] [PubMed]
- Ngo Nonga, B.; Bang, G.A.; Jemea, B.; Savom, E.; Yone, P.; Mbatchou, N.; Ze, J.J. Complex Pulmonary Aspergilloma: Surgical Challenges in a Third World Setting. Surg. Res. Pract. 2018, 2018, 6570741. [Google Scholar] [CrossRef]
- Rakotoson, J.L.; Razafindramaro, N.; Rakotomizao, J.R.; Vololontiana, H.M.D.; Andrianasolo, R.L.; Ravahatra, K.; Tiaray, M.; Rajaoarifetra, J.; Rakotoharivelo, H.; Andrianarisoa, A.C.F. Les aspergillomes pulmonaires: À propos de 37 cas à Nadagascar. Pan Afr. Med. J. 2011, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Gross, A.M.; Diacon, A.H.; Heuvel, M.M.V.D.; Van Rensburg, J.; Harris, D.; Bolliger, C.T. Management of life-threatening haemoptysis in an area of high tuberculosis incidence. Int. J. Tuberc. Lung Dis. 2009, 13, 875–880. [Google Scholar] [PubMed]
- Corr, P. Management of severe hemoptysis from pulmonary aspergilloma using endovascular embolization. Cardiovasc. Intervent. Radiol. 2006, 29, 807–810. [Google Scholar] [CrossRef] [PubMed]
- Falkson, C.; Sur, R.; Pacella, J. External beam radiotherapy: A treatment option for massive haemoptysis caused by mycetoma. Clin. Oncol. 2002, 14, 233–235. [Google Scholar] [CrossRef]
- Oladele, R.O.; Irurhe, N.K.; Foden, P.; Akanmu, A.S.; Gbaja-Biamila, T.; Nwosu, A.; Ekundayo, H.A.; Ogunsola, F.T.; Richardson, M.D.; Denning, D.W. Chronic pulmonary aspergillosis as a cause of smear-negative TB and/or TB treatment failure in Nigerians. Int. J. Tuberc. Lung Dis. 2017, 21, 1056–1061. [Google Scholar] [CrossRef]
- Page, I.D.; Byanyima, R.; Hosmane, S.; Onyachi, N.; Opira, C.; Richardson, M.; Sawyer, R.; Sharman, A.; Denning, D.W. Chronic pulmonary aspergillosis commonly complicates treated pulmonary tuberculosis with residual cavitation. Eur. Respir. J. 2019, 53, 1801184. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Denning, D.; Chakrabarti, A. Estimation of the burden of chronic and allergic pulmonary aspergillosis in India. PLoS ONE 2014, 9, e114745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denning, D.W.; Pleuvry, A.; Cole, D. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Pleuvry, A.; Cole, D. Global burden of chronic pulmonary aspergillosis complicating sarcoidosis. Eur. Respir. J. 2012, 41, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Jhun, B.W.; Jung, W.J.; Hwang, N.Y.; Park, H.Y.; Jeon, K.; Kang, E.S.; Koh, W.G. Risk factors for the development of chronic pulmonary as-pergillosis in patients with nontuberculous mycobacterial lung disease. PLoS ONE 2017, 12, e0188716. [Google Scholar] [CrossRef]
- Baluku, J.B.; Nuwagira, E.; Bongomin, F.; Denning, D.W. Pulmonary TB and chronic pulmonary aspergillosis: Clinical differences and similarities. Int. J. Tuberc. Lung Dis. 2021, 25, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Cadranel, J.; Philippe, B.; Hennequin, C.; Bergeron, A.; Bergot, E.; Bourdin, A.; Cottin, V.; Jeanfaivre, T.; Godet, C.; Pineau, M.; et al. Voriconazole for chronic pulmonary aspergillosis: A prospective multicenter trial. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 3231–3239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Vishwanath, G.; Aggarwal, A.N.; Garg, M.; Gupta, D.; Chakrabarti, A. Itraconazole in chronic cavitary pulmonary aspergillosis: A randomised controlled trial and systematic review of literature. Mycoses 2013, 56, 559–570. [Google Scholar] [CrossRef]
- Izumikawa, K.; Ohtsu, Y.; Kawabata, M.; Takaya, H.; Miyamoto, A.; Sakamoto, S.; Kishi, K.; Tsuboi, E.; Homma, S.; Yoshimura, K. Clinical efficacy of micafungin for chronic pulmonary aspergillosis. Sabouraudia 2007, 45, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Denning, D.W. Diagnosing pulmonary aspergillosis is much easier than it used to be: A new diagnostic landscape. Int. J. Tuberc. Lung Dis. 2021, 25, 525–536. [Google Scholar] [CrossRef]
- Hunter, E.S.; Richardson, M.D.; Denning, D.W. Evaluation of LDBio aspergillus ICT lateral flow assay for IgG and IgM antibody detection in chronic pulmonary aspergillosis. J. Clin. Microbiol. 2019, 57, e00538-19. [Google Scholar] [CrossRef] [Green Version]
- Salzer, H.J.F.; Massango, I.; Bhatt, N.; Machonisse, E.; Reimann, M.; Heldt, S.; Lange, C.; Hoelscher, M.; Khosa, C.; Rachow, A. Seroprevalence of aspergillus-specific IgG antibody among mozambican tuberculosis patients. J. Fungi 2021, 7, 595. [Google Scholar] [CrossRef] [PubMed]
- Rozaliyani, A.; Rosianawati, H.; Handayani, D.; Agustin, H.; Zaini, J.; Syam, R.; Adawiyah, R.; Tugiran, M.; Setianingrum, F.; Burhan, E.; et al. Chronic pulmonary aspergillosis in post tuberculosis patients in indonesia and the role of LDBio aspergillus ICT as part of the diagnosis scheme. J. Fungi 2020, 6, 318. [Google Scholar] [CrossRef] [PubMed]
- Orefuwa, E.; Gangneux, J.P.; Denning, D.W. The challenge of access to refined fungal diagnosis: An investment case for low- and middle-income countries. J. Med. Mycol. 2021, 31, 101140. [Google Scholar] [CrossRef]
- Denning, D.W. The ambitious ’95-95 by 2025’ roadmap for the diagnosis and management of fungal diseases. Thorax 2015, 70, 613–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongomin, F.; Govender, N.P.; Chakrabarti, A.; Robert-Gangneux, F.; Boulware, D.; Zafar, A.; Oladele, R.O.; Richardson, M.D.; Gangneux, J.-P.; Alastruey-Izquierdo, A.; et al. Essential in vitro diagnostics for advanced HIV and serious fungal diseases: International experts’ consensus recommendations. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1581–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmidis, C.; Denning, D.W. The clinical spectrum of pulmonary aspergillosis. Thorax 2014, 70, 270–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Y.; Soubani, A. Advances in the diagnosis and management of pulmonary aspergillosis. Adv. Respir. Med. 2020, 87, 231–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kousha, M.; Tadi, R.; Soubani, A.O. Pulmonary aspergillosis: A clinical review. Eur. Respir. Rev. 2011, 20, 156–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmidis, C.; Newton, P.; Muldoon, E.G.; Denning, D.W. Chronic fibrosing pulmonary aspergillosis: A cause of ‘destroyed lung’ syndrome. Infect. Dis. 2016, 49, 296–301. [Google Scholar] [CrossRef]
- Bongomin, F.; Otu, A. Utility of St. George’s respiratory questionnaire in predicting clinical recurrence in chronic pulmonary aspergillosis. Ther. Adv. Infect. Dis. 2021, 8, 204993612110346. [Google Scholar]
- Kneale, M.; Bartholomew, J.S.; Davies, E.; Denning, D.W. Global access to antifungal therapy and its variable cost. J. Antimicrob. Chemother. 2016, 71, 3599–3606. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Model List of Essential Medicines, 20th List (March 2017, Amended August 2017); World Health Organization: Geneva, Switzerland, 2017; Available online: https://www.who.int/publications/i/item/eml-20 (accessed on 17 September 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Region | Number of Publications | Percentage |
|---|---|---|---|
| Morocco [13,16,18,23,26,37,38,41] | North Africa | 8 | 19.5 |
| South Africa [15,22,27,35,47,48,49] | Southern Africa | 7 | 17.1 |
| Nigeria [14,28,32,34,50] | West Africa | 5 | 12.2 |
| Senegal [17,19,25,44] | West Africa | 4 | 9.8 |
| Uganda [8,29,30,51] | East Africa | 4 | 9.8 |
| Ethiopia [12,20,39] | East Africa | 3 | 7.3 |
| Cameroon [31,45] | Central Africa | 2 | 4.9 |
| Tanzania [24,36] | East Africa | 2 | 4.9 |
| Egypt [21] | North Africa | 1 | 2.4 |
| Ghana [33] | West Africa | 1 | 2.4 |
| Madagascar [46] | East Africa | 1 | 2.4 |
| Mozambique/Somalia [43] | East Africa | 1 | 2.4 |
| Somalia [42] | East Africa | 1 | 2.4 |
| Sudan [40] | North Africa | 1 | 2.4 |
| Study Type | Country | Region | Study Period | CPA Cases | Mean Age (Years) | Male: n (%) | |
|---|---|---|---|---|---|---|---|
| Kwizera et al. (2021) [8] | Case Series | Uganda | East Africa | - | 3 | 38.7 | 0 (0) |
| Alemu et al. (2020) [12] | Retrospective | Ethiopia | East Africa | 2014–2019 | 72 | 35.2 | 46 (63.9) |
| Kwizera et al. (2020) [29] | Case Report | Uganda | East Africa | - | 1 | 40.0 | 0 (0) |
| Harmouchi et al. (2019) [13] | Retrospective | Morocco | North Africa | 2009–2018 | 79 | 40.5 | 57 (72.2) |
| Bongomin et al. (2019) [30] | Case Report | Uganda | East Africa | 2018 | 1 | 45.0 | 1 (100) |
| Nonga et al. (2018) [31] | Case Report | Cameroon | Central Africa | - | 1 | 47.0 | 1 (100) |
| Nonga et al. (2018) [45] | Prospective | Cameroon | Central Africa | 2012–2015 | 20 | 30.0 | 17 (85) |
| Gbaja-Biamila et al. (2018) [32] | Case Report | Nigeria | West Africa | 2016 | 1 | 35.0 | 1 (100) |
| Salami et al. (2018) [14] | Retrospective | Nigeria | West Africa | 2014–2017 | 2 | 32.0 | 1 (50) |
| Masoud et al. (2017) [15] | Retrospective | South Africa | Southern Africa | 2013–2015 | 59 | 46.6 | 36 (61) |
| Oladele et al. (2017) [50] | Cross sectional | Nigeria | West Africa | 2014–2015 | 18 | - | - |
| Page et al. (2019) [51] | Cross sectional | Uganda | East Africa | 2012–2013 | 18 | - | 11 (80.0) |
| Issoufoua et al. (2016) [41] | Case Series | Morocco | North Africa | 2009–2014 | 6 | 38.8 | - |
| Ofori et al. (2016) [33] | Case Report | Ghana | West Africa | 2013 | 1 | 38.0 | 1 (100) |
| Ekwueme et al. (2016) [34] | Case Report | Nigeria | West Africa | - | 1 | 56.0 | 0 (0) |
| Hammoumi et al. (2015) [16] | Retrospective | Morocco | North Africa | 2006–2014 | 274 | 37.8 | 93 (33.9) |
| Ba et al. (2015) [17] | Retrospective | Senegal | West Africa | 2004–2008 | 35 | 43.4 | 28 (80) |
| Benjelloun et al. (2015) [18] | Retrospective | Morocco | West Africa | 2003–2014 | 81 | 51.0 | 48 (59.3) |
| Koegelenberg et al. (2014) [35] | Case Report | South Africa | Southern Africa | - | 1 | 30.0 | 1 (100) |
| Pohl et al. (2013) [36] | Case Report | Tanzania | East Africa | 2011 | 1 | 68.0 | 1 (100) |
| Hammoumi et al. (2013) [37] | Case Report | Morocco | North Africa | - | 3 | 47.7 | 3 (100) |
| Ade et al. (2011) [19] | Retrospective | Senegal | West Africa | 2004–2008 | 35 | 43.4 | 28 (80) |
| Rakotoson et al. (2011) [46] | Prospective | Madagascar | East Africa | 2006–2010 | 37 | 43.0 | 29 (78.4) |
| Smahi et al. (2011) [38] | Case Report | Morocco | North Africa | 1991–2000 | 1 | 60.0 | 1 (100) |
| Gross et al. (2009) [47] | Prospective | South Africa | Southern Africa | - | 10 | 41.4 | - |
| Bekele et al. (2009) [20] | Retrospective | Ethiopia | East Africa | 2005–2008 | 11 | 38.9 | 9 (81.8) |
| Brik et al. (2008) [21] | Retrospective | Egypt | North Africa | 2001–2008 | 42 | 44.0 | 28 (66.7) |
| van den Heuvel et al. (2007) [22] | Retrospective | South Africa | Southern Africa | 2001–2003 | 13 | - | - |
| Hassan et al. (2004a) [42] | Case Series | Somalia | East Africa | 2000–2003 | 1 | - | - |
| Corr (2006) [48] | Prospective | South Africa | Southern Africa | 2002–2003 | 12 | 36.0 | 9 (75) |
| Caidi et al. (2006) * [23] | Retrospective | Morocco | North Africa | 1982–2004 | 320 | 32.0 | 161 (57.9) |
| Hassan et al. (2004b) [43] | Case Series | Mozambique /Somalia | East Africa | - | 8 | 30.0 | 6 (75) |
| Falkson et al. (2002) [49] | Prospective | South Africa | Southern Africa | 1989–1994 | 5 | 45.0 | 5 (100) |
| Mbembati et al. (2001) [24] | Retrospective | Tanzania | East Africa | 1986–2000 | 10 | - | 8 (80) |
| Ba et al. (2000) [25] | Retrospective | Senegal | West Africa | 1991–1998 | 24 | - | - |
| Kabiri et al. (1999) * [26] | Retrospective | Morocco | North Africa | 1982–1998 | - | - | - |
| Aderaye et al. (1996) [39] | Case Report | Ethiopia | East Africa | - | 1 | 25.0 | 0 (0) |
| Conlan et al. (1987) [27] | Retrospective | South Africa | Southern Africa | 1982–1984 | 22 | - | 7 (31.8) |
| Adebayo et al. (1984) [28] | Retrospective | Nigeria | West Africa | 1977–1983 | 11 | 42.2 | 7 (63.6) |
| Kane et al. (1976) [44] | Case Series | Senegal | West Africa | - | 5 | - | - |
| Mahgoub et al. (1972) [40] | Case Report | Sudan | North Africa | 1968–1971 | 1 | 45.0 | 1 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olum, R.; Osaigbovo, I.I.; Baluku, J.B.; Stemler, J.; Kwizera, R.; Bongomin, F. Mapping of Chronic Pulmonary Aspergillosis in Africa. J. Fungi 2021, 7, 790. https://doi.org/10.3390/jof7100790
Olum R, Osaigbovo II, Baluku JB, Stemler J, Kwizera R, Bongomin F. Mapping of Chronic Pulmonary Aspergillosis in Africa. Journal of Fungi. 2021; 7(10):790. https://doi.org/10.3390/jof7100790
Chicago/Turabian StyleOlum, Ronald, Iriagbonse Iyabo Osaigbovo, Joseph Baruch Baluku, Jannik Stemler, Richard Kwizera, and Felix Bongomin. 2021. "Mapping of Chronic Pulmonary Aspergillosis in Africa" Journal of Fungi 7, no. 10: 790. https://doi.org/10.3390/jof7100790
APA StyleOlum, R., Osaigbovo, I. I., Baluku, J. B., Stemler, J., Kwizera, R., & Bongomin, F. (2021). Mapping of Chronic Pulmonary Aspergillosis in Africa. Journal of Fungi, 7(10), 790. https://doi.org/10.3390/jof7100790